
Acoustic, Myoelectric, and Aerodynamic Parameters of Euphonic and Dysphonic Voices: A Systematic Review of Clinical Studies



Abstract
:1. Introduction
2. Materials and Methods
2.1. Eligibility Criteria
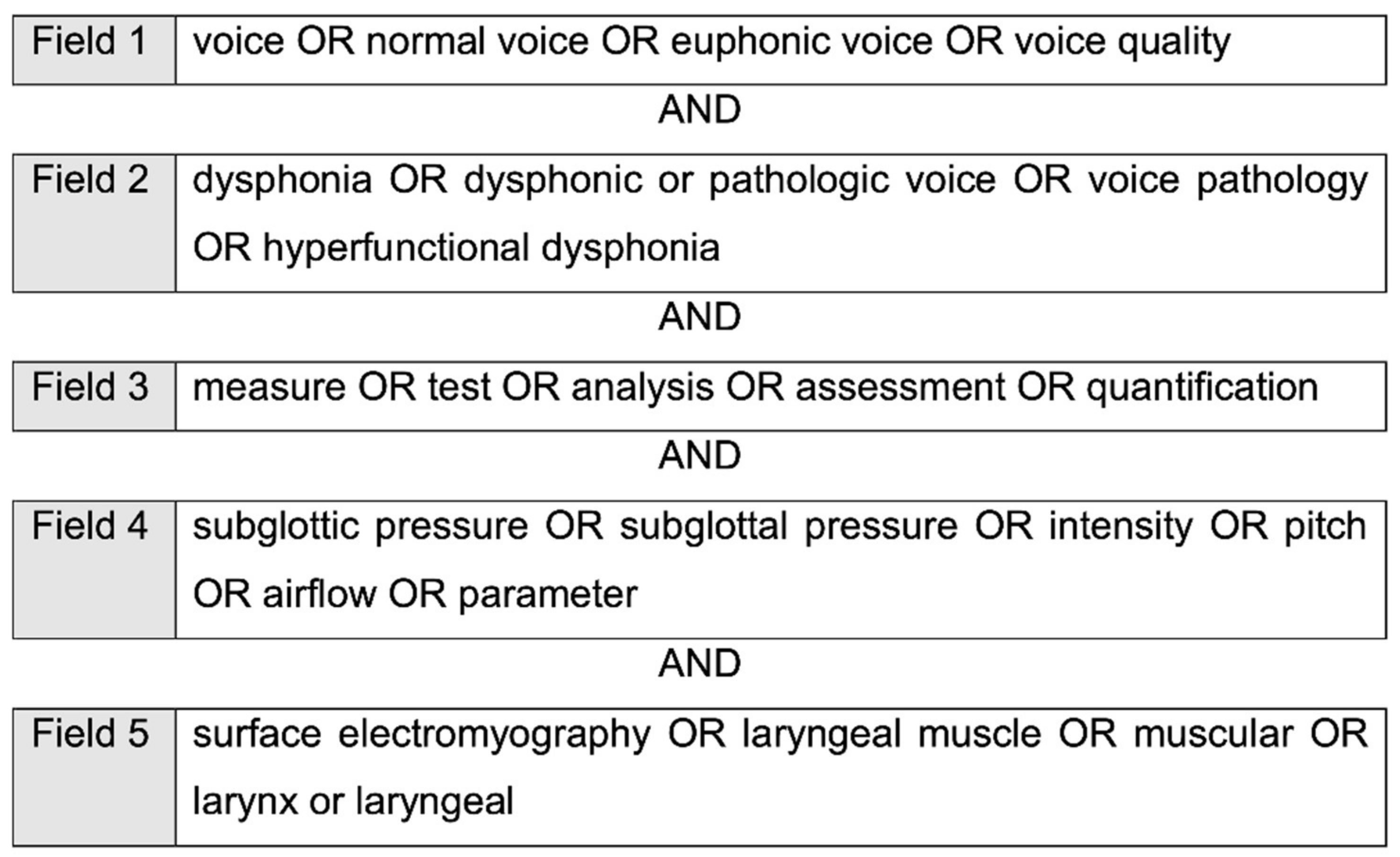
2.2. Search Strategy
2.3. Study Selection Process
2.4. Data Extraction
2.5. Quality Assessment
3. Results
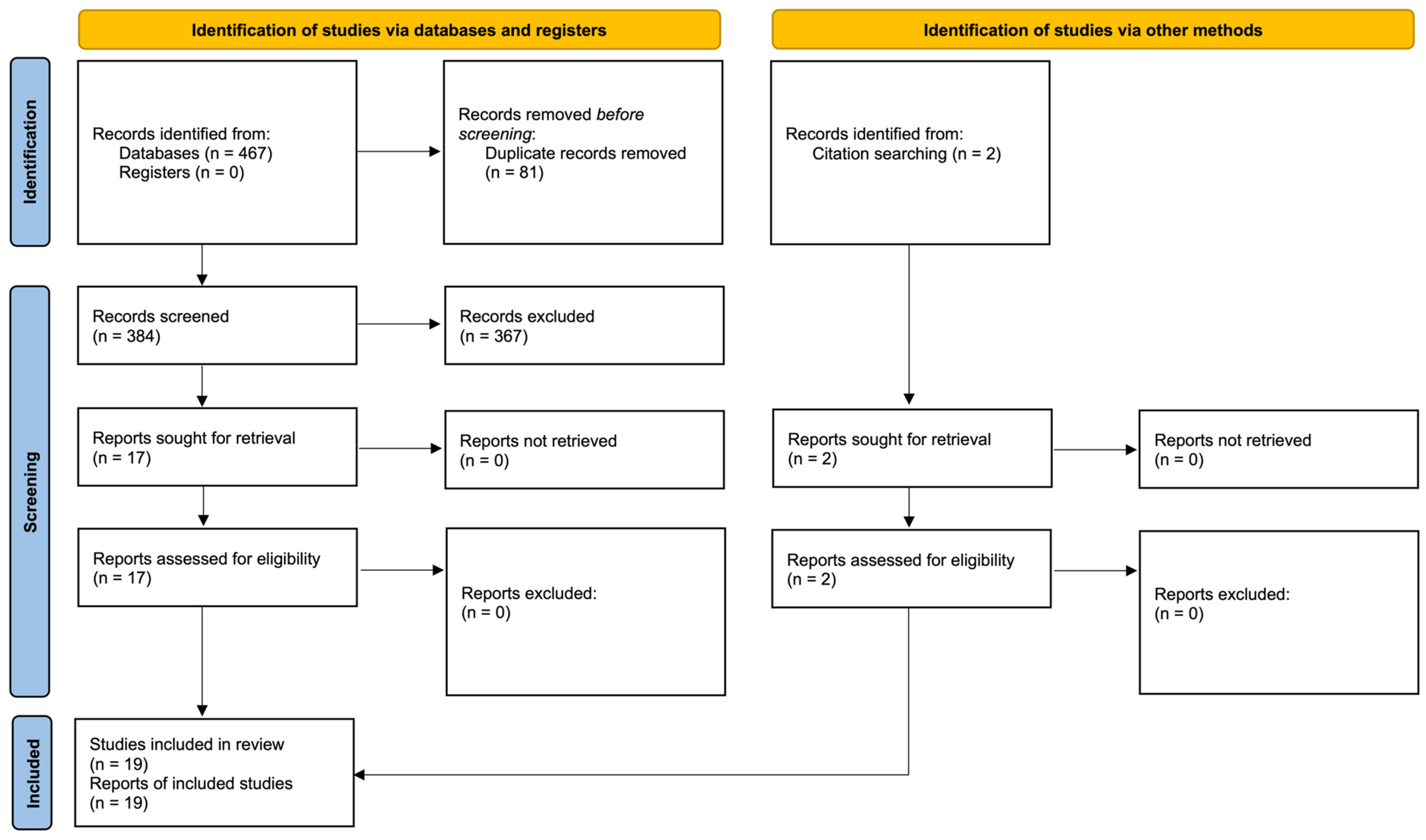
3.1. Search Results and Study Selection
3.2. Study Methodology
3.3. Study Results
3.4. Quality Assessment
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Behlau, M. The 2016 G. Paul Moore Lecture. Lessons in Voice Rehabilitation: Journal of Voice and Clinical Practice. J. Voice 2019, 33, 669–681. [Google Scholar] [CrossRef] [PubMed]
- Saggio, G.; Costantini, G. Worldwide Healthy Adult Voice Baseline Parameters: A Comprehensive Review. J. Voice 2020, in press. [Google Scholar] [CrossRef] [PubMed]
- Shewell, C. The effect of perceptual training on ability to use the vocal profile analysis scheme. Int. J. Lang. Commun. Disord. 1998, 33, 322–326. [Google Scholar] [CrossRef] [PubMed]
- Jackson-Menaldi, M.C. Aspectos generales para tener en cuenta en la evaluación de la voz y organización del laboratorio de voz. In La voz Normal y Patológica; Médica Panamericana: Buenos Aires, Argentina, 2019; pp. 204–217. [Google Scholar]
- Lee, L. Quick Screen for Voice and Supplementary Documents for Identifying Pediatric Voice Disorders. Language, Speech, and Hearing Services in Schools. Lang. Speech Hear. Serv. Sch. 2004, 35, 308–319. [Google Scholar] [CrossRef]
- Awan, S.N.; Roy, N.; Zhang, D.; Cohen, S.M. Validation of the Cepstral Spectral Index of Dysphonia (CSID) as a Screening Tool for Voice Disorders: Development of Clinical Cutoff Scores. J. Voice 2016, 30, 130–144. [Google Scholar] [CrossRef]
- Jannetts, S.; Schaeffler, F.; Beck, J.; Cowen, S. Assessing voice health using smartphones: Bias and random error of acoustic voice parameters captured by different smartphone types. Int. J. Lang. Commun. Disord. 2019, 54, 292–305. [Google Scholar] [CrossRef]
- Page, M.J.; McKenzie, J.E.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Akl, E.A.; Brennan, S.E.; et al. The PRISMA 2020 statement: An updated guideline for reporting systematic reviews. BMJ 2021, 372, n71. [Google Scholar] [CrossRef]
- Liberati, A.; Altman, D.G.; Tetzlaff, J.; Mulrow, C.; Gøtzsche, P.C.; Ioannidism, J.P.A.; Clarke, M.; Devereaux, P.J.; Kleijnen, J.; Moher, D. The PRISMA statement for reporting systematic reviews and meta-analyses of studies that evaluate healthcare interventions: Explanation and elaboration. BMJ 2009, 339, b2700. [Google Scholar] [CrossRef] [Green Version]
- Von Elm, E.; Altman, D.G.; Egger, M.; Pocock, S.J.; Gøtzsche, P.C.; Vandenbroucke, J.P. The Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) Statement: Guidelines for reporting observational studies. Int. J. Surg. 2014, 12, 1495–1499. [Google Scholar] [CrossRef] [Green Version]
- Murad, M.H.; Sultan, S.; Haffar, S.; Bazerbachi, F. Methodological quality and synthesis of case series and case reports. BMJ Evid. Based Med. 2018, 23, 60–63. [Google Scholar] [CrossRef] [Green Version]
- Casado, J.C.; Adrián, J.A.; Conde, M. Estudio objetivo de la voz en población normal y en la disfonía por nódulos y pólipos vocales. Acta Otorrinolaringol. Esp. 2001, 52, 476–482. [Google Scholar] [CrossRef]
- Yiu, E.M.L.; Yuen, Y.; Whitehill, T.; Winkworth, A. Reliability and applicability of aerodynamic measures in dysphonia assessment. Clin. Linguist. Phon. 2004, 18, 463–478. [Google Scholar] [CrossRef]
- Ma, E.P.M.; Yiu, E.M.L. Multiparametric Evaluation of Dysphonic Severity. J. Voice 2006, 20, 380–390. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Vaziri, G.; Almasganj, F.; Behroozmand, R. Pathological assessment of patients speech signals using nonlinear dynamical analysis. Comput. Biol. Med. 2010, 40, 54–63. [Google Scholar] [CrossRef] [PubMed]
