
Creating a Diagnostic Assistance System for Diseases in Kampo Medicine


Abstract
1. Introduction
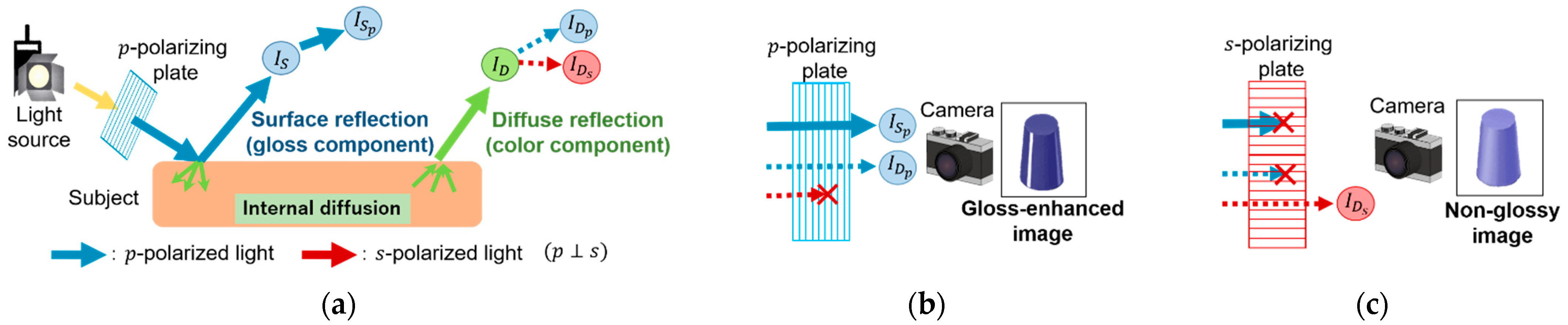
- We proposed a tongue imaging method using a polarized light camera that is simpler and more effective than the conventional method. In particular, the use of polarized