
Intra-Articular Hybrid Hyaluronic Acid Injection Treatment in Overweight Patients with Knee Osteoarthritis: A Single-Center, Open-Label, Prospective Study

 ,
,  , , ,
, , ,
Abstract
1. Introduction
2. Materials and Methods
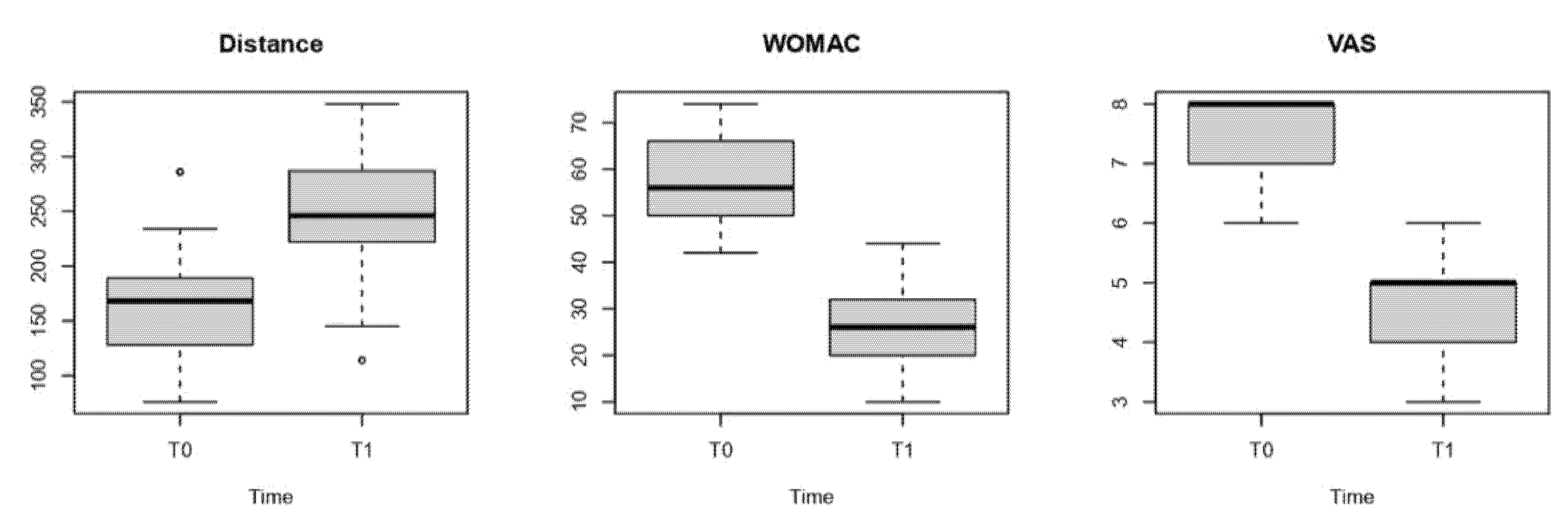
- pain severity, as assessed by VAS scale;
- disease severity, as assessed by the WOMAC Index;
- cardiocirculatory capacity, as assessed by distance walked in a 6MWT.
- quality of life, as assessed by SF-12;
- the percentage of fat and muscle mass, measured by bioelectrical impedance analysis;
- analgesic intake (days per week).