- Petrović-Lazić, M.; Babac, S.; Vuković, M.; Kosanović, R.; Ivanković, Z. Acoustic Voice Analysis of Patients with Vocal Fold Polyp. J. Voice 2011, 25, 94–97. [Google Scholar] [CrossRef] [PubMed]
- Cantarella, G.; Baracca, G.; Pignataro, L.; Forti, S. Assessment of dysphonia due to benign vocal fold lesions by acoustic and aerodynamic indices: A multivariate analysis. Logop. Phoniatr. Vocol. 2011, 36, 21–27. [Google Scholar] [CrossRef] [PubMed]
- Zheng, Y.Q.; Zhang, B.R.; Su, W.Y.; Gong, J.; Yuan, M.Q.; Ding, Y.L.; Rao, S.Q. Laryngeal Aerodynamic Analysis in Assisting With the Diagnosis of Muscle Tension Dysphonia. J. Voice 2012, 26, 177–181. [Google Scholar] [CrossRef]
- Balata, P.M.M.; Silva, H.J.; Pernambuco, L.A.; Amorim, G.O.; Souto Maior Braga, R.; Fernandes Da Silva, E.G.; de Lima, L.M.; Arruda, S.R. Electrical Activity of Extrinsic Laryngeal Muscles in Subjects With and Without Dysphonia. J. Voice 2015, 29, 129.e9–129.e17. [Google Scholar] [CrossRef]
- Hemmerling, D.; Skalski, A.; Gajda, J. Voice data mining for laryngeal pathology assessment. Comput. Biol. Med. 2016, 69, 270–276. [Google Scholar] [CrossRef]
- Nemr, K.; Simões-Zenari, M.; De Souza, G.S.; Hachiya, A.; Tsuji, D.H. Correlation of the Dysphonia Severity Index (DSI), Consensus Auditory-Perceptual Evaluation of Voice (CAPE-V), and Gender in Brazilians With and Without Voice Disorders. J. Voice 2016, 30, 765.e7–765.e11. [Google Scholar] [CrossRef]
- Gilman, M.; Petty, B.; Maira, C.; Pethan, M.; Wang, L.; Hapner, E.R.; Johns, M.M., 3rd. Aerodynamic Patterns in Patients with Voice Disorders: A Retrospective Study. J. Voice 2017, 31, 545–549. [Google Scholar] [CrossRef]
- Shamila Rachel, S.; Snekhalatha, U.; Vedhasorubini, K.; Balakrishnan, D. Spectral Analysis of Speech Signal Characteristics: A Comparison between Healthy Controls and Laryngeal Disorder. In Advances in Intelligent Systems and Computing; Springer: Berlin/Heidelberg, Germany, 2018; Volume 632, pp. 333–341. [Google Scholar] [CrossRef]
- Brockmann-Bauser, M.; Bohlender, J.E.; Mehta, D.D. Acoustic Perturbation Measures Improve with Increasing Vocal Intensity in Individuals With and Without Voice Disorders. J. Voice 2018, 32, 162–168. [Google Scholar] [CrossRef] [Green Version]
- Brockmann-Bauser, M.; Van Stan, J.H.; Carvalho Sampaio, M.; Bohlender, J.E.; Hillman, R.E.; Mehta, D.D. Effects of Vocal Intensity and Fundamental Frequency on Cepstral Peak Prominence in Patients with Voice Disorders and Vocally Healthy Controls. J. Voice 2019, 35, 411–417. [Google Scholar] [CrossRef] [PubMed]
- Holmberg, E.B.; Doyle, P.; Perkell, J.S.; Hammarberg, B.; Hillman, R.E. Aerodynamic and acoustic voice measurements of patients with vocal nodules: Variation in baseline and changes across voice therapy. J. Voice 2003, 17, 269–282. [Google Scholar] [CrossRef]
- Aboras, Y.; El-Banna, M.; El-Magraby, R.; Ibrahim, A. The relationship between subjective self-rating and objective voice assessment measures. Logop. Phoniatr. Vocol. 2010, 35, 34–38. [Google Scholar] [CrossRef]
- Lopes, L.W.; Batista Simões, L.; Da Silva, D.J.; Da Silva Evangelista, D.; Da Nóbrega, A.C.; Oliveira Costa Silva, P.; Dias Vieira, V.J. Accuracy of Acoustic Analysis Measurements in the Evaluation of Patients With Different Laryngeal Diagnoses. J. Voice 2017, 31, 382.e15–382.e26. [Google Scholar] [CrossRef]
- Rosenthal, A.L.; Lowell, S.Y.; Colton, R.H. Aerodynamic and Acoustic Features of Vocal Effort. J. Voice 2014, 28, 144–153. [Google Scholar] [CrossRef] [Green Version]
- Björklund, S.; Sundberg, J. Relationship between Subglottal Pressure and Sound Pressure Level in Untrained Voices. J. Voice 2016, 30, 15–20. [Google Scholar] [CrossRef]
- Lee, S.J.; Cho, Y.; Song, J.Y.; Lee, D.; Kim, Y.; Kim, H. Aging Effect on Korean Female Voice: Acoustic and Perceptual Examinations of Breathiness. Folia Phoniatr. Logop. 2015, 67, 300–307. [Google Scholar] [CrossRef]
