1. Introduction
The third molar is the most commonly impacted tooth. Several causes can lead to impaction of the mandibular third molars. Eruption can be interfered by local physical barriers such as adjacent teeth, dense bones, excessive soft tissue, and lesions [
1]. The prevalence of impacted third molars has been reported in the range of 30.3% to 68.6% [
2,
3,
4,
5,
6]. The extraction of the mandibular third molar is one of the most common surgeries in oral and maxillofacial surgery [
7,
8]. Complications that can occur when extracting the mandibular third molar include damage to the adjacent teeth, swelling, bleeding, infection, and nerve damage. Among the potential complications associated with removal of the third molar, inferior alveolar nerve (IAN) injury is a representative complication. Several studies have reported an incidence of IAN injury of 0.26–8.4% [
9,
10,
11,
12,
13,
14,
15]. Various factors such as the age of the patient, the experience of the surgeon, and the extent and location of the impaction are discussed as the risk factors of the nerve injury [
15,
16,
17].
The most important risk factor for IAN injury is the correlation between the anatomical position of the third molar and the proximity of the IAN [
12,
18]. Panoramic radiographs are widely used for initial examination to assess the third molar. However, it is not possible to accurately determine the buccal and lingual positioning of the third molar and nerves on a two-dimensional panoramic radiograph. Therefore, it is not easy to assess the possibility of nerve injury from panoramic radiographs [
19]. There have been many studies regarding the correlation between the mandibular third molar and the IAN, and the signs that can predict the possibility of IAN injury using a two-dimensional panoramic radiograph [
20]. Previous studies have reported a correlation between some panoramic signals and nerve injury, but the results are not unified [
21,
22,
23,
24,
25,
26,
27,
28,
29,
30]. In order to overcome the limitations of panoramic radiographs, the use of cone beam computed tomography (CBCT) has recently increased. CBCT is very useful for the evaluation of impacted mandibular third molars [
31] and the proximity of the IAN, and to improve the risk assessment prior to surgery [
32].
Panoramic signals of IAN contacts have shown frequently, however, the occurrence of IAN injury is rare and it is very hard to predict nerve injury. The purpose of this study was to analyze the incidence and risk factors of possible IAN injury after extraction of the mandibular third molars. CBCT and panoramic radiography was used to evaluate the factors that may have affected inferior alveolar nerve injury.
4. Discussion
Extraction of the mandibular third molar is the most commonly performed surgical procedure in oral and maxillofacial surgery. IAN injury can cause a lot of discomfort to the patient and lower the quality of life [
35]. However, there are still not many studies on the relationship between the inferior alveolar nerve and mandibular third molars in populations.
This study was to evaluate the pattern of mandibular third molar impaction in Korea and to evaluate the risk factors of inferior alveolar nerve damage that may occur during extraction. Prevalence of third molar impaction is reported to range from 30.3% to 68.6% [
2,
3,
4,
5,
6]. The prevalence of impaction could not be determined in this study as it was intended for patients with impacted mandibular third molars. The gender difference regarding the impacted mandibular third molar varied from study to study. Previous studies showed that women have a higher prevalence of impaction [
6,
36] and another study showed that men have a higher prevalence of impaction [
37]. Impaction of the third molar was 52.1% in men, and the average age was 33.5 years. Patients 10 to 39 years old accounted for 88.4% of this study.
