
Intraosseous Squamous Cell Carcinoma Associated with Denosumab-Induced Osteonecrosis of the Jaw


 ,
,  , ,
, , {kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Abstract
:1. Introduction
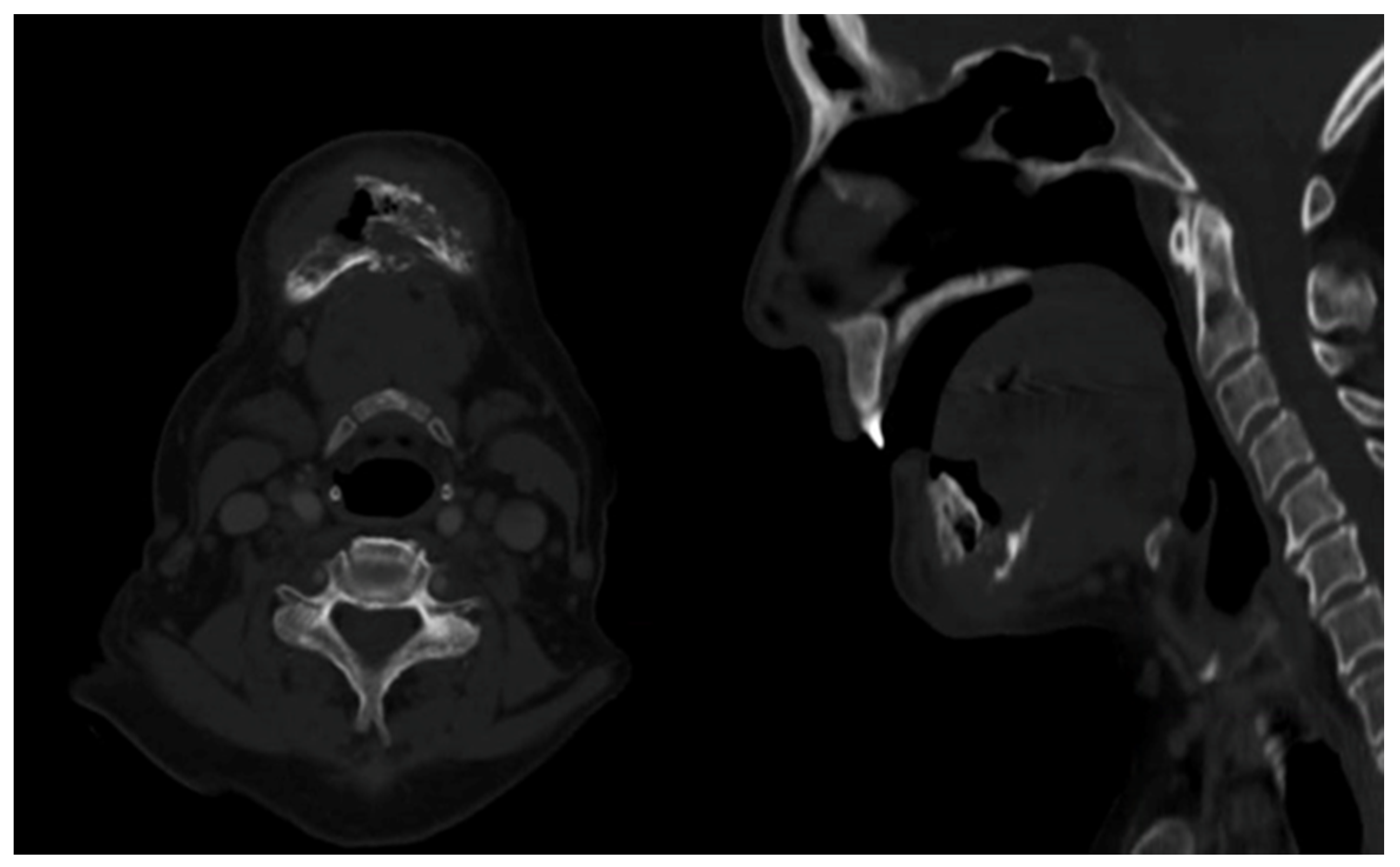
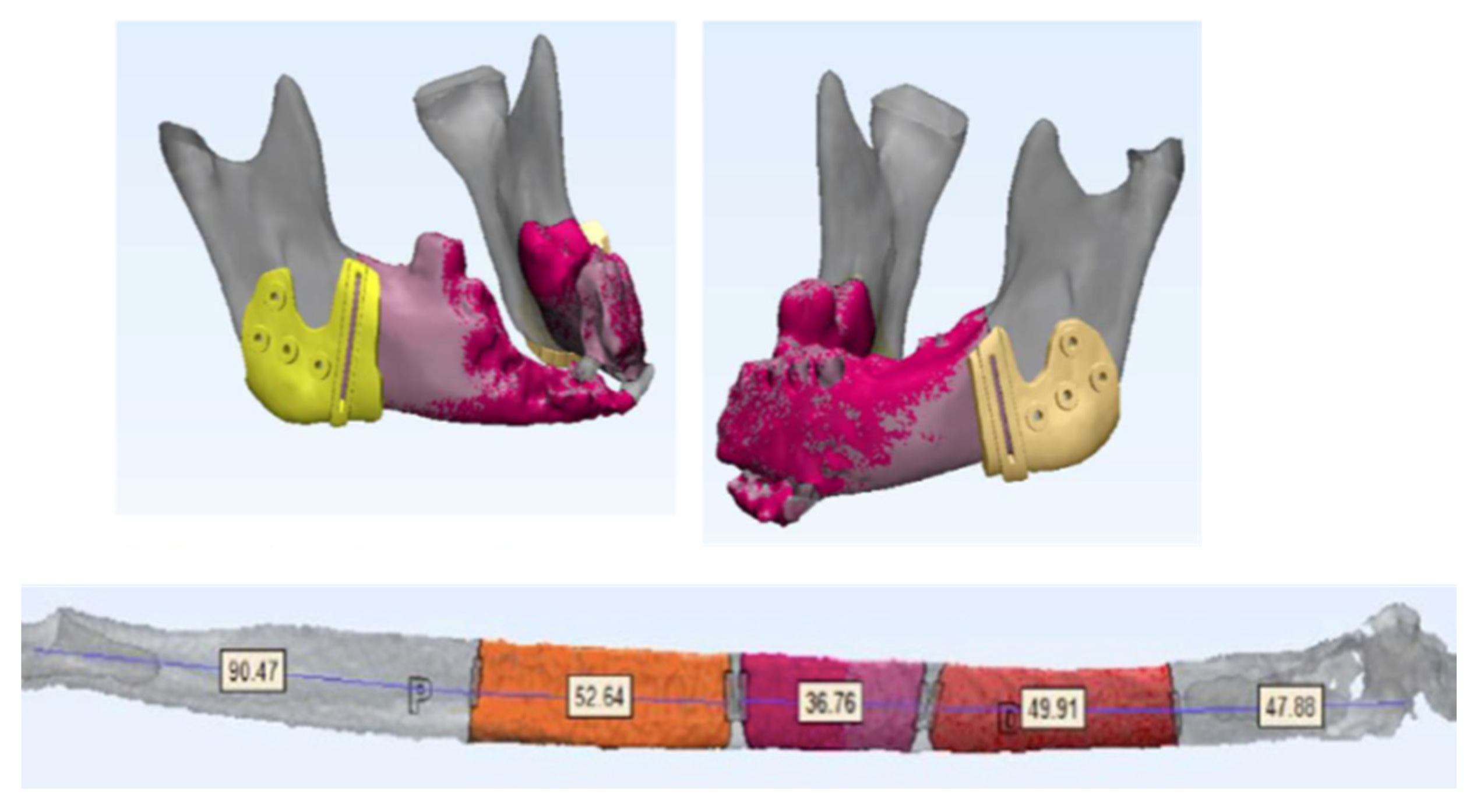
2. Case Presentation
3. Discussion
- Presence of exposed bone (or bone that can be probed through an intraoral or extraoral fistula) in the maxillofacial region for a period of 8 weeks.
- Current or previous treatment with antiresorptive agents (bisphosphonates or denosumab) or antiangiogenic agents.
