
A Cadaveric Study of Ulnar Nerve Movement and Strain around the Elbow Joint

 , , and
, , and 
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Abstract
:1. Introduction
2. Materials and Methods
2.1. Ethics Considerations
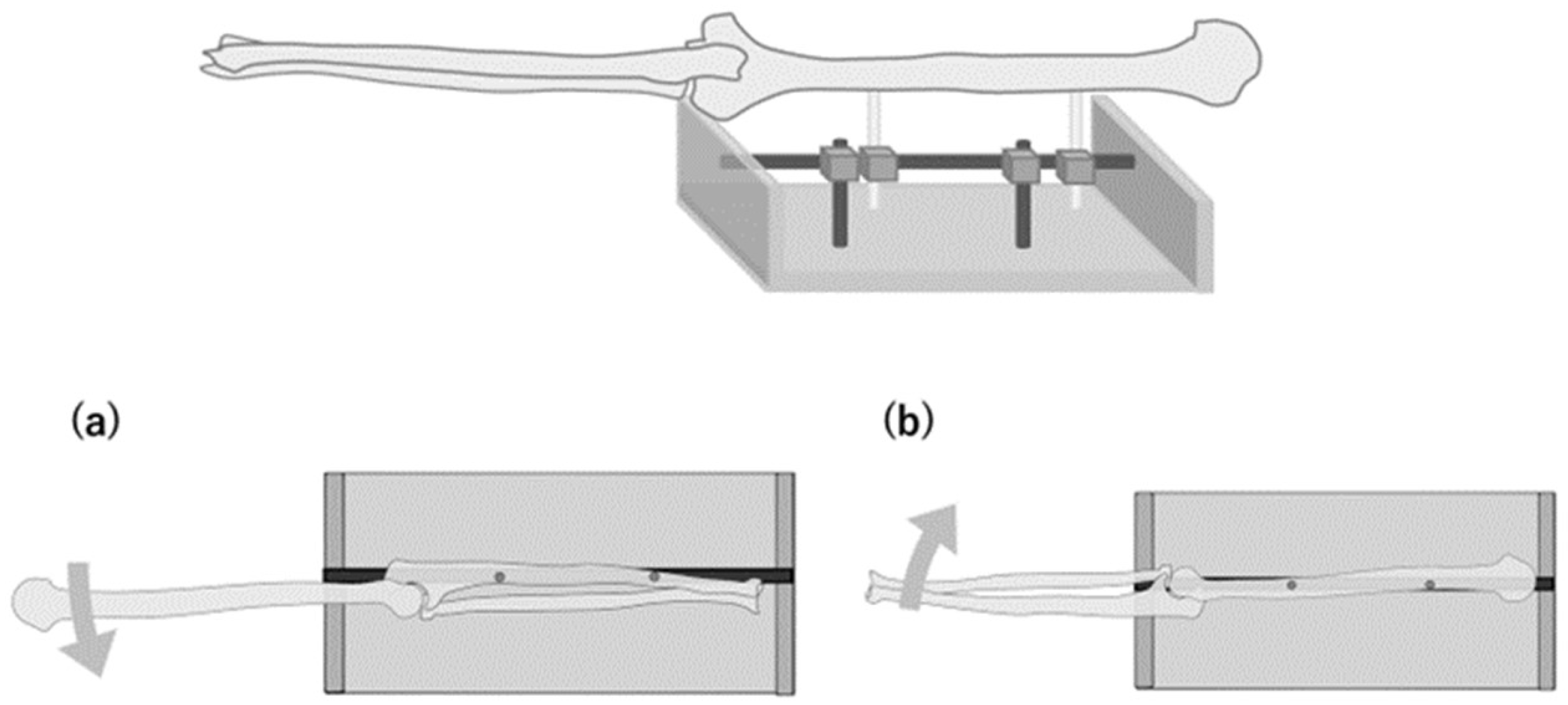
2.2. Specimen Preparation
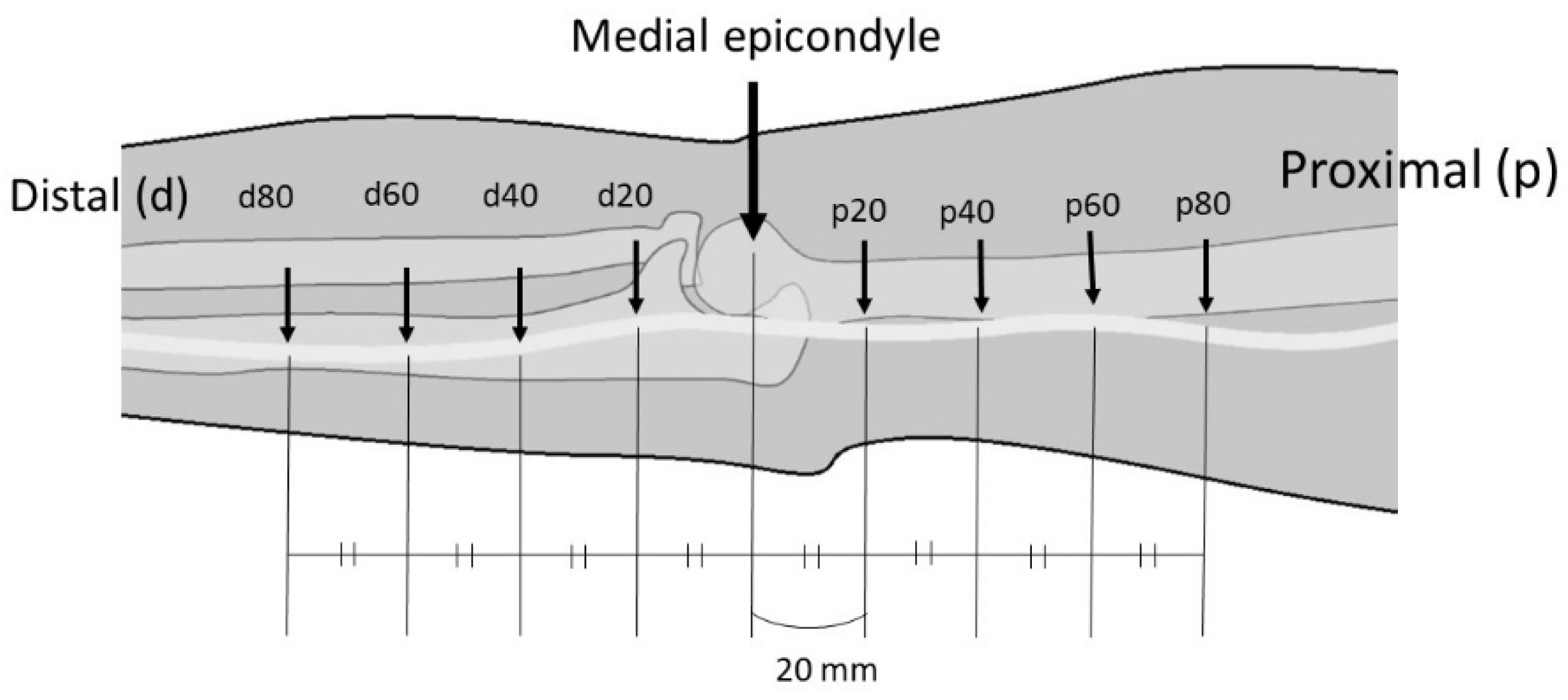
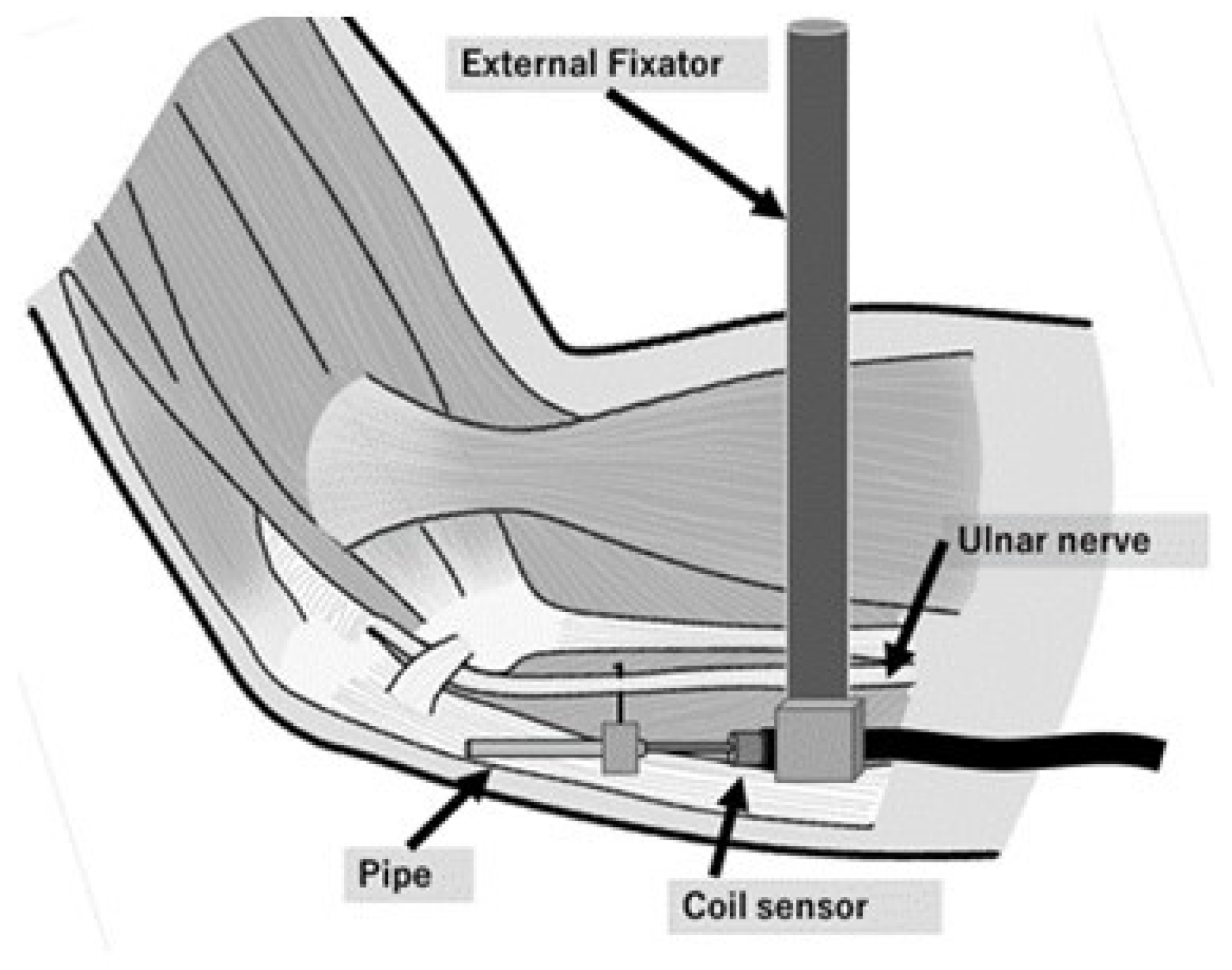
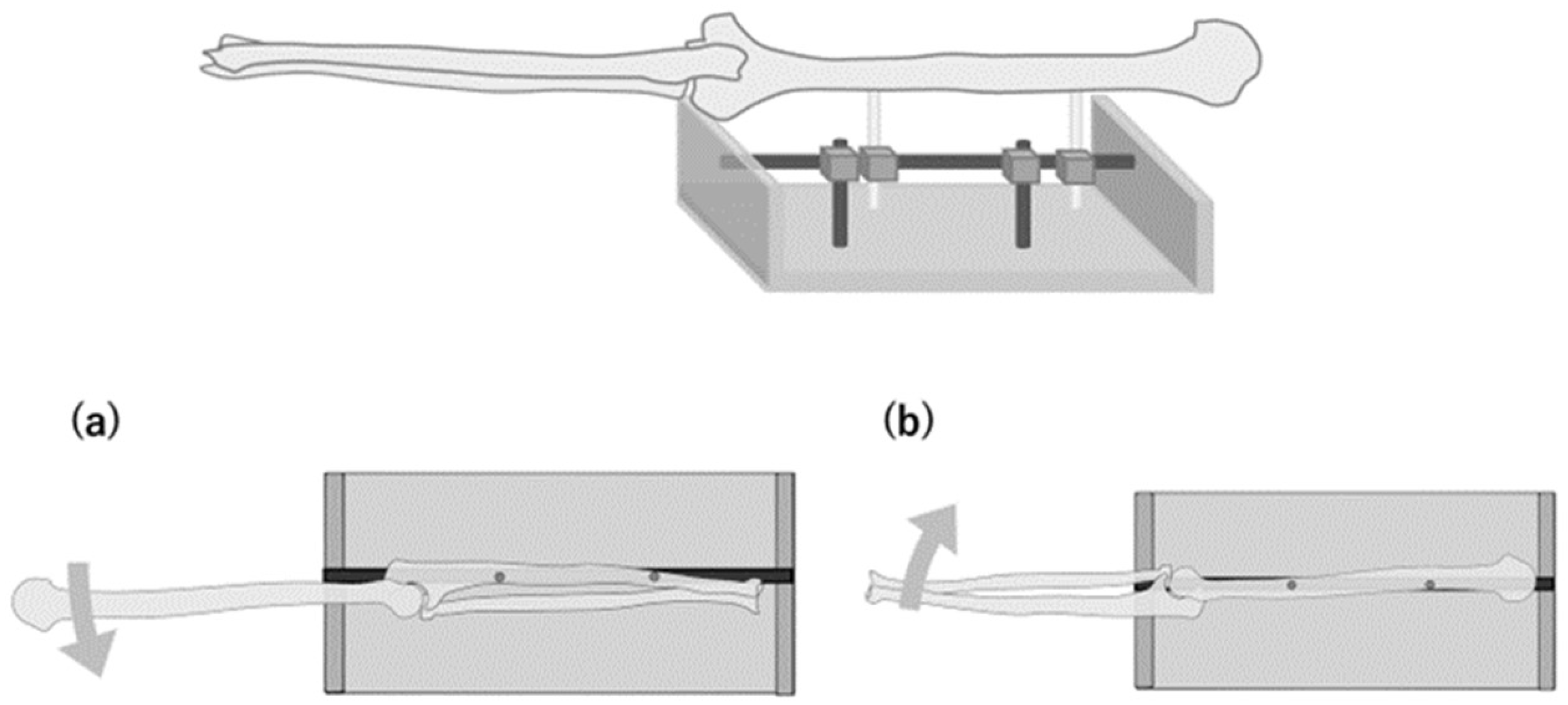
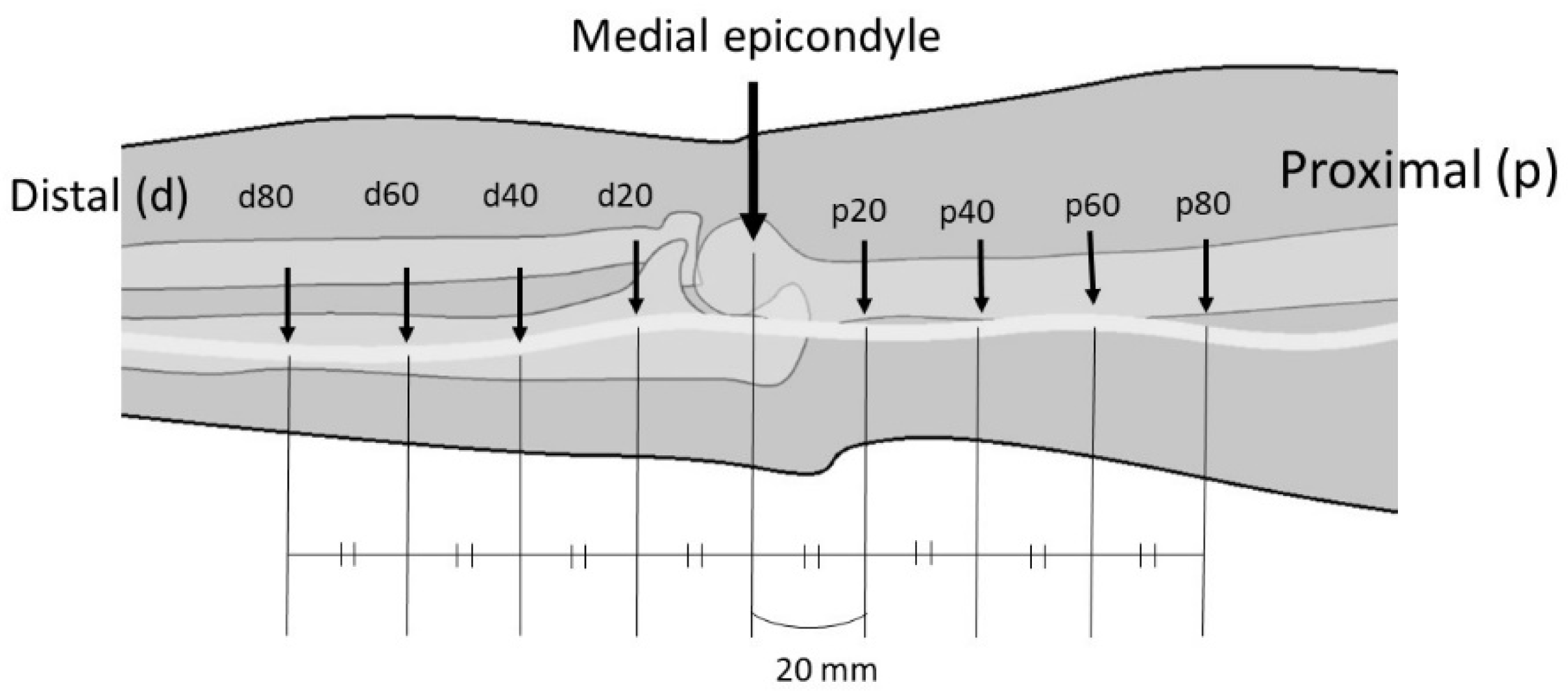
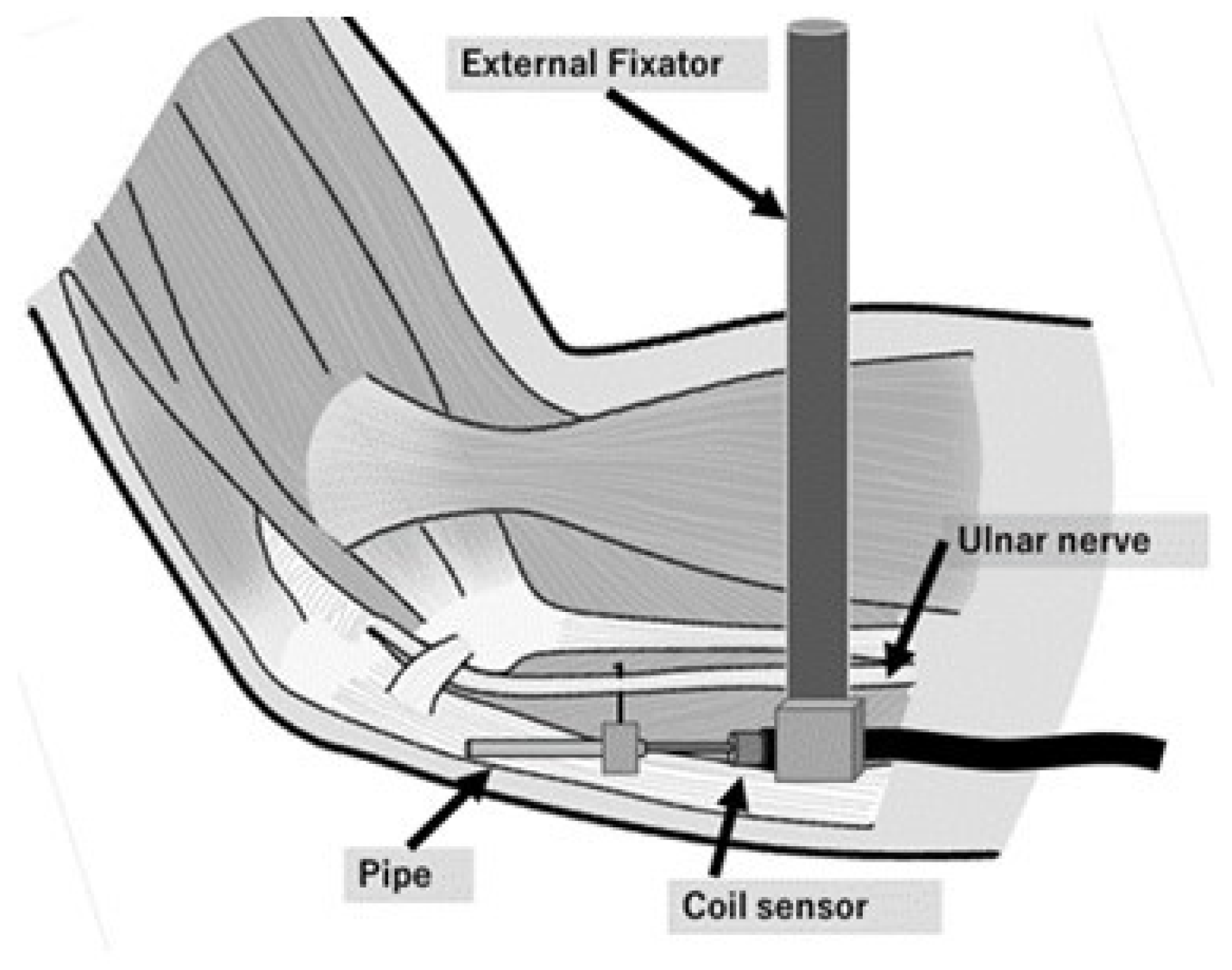
2.3. Measurement of Ulnar Nerve Movement
2.4. Experimental Sequences
2.5. Statistical Analysis
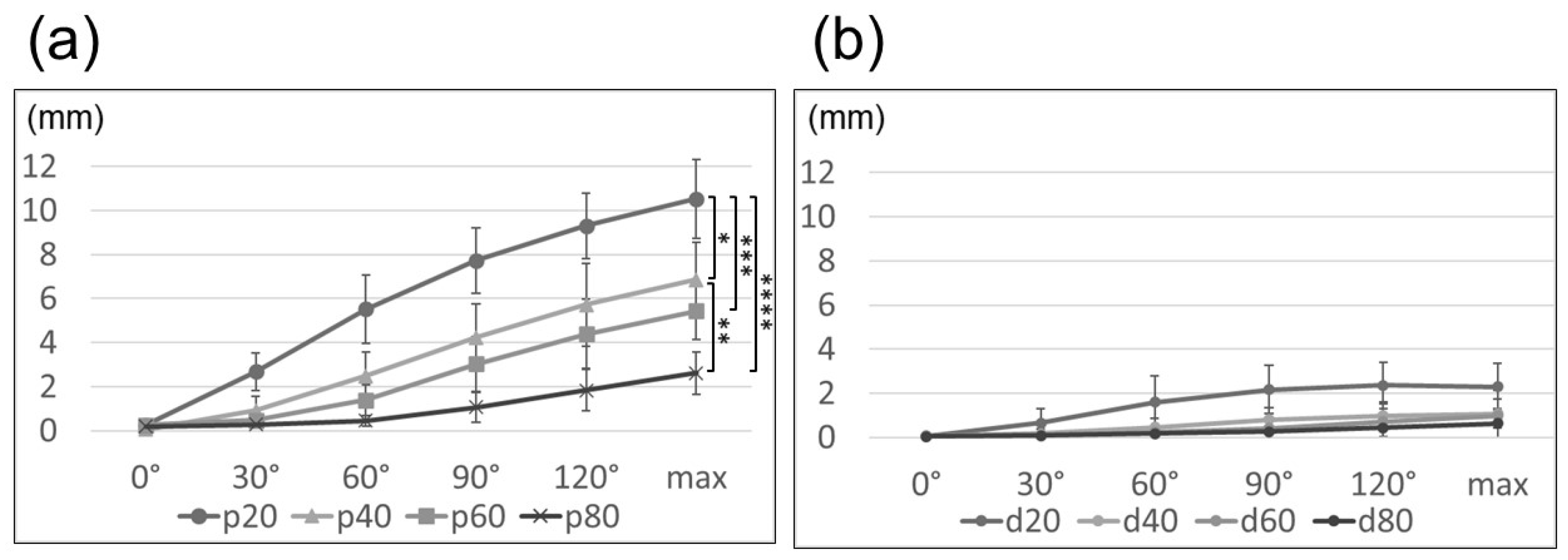
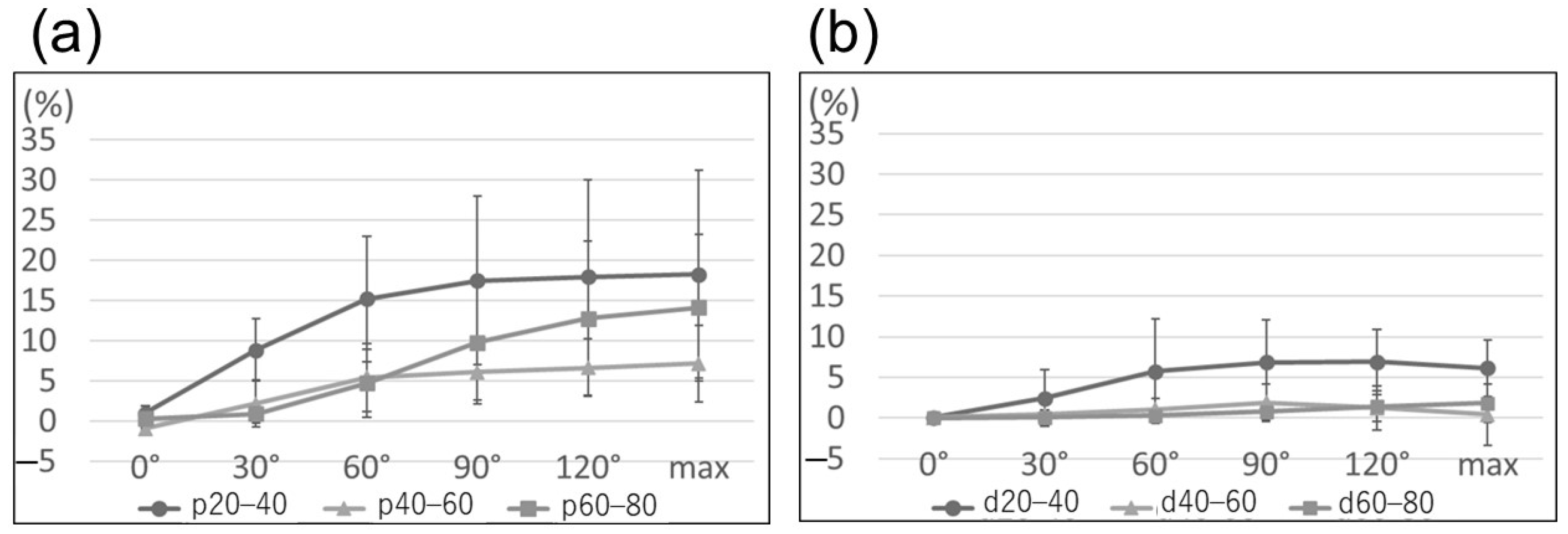
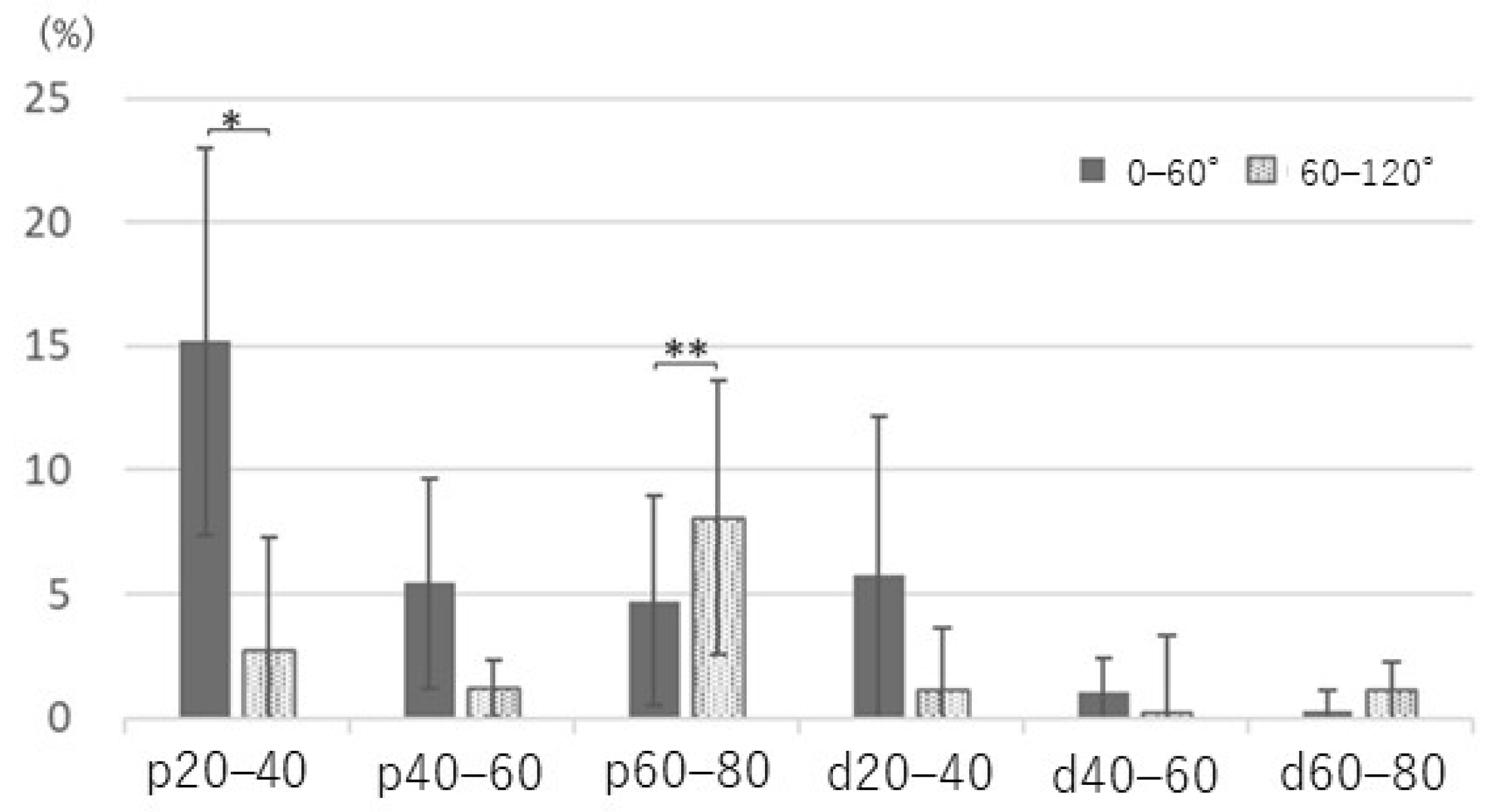
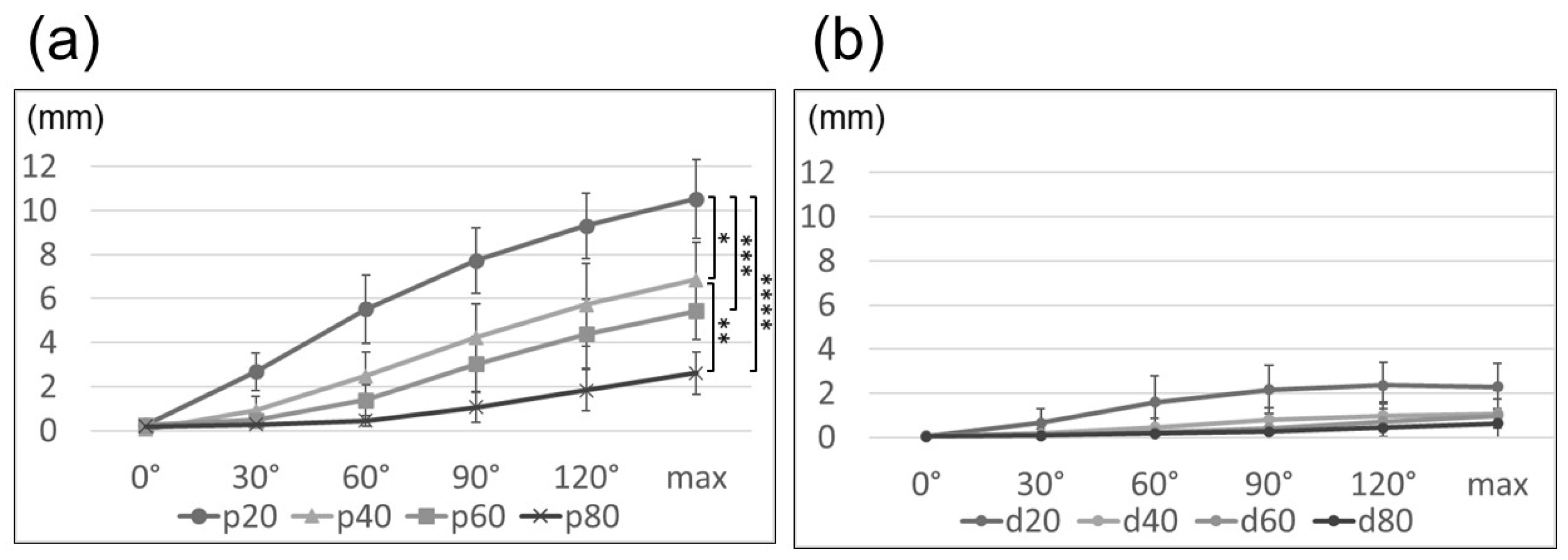
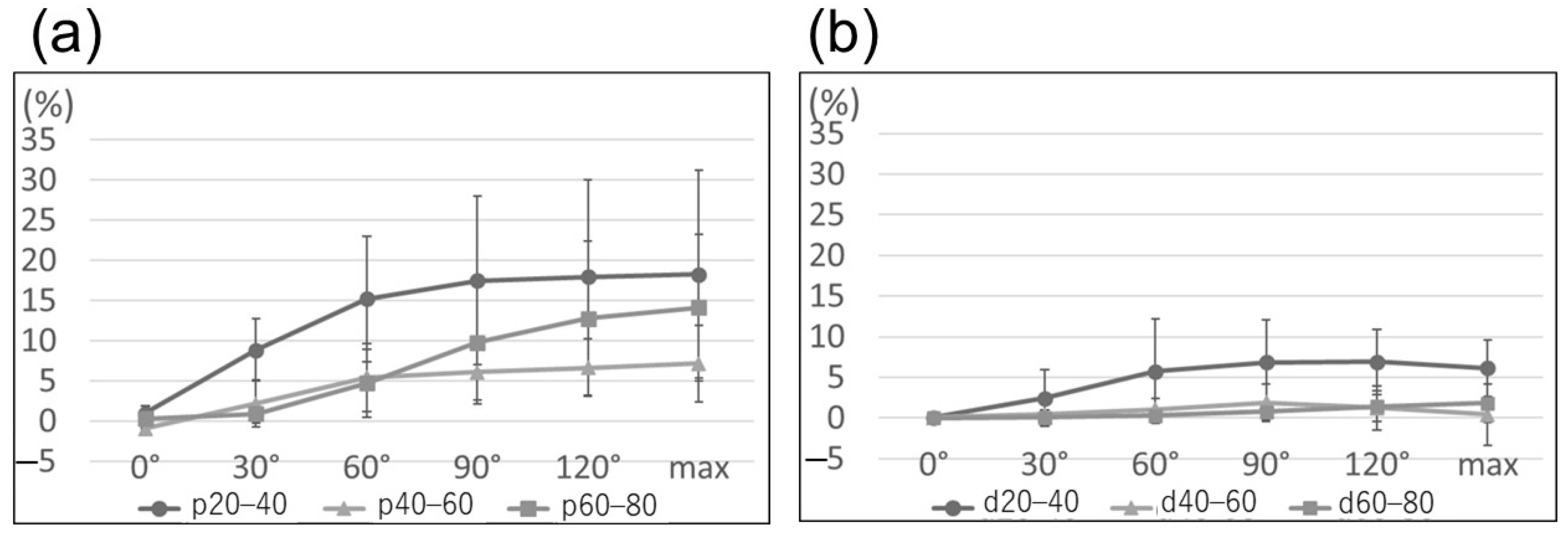
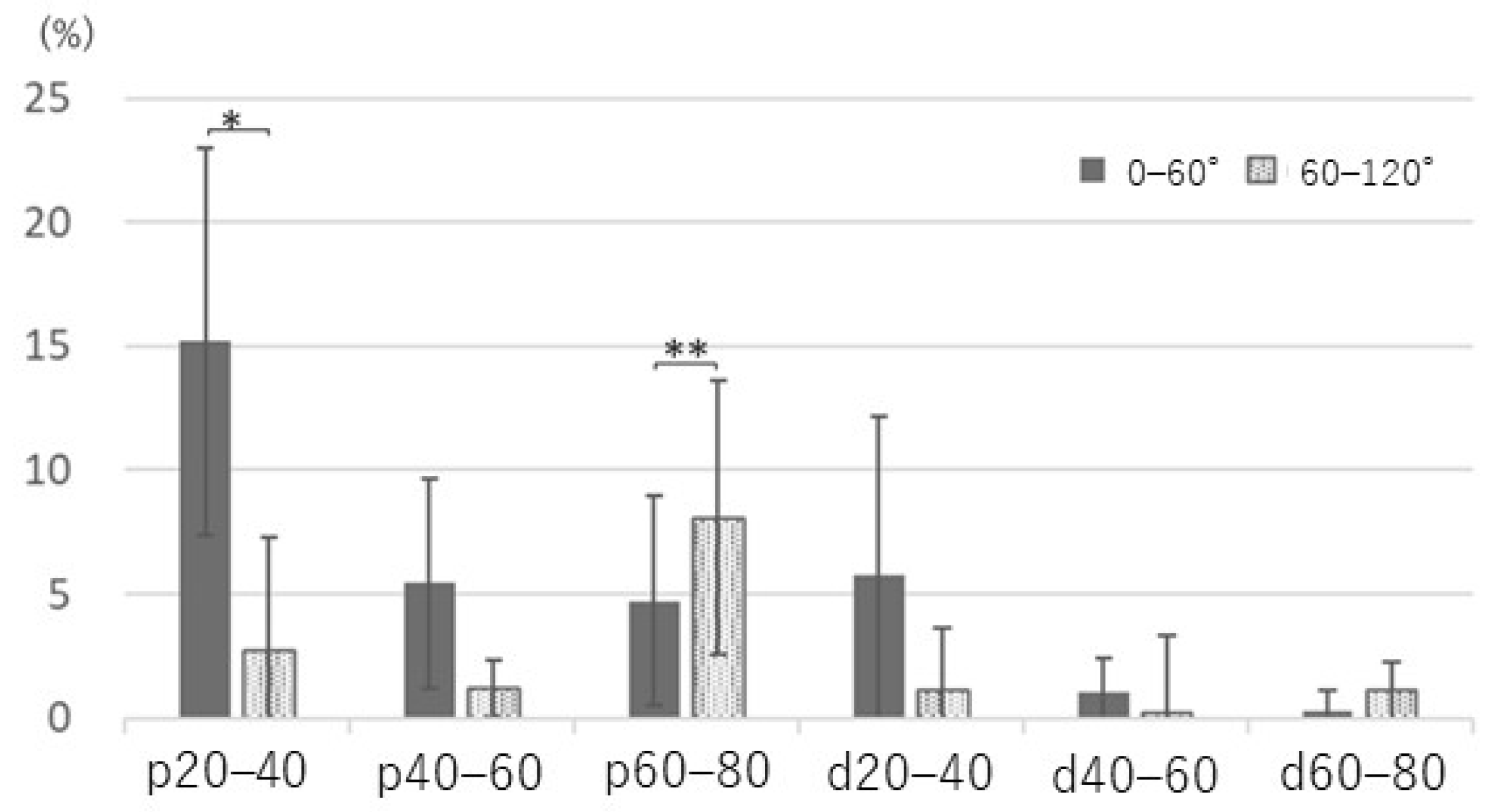
