1. Introduction
The World Health Organization (WHO) estimates that around 50 million people have dementia, with nearly 10 million new cases every year [
1]. Dementia refers to deterioration of cognitive function in the elderly. This syndrome affects memory, thinking, orientation, comprehension, calculations, learning capacity, language, and judgment. It also affects individual quality of life and is a financial burden for families due to expensive costs for healthcare [
2]. According to the Alzheimer’s association (2019), 36% of people aged 85 or older have Alzheimer’s Disease (AD) [
3]. Dementia and other cognitive impairment diseases have become an important global issue, as the number of elderly people is increasing. In 2025, it is predicted that Taiwan will become a super-aged society (National Development Council in Taiwan, 2016). As age increases, problems in cognitive abilities, such as divided attention, memory decline, etc., also increase [
4].
Simple reaction times are valid for measuring cognitive function in both patients and normal subjects [
5]. Furthermore, the authors in [
6] also noted that accuracy rate can correlate significantly with episodic memory performance and other cognitive functions. Reaction time and accuracy rate are thus related to cognitive functions [
5,
6,
7]. Most previous research used neuropsychological tests, such as the Flanker test, the Cambridge Neuropsychological Test Automated Battery, and Repeatable Battery for the Assessment of Neuropsychological Status [
6,
7]. Therefore, in this study, our main objective is to determine the difference in the reaction time and accuracy rate between the aforementioned three categories of subjects (normal subjects, Mild Cognitive Impairment (MCI), and dementia) using our own designed serious games. We intended to determine whether the response performance (also mentioned in [
7]) can differentiate between these three categories. A study by Phillips et al. [
8] found that patients with MCI and Alzheimer’s disease had significantly longer reaction times than normal aging control groups, with reaction times that did not eliminate individual differences. When the factors related to the different reaction times of individuals are excluded, patients with MCI actually behaved similarly to the normal aging control group, but the responses of patients with Alzheimer’s disease, after excluding the effects of individual differences, were still not as good as those of the other two groups.
Numerous methods have been developed to examine Alzheimer’s disease and MCI. Invasive methods are used to collect data from inside the human body and are not considered safe and comfortable for subjects [
9]. Valladares-Rodriguez et al. [
10] found that using noninvasive methods like serious games can detect the onset of MCI or Alzheimer’s disease. In our study, we applied the same method noninvasively by designing PC-based serious games to evaluate the reaction times and accuracy rates related to the cognitive abilities among normal subjects, MCI subjects, and dementia subjects. Our approach was to compare the results of the performance of an elder individual when playing the game using neuropsychological tests of cognitive function based on the MMSE (Mini Mental State Examination).
There are many neuropsychological tests and clinical questionnaires used to assess dementia levels among the elderly. Clinical questionnaires, such as the Mini Mental State Examination (MMSE) [
11] and the Montreal Cognitive Assessment (MoCA) [
12], are a popular way to evaluate cognitive abilities via clinical measurements. Costaz et al. [
13] used an Augmented Reality (AR) serious game called Smartkuber to perform cognitive screening among the elderly. To validate the relationship between game results and MoCa results, the authors used the Pearson correlation statistical method [
13,
14,
15]. In our research, we use the MMSE to evaluate the level of dementia among the elderly due to the heterogeneity of the age-group. A study was conducted by the authors of [
16] in Greece to validate the performance of the MMSE, and the result proved that an MMSE score of 23/24 is a credible test for diagnosis of dementia.
Several well-designed serious video games have been proposed and should be helpful for evaluating cognitive abilities [
10,
11,
17,
18,
19]. Fontana, E et al. [
19] developed a serious game called
TrainBrain, designed to improve concentration and to minimize the effects of the cognitive decline in attention for the elderly and children with ADHD (Attention Deficit Hyperactivity Disorder). In recent years, the products currently on the mainstream market for video and mobile games were designed for young people to experience exciting sight and sound stimulation, which may not be adaptable for the elderly. The development of a serious game is very challenging, especially when addressing dementia patients. Many factors must be considered, such as the needs of the subjects, human–computer interactions, emotions, comfortability, etc., which make development more complicated. A well-designed GUI (Graphical User Interface) is one of the most important aspects to help subjects focus on the game [
20]. In [
21], the authors built a whack-a-mole game for tablets (Android-based). The game was divided into different speeds, and the time was used to record the subject’s score and response time. The authors proved that this game can be used to assess some executive functions, especially those related to inhibition, in their recent study [
22]. They also suggested that this game can be developed for the elderly to assess other executive functions [
22,
23].
