
Anatomical Characteristics of the Lateral Pterygoid Muscle in Mandibular Prognathism





Abstract
:1. Introduction
2. Materials and Methods
2.1. Participants
2.2. Group Classification
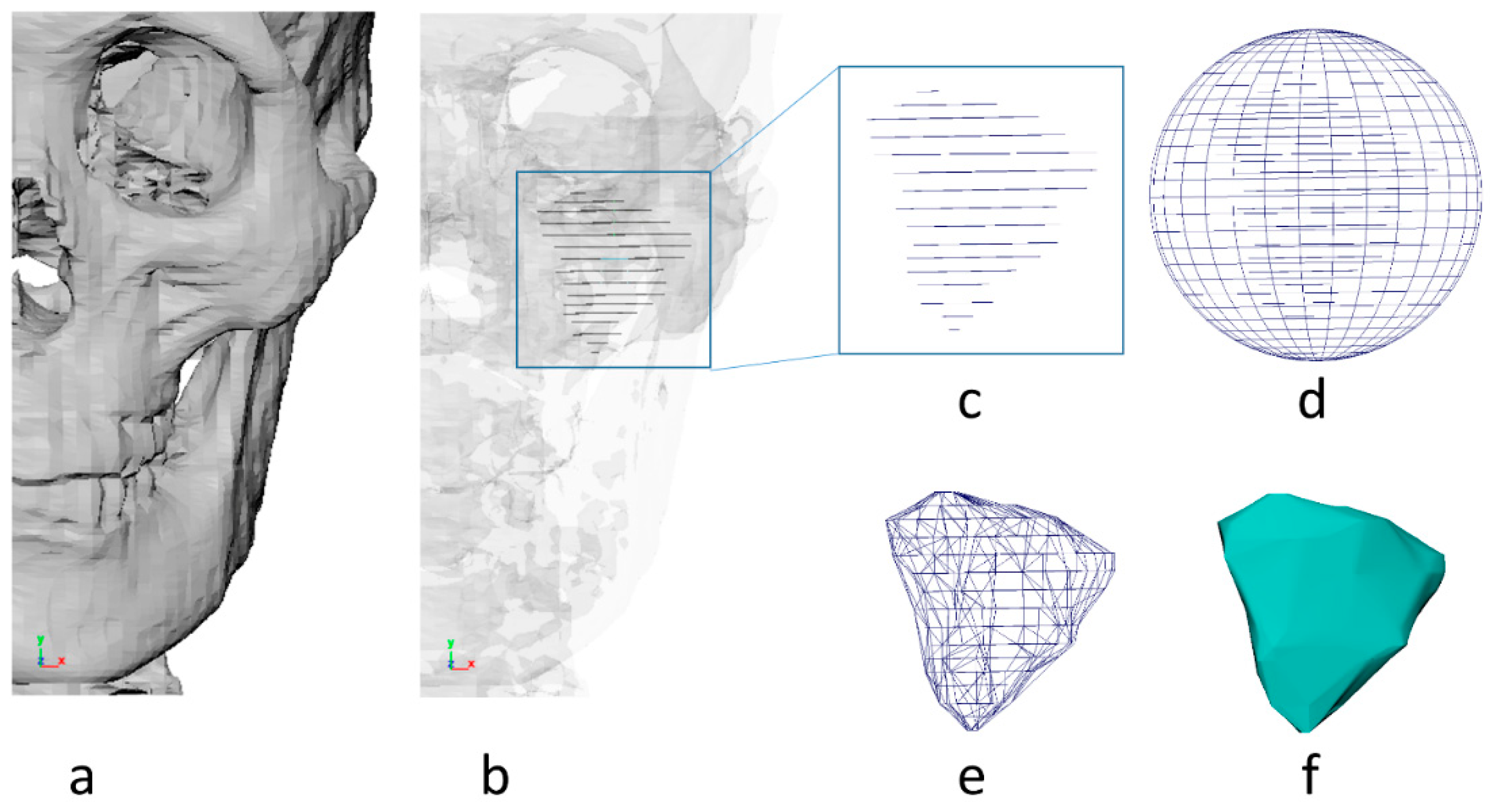
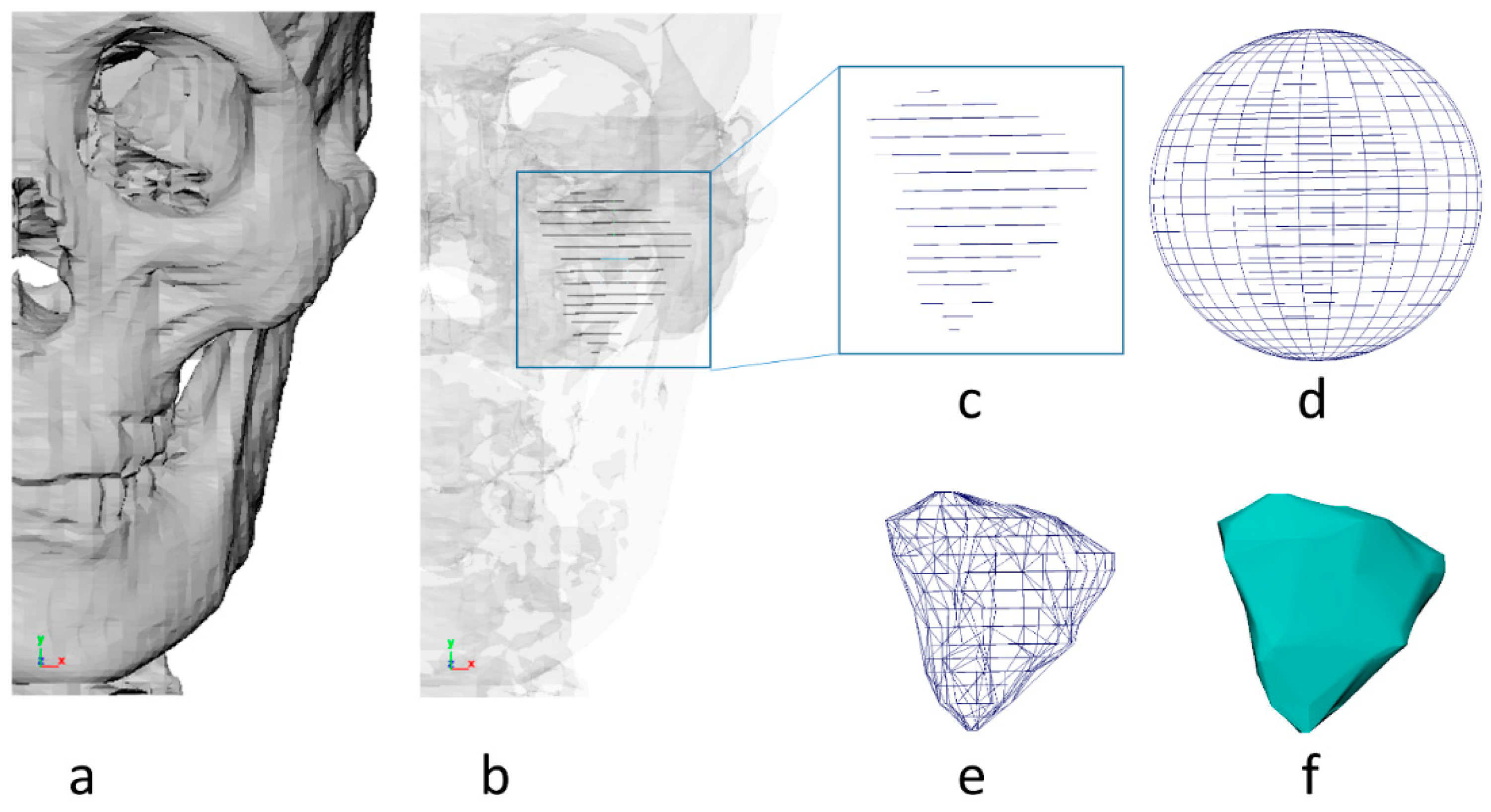
2.3. 3D CT Segmentation