- Goozée, J.V.; Murdoch, B.E.; Theodoros, D.G.; Thompson, E.C. The effects of age and gender on laryngeal aerodynamics. Int. J. Lang. Commun. Disord. 2010, 33, 221–238. [Google Scholar] [CrossRef]
- Patel, R.R.; Awan, S.N.; Barkmeier-Kraemer, J.; Courey, M.; Deliyski, D.; Eadie, T.; Paul, D.; Švec, J.G.; Hillman, R. Recommended Protocols for Instrumental Assessment of Voice: American Speech-Language-Hearing Association Expert Panel to Develop a Protocol for Instrumental Assessment of Vocal Function. Am. J. Speech-Lang. Pathol. 2018, 27, 887–905. [Google Scholar] [CrossRef] [PubMed]

{kind=link}
{kind=link}
| Authors | Year | Sample Characteristics | Sample Size | Age Range | Gender | Voice Evaluation Techniques |
|---|---|---|---|---|---|---|
| Aboras et al. | 2010 | Volunteers with vocal pathology (100) | 100 | 25–55 | -- | VPSS; GRBAS Scale; MDVP; DSI; Aerophone II |
| Balata et al. | 2015 | Volunteers with (19) and without (22) vocal pathology | 41 | 28–57 | W: 36, M: 5 | VAS; Surface electromiography Miotool 200®; Miograph 2.0; Sennheiser PC-20 Microphone; VoxMetria 4.7; GRBAS Scale |
| Björklund and Sundberg | 2016 | Volunteers without vocal pathology | 31 | W: 26–36 M: 25–47 | W: 16, M: 15 | Pressure transducer; Sound card; Pressure gauge; Headset microphone DPA 4066-C; Sound level meter |
| Brockmann-Bauser et al. | 2019 | Volunteers with vocal pathology (58) [vocal nodules (39), vocal polyps (5) and without muscle tension dysphonia (14)] and without vocal pathology (58) | 116 | 18–64 | W | V-RQOL, CAPE-V; Koufman y Isaacson Scheme, modified by Amaral Catani; Sennheiser MKE104 Microphone; Praat |
| Brockmann-Bauser et al. | 2018 | Volunteers with vocal pathology (58) [vocal nodules (39), vocal polyps (5) and muscle tension dysphonia (14)] and without vocal pathology (58) | 116 | 18–64 | W | Koufman and Isaacson Scheme, modified by Amaral Catani; Sennheiser MKE104 Microphone; Pneumotachograph; Preamplifier; Praat |
| Cantarella et al. | 2011 | Volunteers with vocal pathology (53) [vocal nodules (3), vocal polyps (24), cysts (15), Reinke’s edema (11)] and without vocal pathology (39) | 92 | SG: 17–74 CG: 20–65 | SG: (W: 36, M: 17) CG: (W: 19, M: 20) | GRBAS Scale; AKG B29L Microphone; EVA system; Pneumotachograph |
| Casado Morente et al. | 2001 | Volunteers with vocal pathology (60) [vocal nodules (30), vocal polyps (30)] and without vocal pathology (100) | 160 | SG: (Nodules: 25–38), (Polyps: 19–42) CG: 20–40 | SG: (Nodules: W: 19, M: 11), (Polyps: W: 13, M: 17) CG: (W: 43, M: 57) | Telelaryngoscope; Fiberlaryngoscope; Stroboscope; Dr. Speech 3.0 Voice Assessment; Sound card; Professional microphone (600 ohms impedance) |
| Gilman et al. | 2017 | Volunteers with (192) and without (45) vocal pathology | 237 | SG: 19–86 CG: (W: 18–36, M: 17–30) | SG: (W: 133, M: 59) CG: (W: 20, M: 25) | PAS |
| Hemmerling et al. | 2016 | Volunteers with vocal pathology (705) [hyperfunctional dysphonia (213), vocal cord paralysis (213), other pathologies (279) and without vocal pathology (705) | 1.410 | -- | SG: (W: 450, M: 255) CG: (W: 450, M: 255) | SVD |
| Holmberg et al. | 2003 | Volunteers with vocal pathology [vocal nodules (10)] | 10 | W: 19–35 | W: 10 | Microphone (Sony ECM 50); Pressure system (Glottal Enterprises) |
| Lopes et al. | 2017 | Volunteers with vocal pathology [vocal nodules (93 without structural alterations (64), vocal cyst (34), reflux vocal alteration (27), polyps (17), posterior hiatus (18), vocal paralysis (10), sulcus vocalis (8), Reinke’s edema (8)] | 279 | W: 18–65 | W: 279 | FonoView 4.5; Sennheiser 835 Microphone; VoxMetria; Sound ForSG Pro 10.0; Matlab 7.9 |
| Ma and Yiu | 2006 | Volunteers with (112) and without (41) vocal pathology | 153 | 20–55 | SG: (W: 93, M: 19) CG: (W: 35, M: 6) | CSL 4300B; MDVP; Shure Beta 87 Microphone; GRBAS Scale; Interobservers evaluation; Phog 1.0; Aerophone II |