light cameras provided accurate gloss information and showed their effectiveness in diagnosing yin deficiency and fluid stagnation, conditions closely related to fluid content, as shown in Section 2
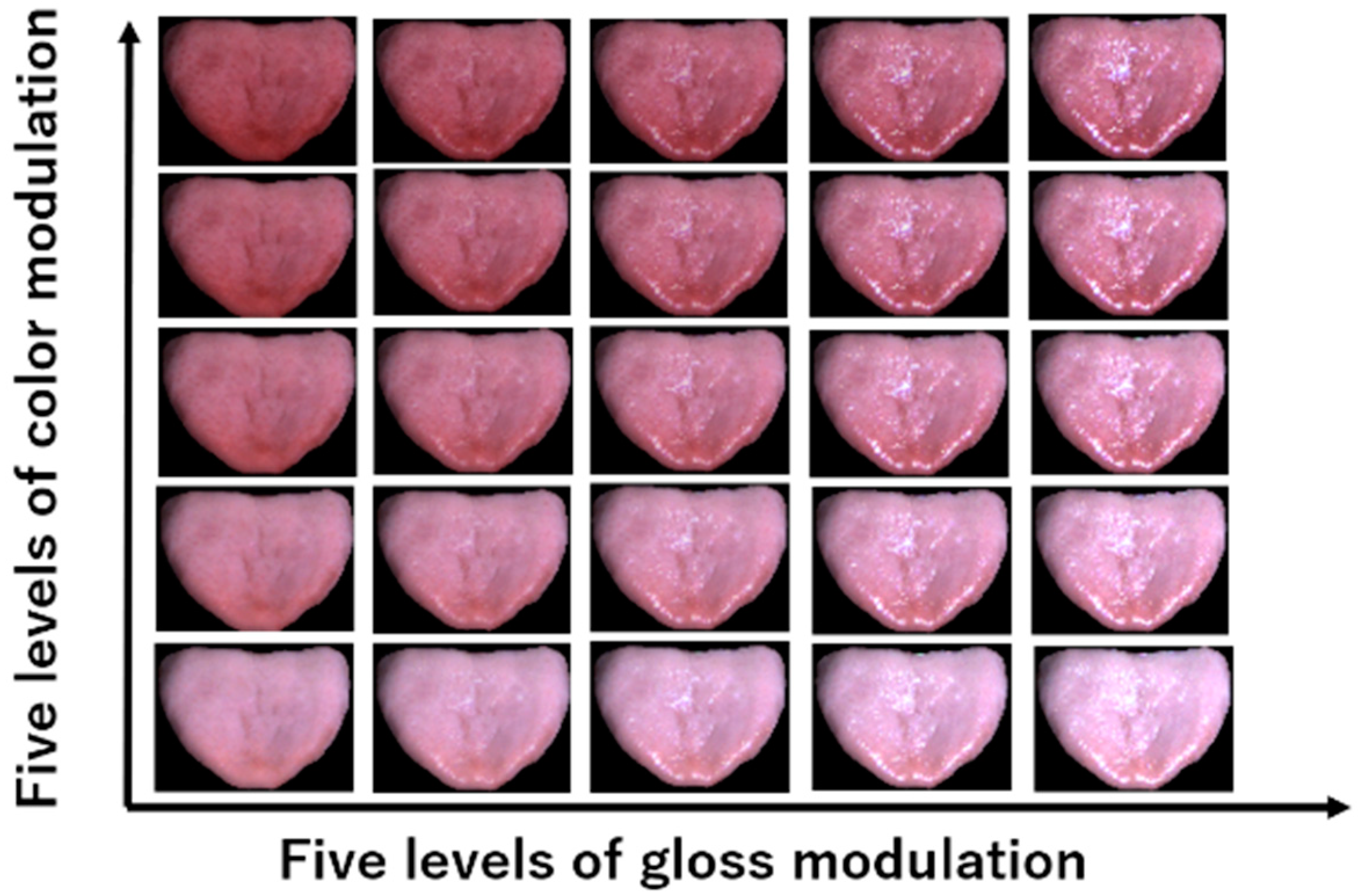
- We proposed a physiologically compensated and effective data augmentation