Mesh-Type Three-Dimensional (3D) Printing of Human Organs and Tumors: Fast, Cost-Effective, and Personalized Anatomic Modeling of Patient-Oriented Visual Aids

 ,
,
Abstract
1. Introduction
2. Methods
2.1. Ethical Considerations
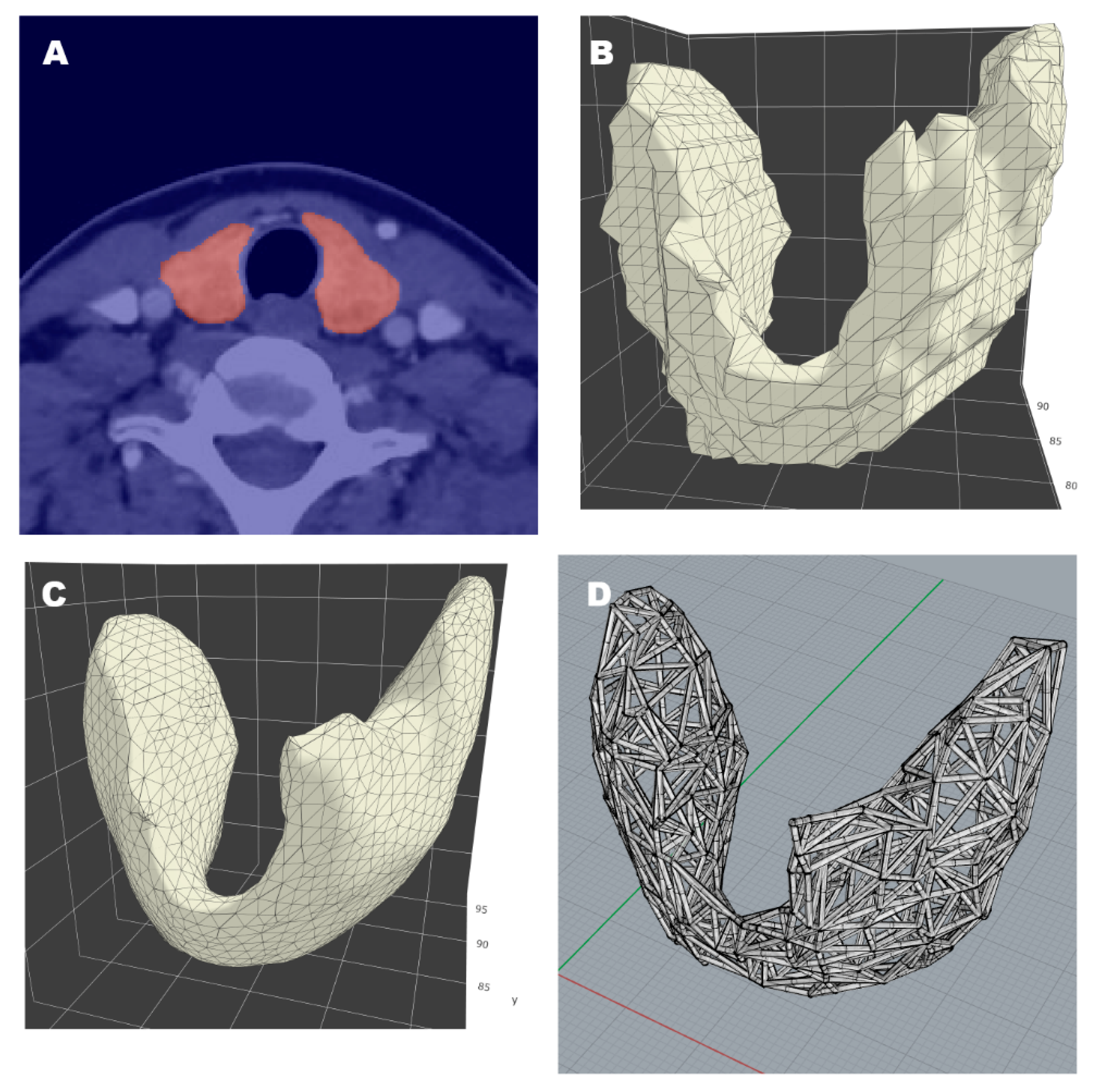
2.2. Personalized Mesh-Type 3D Modeling and Two-Color 3D Printing
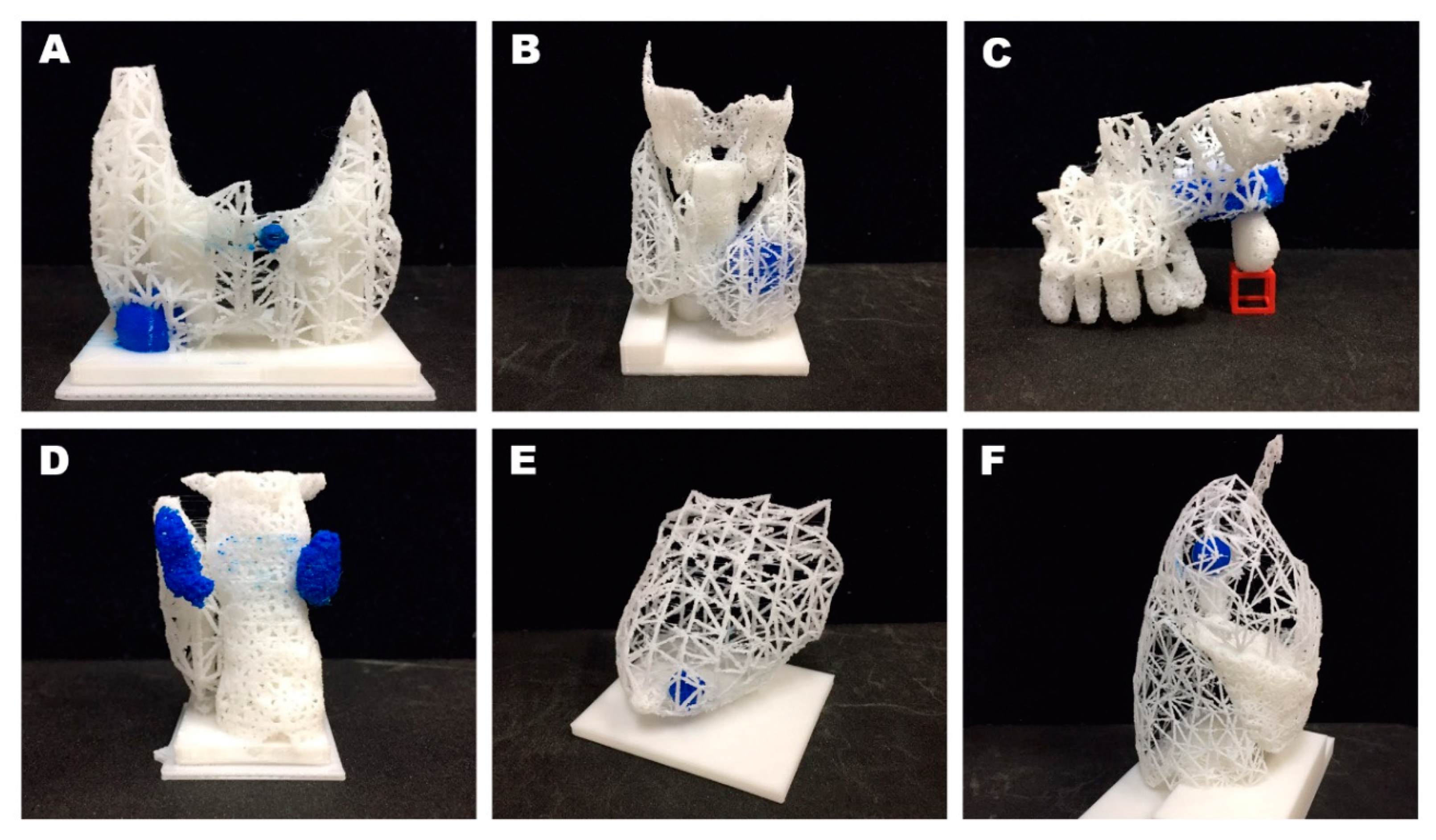
3. Results
4. Discussion and Conclusions
4.1. Discussion
4.2. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Hanson, M.; Pitt, D. Informed consent for surgery: Risk discussion and documentation. Can. J. Surg. 2017, 60, 69–70. [Google Scholar] [PubMed]
- Mishra, P.K.; Ozalp, F.; Gardner, R.S.; Arangannal, A.; Murday, A. Informed consent in cardiac surgery: Is it truly informed? J. Cardiovasc. Med. 2006, 7, 675–681. [Google Scholar] [CrossRef] [PubMed]
- Villanueva, C.; Talwar, A.; Doyle, M. Improving informed consent in cardiac surgery by enhancing preoperative education. Patient Educ. Couns. 2018, 101, 2047–2053. [Google Scholar] [CrossRef] [PubMed]
- Tait, A.R.; Voepel-Lewis, T. Digital multimedia: A new approach for informed consent? JAMA 2015, 313, 463–464. [Google Scholar] [CrossRef] [PubMed]
- Rosenfeld, E.H.; Lopez, M.E.; Yangyang, R.Y.; Justus, C.A.; Borges, M.M.; Mathai, R.C.; Karediy, A.; Zhang, W.; Brandt, M.L. Use of standardized visual aids improves informed consent for appendectomy in children: A randomized control trial. Am. J. Surg. 2018, 216, 730–735. [Google Scholar] [CrossRef] [PubMed]
- Moseley, T.H.; Wiggins, M.N.; O’sullivan, P. Effects of presentation method on the understanding of informed consent. Br. J. Ophthalmol. 2006, 90, 990–993. [Google Scholar] [CrossRef] [PubMed]
