Accuracy Verification of an Anatomical Model Manufactured Using Low-Cost Additive Production

 , , , ,
, , , , 
Abstract
1. Introduction
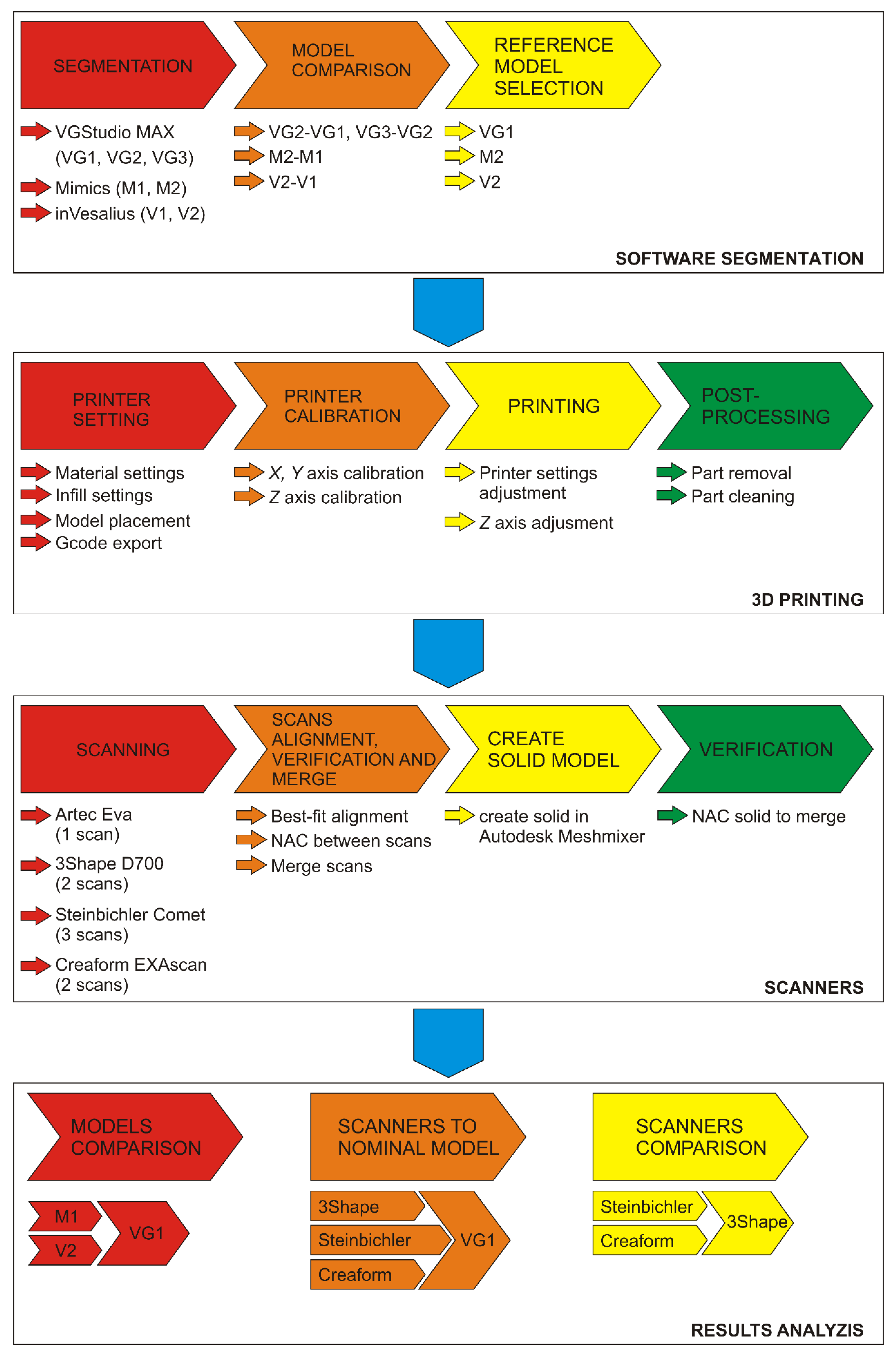
2. Materials and Methods
- CT data processing and analysis of results
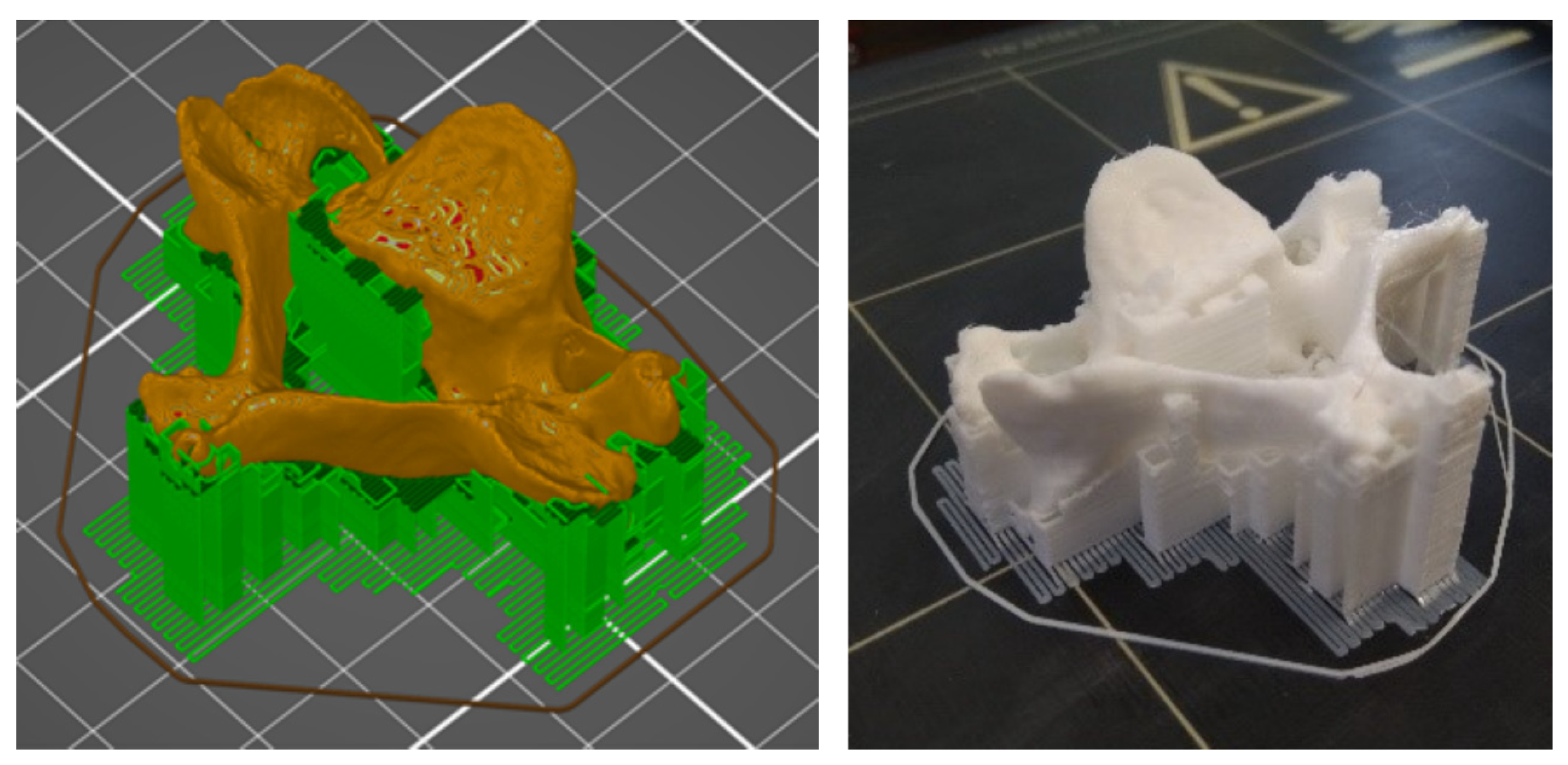
- Model production using additive manufacturing on a low-cost FFF 3D printer
- Scanning with 3D scanners and processing of acquired data
- Analysis of the obtained results
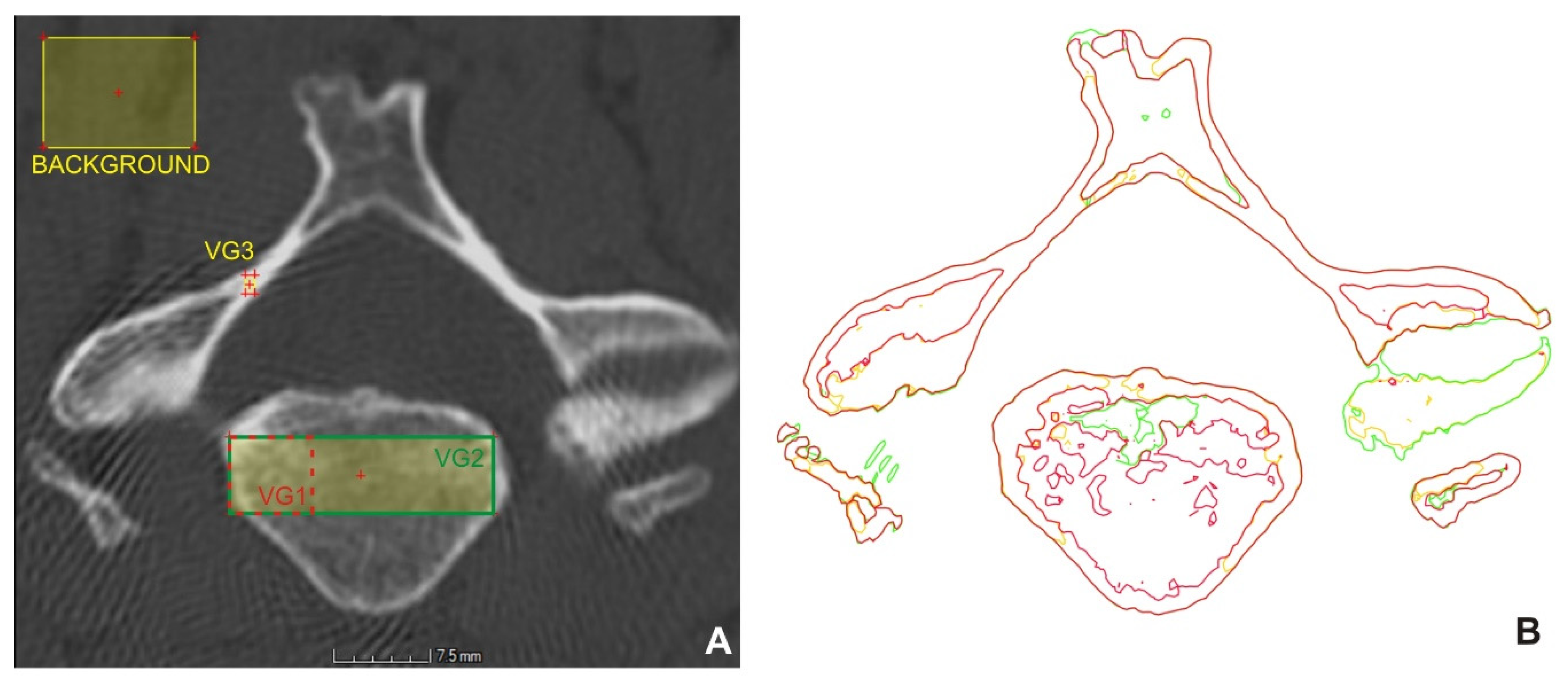