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Aoki, M.; Takasaki, H.; Muraki, T.; Uchiyama, E.; Murakami, G.; Yamashita, T. Strain on the ulnar nerve at the elbow and wrist during throwing motion. J. Bone Joint Surg. Am. 2005, 87, 2508–2514. [Google Scholar]
- Clark, W.L.; Trumble, T.E.; Swiontkowski, M.F.; Tencer, A.F. Nerve tension and blood flow in a rat model of immediate and delayed repairs. J. Hand Surg. Am. 1992, 17, 677–687. [Google Scholar] [CrossRef]
- Wall, E.J.; Massie, J.B.; Kwan, M.K.; Rydevik, B.L.; Myers, R.R.; Garfin, S.R. Experimental stretch neuropathy. Changes in nerve conduction under tension. J. Bone Joint Surg. Br. 1992, 74, 126–129. [Google Scholar] [CrossRef] [PubMed]
- Apfelberg, D.B.; Larson, S.J. Dynamic anatomy of the ulnar nerve at the elbow. Plast. Reconstr. Surg. 1973, 51, 79–81. [Google Scholar] [CrossRef]
- Grewal, R.; Varitimidis, S.E.; Vardakas, D.G.; Fu, F.H.; Sotereanos, D.G. Ulnar nerve elongation and excursion in the cubital tunnel after decompression and anterior transposition. J. Hand Surg. Br. 2000, 25, 457–460. [Google Scholar] [CrossRef]