2.4. 3D Reconstruction and Correction
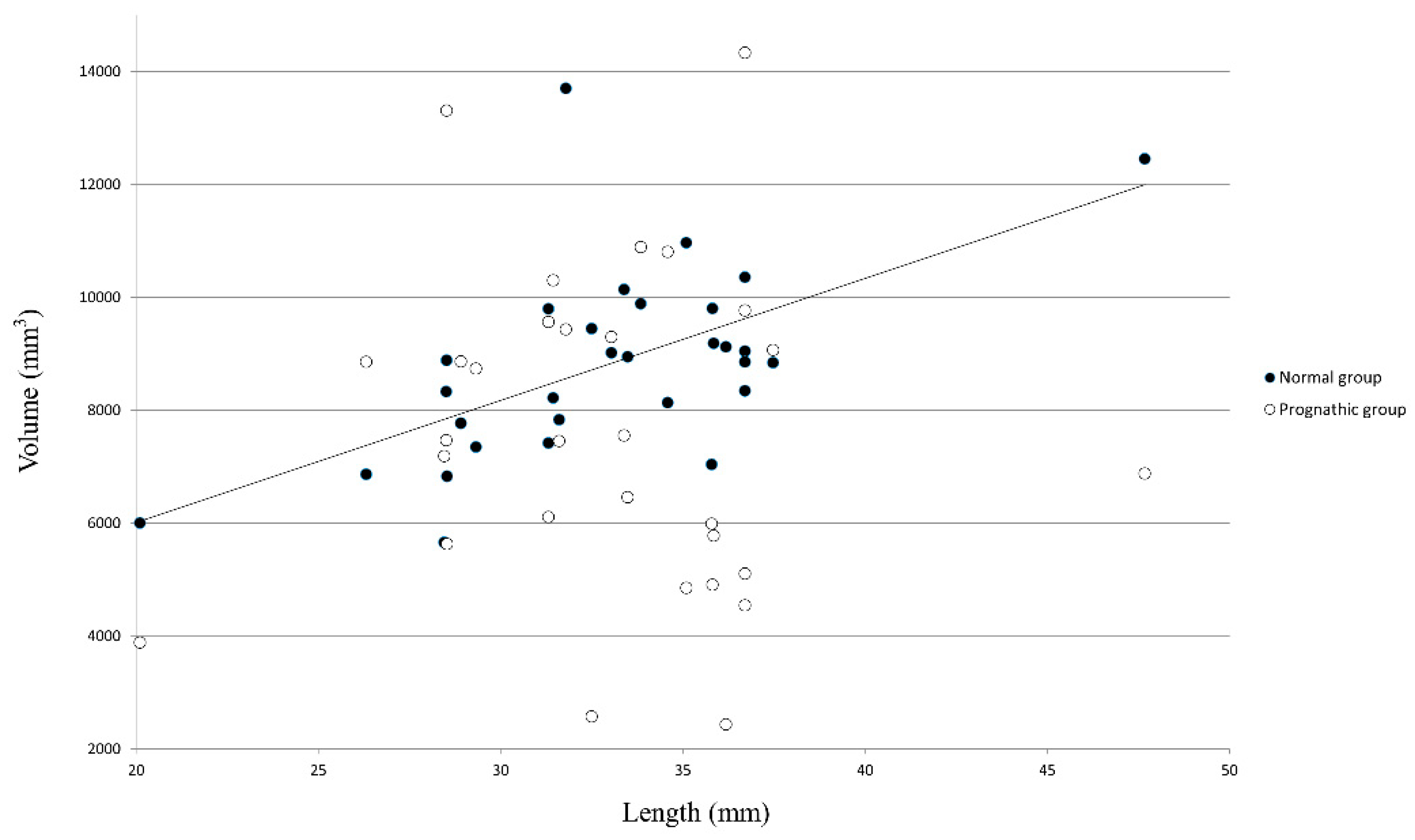
2.5. Volume and Length Calculation for Lateral Pterygoid
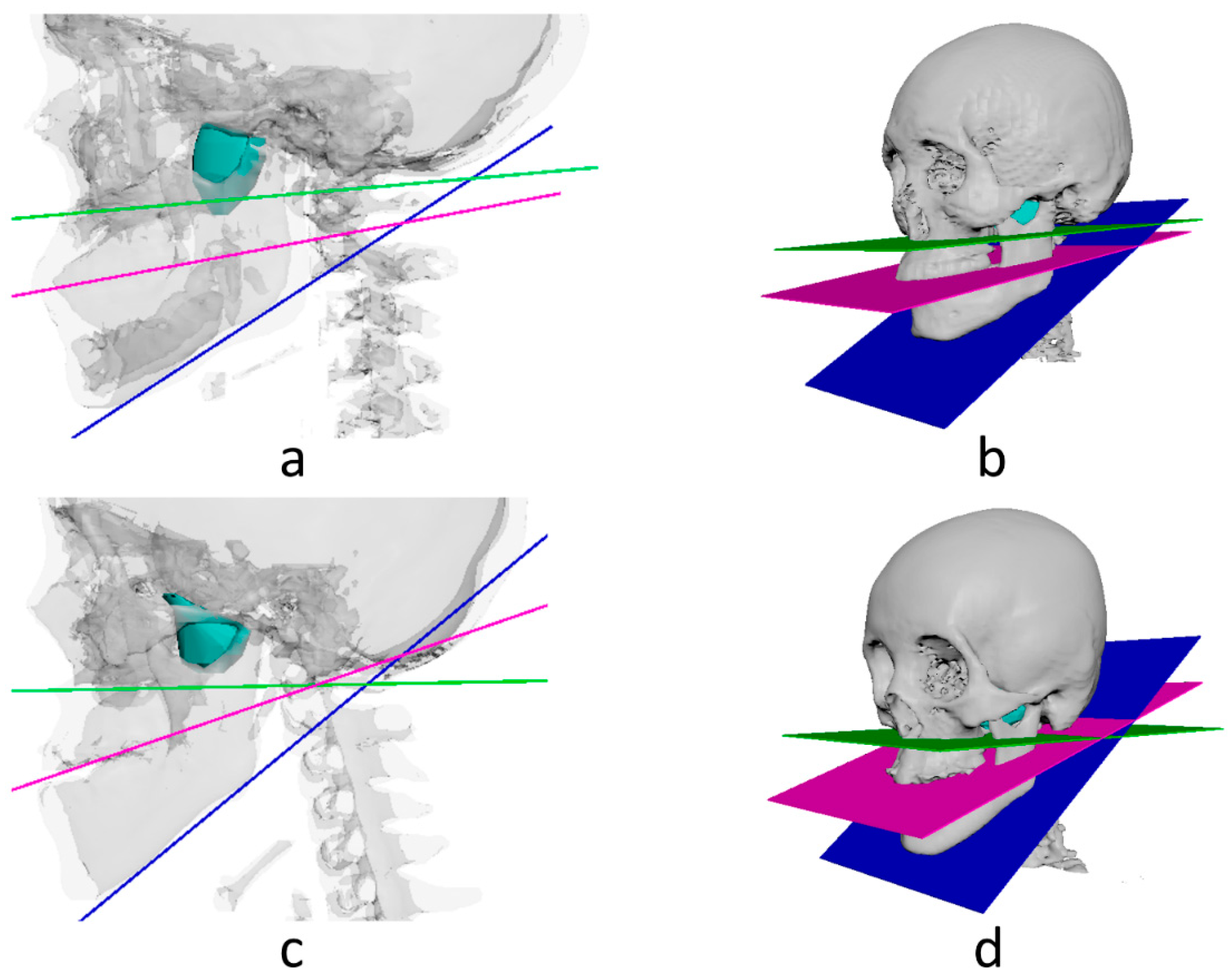
2.6. Angle Calculation between Lateral Pterygoid and Reference Planes
- −
- Midsagittal plane: the plane through falx cerebri, foramen cecum, and center of foramen magnum [12].
- −
- Horizontal plane: the plane through midpoints of both orbital canal and both eyeballs [13].
- −
- Palatal plane: plane perpendicular to midsagittal plane passing through posterior and anterior nasal spine [14].
- −
- Occlusal plane: a plane through the midpoint between incisal edges of upper/lower jaw incisors and mesio-buccal cusp tip of bilateral first molars on mandible [15].
- −
- Mandibular plane: plane perpendicular to midsagittal plane passing through Me (menton) and Go (gonion) [16].