method. We show that the proposed data augmentation method improved the distribution of correct values in Section 4. In addition, the estimation accuracy was improved by the data augmentation. These results indicate the effectiveness of our method.
2. Materials and Methods
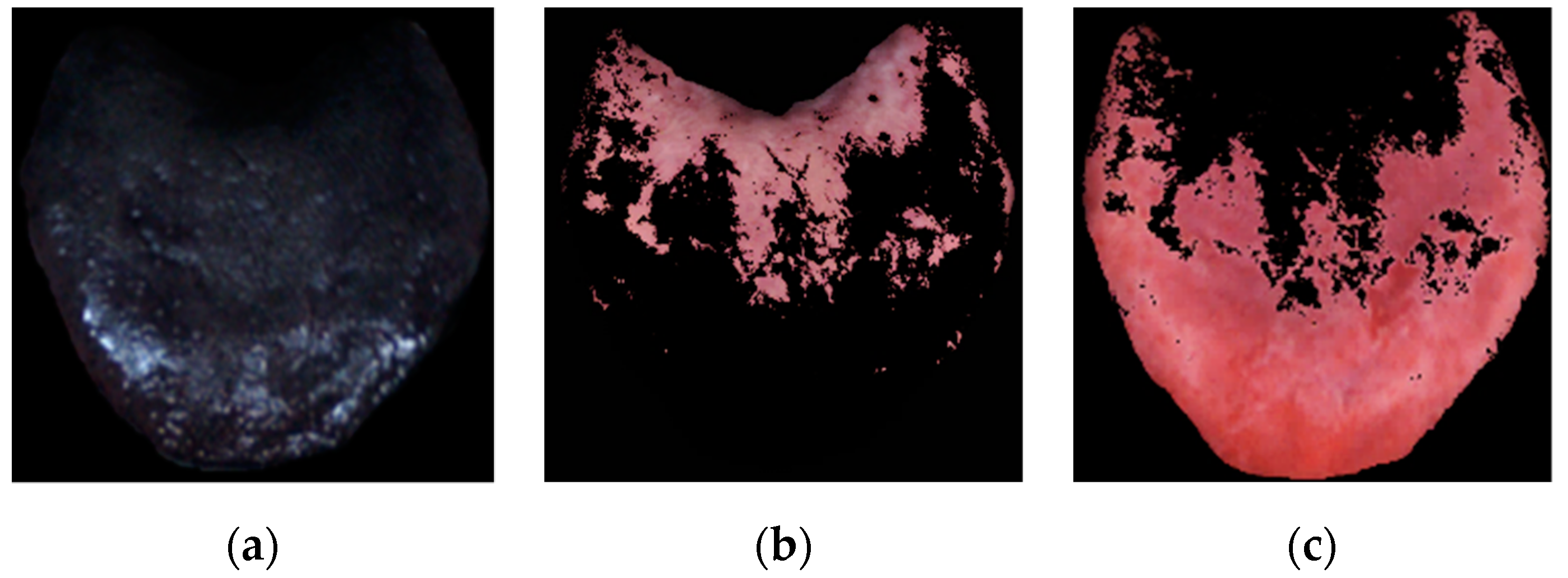