- Bernhard, J.C.; Isotani, S.; Matsugasumi, T.; Duddalwar, V.; Hung, A.J.; Suer, E.; Baco, E.; Satkunasivam, R.; Djaladat, H.; Metcalfe, C.; et al. Personalized 3D printed model of kidney and tumor anatomy: A useful tool for patient education. World J. Urol. 2016, 34, 337–345. [Google Scholar] [CrossRef] [PubMed]
- Yoon, S.H.; Park, S.; Kang, C.H.; Park, I.K.; Goo, J.M.; Kim, Y.T. Personalized 3D-Printed Model for Informed Consent for Stage I Lung Cancer: A Randomized Pilot Trial. Semin. Thorac. Cardiovasc. Surg. 2019, 31, 316–318. [Google Scholar] [CrossRef] [PubMed]
- Zhuang, Y.; Zhou, M.; Liu, S.; Wu, J.; Wang, R.; Chen, C. Effectiveness of personalized 3D printed models for patient education in degenerative lumbar disease. Patient Educ. Couns. 2019, 102, 1875–1881. [Google Scholar] [CrossRef] [PubMed]
- Tack, P.; Victor, J.; Gemmel, P.; Annemans, L. 3D-printing techniques in a medical setting: A systematic literature review. Biomed. Eng. Online 2016, 15, 115. [Google Scholar] [CrossRef] [PubMed]
- Yan, Q.; Dong, H.; Su, J.; Han, J.; Song, B.; Wei, Q.; Shi, Y. A Review of 3D Printing Technology for Medical Applications. Engineering 2018, 4, 729–742. [Google Scholar] [CrossRef]
- Hesamian, M.H.; Jia, W.; He, X.; Kennedy, P. Deep learning techniques for medical image segmentation: Achievements and challenges. J. Digit. Imaging 2019, 32, 582–596. [Google Scholar] [CrossRef] [PubMed]
- Dawson-Haggerty, S. Trimesh [Internet]. Available online: https://trimsh.org/ (accessed on 1 March 2020).
- Lidz, C.W. The therapeutic misconception and our models of competency and informed consent. Behav. Sci. Law 2006, 24, 535–546. [Google Scholar] [CrossRef] [PubMed]
- Garcia, J.; Yang, Z.L.; Mongrain, R.; Leask, R.L.; Lachapelle, K. 3D printing materials and their use in medical education: A review of current technology and trends for the future. BMJ Simul. Technol. Enhanc. Learn. 2018, 4, 27–40. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
