
Ossification of the Anterior Longitudinal Ligament with Dysphagia as the First Symptom: Rehabilitation of Two Cases

 ,
,  ,
, {kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Abstract
:1. Introduction
2. Material and Methods
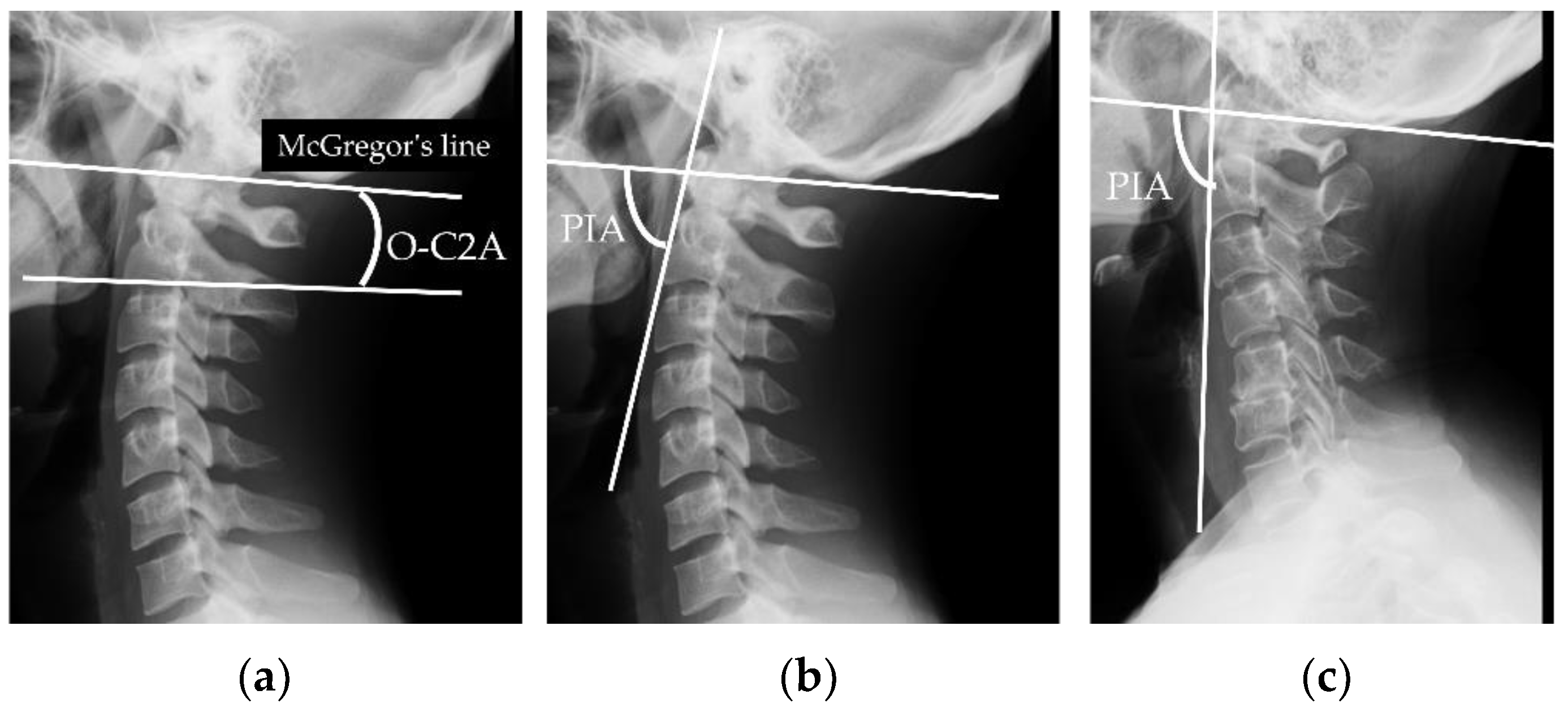
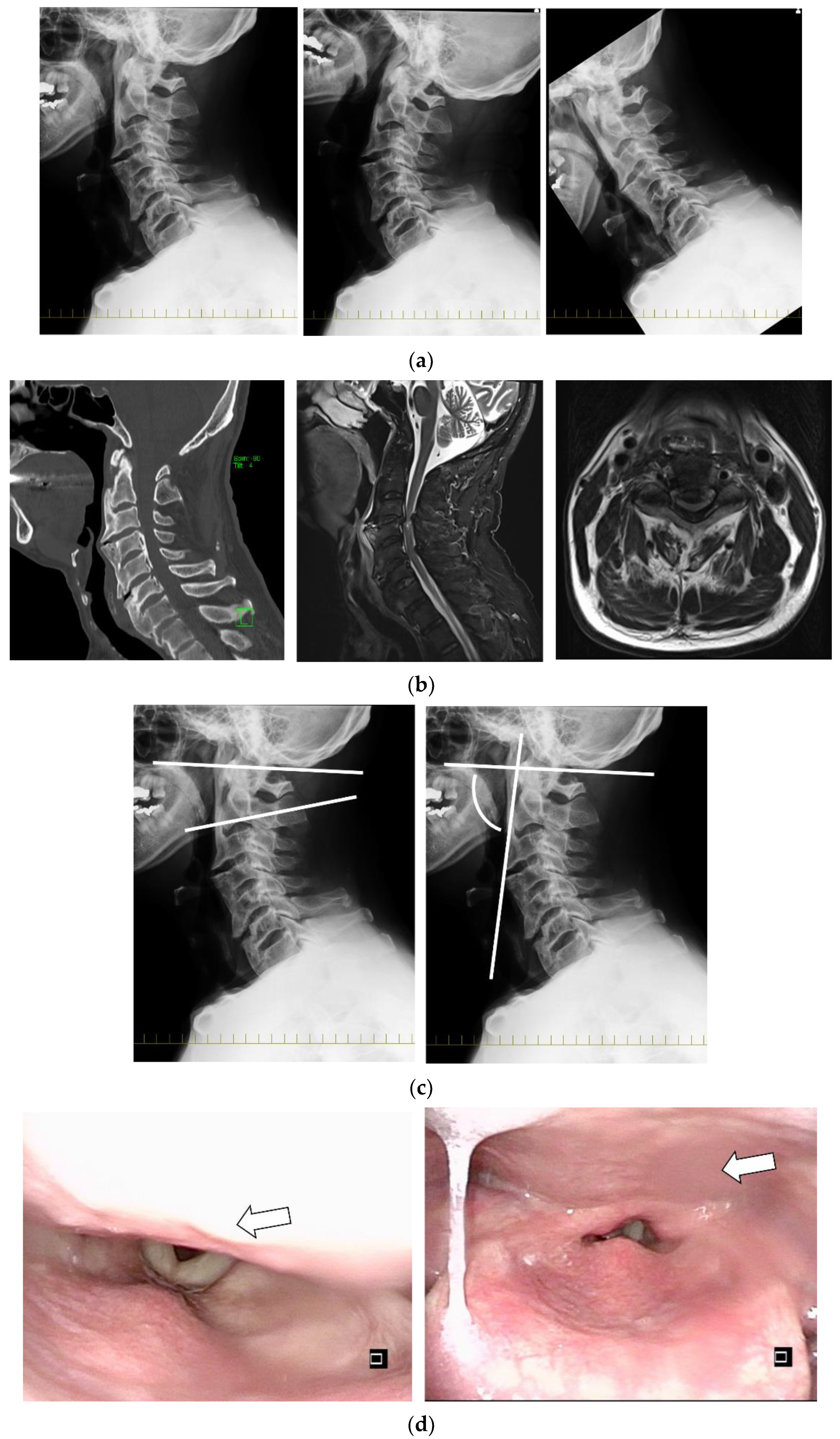
2.1. Radiological Evaluations
2.2. Screening Test
2.3. Practical Assessment Tool
2.4. Clinical Otorhinolaryngology Assessment
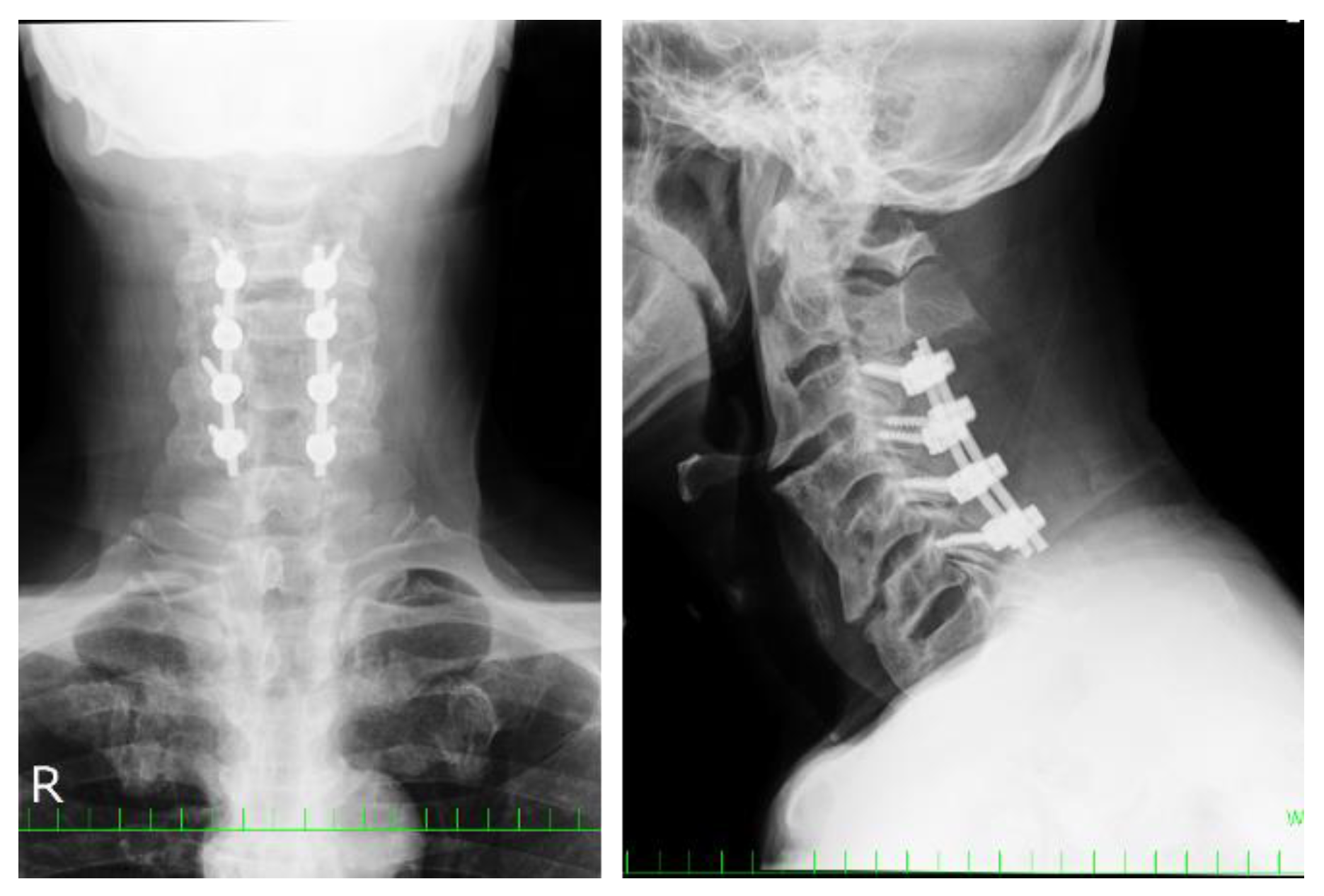
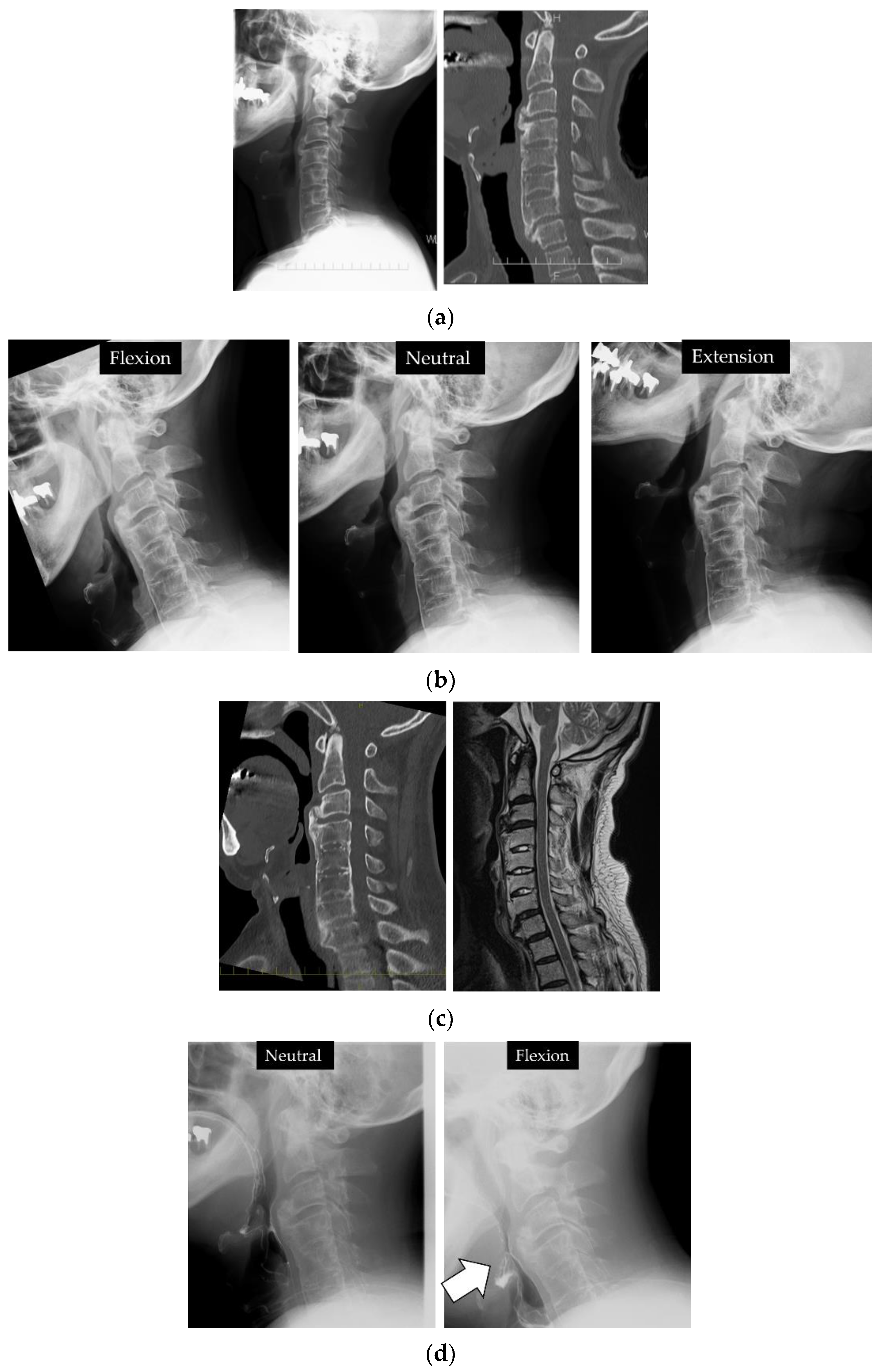
2.5. Clinical Presentations
3. Discussion
4. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Wang, T.; Zhao, Y.; Guo, A. Association of swallowing problems with frailty in Chinese hospitalized older patients. Int. J. Nurs. Sci. 2020, 7, 408–412. [Google Scholar] [CrossRef]
- Forestier, J.; Lagier, R. Ankylosing hyperostosis of the spine. Clin Orthop. Relat. Res. 1971, 74, 65–83. [Google Scholar] [CrossRef]
- Resnick, D.; Niwayama, G. Radiographic and pathologic features of spinal involvement in diffuse idiopathic skeletal hyperostosis (DISH). Radiology 1976, 119, 559–568. [Google Scholar] [CrossRef] [PubMed]
- Mader, R.; Sarzi-Puttini, P.; Atzeni, F.; Olivieri, I.; Pappone, N.; Verlaan, J.J.; Buskila, D. Extraspinal manifestations of diffuse idiopathic skeletal hyperostosis. Rheumatology 2009, 48, 1478–1481. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kmucha, S.T.; Cravens, R.B., Jr. DISH syndrome and its role in dysphagia. Otolaryngol. Head Neck Surg. 1994, 110, 431–436. [Google Scholar] [CrossRef]