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Vina, E.R.; Kwoh, C.K. Epidemiology of Osteoarthritis: Literature Update. Curr. Opin. Rheumatol. 2018, 30, 160–167. [Google Scholar] [CrossRef]
- Fu, K.; Robbins, S.R.; McDougall, J.J. Osteoarthritis: The Genesis of Pain. Rheumatology 2018, 57, iv43–iv50. [Google Scholar] [CrossRef]
- Driban, J.B.; Harkey, M.S.; Barbe, M.F.; Ward, R.J.; MacKay, J.W.; Davis, J.E.; Lu, B.; Price, L.L.; Eaton, C.B.; Lo, G.H.; et al. Risk factors and the natural history of accelerated knee osteoarthritis: A narrative review. BMC Musculoskelet. Disord. 2020, 21, 332. [Google Scholar] [CrossRef]
- Sandhar, S.; Smith, T.O.; Toor, K.; Howe, F.; Sofat, N. Risk factors for pain and functional impairment in people with knee and hip osteoarthritis: A systematic review and meta-analysis. BMJ Open 2020, 10, e038720. [Google Scholar] [CrossRef]
- Bullock, G.S.; Collins, G.S.; Peirce, N.; Arden, N.K.; Filbay, S.R. Playing sport injured is associated with osteoarthritis, joint pain and worse health-related quality of life: A cross-sectional study. BMC Musculoskelet. Disord. 2020, 21, 111. [Google Scholar] [CrossRef] [PubMed]
- Priano, F. Early Efficacy of Intra-Articular HYADD® 4 (Hymovis®) Injections for Symptomatic Knee Osteoarthritis. Joints 2017, 5, 79–84. [Google Scholar] [CrossRef] [PubMed][Green Version]
- Apovian, C.M. Obesity: Definition, comorbidities, causes, and burden. Am. J. Manag. Care 2016, 22 (Suppl. 7), s176–s185. [Google Scholar] [PubMed]
- Di Bonaventura, M.; Nicolucci, A.; Meincke, H.; Le Lay, A.; Fournier, J. Obesity in Germany and Italy: Prevalence, comorbidities, and associations with patient outcomes. Clinicoecon. Outcomes Res. 2018, 10, 457–475. [Google Scholar] [CrossRef]
- Chen, L.; Zheng, J.J.Y.; Li, G.; Yuan, J.; Ebert, J.R.; Li, H.; Papadimitriou, J.; Wang, Q.; Wood, D.; Jones, C.W.; et al. Pathogenesis and clinical management of obesity-related knee osteoarthritis: Impact of mechanical loading. J. Orthop. Translat. 2020, 2, 66–75. [Google Scholar] [CrossRef]
- Raud, B.; Gay, C.; Guiguet-Auclair, C.; Bonnin, A.; Gerbaud, L.; Pereira, B.; Duclos, M.; Boirie, Y.; Coudeyre, E. Level of Obesity Is Directly Associated with the Clinical and Functional Consequences of Knee Osteoarthritis. Sci. Rep. 2020, 10, 3601. [Google Scholar] [CrossRef]
- Hochberg, M.C.; Altman, R.D.; April, K.T.; Benkhalti, M.; Guyatt, G.; McGowan, J.; Towheed, T.; Welch, V.; Wells, G.; Tugwell, P. American College of Rheumatology 2012 Recommendations for the Use of Nonpharmacologic and Pharmacologic Therapies in Osteoarthritis of the Hand, Hip, and Knee. Arthritis Care Res. 2012, 64, 465–474. [Google Scholar] [CrossRef] [PubMed]
- De Sire, A.; Marotta, N.; Marinaro, C.; Curci, C.; Invernizzi, M.; Ammendolia, A. Role of Physical Exercise and Nutraceuticals in Modulating Molecular Pathways of Osteoarthritis. Int. J. Mol. Sci. 2021, 22, 5722. [Google Scholar] [CrossRef] [PubMed]
- Wood, A.M.; Brock, T.M.; Heil, K.; Holmes, R.; Weusten, A. A Review on the Management of Hip and Knee Osteoarthritis. Int. J. Chronic Dis. 2013, 2013, 845015. [Google Scholar] [CrossRef] [PubMed]