| Nemr et al. | 2006 | Volunteers with (24) and without (42) vocal pathology | 66 | 20–83 | SG: (W: 17, M: 7) CG: (W: 25, M: 17) | Audacity®; AKG 520 Microphone; CAPE-V; Praat |
| Petrović-Lazić et al. | 2011 | Volunteers with (46 [vocal polyps]) and without (21) vocal pathology | 67 | SG: (W: 18–61) CG: (W: 21–61) | SG: (W: 46) CG: (W: 21) | MDVP; Sennheiser E825S Microphone; SPSS |
| Rachel et al. | 2018 | Volunteers with (10) and without (10) vocal pathology | 20 | -- | -- | Proton BOOM815 Recorder; Praat; Dr. Speech |
| Rosenthal et al. | 2014 | Volunteers without vocal pathology (18) | 18 | 18–26 | (W: 12, M: 6) | CAPE-V; CSL 4500; Glottal Enterprises MS100-A2; Microphone (Tascam DR-2d Linear PCM) |
| Vaziri et al. | 2010 | Volunteers with (329) and without (58) vocal pathology | 387 | -- | SG: (W: 188, M: 141) CG: (W: 36, M: 22) | APQ; PPQ; CD; LLE; ApEn; FD; ZL |
| Yiu et al. | 2004 | Volunteers with vocal pathology [vocal hyperfunction (28): vocal edema (1); vocal polyp (2); vocal cord thickening (10); vocal nodules (16)] and without pathology (28) | 56 | 20–50 SG: 33.25 ± 9.70 CG: 33.39 ± 9.43 | SG: (W: 28) CG: (W: 28) | Aerophone II |
| Zheng et al. | 2012 | Volunteers with (26) –muscle tension dysphonia- and without (27) vocal pathology | 53 | SG: 18–56 CG: 20–56 | SG: (W: 18, M: 8) CG: (W: 18, M: 9) | MDVP; PAS |
| Authors | Year | Acoustic Measurements | Aerodynamic Parameters | Myoelectric Parameters | Phonatory Tasks | |||||
|---|---|---|---|---|---|---|---|---|---|---|
| SM | QOM | OM | AP | W/T | WO/T | OM | N° Channels | |||
| Aboras et al. | 2010 | VPSS | GRBAS scale | MDVP; DSI | Shim; APQ; NHR | MPT | SGP | -- | -- | -- |
| Balata et al. | 2015 | -- | VAS; GRBAS scale | -- | F0; Intensity | -- | -- | Electrical potentials: SH and IH muscles | 3 | Maintained vowel /ε/ and counting numbers (20–30) with a comfortable and maximum intensities |
| Björklund and Sundberg | 2016 | -- | -- | -- | F0; Intensity | -- | Intraoral pressure; SGP | -- | -- | Syllable [pa] repetition with different intensities and with the same frequency |
| Brockmann-Bauser et al. | 2019 | V-RQOL | CAPE-V | -- | F0; Intensities: minimum, maximum and normal; CPPS | -- | -- | -- | -- | Maintained vowel /a/ with comfortable minimum and maximum intensities |
| Brockmann-Bauser et al. | 2018 | -- | -- | -- | F0; Intensity; Jitter; Shim; HNR | -- | -- | -- | -- | Maintained vowel /a/ with comfortable minimum and maximum intensities |
| Cantarella et al. | 2011 | -- | GRBAS scale | -- | Jitter; Shim; CV F0; CV I; HNR | MPT | SGP; OAF; OA CV; GL; GEI; LE; OAF*P | -- | -- | Maintained vowel /a/ with comfortable intensity and frequency. Words, sentences and conversations repeated |
| Casado Morente et al. | 2001 | -- | -- | -- | Jitter; Shim; NNE (dB); HNR (dB); SNR (dB); F0 | -- | -- | -- | -- | Maintained vowel /a/ with comfortable intensity and frequency |
| Gilman et al. | 2017 | -- | -- | -- | -- | -- |
| -- | -- | Maintained vowel /a/ (comfortable frequency and intensity; Syllable [pa] |
| Hemmerling et al. | 2016 | -- | -- | -- | F0; Jitter; Shim; 1st, 2nd, 3rd formants; MFCC | -- | -- | -- | -- | Maintained vowels /a/, /i/, /u/ with minimum, normal and maximum, frequency |
| Holmberg et al. | 2003 | -- | -- | -- | Intensity; F0; H1; H2; F1; F3 | -- | Intraoral air pressure; OAF; Transglottal air pressure; ACflow; Closed quotient; Speed quotient; Maximum flow declination rate | -- | -- | Maintained vowel /a/ and syllable [pa] with comfortable and maximum intensity |
| Lopes et al. | 2017 | -- | -- | FonoView 4.5 | F0; Jitter; Shim; GNE | -- | -- | -- | -- | Maintained vowel /ε/ with comfortable frequency and intensity |
| Ma and Yiu | 2006 | - | GRBAS | Phonetogram | Minimum and maximum F0; Maximum and minimum intensity; Jitter; Shim; NHR | MPT | Phonatory airflow Air pressure Intraoral pressure | -- | -- | Sentences with comfortable and maximum intensity; Maintained vowel /a/ with maximum and minimum intensity and frequency; Maintained vowels /i/, /u/ with comfortable frequency and intensity; Syllable [pi] |