2.1. Processing of CT Data and Results Analysis
2.1.1. Data Processing Methodology in VGStudio MAX
- Creation a region of interest for the selected vertebra
- Determination of the surface of the bone structures
- Extraction of the selected vertebra
2.1.2. Methodology of Data Processing in Mimics
2.1.3. Methodology of inVesalius Data Processing
2.2. Additive Manufacturing of a Vertebra Model
2.3. Methodology of Scanning with 3D Scanners
2.3.1. Artec Eva scanner
2.3.2. 3Shape D700 Scanner
2.3.3. Steinbichler Comet L3D 2M system
2.3.4. Creaform EXAscan system
3. Results
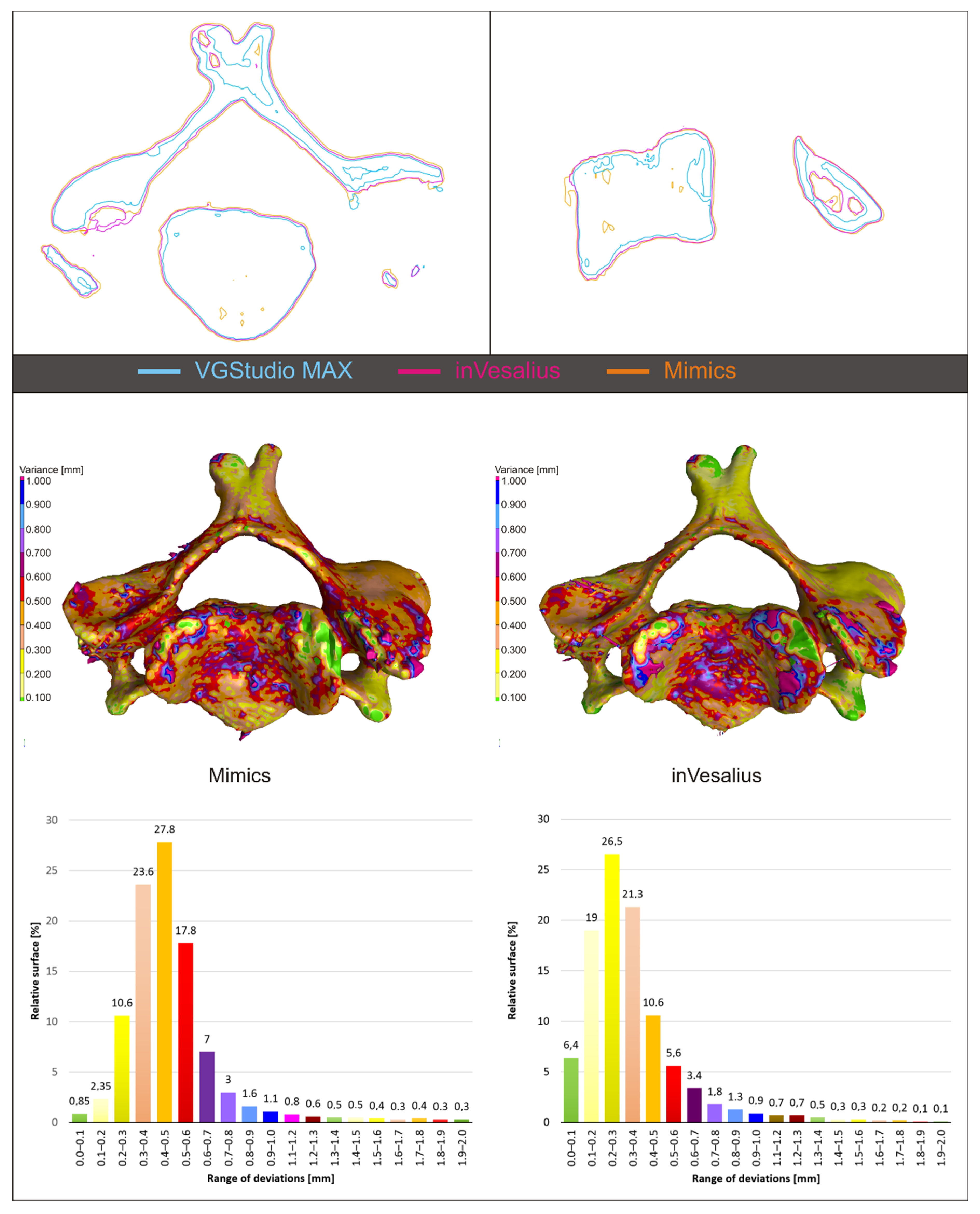
3.1. Results of Thresholding Comparison
3.1.1. VGStudioMAX
3.1.2. Mimics
3.1.3. inVesalius
3.1.4. Comparing Outputs from VGStudio Max, Mimics and inVesalius
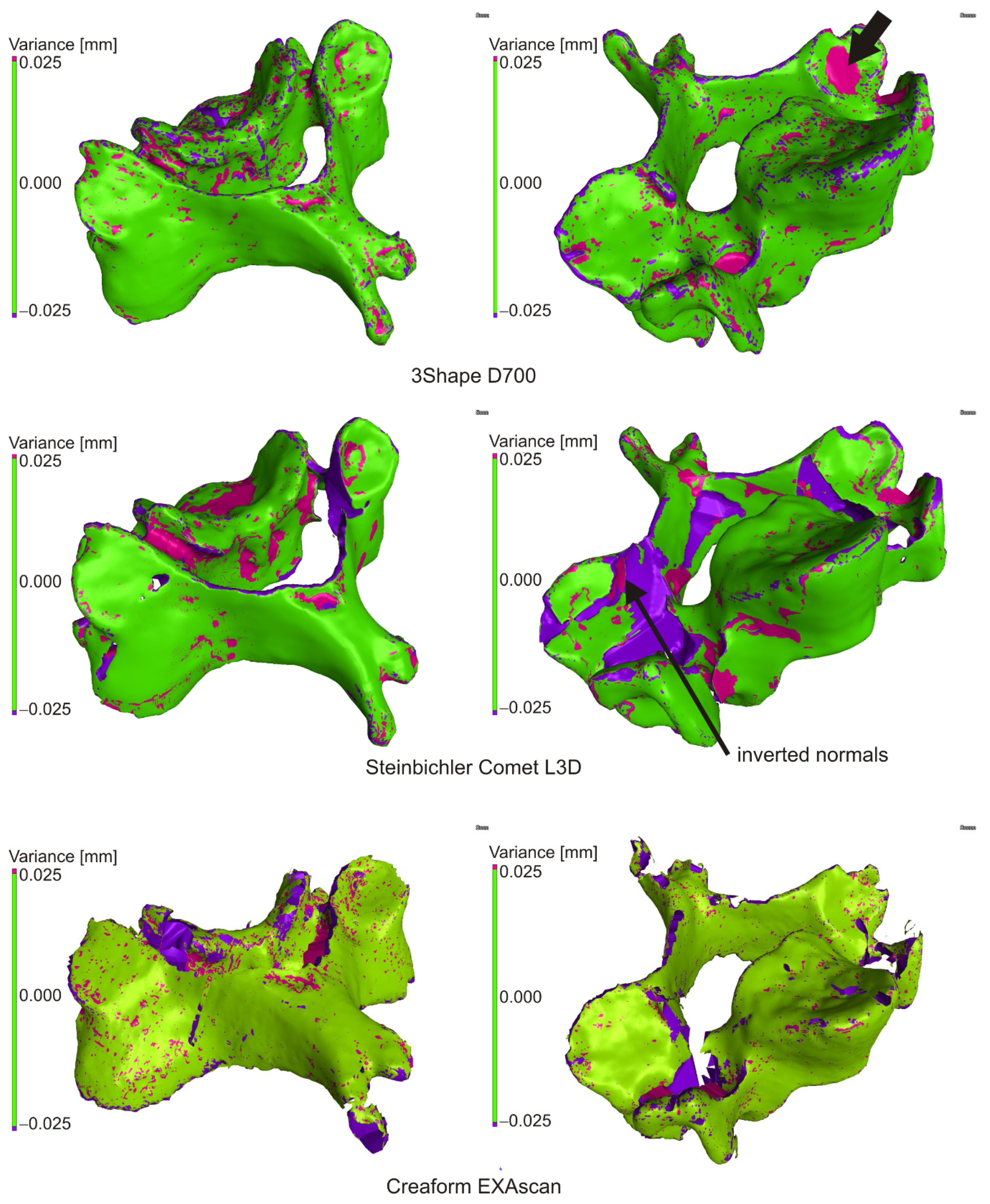
3.2. Checking the Creation of the Solid Model
3.2.1. 3Shape D700
3.2.2. Steinbichler Comet L3D 2M
3.2.3. Creaform EXAscan
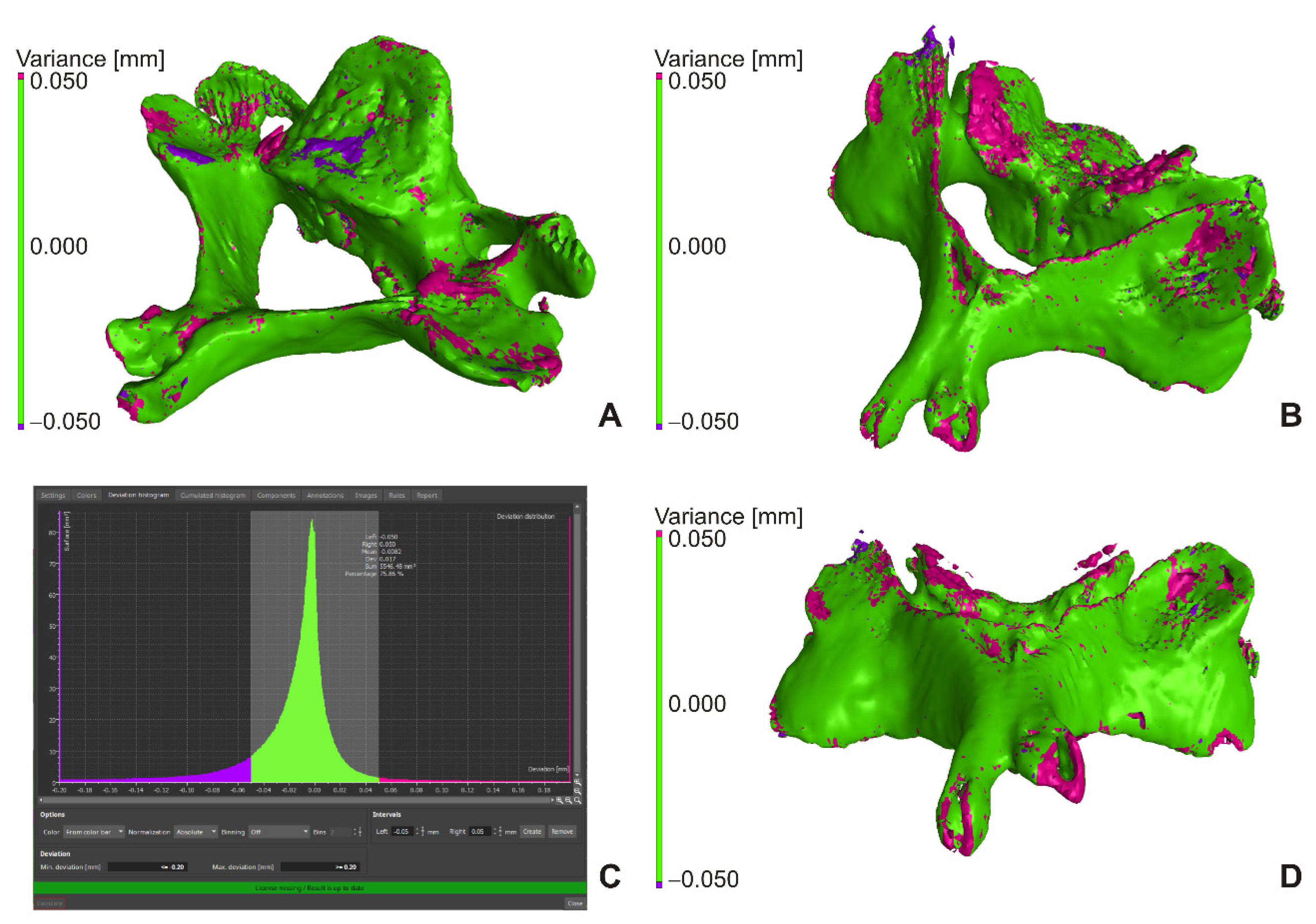