- Wright, T.W.; Glowczewskie, F., Jr.; Cowin, D.; Wheeler, D.L. Ulnar nerve excursion and strain at the elbow and wrist associated with upper extremity motion. J. Hand Surg. Am. 2001, 26, 655–662. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cummins, C.A.; Schneider, D.S. Peripheral nerve injuries in baseball players. Neurol. Clin. 2008, 26, 195–215. [Google Scholar] [CrossRef]
- Byl, C.; Puttlitz, C.; Byl, N.; Lotz, J.; Topp, K. Strain in the median and ulnar nerves during upper-extremity positioning. J. Hand Surg. Am. 2002, 27, 1032–1040. [Google Scholar] [CrossRef]
- Toby, E.B.; Hanesworth, D. Ulnar nerve strains at the elbow. J. Hand Surg. Am. 1998, 23, 992–997. [Google Scholar] [CrossRef]
- Cirpar, M.; Turker, M.; Yalcinozan, M.; Eke, M.; Sahin, F. Effect of partial, distal epicondylectomy on reduction of ulnar nerve strain: A cadaver study. J. Hand Surg. Am. 2013, 38, 666–671. [Google Scholar] [CrossRef] [PubMed]
- Hicks, D.; Toby, E.B. Ulnar nerve strains at the elbow: The effect of in situ decompression and medial epicondylectomy. J. Hand Surg. Am. 2002, 27, 1026–1031. [Google Scholar] [CrossRef] [PubMed]
- Vinitpairot, C.; Jianmongkol, S.; Thammaroj, T.; Wattanakamolchai, S. Ulnar nerve strain in functional elbow and shoulder motions. J. Hand Surg. Asian Pac. Vol. 2019, 24, 323–328. [Google Scholar] [CrossRef]
- de Ruiter, G.C.W.; de Jonge, J.G.H.; Vlak, M.H.M.; van Loon-Felter, A.E. Ulnar neuropathy caused by muscular arcade of struthers. World Neurosurg. 2020, 142, 128–130. [Google Scholar] [CrossRef] [PubMed]
- Ogata, K.; Naito, M. Blood flow of peripheral nerve effects of dissection, stretching and compression. J. Hand Surg. Br. 1986, 11, 10–14. [Google Scholar] [CrossRef]