- Amin, A.K.; Clayton, R.A.E.; Patton, J.T.; Gaston, M.; Cook, R.E.; Brenkel, I.J. Total Knee Replacement in Morbidly Obese Patients: Results of a Prospective, Matched Study. J. Bone Jt. Surg. Ser. B 2006, 88, 1321–1326. [Google Scholar] [CrossRef]
- Bannuru, R.R.; Osani, M.C.; Vaysbrot, E.E.; Arden, N.K.; Bennell, K.; Bierma-Zeinstra, S.M.A.; Kraus, V.B.; Lohmander, L.S.; Abbott, J.H.; Bhandari, M.; et al. OARSI Guidelines for the Non-Surgical Management of Knee, Hip, and Polyarticular Osteoarthritis. Osteoarthr. Cartil 2019, 27, 1578–1589. [Google Scholar] [CrossRef] [PubMed]
- Balazs, E.A.; Denlinger, J.L. Viscosupplementation: A New Concept in the Treatment of Osteoarthritis. J. Rheumatol. 1993, 20, 3–9. [Google Scholar]
- Maheu, E.; Bannuru, R.R.; Herrero-Beaumont, G.; Allali, F.; Bard, H.; Migliore, A. Why we should definitely include intra-articular hyaluronic acid as a therapeutic option in the management of knee osteoarthritis: Results of an extensive critical literature review. Semin. Arthritis Rheum. 2019, 48, 563–572. [Google Scholar] [CrossRef]
- Abatangelo, G.; Vindigni, V.; Avruscio, G.; Pandis, L.; Brun, P. Hyaluronic Acid: Redefining Its Role. Cells 2020, 9, 1743. [Google Scholar] [CrossRef]
- Billesberger, L.M.; Fisher, K.M.; Qadri, Y.J.; Boortz-Marx, R.L. Procedural Treatments for Knee Osteoarthritis: A Review of Current Injectable Therapies. Pain Res. Manag. 2020, 2020, 3873098. [Google Scholar] [CrossRef]
- Ceniti, S.; Morrone, E.G. Hybrid Hyaluronic Acid: Time Course of Pain Relief in the Treatment of Knee and Hip Osteoarthritis. G. Ital. Ortop. Traumatol. 2017, 43, 98–103. [Google Scholar]
- Manciameli, A.; Peruzzi, M. Treating Moderate Gonarthrosis with Intra-Articular Injections of Sodium Salt Hyaluronic Acid. G. Ital. Ortop. Traumatol. 2018, 44, 146–149. [Google Scholar]
- Papalia, R.; Russo, F.; Torre, G.; Albo, E.; Grimaldi, V.; Papalia, G.; Sterzi, S.; Vadalà, G.; Bressi, F.; Denaro, V. Hybrid Hyaluronic Acid versus High Molecular Weight Hyaluronic Acid for the Treatment of Osteoarthritis in Obese Patients. J. Biol. Regul. Homeost. Agents 2017, 31, 103–109. [Google Scholar] [PubMed]
- Hashizume, M.; Koike, N.; Yoshida, H.; Suzuki, M.; Mihara, M. High molecular weight hyaluronic acid relieved joint pain and prevented the progression of cartilage degeneration in a rabbit osteoarthritis model after onset of arthritis. Mod. Rheumatol. 2010, 20, 432–438. [Google Scholar] [CrossRef] [PubMed]
- Wang, C.T.; Lin, Y.T.; Chiang, B.L.; Lin, Y.H.; Hou, S.M. High molecular weight hyaluronic acid down-regulates the gene expression of osteoarthritis-associated cytokines and enzymes in fibroblast-like synoviocytes from patients with early osteoarthritis. Osteoarthr. Cartil. 2006, 14, 1237–1247. [Google Scholar] [CrossRef]
- Bellamy, N.; Buchanan, W.W.; Goldsmith, C.H.; Campbell, J.; Stitt, L.W. Validation Study of WOMAC: A Health Status Instrument for Measuring Clinically Important Patient Relevant Outcomes to Antirheumatic Drug Therapy in Patients with Osteoarthritis of the Hip or Knee. J. Rheumatol. 1988, 15, 1833–1840. [Google Scholar]