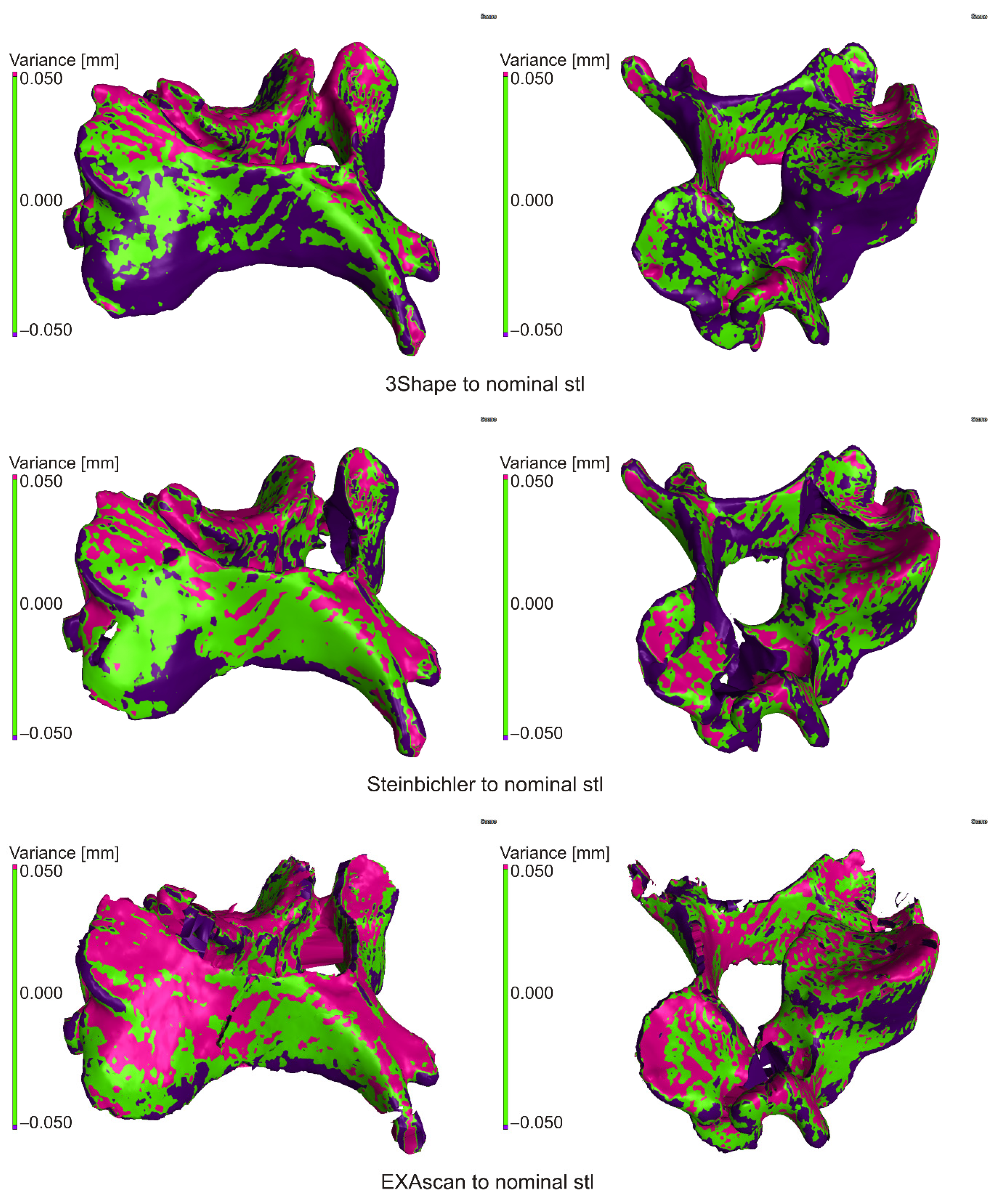
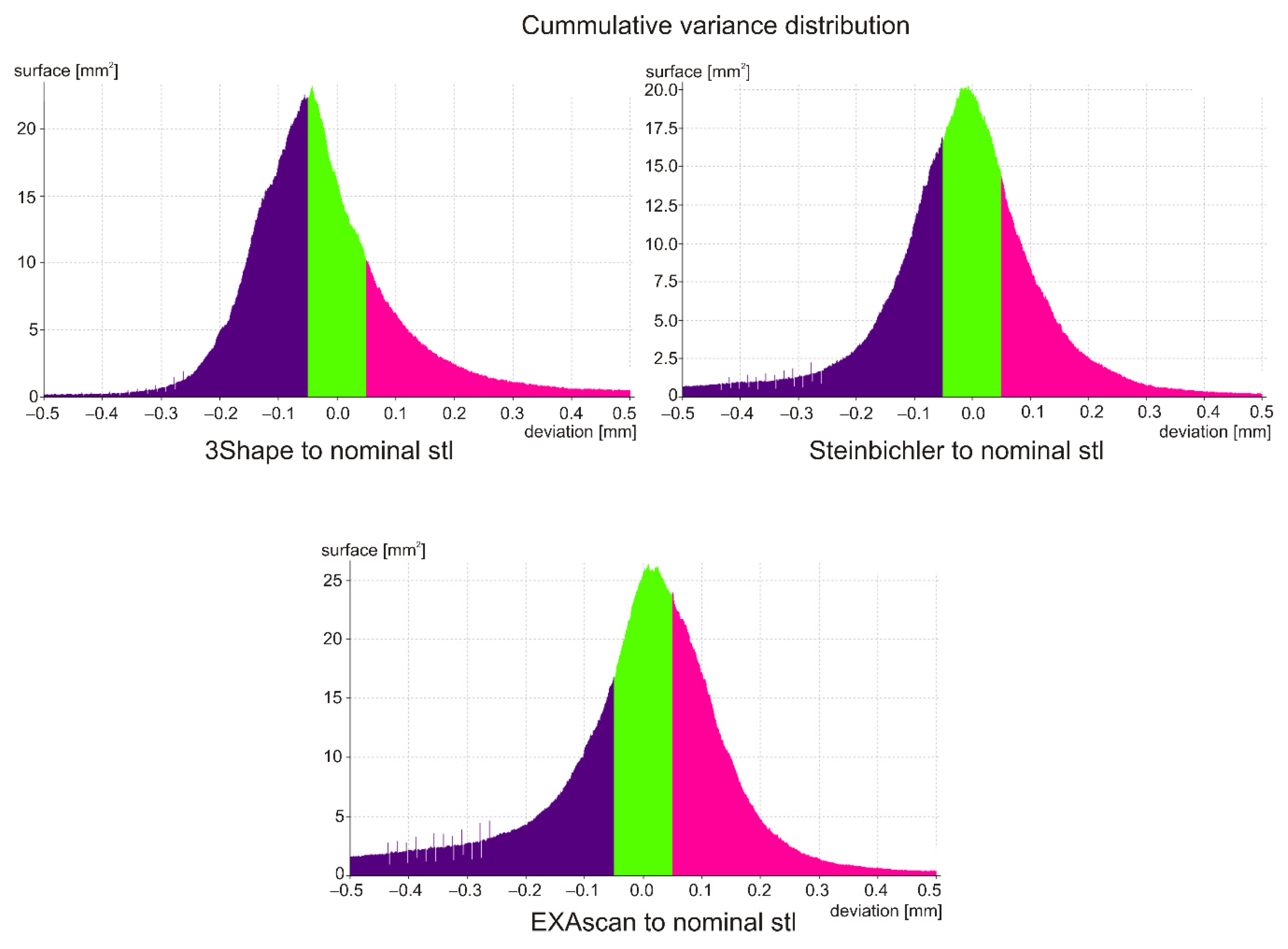
3.3. Evaluation of Production and Scanning Accuracy
3.3.1. Comparison of Scans with Nominal STL File
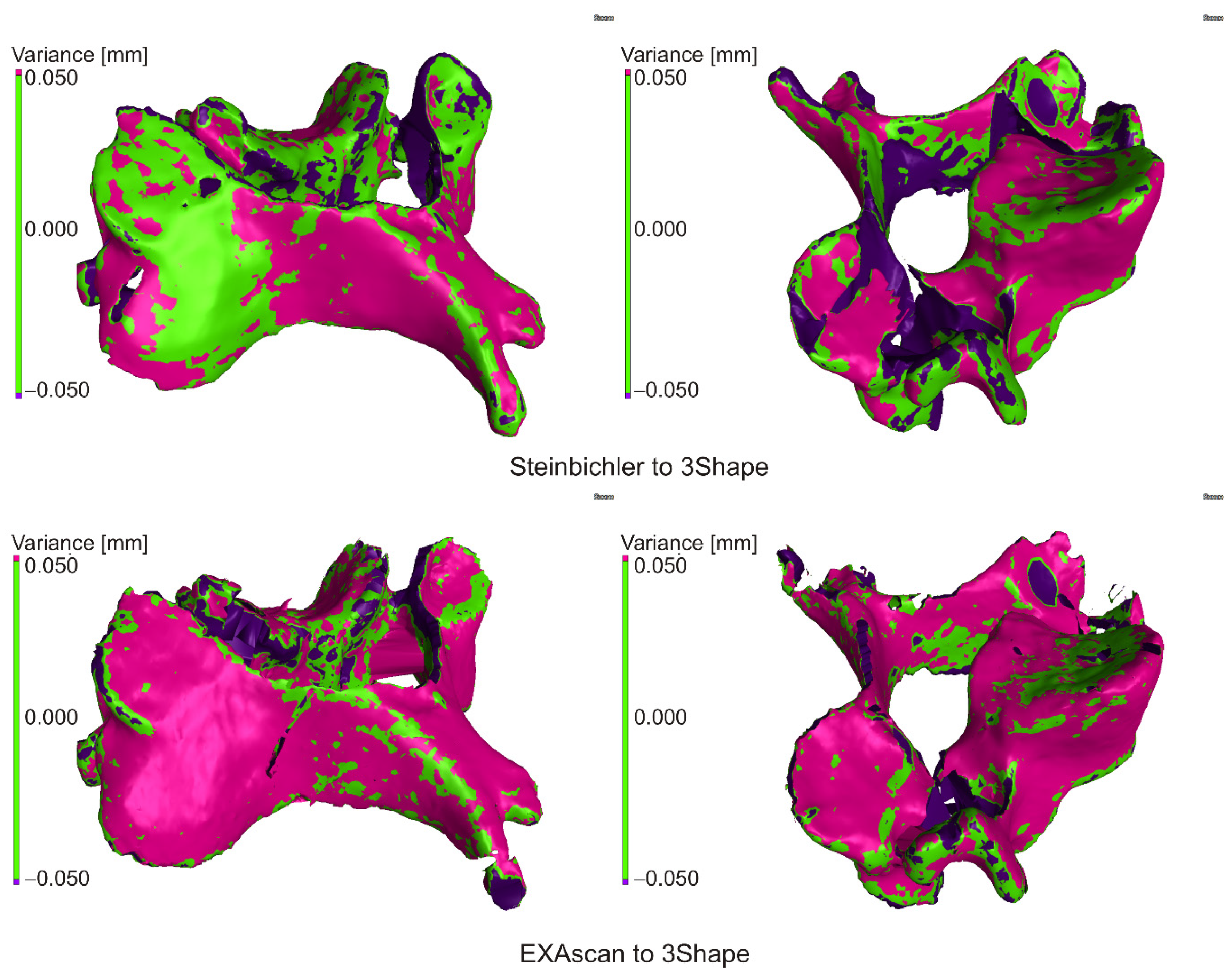
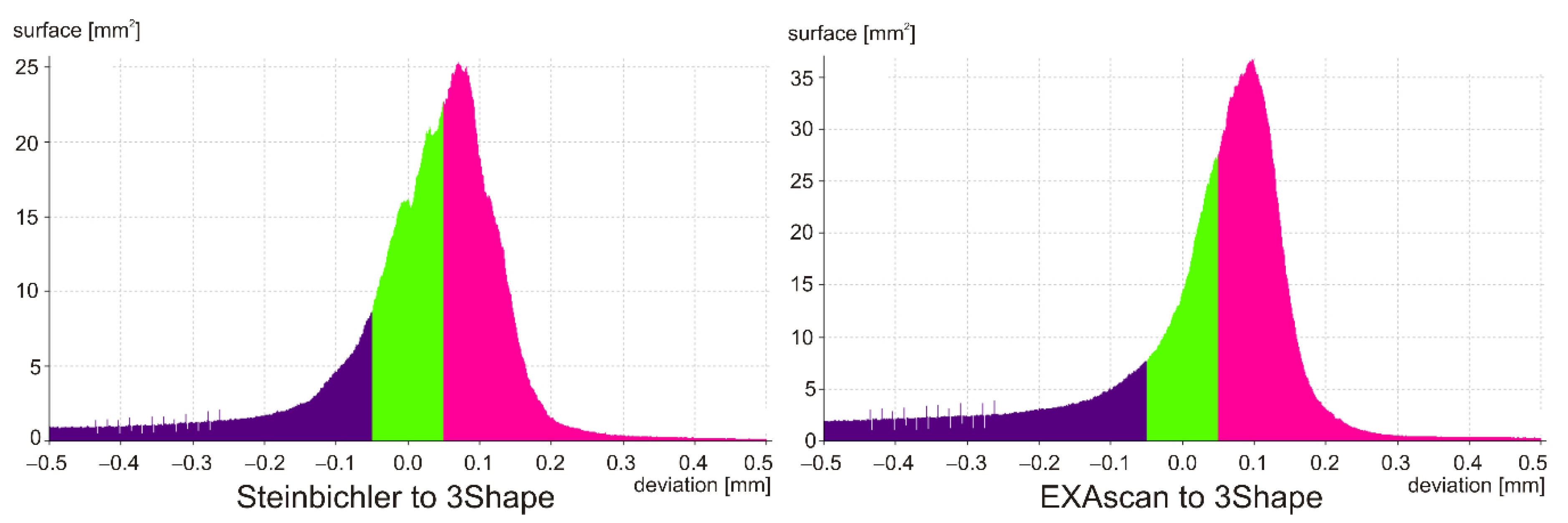
3.3.2. Comparison of Scans
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Wu, A.-M.; Shao, Z.-X.; Wang, J.-S.; Yang, X.-D.; Weng, W.-Q.; Wang, X.-Y.; Xu, H.-Z.; Chi, Y.-L.; Lin, Z.