| Model | Dimensions (cm) | Relation to Actual Size | Printing Time | Post-Processing Time (min) | Cost |
|---|---|---|---|---|---|
| Thyroid tumor | 5.3 × 3.0 × 6.5 | 1 | 2 h 50 min | 10 | $2.72 |
| Thyroid gland and adjacent cartilage | 5.5 × 4.3 × 9.3 | 1 | 9 h 15 min | 10 | $8.69 |
| Maxillary tumor | 7.1 × 5.7 × 4.7 | 1 | 9 h 4 min | 15 | $8.24 |
| Parathyroid adenoma | 4.0 × 3.1 × 5.5 | 1 | 5 h 3 min | 10 | $3.71 |
| Breast tumor | 6.2 × 5.2 × 5.9 | ½ | 6 h 41 min | 5 | $7.78 |
| Lung nodule | 6.8 × 8.0 × 13.5 | ½ | 23 h 4 min | 40 | $33.67 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Seok, J.; Yoon, S.; Ryu, C.H.; Ryu, J.; Kim, S.-k.; Jung, Y.-S. Mesh-Type Three-Dimensional (3D) Printing of Human Organs and Tumors: Fast, Cost-Effective, and Personalized Anatomic Modeling of Patient-Oriented Visual Aids. Appl. Sci. 2021, 11, 1047. https://doi.org/10.3390/app11031047
Seok J, Yoon S, Ryu CH, Ryu J, Kim S-k, Jung Y-S. Mesh-Type Three-Dimensional (3D) Printing of Human Organs and Tumors: Fast, Cost-Effective, and Personalized Anatomic Modeling of Patient-Oriented Visual Aids. Applied Sciences. 2021; 11(3):1047. https://doi.org/10.3390/app11031047
Chicago/Turabian StyleSeok, Jungirl, Sungmin Yoon, Chang Hwan Ryu, Junsun Ryu, Seok-ki Kim, and Yuh-Seog Jung. 2021. "Mesh-Type Three-Dimensional (3D) Printing of Human Organs and Tumors: Fast, Cost-Effective, and Personalized Anatomic Modeling of Patient-Oriented Visual Aids" Applied Sciences 11, no. 3: 1047. https://doi.org/10.3390/app11031047
APA StyleSeok, J., Yoon, S., Ryu, C. H., Ryu, J., Kim, S.-k., & Jung, Y.-S. (2021). Mesh-Type Three-Dimensional (3D) Printing of Human Organs and Tumors: Fast, Cost-Effective, and Personalized Anatomic Modeling of Patient-Oriented Visual Aids. Applied Sciences, 11(3), 1047. https://doi.org/10.3390/app11031047