| Nemr et al. | 2016 | -- | CAPE-V | DSI | F0 max; I min | -- | -- | -- | -- | Maintained vowel /a/ at comfortable and increasing F0; Maintained vowel /a/ at comfortable intensity and decreasing |
| Petrović-Lazić et al. | 2011 | -- | -- | MDVP | vF0; Jitter; Shim; NHR; VTI; PPQ; APQ | -- | -- | -- | -- | Maintained vowel /a/ at comfortable frequency |
| Rachel et al. | 2018 | -- | -- | Praat; Dr. Speech | F0; F0 tremor; Jitter; Shim; HNR; SNR | -- | -- | -- | -- | Maintained vowel /a/ |
| Rosenthal et al. | 2014 | -- | CAPE-V | CSL | F0 | -- | Oral air pressure; OAF; SGP; TLF; Translaryngeal resistance; MFDR | -- | -- | Syllable [pi] with different levels of vocal effort; Sentences |
| Vaziri et al. | 2010 | -- | -- | Vocal samples from Kay Elemetrics Corporation database (model 4337, v 1.03) | F0; PPQ; APQ | -- | -- | -- | -- | Maintained vowel /a/; Lecture |
| Yiu et al. | 2004 | -- | -- | -- | -- | MPT | Intraoral pressure; SGP; Airflow rate | -- | -- | Long vowels (/a/, /i/, /u/) as many time as possible with comfortable tone and volume; Syllable [pi]; Sentences |
| Zheng et al. | 2012 | -- | -- | MDVP model 5105 | Jitter; Shim; PPQ; APQ | MPT | SGP; GR; MFR | -- | -- | Maintained vowel /a/ with comfortable frequency and intensity; Syllable [pa] |
| Author | Year | Vocal Registry | Aerodynamic Registry | Electromyographic Registry | ||||||
|---|---|---|---|---|---|---|---|---|---|---|
| Microphone | MMD | Hardware | Software | Hardware and Tools | Software | Hardware | Software | Material | ||
| Aboras et al. | 2010 | -- | -- | -- | MDVP | -- | Aerophone II Model 6800 | -- | -- | |
| Balata et al. | 2015 | Sennheiser PC-20 | 3 cm | Sony Vaio | VoxMetria 4.7h | -- | -- | Miotool 200®; SDS500 Sensors; LG notebook | Miograph 2.0; Windowa Vista Premium; Butterworth digital filter | MEDITRACE Pediatric electrodes |
| Björklund and Sundberg | 2016 | DPA 4066-C | 12 cm | Symetrix SX202 Preamplifier; TEAC RD 200 PCM Sound card; Ono Sokki LA 210 Sound level meter | Soundswell program | Pressure transdiucer (Glottal Enterprises 162); TEAC RD 200 PMC Sound card; Pressure gauge | Soundswell program; Swellcal Module | -- | -- | -- |
| Brockmann-Bauser et al. | 2019 | Sennheiser MKE104 | 10 cm | Symetrix SX302 Preamplifier; CyberAmp 380 electronic preconditioning; Voltage range: ±10V Digitada 1440A | Praat 5.4.1.4 | Rothenberg’s Mask | -- | -- | -- | -- |
| Brockmann-Bauser et al. | 2018 | Sennheiser MKE104 | 10 cm | Symetrix SX302 Preamplifier; CyberAmp 380 electronic preconditioning; Voltage range: ±10V Digitada 1440A | Praat 5.4.1.4 | -- | -- | -- | -- | -- |
| Cantarella et al. | 2011 | AKG B29L | 5 cm | -- | EVA System | Rothenberg’s Mask | -- | -- | -- | -- |
| Casado Morente et al. | 2001 | Professional microphonel (impedance: 600 ohms) | 15 cm 45° angle | Richard Wolf de 70° Telelaringoscope; Machida ENT-30P-III Fibrolaringoscope; Fiegert Endotech CCD CD5131 Color camera; Super VHS; Richard Wolf 5012 Estrobosocope with cool light source; Pentium personal computer; Sound Blaster-Pro Sound car | “Voice Assessment” from Dr. Speech Science 3.0 software | -- | -- | -- | -- | -- |
| Gilman et al. | 2017 | -- | -- | -- | -- | -- | PAS | -- | -- | -- |
| Hemmerling et al. | 2016 | -- | -- | -- | Vocal database (SVD) | -- | -- | -- | -- | -- |
| Holmberg et al. | 2003 | Sony ECM50 | 15 cm | -- | -- | -- | -- | -- | -- | -- |
| Lopes et al. | 2017 | Sennheiser 835 | 10 cm | Dell all-in-one desktop; Preamplifierr U Phoria UMC 204 | FonoView 4.5; VoxMetria 4.7h; Sound FOrge 10.0 | -- | -- | -- | -- | -- |
| Ma and Yiu | 2006 | Shure Beta 87 | 10 cm | -- | MDVP CSL Phog 1.0 | -- | Aerophone II model 6800 | -- | -- | -- |