- Lundborg, G.; Rydevik, B. Effects of stretching the tibial nerve of the rabbit: A preliminary study of the intraneural circulation and the barrier function of the perineurium. J. Bone Joint Surg. Br. 1973, 55, 390–401. [Google Scholar] [CrossRef] [PubMed]
- Dahlin, L.B.; McLean, W.G. Effects of graded experimental compression on slow and fast axonal transport in rabbit vagus nerve. J. Neurol. Sci. 1986, 72, 19–30. [Google Scholar] [CrossRef]
- Kwan, M.K.; Wall, E.J.; Massie, J.; Garfin, S.R. Strain, stress and stretch of peripheral nerve: Rabbit experiments in vitro and in vivo. Acta Orthop. Scand. 1992, 63, 267–272. [Google Scholar] [CrossRef]
- Mahan, M.A.; Vaz, K.M.; Weingarten, D.; Brown, J.M.; Shah, S.B. Altered ulnar nerve kinematic behavior in a cadaver model of entrapment. Neurosurgery 2015, 76, 747–755. [Google Scholar] [CrossRef] [PubMed]
- Dilley, A.; Summerhayes, C.; Lynn, B. An in vivo investigation of ulnar nerve sliding during upper limb movements. Clin. Biomech. 2007, 22, 774–779. [Google Scholar] [CrossRef]
- Silva, A.; Manso, A.; Andrade, R.; Domingues, V.; Brandão, M.P.; Silva, A.G. Quantitative in vivo longitudinal nerve excursion and strain in response to joint movement: A systematic literature review. Clin. Biomech. 2014, 29, 839–847. [Google Scholar] [CrossRef] [PubMed]
- Paulos, R.; Leclercq, C. Motor branches of the ulnar nerve to the forearm: An anatomical study and guidelines for selective neurectomy. Surg. Radiol. Anat. 2015, 37, 1043–1048. [Google Scholar] [CrossRef] [PubMed]
- Dilley, A.; Lynn, B.; Pang, S.J. Pressure and stretch mechanosensitivity of peripheral nerve fibres following local inflammation of the nerve trunk. Pain 2005, 117, 462–472. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Agnew, S.P.; Minieka, M.M.; Patel, R.M.; Nagle, D.J. Correlation between preoperative Kimura inching studies and intraoperative findings during endoscopic-assisted decompression of the ulnar nerve at the elbow. Hand 2012, 7, 370–373. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Danoff, J.R.; Lombardi, J.M.; Rosenwasser, M.P. Use of a pedicled adipose flap as a sling for anterior subcutaneous transposition of the ulnar nerve. J. Hand Surg. Am. 2014, 39, 552–555. [Google Scholar] [CrossRef] [PubMed]
- Kokkalis, Z.T.; Jain, S.; Sotereanos, D.G. Vein wrapping at cubital tunnel for ulnar nerve problems. J. Shoulder Elbow Surg. 2010, 19, 91–97. [Google Scholar] [CrossRef] [PubMed]
- Millesi, H.; Zöch, G.; Rath, T. The gliding apparatus of peripheral nerve and its clinical significance. Ann. Chir. Main Memb. Super 1990, 9, 87–97. [Google Scholar] [CrossRef]
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Nagashima, M.; Omokawa, S.; Nakanishi, Y.; Mahakkanukrauh, P.; Hasegawa, H.; Tanaka, Y. A Cadaveric Study of Ulnar Nerve Movement and Strain around the Elbow Joint. Appl. Sci. 2021, 11, 6487. https://doi.org/10.3390/app11146487
Nagashima M, Omokawa S, Nakanishi Y, Mahakkanukrauh P, Hasegawa H, Tanaka Y. A Cadaveric Study of Ulnar Nerve Movement and Strain around the Elbow Joint. Applied Sciences. 2021; 11(14):6487. https://doi.org/10.3390/app11146487
Chicago/Turabian StyleNagashima, Mitsuyuki, Shohei Omokawa, Yasuaki Nakanishi, Pasuk Mahakkanukrauh, Hideo Hasegawa, and Yasuhito Tanaka. 2021. "A Cadaveric Study of Ulnar Nerve Movement and Strain around the Elbow Joint" Applied Sciences 11, no. 14: 6487. https://doi.org/10.3390/app11146487
APA StyleNagashima, M., Omokawa, S., Nakanishi, Y., Mahakkanukrauh, P., Hasegawa, H., & Tanaka, Y. (2021). A Cadaveric Study of Ulnar Nerve Movement and Strain around the Elbow Joint. Applied Sciences, 11(14), 6487. https://doi.org/10.3390/app11146487