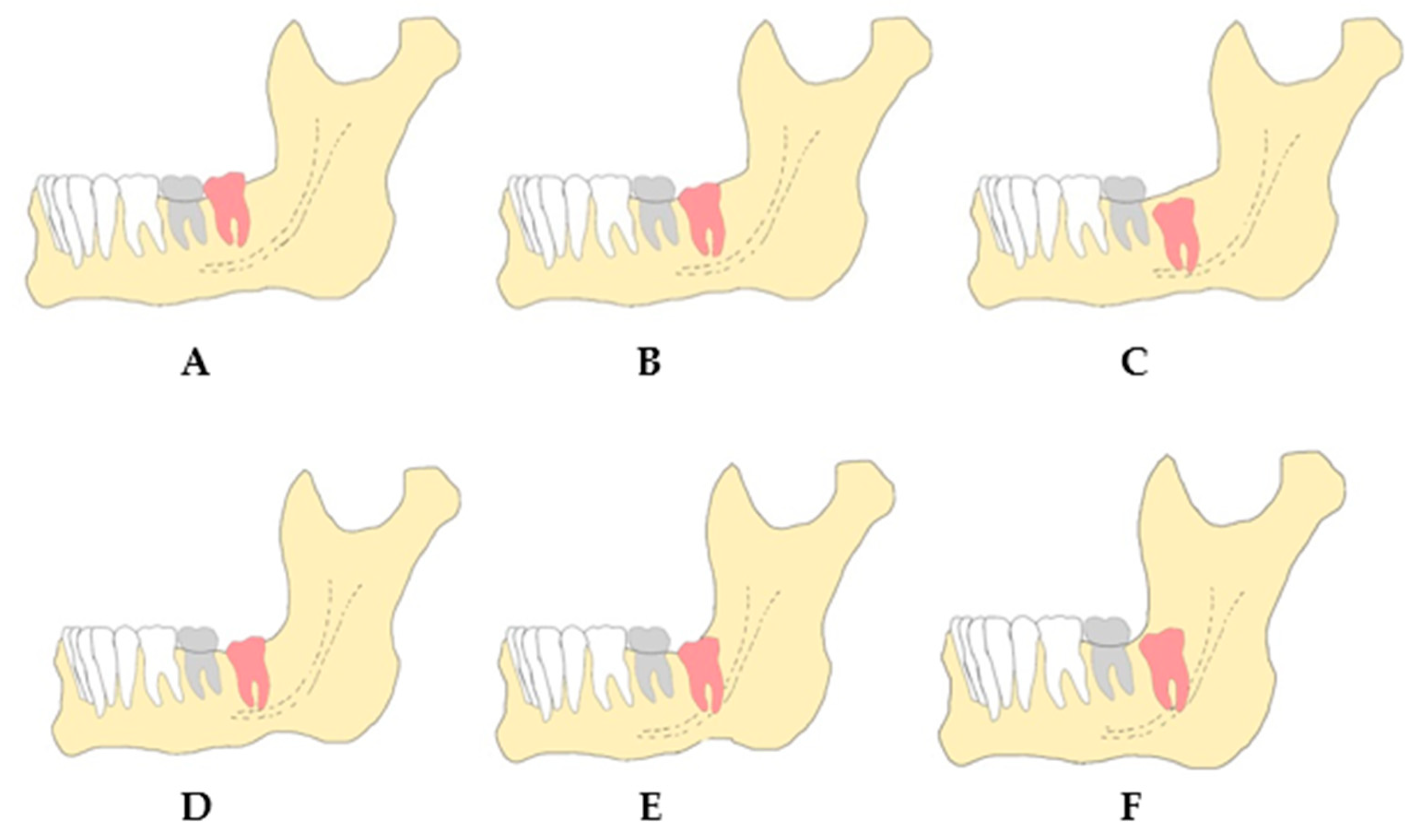
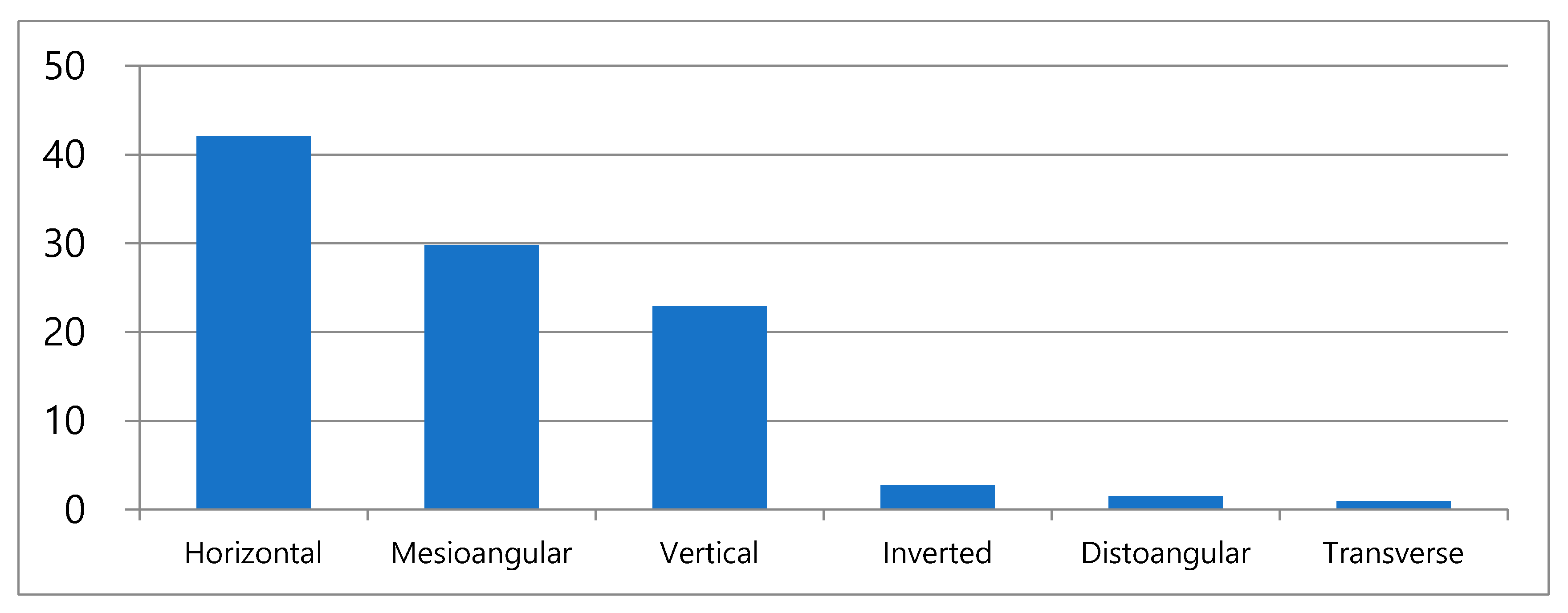
The impaction pattern was varied according to the angulation. Most of studies showed that mesial angulation [
6,
38,
39,
40,
41] and vertical impaction [
42,
43] occur frequently. In this study, horizontal angulation was most popular. CBCT is taken when there is a suspicion of contact between the IAN and the mandibular third molar in panoramic radiographs, or when the third molars are completely impacted. Since the subject of this study was patients who underwent CBCT, this might have affected the outcome as patients with a mandibular third molar impacted by a vertical or a mesial impaction, which is relatively far from the IAN, were not included.