2.7. Method Error
2.8. Statistic Verification
3. Results
3.1. Method Error
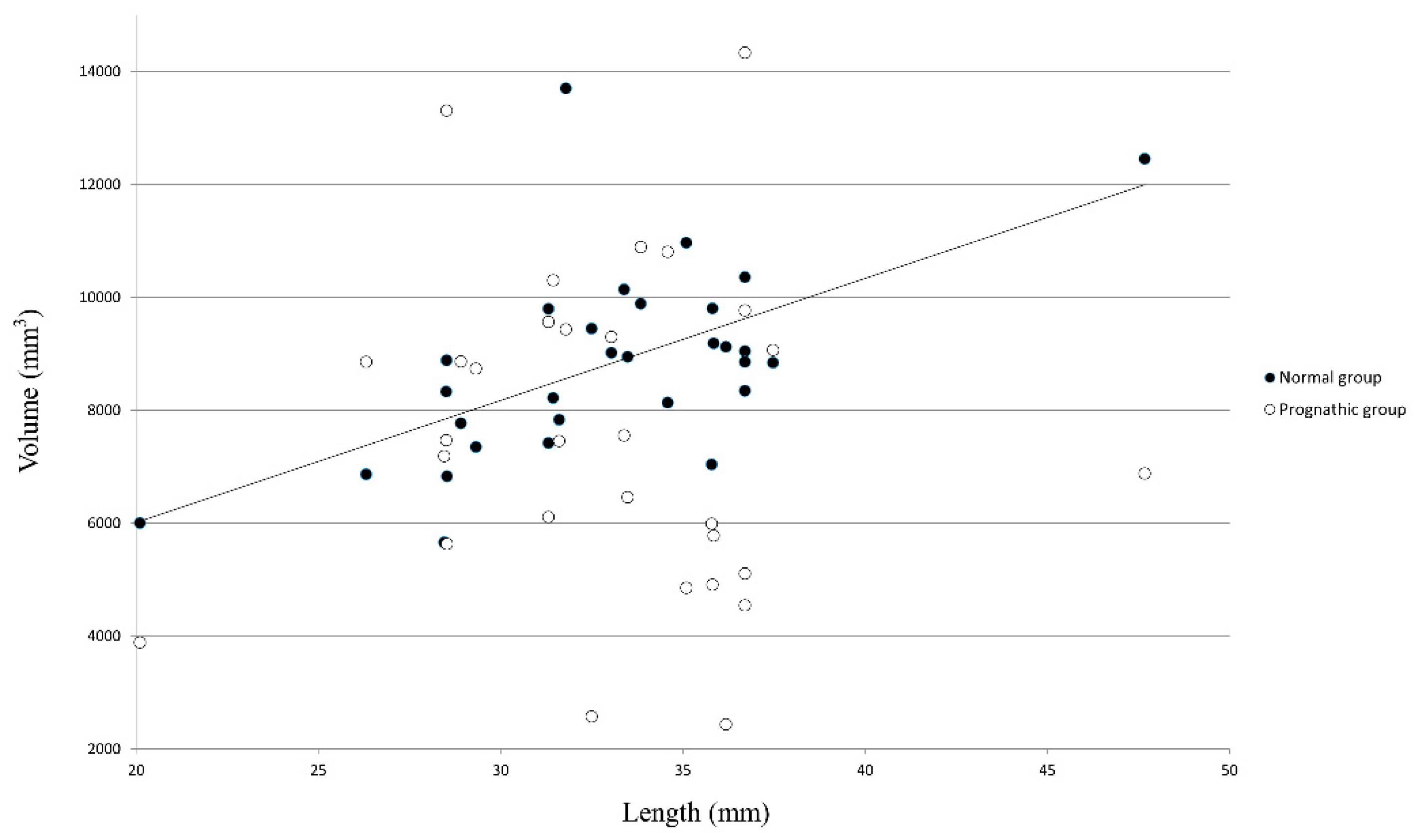
3.2. Comparison of Lateral Pterygoid Ratio between Prognathic and Normal Groups
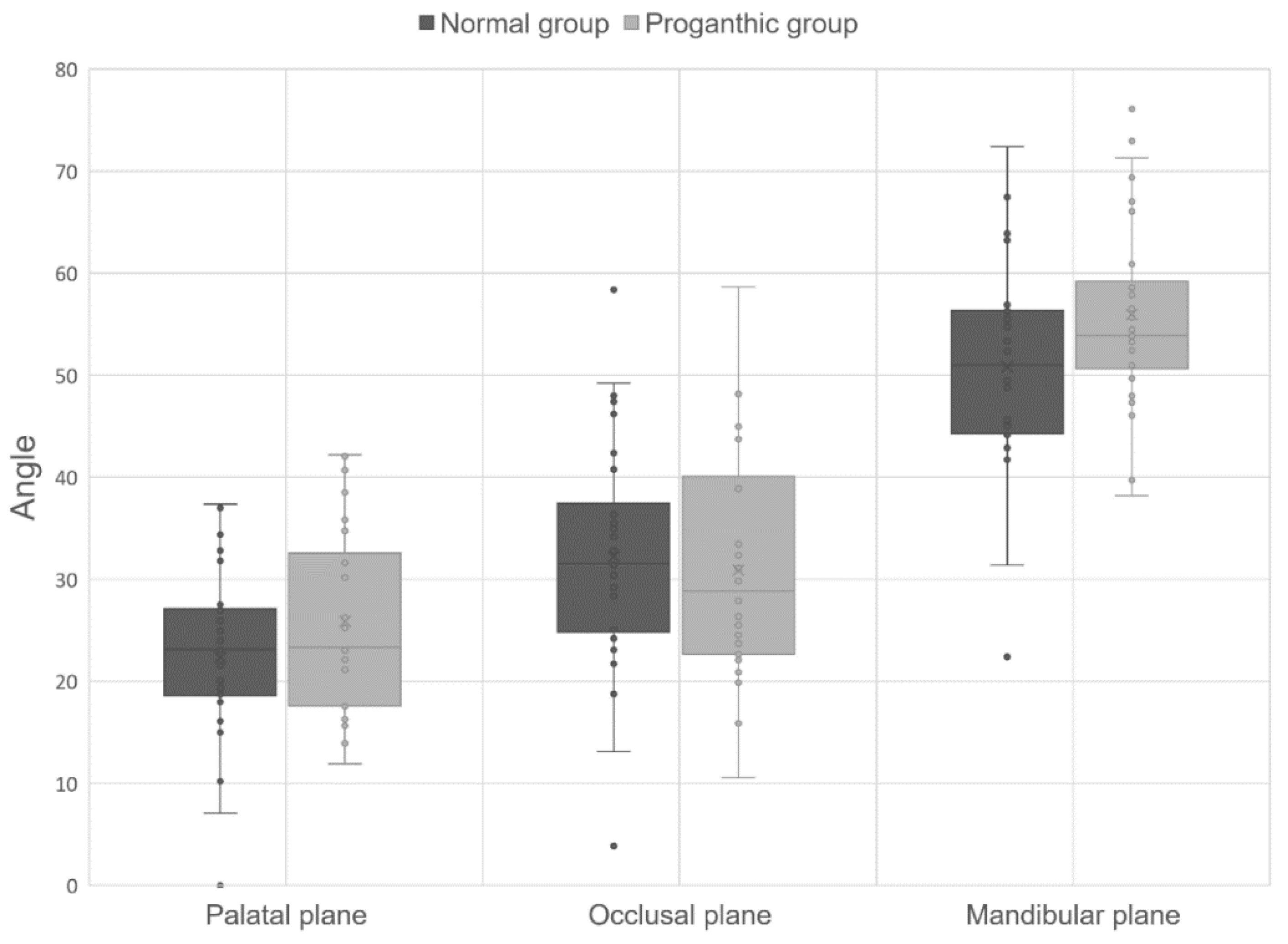
3.3. Comparison of Orientation Angles of Lateral Pterygoid to Three Reference Planes
4. Discussion
5. Conclusions
- (1)
- The volume/length ratio of the lateral pterygoid in the normal group was larger than that in the prognathic group.
- (2)
- The orientation of the angle between the lateral pterygoid and palatal/mandibular plane showed a more horizontal tendency for the normal group than for the prognathic group.