-K. The Accuracy of a Method for Printing Three-Dimensional Spinal Models. PLoS ONE 2015, 10, e0124291. [Google Scholar] [CrossRef] [PubMed]
- Ford, S.; Minshall, T. Invited Review Article: Where and How 3D Printing Is Used in Teaching and Education. Addit. Manuf. 2019, 25, 131–150. [Google Scholar] [CrossRef]
- Cheung, C.L.; Saber, N.R. Bioengineering for Surgery—1st Edition. In Bioengineering for Surgery; Farhat, W., Drake, J., Eds.; Elsevier B.V.: Amsterdam, The Netherland, 2015; pp. 151–166. ISBN 9780081001301. [Google Scholar]
- Rengier, F.; Mehndiratta, A.; Von Tengg-Kobligk, H.; Zechmann, C.M.; Unterhinninghofen, R.; Kauczor, H.U.; Giesel, F.L. 3D Printing Based on Imaging Data: Review of Medical Applications. Int. J. Comput. Assist. Radiol. Surg. 2010, 5, 335–341. [Google Scholar] [CrossRef] [PubMed]
- Khanesar, M.A. Medical Applications of 3D Printing|Iris Publishers. Available online: https://irispublishers.com/abeb/fulltext/medical-applications-of-3d-printing.ID.000531.php (accessed on 11 August 2020).