In this present study, two serious games were designed to meet the standards of play for the elderly. The purpose of our PC-based games was to measure response performance (reaction time and accuracy rate). Psychologists and clinicians were continuously consulted during system development to obtain a better understanding about the complexity of the external appearance of cognitive functions and the reactions of the elderly. Based on [
22], first, we built a similar whack-a-mole game without distractors (the objects in addition to the mole) to focus only on reaction time and accuracy rate when playing the game, as the game’s target is to collect information on the reaction time and accuracy rate of the subjects. Then, we designed the second game, hit-the-ball (with a distractor), also to assess judgment ability and to observe how the subjects distinguish between objects. Another issue, as explained in [
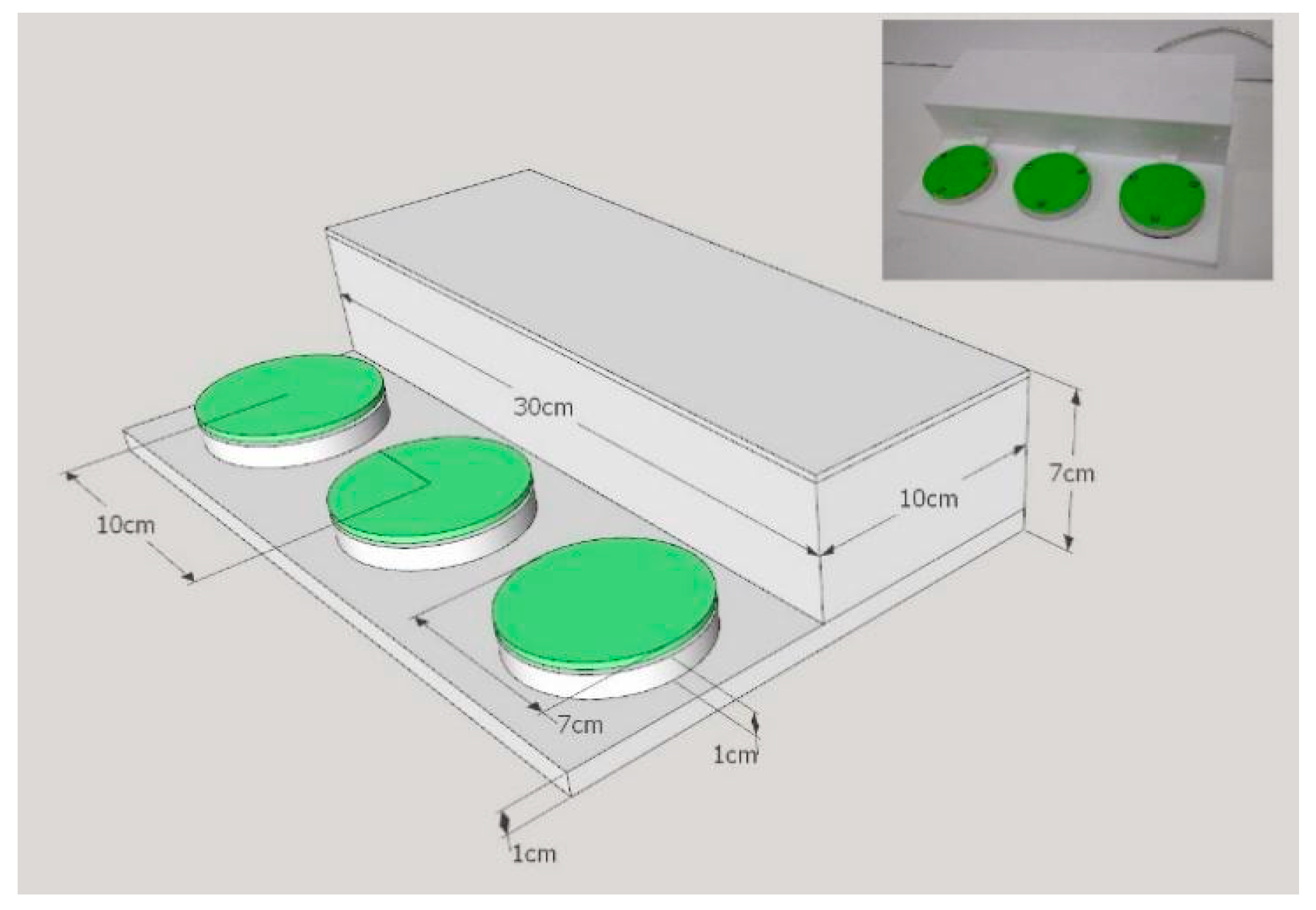
24], is that elderly people may think that computers are not friendly for them, making these games uncomfortable to play. Therefore, our games were designed to be as simple as possible and easy to play, considering that the subjects are old and that most of them have never experienced playing PC-based games before. It was found that the traditional whack-a-mole machine game was a famous game in the past for Taiwanese people. We designed a special board-button to allow the subjects to be more familiar and comfortable with the game. In our discussion, we analyze and explain the response time and the accuracy rate as the dependent variables. We used the MMSE score (normal group, MCI group, and moderate-to-severe dementia group) and game level (slow, medium, and fast) as the independent variables. We also analyzed judgment ability for the hit-the-ball game. All results were calculated using statistical methods (Kruskal–Wallis Test and Friedman Test) for accuracy rate and one-way ANOVA for reaction time. We found that there are significant differences between these three categories of subjects.
4. Conclusions
In this study, we found that the response performance of subjects with mild cognitive impairment and dementia were poor compared to normal subjects comprehensively evaluated by reaction time and accuracy rate. Although in the reaction-time analysis, the performance times of the MCI and dementia groups seemed to be shorter than those of the normal group for the same speed level, the accuracy-rate analysis showed poor performance for both the MCI and dementia groups. We observed that these groups reacted randomly by pressing the button when the speed was increased, without considering the accuracy of the object in both the whack-a-mole and hit-the-ball games. Our results, along with those in [