| Nemr et al. | 2016 | AKG 520 | 10 cm 30° angle | Desktop computer with USB 5.1 3D; Edirol UA-101 Sound card; Class B external digital amplifier; Sound level meter (Center model 322) | Audacity® Praat | -- | -- | -- | -- | -- |
| Petrović-Lazić et al. | 2011 | Sennheiser E825S | 5 cm | Laptop HACER ICK 70 | MDVP CSL | -- | -- | -- | -- | -- |
| Rachel et al. | 2018 | BOOM815 Recorder; Microphone with NX Audio sound cable | 5 cm | -- | Praat 6.022 Dr. Speech 4 Matlab | -- | -- | -- | -- | -- |
| Rosenthal et al. | 2014 | Micro condenser inside a Tascam DR-2d recorder | 8 cm | Sound level meter | CSL | Rothenberg’s Mask | Glottal Enterprises MS100-A2 with MCU-4 calibration Unit; TF32 | -- | -- | -- |
| Vaziri et al. | 2010 | DAT | -- | -- | Kay Elemetrics Corporation (model 4337, v 1.03) | -- | -- | -- | -- | -- |
| Yiu et al. | 2004 | -- | -- | -- | -- | Rothenberg’s Mask | Aerophone II model 6800 | -- | -- | -- |
| Zheng et al. | 2012 | -- | -- | -- | -- | Rothenberg’s Mask | Kay Elemetrics Phonatory Aerodynamic System (model 6600 | -- | -- | -- |
| Author | Year | Group | Acoustic Parameters | ||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Frequency | Intensity | Perturbation parameters | |||||||||||||||
| F0 | Max F0 | Min F0 | Intensity | Max I | Min I | CPPS | Jitt | Shim | HNR | NHR | VTI | PPQ | APQ | GNE | |||
| Aboras et al. | 2010 | SG | -- | -- | -- | -- | -- | -- | -- | -- | 3.653 | 2.703 | -- | -- | -- | 2.449 | -- |
| Balata et al. | 2015 | CG | 194.66 ± 7.59 | 262.52 ± 12.48 | -- | 68.74 ± 1.23 | 83.38 ± 0.94 | -- | -- | - | -- | -- | -- | - | - | - | - |
| SG | 195.08 ± 14.10 | 244.77 ± 10.88 | -- | 64.20 ± 1.05 | 79.54 ± 1.36 | -- | -- | - | - | - | - | - | - | - | - | ||
| Brockmann-Bauser et al. | 2019 | CG | 249.2 | 266.6 | 244.1 | 87.7 | 95.8 | 81.1 | 16 | -- | -- | -- | -- | -- | - | -- | -- |
| SG | 243.3 | 253.4 | 248.4 | 88.0 | 95.9 | 79.5 | 15.6 | -- | -- | -- | -- | -- | -- | -- | -- | ||
| Brockmann-Bauser et al. | 2018 | CG | 249.2 | 266.6 | 244.1 | 87.7 | 95.8 | 81.1 | -- | Min: 0.38 | 2.66 | 25.1 | -- -- -- | -- -- -- | - -- - | -- -- -- | -- -- -- |
| Comf: 0.30 | 1.65 | 27.7 | |||||||||||||||
| Max: 0.24 | 1.19 | 29.8 | |||||||||||||||
| SG | 243.3 | 253.4 | 248.4 | 88.0 | 95.9 | 79.5 | -- | Min: 0.41 | 2.74 | 24.4 | -- | -- | -- | -- | -- | ||
| Comf: 0.32 | 1.97 | 26.5 | |||||||||||||||
| Max: 0.24 | 1.32 | 29.4 | |||||||||||||||
| Cantarella et al. | 2011 | CG | CV F0: 0.79 ± 0.28 | CV I: 0.92 ± 0.32 | -- | 0.45 ± 0.22 | 0.26 ± 0.14 | 20.61 ± 2.96 | -- | -- | -- | -- | -- | ||||
| SG | CV F0: 2.32 ±s 3.21 | CV I: 1.20 ±0.50 | -- | 2.15 ± 4.70 | 0.96 ± 0.92 | 14.62 ± 7.00 | -- | -- | -- | -- | -- | ||||||
| Holmberg et al. | 2003 | SG | 207 ± 20.2 | 245 ± 29.6 | -- | 83 ± 2.9 | 92 ± 3.2 | -- | -- | - | -- | -- | -- | -- | -- | -- | -- |
| Lopes et al. | 2017 | CG | 201.87 ± 27.39 | -- | -- | -- | -- | -- | -- | 0.27± 0.16 | 5.22± 2.84 | -- | -- | -- | -- | -- | 0.81± 0.18 |
| SG | 194.24 ± 47.23 | -- | -- | -- | -- | -- | -- | 1.54± 2.58 | 8.22± 6.88 | -- | -- | -- | -- | -- | 0.70± 0.20 | ||
| Ma and Yiu | 2006 | CG | 216.03 ± 34.09 | 1141.35 ± 311.38 | 40.08 ± 4.87 | -- | 105.24 ±6.32 | 48.71 ±3.12 | -- | -- | 6.25± 7.58 | -- | 0.24 ±0.04 | -- | -- | 0.98 ±0.38 | -- |
| SG | 196.72 ± 38.01 | 832.19 ± 266.51 | 120.04 ± 25.81 | -- | 109.29 ±6.08 | 60.78 ±7.25 | -- | -- | 9.71± 3.66 | -- | 0.24 ±0.07 | -- | -- | 1.81 ±0.99 | -- | ||
| Nemr et al. | 2016 | CG | 452.9 ± 101.0 | -- | -- | -- | -- | 55.2 ± 4.4 | -- | 0.38 ± 0.24 | -- | -- | -- | -- | -- | -- | -- |
| SG | 449.1 ± 90.2 | -- | -- | -- | -- | 58.4 ± 4.9 | -- | 1.04 ± 0.84 | -- | -- | -- | -- | -- | -- | -- | ||
| Petrović-Lazić et al. | 2011 | CG | CV F0: 1.117 ± 0.439 | -- | -- | -- | -- | 0.509 ± 0.168 | 1.845 ± 0.439 | -- | -- | 0.044 ± 0.014 | 0.319 ± 0.148 | 1.102 ± 0.365 | -- | ||
| SG | CV F0: 2.096 ± 1.241 | -- | -- | -- | -- | 1.986 ± 1.387 | 5.647 ± 2.457 | -- | -- | 0.065 ± 0.027 | 1.191 ± 0.850 | 4.156 ± 2.156 | -- | ||||