- Witowski, J.; Sitkowski, M.; Hołda, M.K.; Pędziwiatr, M. 9783110667219-005. Available online: https://www.degruyter.com/view/book/9783110667219/10.1515/9783110667219-005.xml (accessed on 14 October 2020).
- Vaishya, R.; Patralekh, M.K.; Vaish, A.; Agarwal, A.K.; Vijay, V. Publication Trends and Knowledge Mapping in 3D Printing in Orthopaedics. J. Clin. Orthop. Trauma 2018, 9, 194–201. [Google Scholar] [CrossRef] [PubMed]
- Wu, A.M.; Lin, J.L.; Kwan, K.Y.H.; Wang, X.Y.; Zhao, J. 3D-Printing Techniques in Spine Surgery: The Future Prospects and Current Challenges. Expert Rev. Med. Devices 2018, 15, 399–401. [Google Scholar] [CrossRef] [PubMed]
- Haleem, A.; Javaid, M. Role of CT and MRI in the Design and Development of Orthopaedic Model Using Additive Manufacturing. J. Clin. Orthop. Trauma 2018, 9, 213–217. [Google Scholar] [CrossRef]
- Zadpoor, A.A.; Malda, J. Additive Manufacturing of Biomaterials, Tissues, and Organs. Ann. Biomed. Eng. 2017, 45, 1–11. [Google Scholar] [CrossRef]
- Skrzat, J.; Zdilla, M.J.; Brzegowy, P.; Hołda, M. 3D Printed Replica of the Human Temporal Bone Intended for Teaching Gross Anatomy. Folia Med. Cracov. 2019, 59, 23–30. [Google Scholar] [CrossRef]
- Clifton, W.; Damon, A.; Valero-Moreno, F.; Nottmeier, E.; Pichelmann, M. The SpineBox: A Freely Available, Open-Access, 3D-Printed Simulator Design for Lumbar Pedicle Screw Placement. Cureus 2020, 12. [Google Scholar] [CrossRef]
- Hasan, O.; Atif, M.; Jessar, M.M.; Hashmi, P. Application of 3D Printing in Orthopaedic Surgery. A New Affordable Horizon for Cost-Conscious Care—PubMed. Available online: https://pubmed.ncbi.nlm.nih.gov/30697019/ (accessed on 11 August 2020).
- Marro, A.; Bandukwala, T.; Mak, W. Three-Dimensional Printing and Medical Imaging: A Review of the Methods and Applications. Curr. Probl. Diagn. Radiol. 2016, 45, 2–9. [Google Scholar] [CrossRef]
- Bücking, T.M.; Hill, E.R.; Robertson, J.L.; Maneas, E.; Plumb, A.A.; Nikitichev, D.I. From Medical Imaging Data to 3D Printed Anatomical Models. PLoS ONE 2017, 12. [Google Scholar] [CrossRef] [PubMed]
- Ganguli, A.; Pagan-Diaz, G.J.; Grant, L.; Cvetkovic, C.; Bramlet, M.; Vozenilek, J.; Kesavadas, T.; Bashir, R. 3D Printing for Preoperative Planning and Surgical Training: A Review. Biomed. Microdevices 2018, 20, 1–24. [Google Scholar] [CrossRef] [PubMed]
- Salmi, M. Possibilities of Preoperative Medical Models Made by 3D Printing or Additive Manufacturing. J. Med. Eng. 2016, 2016, 1–6. [Google Scholar] [CrossRef] [PubMed]
- Anderson, P.A. 3D Printing for Education and Surgical Planning in Orthopedic Surgery. In 3D Printing in Orthopaedic Surgery; Elsevier: Amsterdam, The Netherland, 2019; pp. 55–63. [Google Scholar]
- Hedelin, H.; Swinkels, C.S.; Laine, T.; Mack, K.; Lagerstrand, K. Using a 3D Printed Model as a Preoperative Tool for Pelvic Triple Osteotomy in Children. JAAOS Glob. Res. Rev. 2019, 3, e074. [Google Scholar] [CrossRef]
- Lee, H.; Nguyen, N.H.; Hwang, S.I.L.; Lee, H.J.; Hong, S.K.; Byun, S.S. Personalized 3D Kidney Model Produced by Rapid Prototyping Method and Its Usefulness in Clinical Applications. Int. Braz. J. Urol. 2018, 44, 952–957. [Google Scholar] [CrossRef]
- Bernhard, J.C.; Isotani, S.; Matsugasumi, T.; Duddalwar, V.; Hung, A.J.; Suer, E.; Baco, E.; Satkunasivam, R.; Djaladat, H.; Metcalfe, C.; et al. Personalized 3D Printed Model of Kidney and Tumor Anatomy: A Useful Tool for Patient Education. World J. Urol. 2016, 34, 337–345. [Google Scholar] [CrossRef]
- Biglino, G.; Capelli, C.; Wray, J.; Schievano, S.; Leaver, L.K.; Khambadkone, S.; Giardini, A.; Derrick, G.; Jones, A.; Taylor, A.M. 3D-Manufactured Patient-Specific Models of Congenital Heart Defects for Communication in Clinical Practice: Feasibility and Acceptability. BMJ Open 2015, 5, e007165. [Google Scholar] [CrossRef]
- Garcia, J.; Yang, Z.L.; Mongrain, R.; Leask, R.L.; Lachapelle, K. 3D Printing Materials and Their Use in Medical Education: A Review of Current Technology and Trends for the Future. BMJ Simul. Technol. Enhanc. Learn. 2018, 4, 27–40. [Google Scholar] [CrossRef]
- Wake, N.; Rosenkrantz, A.B.; Huang, R.; Park, K.U.; Wysock, J.S.; Taneja, S.S.; Huang, W.C.; Sodickson, D.K.; Chandarana, H. Patient-Specific 3D Printed and Augmented Reality Kidney and Prostate Cancer Models: Impact on Patient Education. 3D Print. Med. 2019, 5, 4. [Google Scholar] [CrossRef]
- van de Belt, T.H.; Nijmeijer, H.; Grim, D.; Engelen, L.J.L.P.G.; Vreeken, R.; van Gelder, M.M.H.J.; Ter Laan, M. Patient-Specific Actual-Size Three-Dimensional Printed Models for Patient Education in Glioma Treatment: First Experiences. World Neurosurg. 2018, 117, e99–e105. [Google Scholar] [CrossRef]
- Prinold, J.A.I.; Mazzà, C.; Di Marco, R.; Hannah, I.; Malattia, C.; Magni-Manzoni, S.; Petrarca, M.; Ronchetti, A.B.; Tanturri de Horatio, L.; van Dijkhuizen, E.H.P.; et al. A Patient-Specific Foot Model for the Estimate of Ankle Joint Forces in Patients with Juvenile Idiopathic Arthritis. Ann. Biomed. Eng. 2016, 44, 247–257. [Google Scholar] [CrossRef] [PubMed]