6,
7], show that those subjects had significantly poorer performance when measured by simple reaction time and accuracy rate. Moreover, we successfully differentiated these three categories of subjects using our serious games. For the reaction-time analysis, we established that the time-unlimited mode in our experiment is a better method to explain the results.
We also found that, even though the two games were designed together to evaluate the reaction performance of the subjects, there were some observable differences in the results of each game. Most subjects had better results with the whack-a-mole game than with the hit-the-ball game. The first reason for this result may be because the hit-the-ball game provides some time for the subject to wait before the ball is on the fairway, which might be related to other cognitive abilities. Further related investigations could be explored in the future. The second reason is because the subjects had to choose between the ball or the meteor ball, which might be related to inhibition ability mentioned by [
23], which affect reaction time. This result could also be because the subjects played a similar game (like a whack-a-mole machine at an amusement park (especially in Taiwan)) in the past. This result could, thus, indicate muscle memory that was trained several years ago.
Finally, we concluded that the reaction time and accuracy rates can be evaluated using our two serious games while distinguishing between the three different subjects. However, participation of more subjects will be an important factor for future research. We also believe that these research results could be developed to investigate cognitive function for healthy subjects and patients because such results are associated with neural functioning [
5,
7]. Therefore, we will also observe potential neural cognitive dysfunction using noninvasive methods such as EEG, MRI, and FMRI with our PC-based serious game. We will also conduct intraindividual variability analysis in future studies to observe the behavior of these subjects. Our hope is that these serious games will be used in the daily life lives of elders to evaluate their performance, followed by and to be followed-up by clinical treatment in the future.

 ,
, 




{kind=link}
{kind=link}
{kind=link}
{kind=link}