- Presutti, L.; Alicandri-Ciufelli, M.; Piccinini, A.; Trebbi, M.; Marchioni, D.; Ghidini, A.; Ruberto, M. Forestier disease: Single-center surgical experience and brief literature review. Ann. Otol. Rhinol. Laryngol. 2010, 119, 602–608. [Google Scholar] [CrossRef]
- Carlson, M.L.; Archibald, D.J.; Graner, D.E.; Kasperbauer, J.L. Surgical management of dysphagia and airway obstruction in patients with prominent ventral cervical osteophytes. Dysphagia 2011, 26, 34–40. [Google Scholar] [CrossRef]
- Eviatar, E.; Harell, M. Diffuse idiopathic skeletal hyperostosis with dysphagia (a review). J. Laryngol. Otol. 1987, 101, 627–632. [Google Scholar] [CrossRef] [PubMed]
- Kos, M.P.; van Royen, B.J.; David, E.F.; Mahieu, H.F. Anterior cervical osteophytes resulting in severe dysphagia and aspiration: Two case reports and literature review. J. Laryngol. Otol. 2009, 123, 1169–1173. [Google Scholar] [CrossRef] [PubMed]
- Lofrese, G.; Scerrati, A.; Balsano, M.; Bassani, R.; Cappuccio, M.; Cavallo, M.A.; Cofano, F.; Cultrera, F.; De Iure, F.; Biase, F.D.; et al. Surgical Treatment of Diffuse Idiopathic Skeletal Hyperostosis (DISH) Involving the Cervical Spine: Technical Nuances and Outcome of a Multicenter Experience. Global Spine J. 2021, 2192568220988272. [Google Scholar] [CrossRef]