2.1. Capturing Glossy and Non-Glossy Images Using Polarized Light
2.2. Separating the Tongue Coating from the Tongue Body
2.3. Extracting Feature Values from Tongue Images
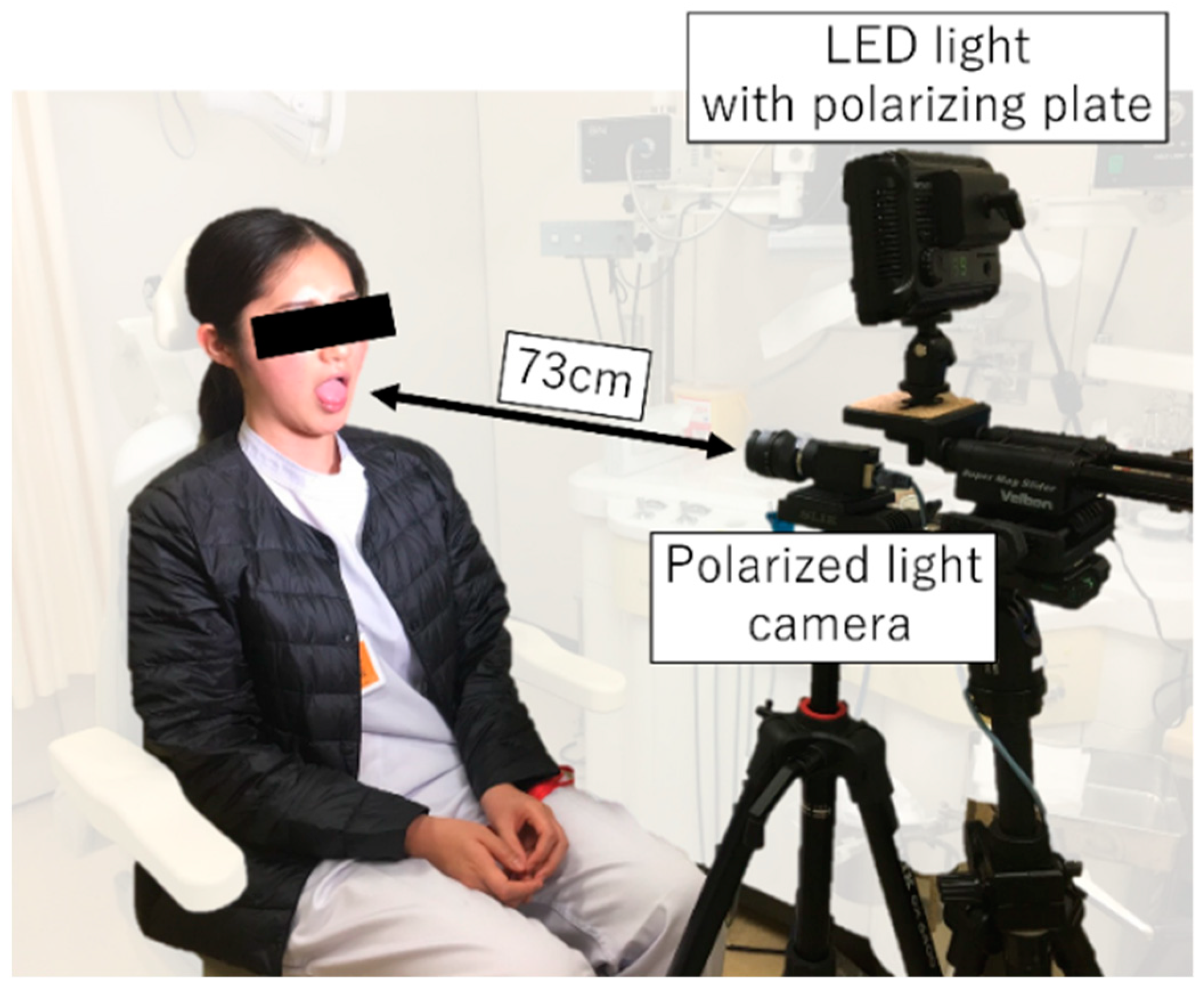
2.4. Set-Up for Capturing Tongue Images
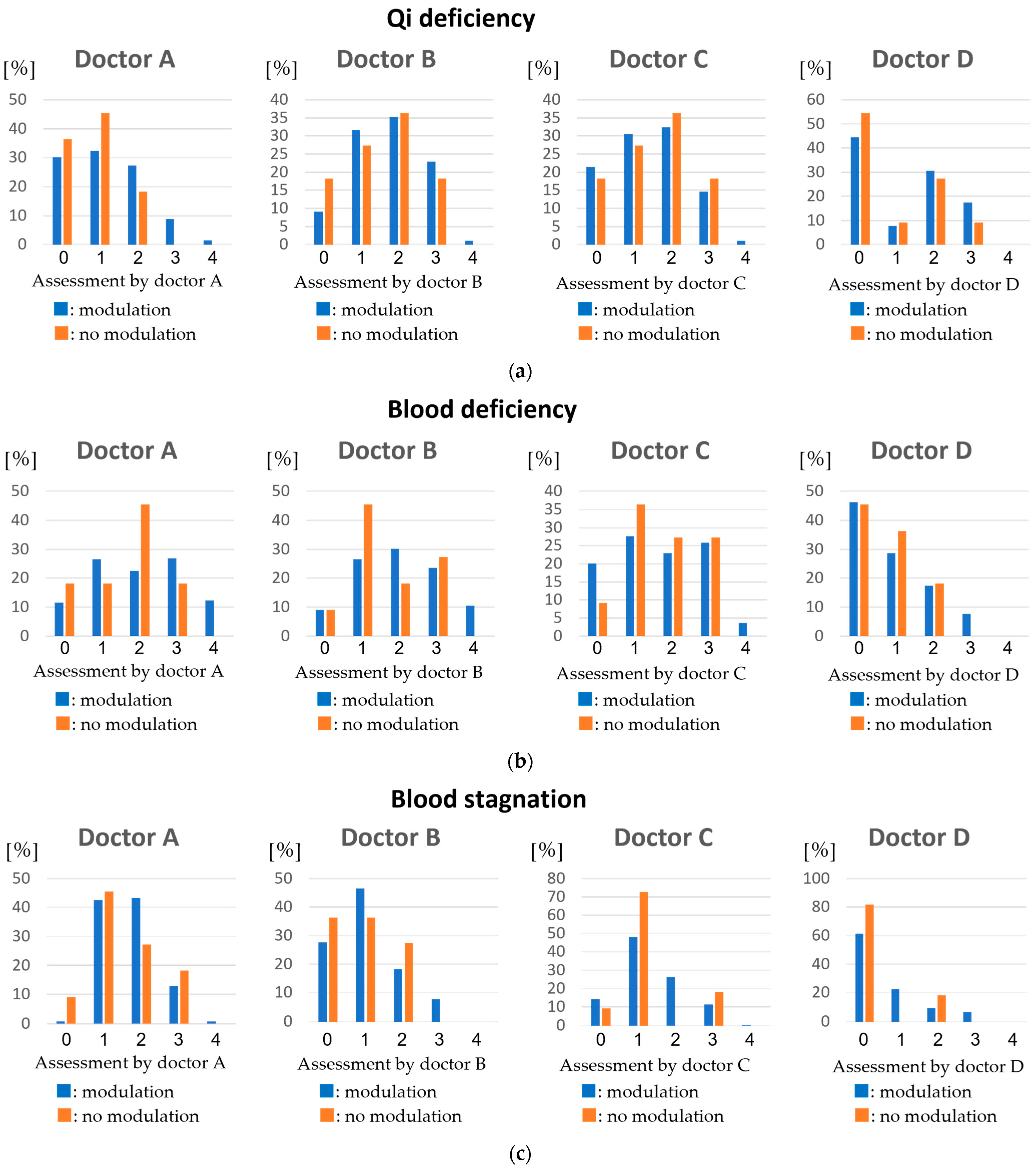