According to the Pell and Gregory classification, the most prevalent was Class IIA (30.0%), followed by Class IIB (19.3%). This is consistent with previous results [
1,
14,
44]. Monaco [
45] reported that Class A (56.2%) and Class II (63%) were the most common among Italians, and Blondeau [
46] and Almendros-Marques [
43] reported that Class IIB was the most common. It can be seen that Koreans do not differ in the degree and distribution of impaction from different races. In addition, it was found that the depth of the impaction increased as age increased. This suggests that patients with low impacted mandibular third molars remove their teeth at a relatively young age, so as the age increases, deep impacted mandibular third molars, which are difficult to extract, are present at a higher rate.
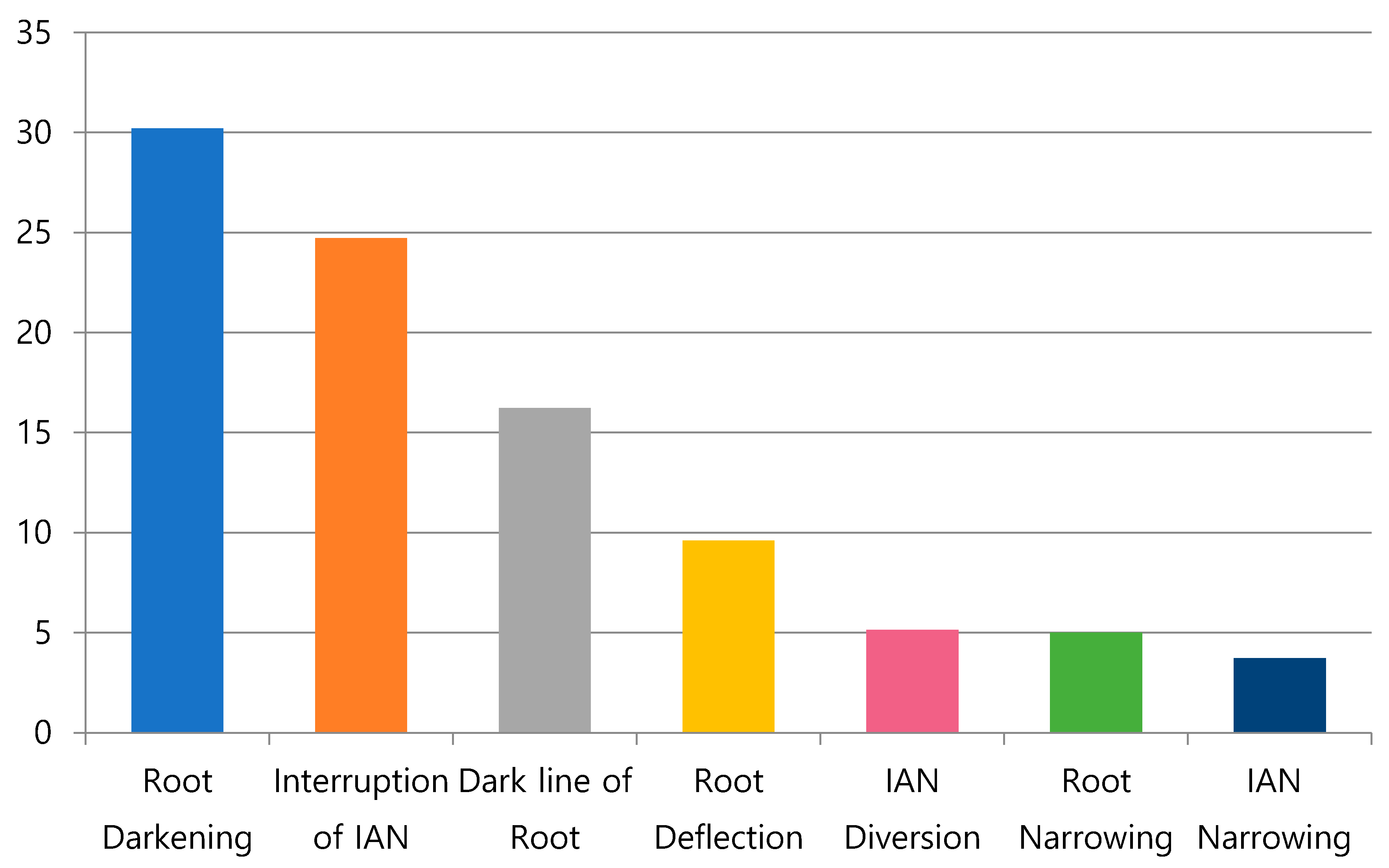
Panoramic radiographic signs were reported to occur at a low frequency of 0.1%~3.3% in the study by Rood and Shehab [
20]. Sedaghatfar et al. [
11] reported the occurrence at a rate of 11.8–35.9%, similar to this study. This difference is thought to be due to the difference between observers in determining the symptoms, as the evaluation of the signs in the panoramic radiograph is not standardized. In addition, the subjects of this study had panoramic radiographs of the mandibular third molar and inferior alveolar nerves that were in contact with each other, so it is thought that the incidence of signs was higher than that of a completely randomized study.