- No history of radiotherapy or metastatic disease in the jaw.
4. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Conflicts of Interest
References
- Sung, H.; Ferlay, J.; Siegel, R.L.; Laversanne, M.; Soerjomataram, I.; Jemal, A.; Bray, F. Global Cancer Statistics 2020: GLOBOCAN Estimates of Incidence and Mortality Worldwide for 36 Cancers in 185 Countries. CA Cancer J. Clin. 2021, 71, 209–249. [Google Scholar] [CrossRef] [PubMed]
- Woolgar, J.A.; Triantafyllou, A.; Ferlito, A.; Devaney, K.O.; Lewis, J.S.; Rinaldo, A.; Slootweg, P.J.; Barnes, L. Intraosseous carcinoma of the jaws: A clinicopathologic review. Part III: Primary intraosseous squamous cell carcinoma. Head Neck 2013, 35, 906–909. [Google Scholar] [CrossRef] [PubMed]
- Li, K.; Yang, L.; Qiao, Y.-J.; Liang, Y.-J.; Wang, X.; Liao, G.-Q. Risk factors and prognosis for the primary intraosseous carcinoma of the jaw. Int. J. Oral Maxillofac. Surg. 2019, 48, 157–162. [Google Scholar] [CrossRef] [PubMed]
- Marx, R. Pamidronate (Aredia) and zolendronate (Zometa) induced avascular necrosis of the jaws: A growing epidemic. J. Oral Maxilofac. Surg. 2003, 61, 1115–1118. [Google Scholar] [CrossRef]
- Tocaciu, S.; Breik, O.; Lim, B.; Angel, C.; Rutherford, N. Diagnostic dilemma between medication-related osteonecrosis and oral squamous cell carcinoma in a mandibular lytic lesion. Br. J. Oral Maxillofac. Surg. 2017, 55, e53–e57. [Google Scholar] [CrossRef] [PubMed]
- Samieirad, S.; Labafchi, A.; Famili, K.; Hashemzadeh, H. Medication-Related Osteonecrosis of the Jaw (MRONJ) due to Simvastatin: An Unusual Case Report. World J. Plast. Surg. 2021, 10, 132–135. [Google Scholar] [PubMed]
- Qaisi, M.; Hargett, J.; Loeb, M.; Brown, J.; Caloss, R. Denosumab Related Osteonecrosis of the Jaw with Spontaneous Necrosis of the Soft Palate: Report of a Life Threatening Case. Case Rep. Dent. 2016, 2016, 5070187. [Google Scholar] [CrossRef] [PubMed]
- Ruggiero, S.L.; Dodson, T.B.; Fantasia, J.; Goodday, R.; Aghaloo, T.; Mehrotra, B.; O’Ryan, F. American association of oral and maxillofacial surgeons position paper on medication-related osteonecrosis of the jaw—2014 update. J. Oral Maxillofac. Surg. 2014, 72, 1938–1956. [Google Scholar] [CrossRef] [PubMed]
- Owosho, A.A.; Xu, B.; Kadempour, A.; Yom, S.K.; Joseph Randazzo, J.; Ghossein, R.A.; Huryn, J.M.; Estilo, C.L. Metastatic solid tumors to the jaw and oral soft tissue: A retrospective clinical analysis of 44 patients from a single institution. J. Craniomaxillofac. Surg. 2016, 44, 1047–1053. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Krestan, C.R.; Mitchell, D.A.; Kirschke, J.S.; Wutzl, A.; Mücke, T. Bisphosphonate and Medication-Related Osteonecrosis of the Jaw: A Review. Semin. Musculoskelet. Radiol. 2016, 20, 305–314. [Google Scholar] [CrossRef] [PubMed]
- Diaz-Reverand, S.A.; Naval-Gíaz, L.; Muñoz-Guerra, M.F.; Sastre-Pérez, J.; Rodríguez-Campo, F.J.; Gil-Diez, J.L. Manejo de la osteonecrosis maxilar asociada al uso de medicamentos en virtud de su estadio clínico: Análisis de 19 casos. Rev. Española Cirugía Oral Maxilofac. 2018, 40, 104–111. [Google Scholar] [CrossRef]