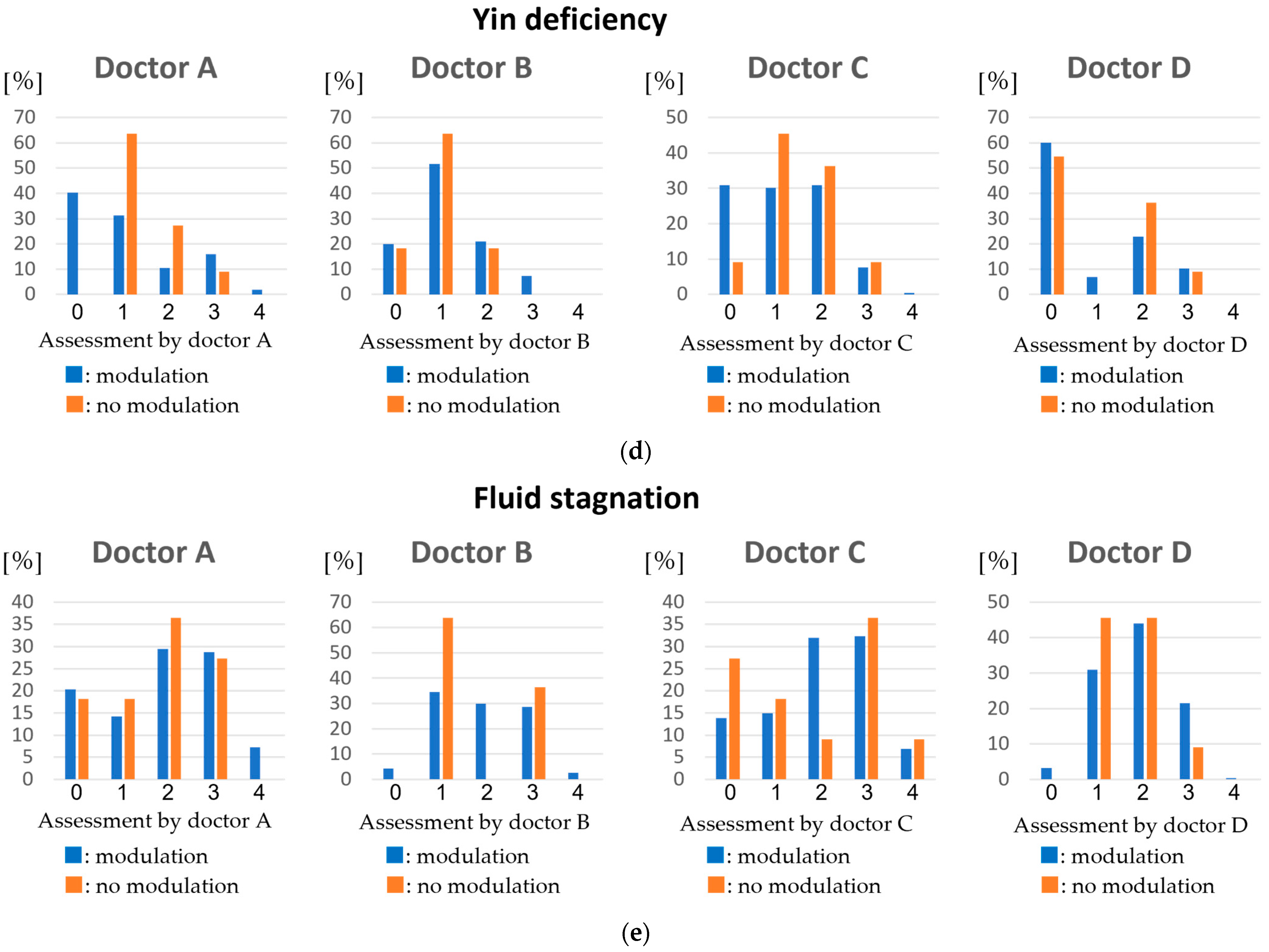
2.5. Data Augmentation by Color and Gloss Modulation
2.6. Subjective Evaluation of Diseases by Kampo Doctors Using Tongue Images
2.7. Feature Selection from 27 Features
3. Results
4. Discussion
- Some modulated data for data augmentation were not naturally observed tongue data.