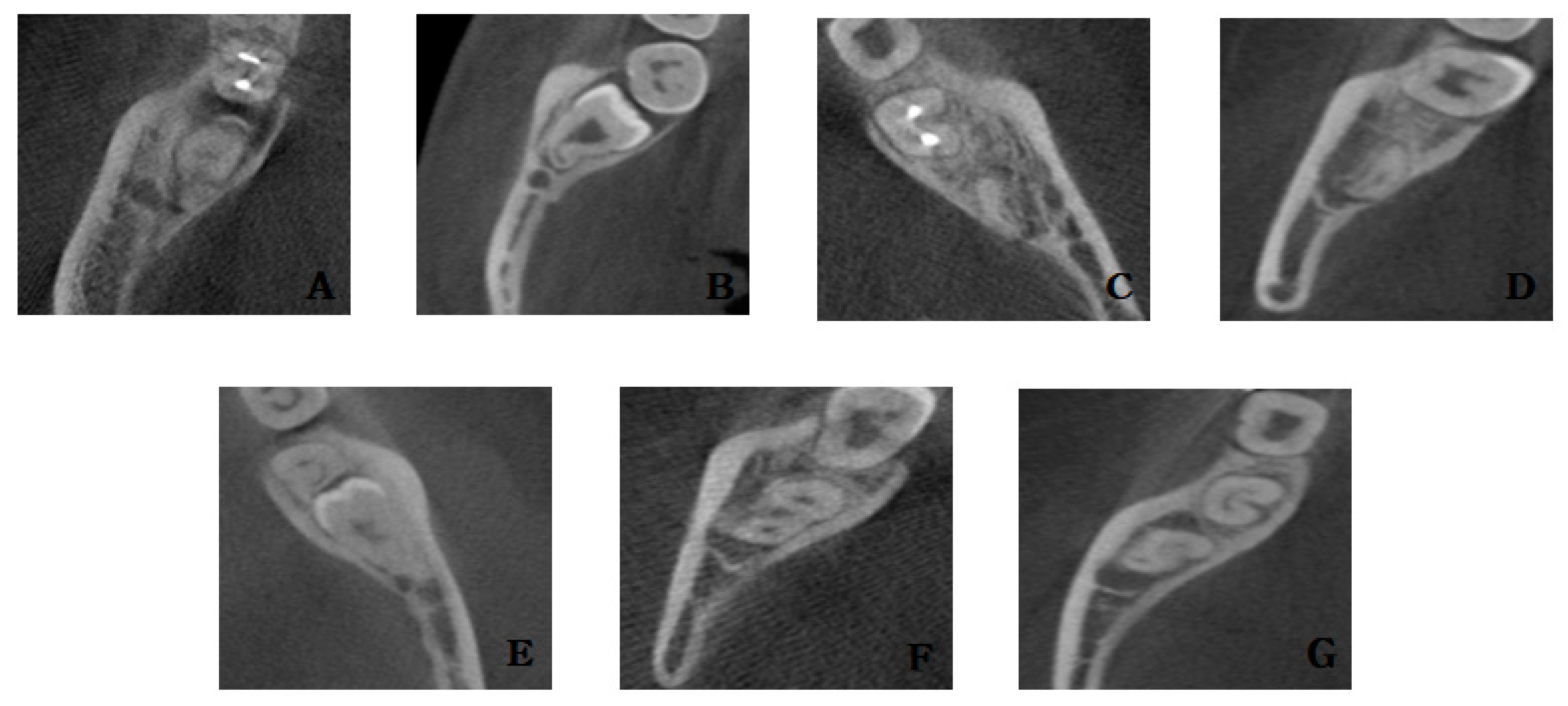
In CBCT, the contact between the mandibular third molar and the inferior alveolar nerve was observed in 61%, which was less than the cases with contact on the panoramic radiograph (88.67%). This means that it was not possible to accurately determine whether the mandibular third molar and the inferior alveolar nerve were actually in contact with the panoramic radiograph. There was a significant correlation between the Pell and Gregory classification, the contact between the mandibular third molar and the IAN in CBCT, and the narrowing of the IAN in CBCT. This means that the deeper the degree of impaction of the mandibular third molar, the closer it was to the IAN. As for the signs on the panoramic radiograph, there was a correlation between the actual contact between the mandibular third molar and the IAN in CBCT, except when the root was narrowed and there was a dark line at the root apex [
47,
48,
49].
There was a correlation between the disappearance of the continuity of the lingual cortical bone at the root of the mandibular third molar and the dark line at the root apex. Dark lines were observed in 55.7% of cases with lingual cortical bone perforation, and were absent in 44.3% of cases with lingual cortical bone perforation. In the literature examining the dark area of the root and lingual cortical bone perforation, it was suggested that the dark area showed proximity to the IAN rather than the lingual cortical bone perforation [
50]. It is believed that this is caused by not distinguishing from dark lines when irradiating the dark area. If the root is in the lingual cortical bone, it is thought that the presence of the periodontal ligament in the dense cortical bone and the perforated area of the cortical bone appear as dark lines. The possibility of root fracture occurring during extraction increases, and the fractured root may fall into the submandibular space, so care should be taken during extraction. It would be useful if we could predict the existence of roots in the lingual cortical bone only with panoramic radiographs, not CBCT.