- Gimigliano, F.; Moretti, A.; de Sire, A.; Calafiore, D.; Iolascon, G. The combination of vitamin D deficiency and overweight affects muscle mass and function in older post-menopausal women. Aging Clin. Exp. Res. 2018, 30, 625–631. [Google Scholar] [CrossRef]
- El Masri, D.; Itani, L.; Tannir, H.; Kreidieh, D.; El Ghoch, M. The Relationship between Sarcopenic Obesity, Weight-Loss and Maintenance Outcomes during Obesity Management: Are Additional Strategies Required? Clin. Pract. 2021, 11, 525–531. [Google Scholar] [CrossRef]
- Berenbaum, F.; Wallace, I.J.; Lieberman, D.E.; Felson, D.T. Modern-Day Environmental Factors in the Pathogenesis of Osteoarthritis. Nat. Rev. Rheumatol. 2018, 14, 674–681. [Google Scholar] [CrossRef]
- de Sire, A.; Stagno, D.; Minetto, M.A.; Cisari, C.; Baricich, A.; Invernizzi, M. Long-term effects of intra-articular oxygen-ozone therapy versus hyaluronic acid in older people affected by knee osteoarthritis: A randomized single-blind extension study. J. Back Musculoskelet. Rehabil. 2020, 33, 347–354. [Google Scholar] [CrossRef]
- Rabini, A.; De Sire, A.; Marzetti, E.; Gimigliano, R.; Ferriero, G.; Piazzini, D.B.; Iolascon, G.; Gimigliano, F. Effects of focal muscle vibration on physical functioning in patients with knee osteoarthritis: A randomized controlled trial. Eur. J. Phys. Rehabil. Med. 2015, 51, 513–520. [Google Scholar]
- Ip, H.L.; Nath, D.K.; Sawleh, S.H.; Kabir, M.H.; Jahan, N. Regenerative Medicine for Knee Osteoarthritis—The Efficacy and Safety of Intra-Articular Platelet-Rich Plasma and Mesenchymal Stem Cells Injections: A Literature Review. Cureus 2020, 12, e10575. [Google Scholar] [CrossRef]
- Chevalier, X.; Jerosch, J.; Goupille, P.; Van Dijk, N.; Luyten, F.P.; Scott, D.L.; Bailleul, F.; Pavelka, K. Single, intra-articular treatment with 6 mL hylan G-F 20 in patients with symptomatic primary osteoarthritis of the knee: A randomised, multicentre, double-blind, placebo controlled trial. Ann. Rheum. Dis. 2010, 69, 113–119. [Google Scholar] [CrossRef]
- Maia, P.A.V.; Cossich, V.R.A.; Salles-Neto, J.I.; Aguiar, D.P.; de Sousa, E.B. Viscosupplementation improves pain, function and muscle strength, but not proprioception, in patients with knee osteoarthritis: A prospective randomized trial. Clinics 2019, 25, e1207. [Google Scholar] [CrossRef]
- Sun, S.F.; Hsu, C.W.; Lin, H.S.; Liou, I.H.; Chen, Y.H.; Hung, C.L. Comparison of Single Intra-ArticularInjection of NovelHyaluronan (HYA-JOINT Plus) with Synvisc-One for KneeOsteoarthritis: A Randomized, Controlled, Double-Blind Trial of Efficacy and Safety. J. Bone Jt. Surg. Am. 2017, 99, 462–471. [Google Scholar] [CrossRef]
- Johnston, J.; Brown, K.; Muir, J.; Sloniewsky, M.J. Long-Term Outcomes of Single versus Multiple Courses of Viscosupplementation for Osteoarthritic Knee Pain: Real-World, Multi-Practice Experience Over a Six-Year Period. J. Pain Res. 2021, 14, 2413–2421. [Google Scholar] [CrossRef] [PubMed]
- Katz, J.N.; Arant, K.R.; Loeser, R.F. Diagnosis and Treatment of Hip and Knee Osteoarthritis: A Review. JAMA J. Am. Med. Assoc. 2021, 325, 568–578. [Google Scholar] [CrossRef]