- Lashkarinia, S.S.; Piskin, S.; Bozkaya, T.A.; Salihoglu, E.; Yerebakan, C.; Pekkan, K. Computational Pre-Surgical Planning of Arterial Patch Reconstruction: Parametric Limits and In Vitro Validation. Ann. Biomed. Eng. 2018, 46, 1292–1308. [Google Scholar] [CrossRef] [PubMed]
- George, E.; Liacouras, P.; Rybicki, F.J.; Mitsouras, D. Measuring and Establishing the Accuracy and Reproducibility of 3D Printed Medical Models. Radiographics 2017, 37, 1424–1450. [Google Scholar] [CrossRef] [PubMed]
- Mcmenamin, P.G.; Quayle, M.R.; Mchenry, C.R.; Adams, J.W. The Production of Anatomical Teaching Resources Using Three-Dimensional (3D) Printing Technology. Anat. Sci. Educ. 2014, 7, 479–486. [Google Scholar] [CrossRef]
- Tong, Y.; Kaplan, D.J.; Spivak, J.M.; Bendo, J.A. Three-Dimensional Printing in Spine Surgery: A Review of Current Applications. Spine J. 2020, 20, 833–846. [Google Scholar] [CrossRef]
- Abate, K.M.; Nazir, A.; Yeh, Y.P.; Chen, J.E.; Jeng, J.Y. Design, Optimization, and Validation of Mechanical Properties of Different Cellular Structures for Biomedical Application. Int. J. Adv. Manuf. Technol. 2020, 106, 1253–1265. [Google Scholar] [CrossRef]
- Nazir, A.; Jeng, J.-Y. A High-Speed Additive Manufacturing Approach for Achieving High Printing Speed and Accuracy. Proc. Inst. Mech. Eng. Part C J. Mech. Eng. Sci. 2020, 234, 2741–2749. [Google Scholar] [CrossRef]
- Gadia, A.; Shah, K.; Nene, A. Emergence of Three-Dimensional Printing Technology and Its Utility in Spine Surgery. Asian Spine J. 2018, 12, 365–371. [Google Scholar] [CrossRef]
- Liew, Y.; Beveridge, E.; Demetriades, A.K.; Hughes, M.A. 3D Printing of Patient-Specific Anatomy: A Tool to Improve Patient Consent and Enhance Imaging Interpretation by Trainees. Br. J. Neurosurg. 2015, 29, 712–714. [Google Scholar] [CrossRef]
- Chepelev, L.; Wake, N.; Ryan, J.; Althobaity, W.; Gupta, A.; Arribas, E.; Santiago, L.; Ballard, D.H.; Wang, K.C.; Weadock, W.; et al. Radiological Society of North America (RSNA) 3D Printing Special Interest Group (SIG): Guidelines for Medical 3D Printing and Appropriateness for Clinical Scenarios. 3D Print. Med. 2018, 4, 1–38. [Google Scholar] [CrossRef]
- Mitsouras, D.; Liacouras, P.; Imanzadeh, A.; Giannopoulos, A.A.; Cai, T.; Kumamaru, K.K.; George, E.; Wake, N.; Caterson, E.J.; Pomahac, B.; et al. Medical 3D Printing for the Radiologist. Radiographics 2015, 35, 1965–1988. [Google Scholar] [CrossRef] [PubMed]
- Šljivić, M.; Mirjanić, D.; Šljivić, N.; Fragassa, C.; Pavlović, A. 3D Printing and 3D Bioprinting to Use for Medical Applications. Contemp. Mater. 2019, 82–92. [Google Scholar] [CrossRef]
- Goff, R.P.; Spencer, J.H.; Iaizzo, P.A. MRI Reconstructions of Human Phrenic Nerve Anatomy and Computational Modeling of Cryoballoon Ablative Therapy. Ann. Biomed. Eng. 2016, 44, 1097–1106. [Google Scholar] [CrossRef] [PubMed]
- Wilcox, B.; Mobbs, R.J.; Wu, A.-M.; Phan, K. Systematic Review of 3D Printing in Spinal Surgery: The Current State of Play. J. Spine Surg. 2017, 3, 433–443. [Google Scholar] [CrossRef] [PubMed]











{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Surface Determination | VG1 | VG2 | VG3 |
|---|---|---|---|
| Background | 32 | 18 | 29 |
| Material | 743 | 545 | 1746 |
| Isosurface | 388 | 282 | 887 |
| NOMINAL | 3Shape D700 | Steinbichler Comet | Creaform EXAscan |
|---|---|---|---|
| DEV50 (%) | 32.100 | 37.500 | 33.900 |
| PER95 (mm) | 0.272 | 0.312 | 0.361 |
| 3Shape D700 | Steinbichler Comet | Creaform EXAscan |
|---|---|---|
| DEV50 (%) | 34.300 | 24.500 |
| PER95 (mm) | 0.305 | 0.363 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Tóth, T.; Varga, P.; Štefanovič, B.; Bednarčíková, L.; Schnitzer, M.; Hudák, R.; Živčák, J. Accuracy Verification of an Anatomical Model Manufactured Using Low-Cost Additive Production. Appl. Sci. 2021, 11, 594. https://doi.org/10.3390/app11020594
Tóth T, Varga P, Štefanovič B, Bednarčíková L, Schnitzer M, Hudák R, Živčák J. Accuracy Verification of an Anatomical Model Manufactured Using Low-Cost Additive Production. Applied Sciences. 2021; 11(2):594. https://doi.org/10.3390/app11020594
Chicago/Turabian StyleTóth, Teodor, Patrik Varga, Branko Štefanovič, Lucia Bednarčíková, Marek Schnitzer, Radovan Hudák, and Jozef Živčák. 2021. "Accuracy Verification of an Anatomical Model Manufactured Using Low-Cost Additive Production" Applied Sciences 11, no. 2: 594. https://doi.org/10.3390/app11020594
APA StyleTóth, T., Varga, P., Štefanovič, B., Bednarčíková, L., Schnitzer, M., Hudák, R., & Živčák, J. (2021). Accuracy Verification of an Anatomical Model Manufactured Using Low-Cost Additive Production. Applied Sciences, 11(2), 594. https://doi.org/10.3390/app11020594