In the case of proximal dental caries 46.9% had mesial impaction and 36.4% had horizontal impaction. This is consistent with other studies that stated that the mesial and horizontal impaction of the third molar accounts for most of the proximal caries of the second molar [
51,
52]. In addition, when examining the relationship between pericoronitis and impaction angulation in various studies, it was reported that vertical impaction was the most common, followed by mesial impaction, and bone loss was most observed in mesial impaction [
53,
54]. In this study, horizontal impaction was the most common (39.4%), followed by vertical impaction (25.0%) and mesial impaction (23.2%). Out of 158 distal impactions, 38 cases had pericoronitis, showing a high morbidity rate of about 24%.
The incidence of IAN injury was 0.637%, which is similar to or lower than that reported in other studies [
9,
10,
11,
12,
13,
14,
15]. Of the 30 patients with IAN injury, there was a statistically significant correlation with gender (
p = 0.038), with risk of nerve damage being higher in women than men. Other studies reported that there was no correlation between gender and nerve injury [
31], but many studies have reported that women have a higher risk of nerve injury [
23,
24,
55]. In addition, there was a significant correlation between age and IAN injury. It can be seen that the possibility IAN injury increases with age. There was also literature reporting that the age and risk of nerve injury were not correlated [
55,
56]. However, many studies have shown that the risk of IAN injury increases in those over 25 years of age, and age is a risk factor for nerve injury [
15,
23,
57,
58,
59,
60,
61]. Age-related changes such as a decrease in bone elasticity, an increase in the occurrence of hypercementosis, and an increase in the amount of bone removal are thought to be the major causes of the increase in the difficulty of surgery. There are studies suggesting a relationship between the depth of impaction and the incidence of IAN injury [
9,
13,
23,
30,
55,
56,
58,
60], and a study suggesting no relationship [
31]. In the present study, it was found that there is a relationship between the depth of impaction and the incidence of IAN injury. Naturally, the deeper the impaction depth, the closer it is to the inferior alveolar nerve, and therefore, the probability of nerve injury is thought to increase. No significant correlation was found between the signs of panoramic radiographs and the incidence of IAN injury. This result is similar to most studies [
9,
11,
20,
23,
26,
28,
31]. It is considered that the prediction of IAN injury is inadequate, as a panoramic radiograph sign has low sensitivity and high specificity. In this study, among 30 patients with IAN injury, 24 showed that the IAN was driven to the lingual side of the mandibular third molar root in CBCT, and at the same time, a narrowing of the IAN was observed. When these two features are observed at the same time, it can be said that the incidence of IAN injury increases. The narrowed IAN in CBCT and the lingual pathway of the IAN is consistent with other studies that suggested increased risk of IAN injury [
27,
32,
62,
63]. The narrowing of the IAN canal means that the distance between the root of the mandibular third molar and the IAN canal is less. Clinically, when the mandibular third molar is extracted, most of the instrumentation is performed on the buccal side. Because of this, there are many cases where the tooth comes out while applying force in the lingual direction. Due to this effect, it is thought that the lingual movement and narrowing of the IAN cause IAN injury during extraction. This is thought to be a good factor in predicting the occurrence of nerve injury.
This study examined the impaction pattern and the risk factors affecting injury to the IAN in Koreans. The study had several limitations. First, it cannot be concluded that the study reflects the overall characteristics of Koreans, as it was short-term research by a single institution. Second, the study only included patients who underwent panoramic radiography and CBCT, instead of using random target collection. Unlike other studies, this study was intended for patients with impacted mandibular third molars and also for patients who underwent CBCT, following a suspicion of an impacted third mandibular molar being in contact with the inferior alveolar nerve. For this reason, there are limitations to consider when interpreting the results; therefore, the study cannot be generalized to the Korean population with impacted third mandibular molars. Third, the symptoms of patients with an IAN injury could not be described in detail due to the incomplete medical records and the loss of follow-up. As in other studies, it is necessary to classify the symptoms of temporary and permanent nerve injury and investigate the intensity of the symptoms.
The data and results of this study can be used to set the direction of future research. With more complementary studies, we can set the criteria for classification of the mandibular third molar in Koreans, analyze the third molar conveniently and quickly using artificial intelligence, and further create programs that can determine the degree of difficulty in the extraction, the possibility of injury to the IAN, and the possibility of complications.













{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}