- Boquete-Castro, A.; Gómez-Moreno, G.; Calvo-Guirado, J.L.; Aguilar-Salvatierra, A.; Delgado-Ruiz, R.A. Denosumab and osteonecrosis of the jaw. A systematic analysis of events reported in clinical trials. Clin. Oral Implant. Res. 2016, 27, 367–375. [Google Scholar] [CrossRef] [PubMed]
- Saad, F.; Brown, J.E.; Van Poznaketal, C. Incidence, risk factors, and outcomes of osteonecrosis of the jaw: Integrated analysis from three blinded active-controlled phase III trials in cancer patients with bone metastases. Ann. Oncol. 2012, 23, 1341–1347. [Google Scholar] [CrossRef] [PubMed]
- Stopeck, A.T.; Lipton, A.; Body, J.-J.; Steger, G.G.; Tonkin, K.; De Boer, R.H.; Lichinitser, M.; Fujiwara, Y.; Yardley, D.A.; Viniegra, M.; et al. Denosumab Compared With Zoledronic Acid for the Treatment of Bone Metastases in Patients With Advanced Breast Cancer: A Randomized, Double-Blind Study. J. Clin. Oncol. 2010, 28, 5132–5139. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Henry, D.; Vadhan-Raj, S.; Hirsh, V.; Von Moos, R.; Hungria, V.; Costa, L.; Woll, P.; Scagliotti, G.; Smith, G.; Feng, A.; et al. Delaying skeletal-related events in a randomized phase 3 study of denosumab versus zoledronic acid in patients with advanced cancer: An analysis of data from patients with solid tumors. Support. Care Cancer 2014, 22, 679–687. [Google Scholar] [CrossRef] [PubMed]







Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Bacián Martínez, S.; Navarro Cuéllar, C.; Navarro Vila, C.; Palacios Weiss, E.; Pujol Romanyá, R.; del Amo Fernández de Velasco, Á.; Escrig de Teijeiro, M.; del Castillo Pardo de Vera, J.L.; Rodríguez Pérez, I.; Sánchez-Pérez, A.; et al. Intraosseous Squamous Cell Carcinoma Associated with Denosumab-Induced Osteonecrosis of the Jaw. Appl. Sci. 2021, 11, 7646. https://doi.org/10.3390/app11167646
Bacián Martínez S, Navarro Cuéllar C, Navarro Vila C, Palacios Weiss E, Pujol Romanyá R, del Amo Fernández de Velasco Á, Escrig de Teijeiro M, del Castillo Pardo de Vera JL, Rodríguez Pérez I, Sánchez-Pérez A, et al. Intraosseous Squamous Cell Carcinoma Associated with Denosumab-Induced Osteonecrosis of the Jaw. Applied Sciences. 2021; 11(16):7646. https://doi.org/10.3390/app11167646
Chicago/Turabian StyleBacián Martínez, Sandra, Carlos Navarro Cuéllar, Carlos Navarro Vila, Edurne Palacios Weiss, Roser Pujol Romanyá, Álvaro del Amo Fernández de Velasco, Margarita Escrig de Teijeiro, José Luis del Castillo Pardo de Vera, Irene Rodríguez Pérez, Arturo Sánchez-Pérez, and et al. 2021. "Intraosseous Squamous Cell Carcinoma Associated with Denosumab-Induced Osteonecrosis of the Jaw" Applied Sciences 11, no. 16: 7646. https://doi.org/10.3390/app11167646
APA StyleBacián Martínez, S., Navarro Cuéllar, C., Navarro Vila, C., Palacios Weiss, E., Pujol Romanyá, R., del Amo Fernández de Velasco, Á., Escrig de Teijeiro, M., del Castillo Pardo de Vera, J. L., Rodríguez Pérez, I., Sánchez-Pérez, A., Zamorano-León, J. J., López-Farré, A., García-Hidalgo Alonso, M. I., & Navarro Cuéllar, I. (2021). Intraosseous Squamous Cell Carcinoma Associated with Denosumab-Induced Osteonecrosis of the Jaw. Applied Sciences, 11(16), 7646. https://doi.org/10.3390/app11167646