- Park, B.J.; Gold, C.J.; Piscopo, A.; Schwickerath, L.; Bathla, G.; Chieng, L.O.; Yamaguchi, S.; Hitchon, P.W. Outcomes and complications of surgical treatment of anterior osteophytes causing dysphagia: Single center experience. Clin. Neurol. Neurosurg. 2021, 207, 106814. [Google Scholar] [CrossRef]
- Cherfane, P.; Smaily, H.; Khalaf, M.G.; Ghaoui, N.; Melkane, A.E. Otolaryngologic manifestations of diffuse idiopathic skeletal hyperostosis (Forestier’s disease): A systematic review of the literature. Joint Bone Spine 2021, 88, 105218. [Google Scholar] [CrossRef]
- Gendreau, J.L.; Sheaffer, K.; Bennett, J.; Abraham, M.; Patel, N.V.; Herschman, Y.; Ruh, N.; Lindley, J.G. Timing of Surgical Intervention for Dysphagia in Patients With Diffuse Idiopathic Skeletal Hyperostosis: A Systematic Review and Meta-Analysis. Clin. Spine Surg. 2021, 34, 220–227. [Google Scholar] [CrossRef]
- Miyata, M.; Neo, M.; Fujibayashi, S.; Ito, H.; Takemoto, M.; Nakamura, T. O-C2 angle as a predictor of dyspnea and/or dysphagia after occipitocervical fusion. Spine 2009, 34, 184–188. [Google Scholar] [CrossRef]
- Yoshida, M.; Neo, M.; Fujibayashi, S.; Nakamura, T. Upper-airway obstruction after short posterior occipitocervical fusion in a flexed position. Spine 2007, 32, E267–E270. [Google Scholar] [CrossRef] [PubMed]