- A polarization camera is required instead of a regular camera.
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Sato, Y. Introduction to Kampo: Japanese Traditional Medicine; The Japan Society for Oriental Medicine: Tokyo, Japan, 2005. [Google Scholar]
- Mitani, K. The lecture for the diagnosis of Kampo medicine: Boshin, especially for the diagnosis of tongue. Kampo Med. 2007, 58, 673–685. [Google Scholar] [CrossRef][Green Version]
- Satoh, H. An introduction to Kampo medicine. Folia Pharmacol. Jpn. 2008, 132, 260–264. [Google Scholar] [CrossRef] [PubMed]
- Yamamoto, S.; Ishilawa, Y.; Nakaguchi, T.; Ogawa-Ochiai, K.; Tsumura, N.; Kasahara, Y.; Namiki, T.; Miyake, Y. Temporal Changes in Tongue Color as Criterion for Tongue Diagnosis in Kampo Medicine. Forsch. Komplementmed. 2012, 19, 80–85. [Google Scholar] [CrossRef] [PubMed]
- Wang, Y.; Zhou, Y.; Yang, J.; Xu, Q. An image analysis system for tongue diagnosis in traditional Chinese medicine. Comput. Inf. Sci. 2005, 3314, 1181–1186. [Google Scholar]
- Matsushita, F.; Kiyomitsu, K.; Ogawa, K.; Tsumura, N. Evaluation of Kampo disease states using facial images. Artif. Life Robot. 2019, 24, 44–51. [Google Scholar] [CrossRef]
- Zhang, J.; Xu, J.; Hu, X.; Chen, Q.; Tu, L.; Huang, J.; Cui, J. Diagnostic method of diabetes based on support vector machine and tongue images. BioMed Res. Int. 2017, 2017, 7961494. [Google Scholar] [CrossRef] [PubMed]
- Kainuma, M.; Furusyo, N.; Urita, Y.; Ikezaki, H.; Ura, K.; Nakaguchi, T.; Namiki, T. Objective tongue color and gastroesophageal reflux disease: Cross-sectional study. Tradit. Kampo Med. 2019, 6, 19–25. [Google Scholar] [CrossRef]
- Nakaguchi, T.; Ishilawa, Y.; Oji, T.; Yamamoto, S.; Tsumura, N.; Ueda, K.; Nagamine, K.; Namiki, T.; Miyake, Y. Proposal for a new noncontact method for measuring tongue moisture to assist in tongue diagnosis and development of the tongue image analyzing system, which can separately record the gloss components of the tongue. BioMed Res. Int. 2015, 2015, 249609. [Google Scholar] [CrossRef] [PubMed]
- Danser, M.M.; Mantilla Gomez, S.; Van der Weijden, G.A. Tongue coating and tongue brushing: A literature review. Int. J. Dent. Hyg. 2003, 1, 151–158. [Google Scholar] [CrossRef] [PubMed]
- Xu, J.; Tu, L.; Zhang, Z.; Zhou, C. The region partition of quality and coating for tongue image based on color image segmentation method. In Proceedings of the 2008 IEEE International Symposium on IT in Medicine and Education, Xiamen, China, 12–14 December 2008; pp. 817–821. [Google Scholar]
- Tsumura, N.; Ojima, N.; Sato, K.; Shiraishi, M.; Shimizu, H. Image-based skin color and quality analysis/synthesis by extracting hemoglobin and melanin information in the skin. ACM Trans. Graph. 2003, 22, 770–779. [Google Scholar] [CrossRef]
- Burges, C.J. A Tutorial on support vector machines for pattern recognition. Data Min. Knowl. Discov. 1998, 2, 121–167. [Google Scholar] [CrossRef]
- Leslie, K.P. An Introduction to Variable and Feature Selection. J. Mach. Learn. Res. 1998, 3, 1157–1182. [Google Scholar]
- Pianykh, O.S.; Langs, G.; Dewey, M.; Enzmann, D.R.; Herold, C.J.; Schoenberg, S.O.; Brink, J.A. A tutorial on support vector machines for pattern recognition. Radiology 2020, 297, 6–14. [Google Scholar]