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Kim, K.-J.; Park, J.H.; Chang, N.-Y.; Kim, B.C.; Chae, J.-M. Hemimandibular hyperplasia treatment with condylectomy and orthodontic camouflage treatment using miniplate. Am. J. Orthod. Dentofac. Orthop. Off. Publ. Am. Assoc. Orthod. Its Const. Soc. Am. Board Orthod. 2021, 159, 852–865. [Google Scholar]
- Park, J.C.; Lee, J.; Lim, H.J.; Kim, B.C. Rotation tendency of the posteriorly displaced proximal segment after vertical ramus osteotomy. J. Cranio-Maxillo-Facial Surg. Off. Publ. Eur. Assoc. Cranio-Maxillo-Facial Surg. 2018, 46, 2096–2102. [Google Scholar] [CrossRef] [PubMed]
- Woon, S.C.; Thiruvenkatachari, B. Early orthodontic treatment for class iii malocclusion: A systematic review and meta-analysis. Am. J. Orthod. Dentofac. Orthop. Off. Publ. Am. Assoc. Orthod. Its Const. Soc. Am. Board Orthod. 2017, 151, 28–52. [Google Scholar] [CrossRef] [PubMed]
- Ngan, P.; Moon, W. Evolution of class iii treatment in orthodontics. Am. J. Orthod. Dentofac. Orthop. Off. Publ. Am. Assoc. Orthod. Its Const. Soc. Am. Board Orthod. 2015, 148, 22–36. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ginszt, M.; Zieliński, G.; Berger, M.; Szkutnik, J.; Bakalczuk, M.; Majcher, P. Acute effect of the compression technique on the electromyographic activity of the masticatory muscles and mouth opening in subjects with active myofascial trigger points. Appl. Sci. 2020, 10, 7750. [Google Scholar] [CrossRef]
- Costa, Y.M.; Exposto, F.G.; Castrillon, E.E.; Conti, P.C.R.; Bonjardim, L.R.; Svensson, P. Local anaesthesia decreases nerve growth factor induced masseter hyperalgesia. Sci. Rep. 2020, 10, 15458. [Google Scholar] [CrossRef] [PubMed]
- Heyat, M.B.B.; Akhtar, F.; Khan, A.; Noor, A.; Benjdira, B.; Qamar, Y.; Abbas, S.J.; Lai, D. A novel hybrid machine learning classification for the detection of bruxism patients using physiological signals. Appl. Sci. 2020, 10, 7410. [Google Scholar] [CrossRef]
- Stutzmann, J.J.; Petrovic, A.G. Role of the lateral pterygoid muscle and meniscotemporomandibular frenum in spontaneous growth of the mandible and in growth stimulated by the postural hyperpropulsor. Am. J. Orthod. Dentofac. Orthop. Off. Publ. Am. Assoc. Orthod. Its Const. Soc. Am. Board Orthod. 1990, 97, 381–392. [Google Scholar] [CrossRef]
- Mun, S.H.; Park, M.; Lee, J.; Lim, H.J.; Kim, B.C. Volumetric characteristics of prognathic mandible revealed by skeletal unit analysis. Ann. Anat.-Anat. Anz. Off. Organ Anat. Ges. 2019, 226, 3–9. [Google Scholar] [CrossRef] [PubMed]
- Yang, J.H.; Shin, D.S.; Yoo, J.-H.; Lim, H.J.; Lee, J.; Kim, B.C. Anatomical characteristics of the masseter muscle in mandibular prognathism. Appl. Sci. 2021, 11, 4444. [Google Scholar] [CrossRef]
- Lee, S.H.; Kil, T.J.; Park, K.R.; Kim, B.C.; Kim, J.G.; Piao, Z.; Corre, P. Three-dimensional architectural and structural analysis—A transition in concept and design from delaire’s cephalometric analysis. Int. J. Oral Maxillofac. Surg. 2014, 43, 1154–1160. [Google Scholar] [CrossRef] [PubMed]
- Kim, H.-J.; Kim, B.C.; Kim, J.-G.; Zhengguo, P.; Kang, S.H.; Lee, S.-H. Construction and validation of the midsagittal reference plane based on the skull base symmetry for three-dimensional cephalometric craniofacial analysis. J. Craniofacial Surg. 2014, 25, 338–342. [Google Scholar] [CrossRef] [PubMed]