- Kaneyama, S.; Sumi, M.; Takabatake, M.; Kasahara, K.; Kanemura, A.; Hirata, H.; Darden, B.V. The Prediction and Prevention of Dysphagia After Occipitospinal Fusion by Use of the S-line (Swallowing Line). Spine 2017, 42, 718–725. [Google Scholar] [CrossRef] [PubMed]
- Pouderoux, P.; Jacquot, J.M.; Royer, E.; Finiels, H. Deglutition disorders in the elderly. Evaluation methods. Presse Med. 2001, 30, 1635–1644. [Google Scholar] [PubMed]
- Kunieda, K.; Ohno, T.; Fujishima, I.; Hojo, K.; Morita, T. Reliability and validity of a tool to measure the severity of dysphagia: The Food Intake LEVEL Scale. J. Pain Symptom. Manag. 2013, 46, 201–206. [Google Scholar] [CrossRef] [PubMed]
- Tohara, H.; Palmer, J.B.; Reynolds, K.; Kuhlemeier, K.V.; Palmer, S. Dysphagia severity scale]. Kokubyo Gakkai Zasshi 2003, 70, 242–248. [Google Scholar] [CrossRef] [Green Version]
- O’Neil, K.H.; Purdy, M.; Falk, J.; Gallo, L. The Dysphagia Outcome and Severity Scale. Dysphagia 1999, 14, 139–145. [Google Scholar] [CrossRef]
- McCafferty, R.R.; Harrison, M.J.; Tamas, L.B.; Larkins, M.V. Ossification of the anterior longitudinal ligament and Forestier’s disease: An analysis of seven cases. J. Neurosurg. 1995, 83, 13–17. [Google Scholar] [CrossRef]