{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Qi | Blood | Fluid | |
|---|---|---|---|
| Deficiency | Tongue | Face Tongue | Face Tongue |
| Stagnation | Face Tongue | Tongue |
| From Glossy Image | From Tongue Coating | From Tongue Body |
|---|---|---|
| Mean of gloss | Mean of coating | Mean of body |
| Max of gloss | Max of coating | Max of body |
| Min of gloss | Min of coating | Min of body |
| Median of gloss | Median of coating | Median of body |
| Std of gloss | Std of coating | Std of body |
| Gross area | Coating area |
| Diseases | ||||
|---|---|---|---|---|
| Qi Deficiency | Blood Deficiency | Blood Stagnation | Yin Deficiency | Fluid Stagnation |
| Median of body Max of gloss | Mean of body Median of body Max of gloss | Mean of body | Std of gloss Mean of gloss Min of gloss | Min of body Min of gloss Max of gloss Median of gloss |
| Diseases | |||||
|---|---|---|---|---|---|
| Qi Deficiency | Blood Deficiency | Blood Stagnation | Yin Deficiency | Fluid Stagnation | |
| Using all features | 0.51 | 0.52 | 0.49 | 0.50 | 0.60 |
| Using selected features | 0.44 | 0.42 | 0.33 | 0.36 | 0.55 |
| Diseases | ||||||
|---|---|---|---|---|---|---|
| Qi deficiency | Blood Deficiency | Blood Stagnation | Yin Deficiency | Fluid Stagnation | ||
| Doctor.A | no modu. | 0.94 | 0.75 | 0.91 | 1.00 | 0.62 |
| modu. | 0.64 | 0.71 | 0.62 | 0.55 | 0.77 | |
| Doctor.B | no modu. | 0.99 | 0.90 | 0.80 | 0.85 | 0.84 |
| modu. | 0.70 | 0.73 | 0.55 | 0.57 | 0.75 | |
| Doctor.C | no modu. | 1.01 | 0.93 | 0.82 | 0.94 | 0.73 |
| modu. | 0.84 | 0.99 | 0.64 | 0.81 | 0.90 | |
| Doctor.D | no modu. | 0.95 | 0.76 | 0.62 | 0.91 | 0.65 |
| modu. | 0.83 | 0.71 | 0.60 | 0.86 | 0.56 | |
| Average of all doctors | no modu. | 0.59 | 0.61 | 0.53 | 0.58 | 0.68 |
| modu. | 0.44 | 0.42 | 0.33 | 0.36 | 0.55 | |
| Diseases | ||||||
|---|---|---|---|---|---|---|
| Qi Deficiency | Blood Deficiency | Blood Stagnation | Yin Deficiency | Fluid Stagnation | ||
| Average of all doctors | no modu. | 0.71 | 0.73 | 0.62 | 0.67 | 0.77 |
| modu. | 0.53 | 0.50 | 0.41 | 0.43 | 0.56 | |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Koike, R.; Ogawa-Ochiai, K.; Shirai, A.; Hayashi, K.; Arimitsu, J.; Li, H.; Tsumura, N. Creating a Diagnostic Assistance System for Diseases in Kampo Medicine. Appl. Sci. 2021, 11, 9716. https://doi.org/10.3390/app11219716
Koike R, Ogawa-Ochiai K, Shirai A, Hayashi K, Arimitsu J, Li H, Tsumura N. Creating a Diagnostic Assistance System for Diseases in Kampo Medicine. Applied Sciences. 2021; 11(21):9716. https://doi.org/10.3390/app11219716
Chicago/Turabian StyleKoike, Reimei, Keiko Ogawa-Ochiai, Akiko Shirai, Katsumi Hayashi, Junsuke Arimitsu, Hongyang Li, and Norimichi Tsumura. 2021. "Creating a Diagnostic Assistance System for Diseases in Kampo Medicine" Applied Sciences 11, no. 21: 9716. https://doi.org/10.3390/app11219716
APA StyleKoike, R., Ogawa-Ochiai, K., Shirai, A., Hayashi, K., Arimitsu, J., Li, H., & Tsumura, N. (2021). Creating a Diagnostic Assistance System for Diseases in Kampo Medicine. Applied Sciences, 11(21), 9716. https://doi.org/10.3390/app11219716