- Lee, M.I.; Kim, J.H.; Kwak, H.H.; Woo, H.M.; Han, J.H.; Yayon, A.; Jung, Y.C.; Cho, J.M.; Kang, B.J. A placebo-controlled study comparing the efficacy of intra-articular injections of hyaluronic acid and a novel hyaluronic acid-platelet-rich plasma conjugate in a canine model of osteoarthritis. J. Orthop. Surg. Res. 2019, 14, 314. [Google Scholar] [CrossRef] [PubMed]
- Han, S.B.; Seo, I.W.; Shin, Y.S. Intra-Articular Injections of Hyaluronic Acid or Steroids Associated With Better Outcomes Than Platelet-Rich Plasma, Adipose Mesenchymal Stromal Cells, or Placebo in Knee Osteoarthritis: A Network Meta-analysis. Arthroscopy 2021, 37, 292–306. [Google Scholar] [CrossRef]
- Gazendam, A.; Ekhtiari, S.; Bozzo, A.; Phillips, M.; Bhandari, M. Intra-articular saline injection is as effective as corticosteroids, platelet-rich plasma and hyaluronic acid for hip osteoarthritis pain: A systematic review and network meta-analysis of randomised controlled trials. Br. J. Sports Med. 2021, 55, 256–261. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| T0 | T1 | p-Value | |
|---|---|---|---|
| Distance (mean ± SD) | 164.3 ± 52.9 | 254.9 ± 52.6 | <0.01 |
| WOMAC (median (IQR)) | 56 (16) | 26 (12) | <0.01 |
| VAS(median
(IQR)) | 8 (1) | 5 (1) | <0.01 |
| T0 | T1 | p-Value | |
|---|---|---|---|
| SF-12 (median (IQR)) | 25 (4) | 28 (8) | <0.05 |
| Muscle mass (mean ± SD) | 36.1 ± 4.5 | 37.0 ± 3.8 | 0.62 |
| Fat mass (mean ± SD) | 35 ± 3.6 | 34.5 ± 3.6 | 0.54 |
| Number of days taking analgesics (median (IQR)) | 0 | 0 (0) | 21 (56.8) |
| 1–2 | 19 (51.4) | 16 (43.2) | |
| >2 | 18 (48.6) | 0 (0) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Scaturro, D.; Vitagliani, F.; Terrana, P.; Cuntrera, D.; Falco, V.; Tomasello, S.; Letizia Mauro, G. Intra-Articular Hybrid Hyaluronic Acid Injection Treatment in Overweight Patients with Knee Osteoarthritis: A Single-Center, Open-Label, Prospective Study. Appl. Sci. 2021, 11, 8711. https://doi.org/10.3390/app11188711
Scaturro D, Vitagliani F, Terrana P, Cuntrera D, Falco V, Tomasello S, Letizia Mauro G. Intra-Articular Hybrid Hyaluronic Acid Injection Treatment in Overweight Patients with Knee Osteoarthritis: A Single-Center, Open-Label, Prospective Study. Applied Sciences. 2021; 11(18):8711. https://doi.org/10.3390/app11188711
Chicago/Turabian StyleScaturro, Dalila, Fabio Vitagliani, Pietro Terrana, Daniele Cuntrera, Vincenzo Falco, Sofia Tomasello, and Giulia Letizia Mauro. 2021. "Intra-Articular Hybrid Hyaluronic Acid Injection Treatment in Overweight Patients with Knee Osteoarthritis: A Single-Center, Open-Label, Prospective Study" Applied Sciences 11, no. 18: 8711. https://doi.org/10.3390/app11188711
APA StyleScaturro, D., Vitagliani, F., Terrana, P., Cuntrera, D., Falco, V., Tomasello, S., & Letizia Mauro, G. (2021). Intra-Articular Hybrid Hyaluronic Acid Injection Treatment in Overweight Patients with Knee Osteoarthritis: A Single-Center, Open-Label, Prospective Study. Applied Sciences, 11(18), 8711. https://doi.org/10.3390/app11188711