- Oppenlander, M.E.; Orringer, D.A.; La Marca, F.; McGillicuddy, J.E.; Sullivan, S.E.; Chandler, W.F.; Park, P. Dysphagia due to anterior cervical hyperosteophytosis. Surg. Neurol. 2009, 72, 266–270. [Google Scholar] [CrossRef]
- Belafsky, P.C.; Mouadeb, D.A.; Rees, C.J.; Pryor, J.C.; Postma, G.N.; Allen, J.; Leonard, R.J. Validity and reliability of the Eating Assessment Tool (EAT-10). Ann. Otol. Rhinol. Laryngol. 2008, 117, 919–924. [Google Scholar] [CrossRef] [PubMed]
- Song, J.; Mizuno, J.; Nakagawa, H. Clinical and radiological analysis of ossification of the anterior longitudinal ligament causing dysphagia and hoarseness. Neurosurgery 2006, 58, 913–919; discussion 913–919. [Google Scholar] [CrossRef]
- Von der Hoeh, N.H.; Voelker, A.; Jarvers, J.S.; Gulow, J.; Heyde, C.E. Results after the surgical treatment of anterior cervical hyperostosis causing dysphagia. Eur. Spine J. 2015, 24 (Suppl. 4), S489–S493. [Google Scholar] [CrossRef] [PubMed]
- Seidler, T.O.; Pèrez Alvarez, J.C.; Wonneberger, K.; Hacki, T. Dysphagia caused by ventral osteophytes of the cervical spine: Clinical and radiographic findings. Eur. Arch. Otorhinolaryngol. 2009, 266, 285–291. [Google Scholar] [CrossRef] [PubMed]
- Tian, W.; Yu, J. The role of C2-C7 and O-C2 angle in the development of dysphagia after cervical spine surgery. Dysphagia 2013, 28, 131–138. [Google Scholar] [CrossRef]