- Kang, Y.H.; Kim, B.C.; Park, K.R.; Yon, J.Y.; Kim, H.J.; Tak, H.; Piao, Z.; Kim, M.K.; Lee, S.H. Visual pathway-related horizontal reference plane for three-dimensional craniofacial analysis. Orthod. Craniofacial Res. 2012, 15, 245–254. [Google Scholar] [CrossRef] [PubMed]
- Nahoum, H.I. Vertical proportions and the palatal plane in anterior open-bite. Am. J. Orthod. 1971, 59, 273–282. [Google Scholar] [CrossRef]
- Del Santo, M., Jr. Influence of occlusal plane inclination on anb and wits assessments of anteroposterior jaw relationships. Am. J. Orthod. Dentofac. Orthop. 2006, 129, 641–648. [Google Scholar] [CrossRef] [PubMed]
- Nelson, C.; Harkness, M.; Herbison, G.P. Mandibular changes during functional appliance treatment. Am. J. Orthod. Dentofac. Orthop. 1993, 104, 153–161. [Google Scholar] [CrossRef]
- Tecco, S.; Cattoni, F.; Darvizeh, A.; Bosco, F.; Sanci, V.; Nota, A.; Gastaldi, G.; Gherlone, E.F. Evaluation of masticatory muscle function using digital versus traditional techniques for mockup fabrication: A controlled prospective study. Appl. Sci. 2020, 10, 6013. [Google Scholar] [CrossRef]
- Stöckle, M.; Fanghänel, J.; Knüttel, H.; Alamanos, C.; Behr, M. The morphological variations of the lateral pterygoid muscle: A systematic review. Ann. Anat. 2019, 222, 79–87. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rathee, M.; Jain, P. Anatomy, Head and Neck, Lateral Pterygoid Muscle. In StatPearls [Internet]; StatPearls Publishing: Treasure Island, FL, USA, 2021; Updated 13 February 2021; Available online: https://www.ncbi.nlm.nih.gov/books/NBK549799/ (accessed on 28 August 2021).



{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Prognathic Group (n = 30) | Normal Group (n = 30) | p Value | |
|---|---|---|---|
| Ratio | 231.8 ± 58.5 | 268.5 ± 42.6 | 0.000 * |
| Prognathic Group (n = 30) | Normal Group (n = 30) | p Value | ||
|---|---|---|---|---|
| Lateral pterygoid | Palatal plane | 25.9 ± 8.8° | 22.4 ± 8.2° | 0.04 * |
| Occlusal plane | 30.9 ± 11.0° | 32.2 ± 11.3° | 0.34 | |
| Mandibular plane | 56.0 ± 9.0° | 50.8 ± 10.6° | 0.02 * |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kim, H.; Shin, D.; Kang, J.; Kim, S.; Lim, H.; Lee, J.; Kim, B. Anatomical Characteristics of the Lateral Pterygoid Muscle in Mandibular Prognathism. Appl. Sci. 2021, 11, 7970. https://doi.org/10.3390/app11177970
Kim H, Shin D, Kang J, Kim S, Lim H, Lee J, Kim B. Anatomical Characteristics of the Lateral Pterygoid Muscle in Mandibular Prognathism. Applied Sciences. 2021; 11(17):7970. https://doi.org/10.3390/app11177970
Chicago/Turabian StyleKim, Hwikang, Dongsun Shin, Jaehyun Kang, Seewoon Kim, Hunjun Lim, Jun Lee, and Bongchul Kim. 2021. "Anatomical Characteristics of the Lateral Pterygoid Muscle in Mandibular Prognathism" Applied Sciences 11, no. 17: 7970. https://doi.org/10.3390/app11177970
APA StyleKim, H., Shin, D., Kang, J., Kim, S., Lim, H., Lee, J., & Kim, B. (2021). Anatomical Characteristics of the Lateral Pterygoid Muscle in Mandibular Prognathism. Applied Sciences, 11(17), 7970. https://doi.org/10.3390/app11177970