| Rachel et al. | 2018 | CG | 180.25 ± 62.99 | -- | -- | -- | -- | -- | -- | 0.463 ± 0.377 | (in dB) 0.384 ± 0.443 | 20.34 ± 5.57 | -- | -- | -- | -- | -- |
| SG | 201.23 ± 67.9 | -- | -- | -- | -- | -- | -- | 0.64 ± 0.574 | (in dB) 4.225 ± 3.24 | 20.51 ± 6.29 | -- | -- | -- | -- | -- | ||
| Vaziri et al. | 2010 | CG | -- | -- | -- | -- | -- | -- | -- | -- | -- | -- | -- | -- | 0.3229 ± 0.0673 | 1.4698 ± 0.7359 | -- |
| SG | -- | -- | -- | -- | -- | -- | -- | -- | -- | -- | -- | -- | 1.3904 ± 4.2573 | 4.8993 ± 11.7756 | -- | ||
| Author | Year | Group | Aerodynamic Parameters | |||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| MPT | SGP | OAF | OA CV | GL | TGI | LE | MFR | TGP | SQ | CQ | MFDR | TLF | GR | |||
| Aboras et al. | 2010 | SG | 4.019 | -- | -- | -- | -- | -- | -- | -- | -- | -- | -- | -- | -- | -- |
| Björklund and Sundberg | 2016 | CG | -- | W: 78.1 M: 80.0 | -- | -- | -- | -- | -- | -- | -- | -- | -- | -- | -- | -- |
| Cantarella et al. | 2011 | CG | 19.90 ± 6.93 | 12.05 ± 4.51 | 144.86 ± 58.36 | 6.64 ± 5.20 | 1.87 ± 0.78 | 10.62 ± 3.26 | 88.69 ± 84.05 | -- | -- | -- | -- | -- | -- | -- |
| SG | 11.52 ± 5.54 | 8.31 ± 2.64 | 213.70 ± 156.24 | 6.43 ± 6.66 | 2.85 ± 2.00 | 7.41 ± 2.62 | 43.76 ± 45.37 | -- | -- | -- | -- | -- | -- | -- | ||
| Gilman et al. | 2017 | CG | -- | -- | 6.3 ± 1.4 | -- | -- | -- | -- | 0.19 ± 0.07 | -- | -- | -- | -- | -- | -- |
| SG | -- | -- | 7.78 ± 3.17 | -- | -- | -- | -- | 0.17 ± 0.12 | -- | -- | -- | -- | -- | -- | ||
| Holmberg et al. | 2003 | SG | -- | -- | -- | -- | -- | -- | -- | 0.31 ±0.09 | 11.0 ± 3.7 | 2.6 ± 0.4 | 40.4 ± 3.5 | 502 ±129 | -- | -- |
| Ma and Yiu | 2006 | CG | [a]: 22.90 ±8.86 [i]: 24.45 ±8.79 [u]: 23.06± 9.05 | [pi]: 9.75± 1.85 Sentence: 7.71± 1.72 | -- | -- | -- | -- | -- | [a]: 0.11 ± 0.04 [i]: 0.11 ± 0.04 [u]: 0.12 ± 0.05 | -- | -- | -- | -- | -- | -- |
| SG | [a]: 15.29 ± 7.79 [i]: 16.45 ± 7.64 [u]: 15.40 ± 6.67 | [pi]: 16.95 ± 5.49 Sentence: 12.32 ± 4.13 | -- | -- | -- | -- | -- | [a]: 0.15 ± 0.08 [i]: 0.14 ± 0.08 [u]: 0.17 ± 0.09 | -- | -- | -- | -- | -- | -- | ||
| Nemr et al. | 2016 | CG | 17.4 ± 5.4 | -- | -- | -- | -- | -- | -- | -- | -- | -- | -- | -- | -- | -- |
| SG | 11.1 ± 5.5 | -- | -- | -- | -- | -- | -- | -- | -- | -- | -- | -- | -- | -- | ||
| Rosenthal et al. | 2014 | CG | Comfortable | 7.03 ± 2.33 | -- | -- | -- | -- | -- | -- | -- | -- | -- | 319.91 ± 194.30 | 174.87 ± 68.06 | -- |
| Maximum | 10.19 ± 4.55 | -- | -- | -- | -- | -- | -- | -- | -- | -- | 540.96 ± 331.79 | 236.55 ± 60.00 | -- | |||
| Minimum | 5.37 ± 1.10 | -- | -- | -- | -- | -- | -- | -- | -- | -- | 229.61 ± 115.18 | 202.72 ± 79.78 | -- | |||
| Zheng et al. | 2012 | CG | W: 23.36 ± 4.84 | 5.71 ± 1.49 | -- | -- | -- | -- | -- | 0.08 ± 0.04 | -- | -- | -- | -- | -- | 78.17 ± 58.50 |
| M: 25.74 ± 9 59 | 5.94 ± 1.26 | -- | -- | -- | -- | -- | 0.11 ± 0.04 | -- | -- | -- | -- | -- | 36.14 ± 22.15 | |||
| SG | W: 12.3 ± 4.61 | 10.47 ± 3.51 | -- | -- | -- | -- | -- | 0.06 ± 0.04 | -- | -- | -- | -- | -- | 180.85 ± 285.67 | ||
| M: 15.5 ± 6.47 | 10.25 ± 2.69 | -- | -- | -- | -- | -- | 0.07 ± 0.04 | -- | -- | -- | -- | -- | 63.98 ± 21.30 | |||
| Author | STROBE Checklist Items for Study Title, Abstract, Introduction and Methodology | |||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| 1a | 1b | 2 | 3 | 4 | 5 | 6a | 6b | 7 | 8 | 9 | 10 | 11 | 12a | 12b | 12c | 12d | 12e | |
| Aboras et al., 2010 | N | Y | Y | Y | Y | N | N | - | Y | Y | N | N | Y | Y | N | N | - | N |
| Balata et al., 2015 | N | Y | Y | Y | Y | N | Y | - | Y | Y | Y | N | Y | Y | Y | N | - | N |
| Björklund & Sundberg et al., 2016 | N | Y | Y | Y | Y | N | N | - | Y | Y | Y | N | Y | Y | Y | N | - | N |
| Brockmann-Bauser et al., 2019 | Y | Y | Y | Y | Y | N | Y | - | Y | Y | Y | N | Y | Y | Y | N | - | N |
| Brockmann-Bauser et al., 2018 | Y | Y | Y | Y | Y | N | Y | - | Y | Y | Y | N | Y | Y | Y | N | - | N |