- Goh, P.Y.; Dobson, M.; Iseli, T.; Maartens, N.F. Forestier’s disease presenting with dysphagia and dysphonia. J. Clin. Neurosci. 2010, 17, 1336–1338. [Google Scholar] [CrossRef]
- Spanu, G.; Marchionni, M.; Adinolfi, D.; Knerich, R. Complications following anterior cervical spine surgery for disc diseases: An analysis of ten years experience. Chir. Organi. Mov. 2005, 90, 229–240. [Google Scholar] [PubMed]
- Urrutia, J.; Bono, C.M. Long-term results of surgical treatment of dysphagia secondary to cervical diffuse idiopathic skeletal hyperostosis. Spine J. 2009, 9, e13–e17. [Google Scholar] [CrossRef] [PubMed]
- Lui Jonathan, Y.C.; Sayal, P.; Prezerakos, G.; Russo, V.; Choi, D.; Casey, A.T.H. The surgical management of dysphagia secondary to diffuse idiopathic skeletal hyperostosis. Clin. Neurol. Neurosurg. 2018, 167, 36–42. [Google Scholar] [CrossRef] [PubMed]
- Kaur, J.; Virk, J.S. Dysphagia due to DISH-related anterior osteophytes: DISHphagia!! BMJ Case Rep. 2017, 2017, bcr-2017. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Egerter, A.C.; Kim, E.S.; Lee, D.J.; Liu, J.J.; Cadena, G.; Panchal, R.R.; Kim, K.D. Dysphagia Secondary to Anterior Osteophytes of the Cervical Spine. Global Spine J. 2015, 5, 78–83. [Google Scholar] [CrossRef] [PubMed]
- Miyamoto, K.; Sugiyama, S.; Hosoe, H.; Iinuma, N.; Suzuki, Y.; Shimizu, K. Postsurgical recurrence of osteophytes causing dysphagia in patients with diffuse idiopathic skeletal hyperostosis. Eur. Spine J. 2009, 18, 1652–1658. [Google Scholar] [CrossRef] [Green Version]

Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Nishida, N.; Ogasa, H.; Seki, K.; Kato, T.; Imajo, Y.; Suzuki, H.; Funaba, M.; Yukata, K.; Sakai, T. Ossification of the Anterior Longitudinal Ligament with Dysphagia as the First Symptom: Rehabilitation of Two Cases. Appl. Sci. 2021, 11, 7300. https://doi.org/10.3390/app11167300
Nishida N, Ogasa H, Seki K, Kato T, Imajo Y, Suzuki H, Funaba M, Yukata K, Sakai T. Ossification of the Anterior Longitudinal Ligament with Dysphagia as the First Symptom: Rehabilitation of Two Cases. Applied Sciences. 2021; 11(16):7300. https://doi.org/10.3390/app11167300
Chicago/Turabian StyleNishida, Norihiro, Hiroyoshi Ogasa, Kazushige Seki, Tomohiro Kato, Yasuaki Imajo, Hidenori Suzuki, Masahiro Funaba, Kiminori Yukata, and Takashi Sakai. 2021. "Ossification of the Anterior Longitudinal Ligament with Dysphagia as the First Symptom: Rehabilitation of Two Cases" Applied Sciences 11, no. 16: 7300. https://doi.org/10.3390/app11167300
APA StyleNishida, N., Ogasa, H., Seki, K., Kato, T., Imajo, Y., Suzuki, H., Funaba, M., Yukata, K., & Sakai, T. (2021). Ossification of the Anterior Longitudinal Ligament with Dysphagia as the First Symptom: Rehabilitation of Two Cases. Applied Sciences, 11(16), 7300. https://doi.org/10.3390/app11167300