| Cantarella et al., 2011 | Y | Y | Y | Y | Y | N | Y | - | Y | Y | Y | N | Y | Y | Y | N | - | N |
| Casado et al., 2001 | Y | Y | Y | Y | Y | N | Y | - | Y | Y | N | N | Y | Y | Y | N | - | N |
| Gillman et al., 2017 | Y | Y | Y | Y | Y | Y | Y | - | Y | Y | N | N | Y | Y | Y | N | - | N |
| Lopes et al., 2017 | N | Y | Y | N | Y | N | Y | - | Y | Y | Y | N | Y | Y | Y | N | - | Y |
| Ma & Yiu et al., 2006 | N | Y | Y | Y | Y | N | Y | - | Y | Y | Y | N | Y | Y | Y | N | - | N |
| Nemr et al., 2006 | N | Y | Y | Y | Y | N | Y | - | Y | Y | N | N | Y | Y | Y | N | - | N |
| Petrović-Lazić et al., 2011 | N | Y | Y | Y | Y | N | Y | - | Y | Y | N | N | Y | Y | Y | N | - | N |
| Rachel et al., 2018 | Y | Y | Y | Y | Y | N | Y | - | Y | Y | N | N | Y | N | N | N | - | N |
| Rosenthal et al., 2014 | Y | Y | Y | Y | Y | N | Y | - | Y | Y | N | N | Y | Y | Y | N | - | N |
| Yiu et al., 2004 | N | Y | Y | Y | Y | N | Y | - | Y | Y | N | N | Y | Y | Y | N | - | N |
| Zheng et al., 2012 | N | Y | Y | Y | Y | N | Y | - | Y | Y | N | N | Y | Y | Y | N | - | N |
| Author | STROBE Checklist Items for Study Results and Discussion | |||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| 13a | 13b | 13c | 14a | 14b | 14c | 15 | 16a | 16b | 16c | 17 | 18 | 19 | 20 | 21 | 22 | |
| Aboras et al., 2010 | N | N | N | N | N | - | Y | Y | - | N | N | Y | N | Y | N | N |
| Balata et al., 2015 | N | N | N | N | N | - | Y | Y | - | N | N | Y | Y | Y | Y | Y |
| Björklund & Sundberg et al., 2016 | N | N | N | N | N | - | Y | Y | - | N | N | Y | Y | Y | Y | Y |
| Brockmann-Bauser et al., 2019 | N | N | N | N | N | - | Y | Y | - | N | N | Y | Y | Y | Y | Y |
| Brockmann-Bauser et al., 2018 | N | N | N | N | N | - | Y | Y | - | N | N | Y | Y | Y | Y | Y |
| Cantarella et al., 2011 | N | N | N | N | N | - | Y | Y | - | N | N | Y | Y | Y | Y | Y |
| Casado et al., 2001 | N | N | N | N | N | - | Y | Y | - | N | Y | Y | Y | Y | Y | Y |
| Gillman et al., 2017 | N | N | N | N | N | - | Y | Y | - | N | Y | Y | Y | Y | Y | Y |
| Lopes et al., 2017 | Y | Y | Y | N | N | - | Y | Y | - | N | Y | Y | Y | Y | Y | Y |
| Ma & Yiu et al., 2006 | N | N | N | N | N | - | Y | Y | - | N | N | Y | N | Y | Y | Y |
| Nemr et al., 2006 | N | N | N | N | N | - | Y | Y | - | N | N | Y | Y | Y | Y | Y |
| Petrović-Lazić et al., 2011 | N | N | N | N | N | - | Y | Y | - | N | N | Y | N | Y | Y | Y |
| Rachel et al., 2018 | N | N | N | N | N | - | Y | Y | - | N | N | Y | N | Y | Y | Y |
| Rosenthal et al., 2014 | N | N | N | N | N | - | Y | Y | - | N | N | Y | Y | Y | Y | Y |
| Yiu et al., 2004 | N | N | N | N | N | - | Y | Y | - | N | N | Y | Y | Y | Y | Y |
| Zheng et al., 2012 | N | N | N | N | N | - | Y | Y | - | N | N | Y | Y | Y | Y | Y |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Puig-Herreros, C.; Sanz, J.L.; Barona, L.; Rosell-Clari, V. Acoustic, Myoelectric, and Aerodynamic Parameters of Euphonic and Dysphonic Voices: A Systematic Review of Clinical Studies. Appl. Sci. 2021, 11, 8191. https://doi.org/10.3390/app11178191
Puig-Herreros C, Sanz JL, Barona L, Rosell-Clari V. Acoustic, Myoelectric, and Aerodynamic Parameters of Euphonic and Dysphonic Voices: A Systematic Review of Clinical Studies. Applied Sciences. 2021; 11(17):8191. https://doi.org/10.3390/app11178191
Chicago/Turabian StylePuig-Herreros, Clara, José Luis Sanz, Luz Barona, and Vicent Rosell-Clari. 2021. "Acoustic, Myoelectric, and Aerodynamic Parameters of Euphonic and Dysphonic Voices: A Systematic Review of Clinical Studies" Applied Sciences 11, no. 17: 8191. https://doi.org/10.3390/app11178191
APA StylePuig-Herreros, C., Sanz, J. L., Barona, L., & Rosell-Clari, V. (2021). Acoustic, Myoelectric, and Aerodynamic Parameters of Euphonic and Dysphonic Voices: A Systematic Review of Clinical Studies. Applied Sciences, 11(17), 8191. https://doi.org/10.3390/app11178191