
Alexander Technique vs. Targeted Exercise for Neck Pain—A Preliminary Comparison


Abstract

1. Introduction
2. Materials and Methods
2.1. Design
2.2. Participants
2.3. Interventions
2.4. Outcomes
2.4.1. Protocol
2.4.2. Self-Report Measures
2.5. Data Reduction
2.6. Statistical Analysis
3. Results
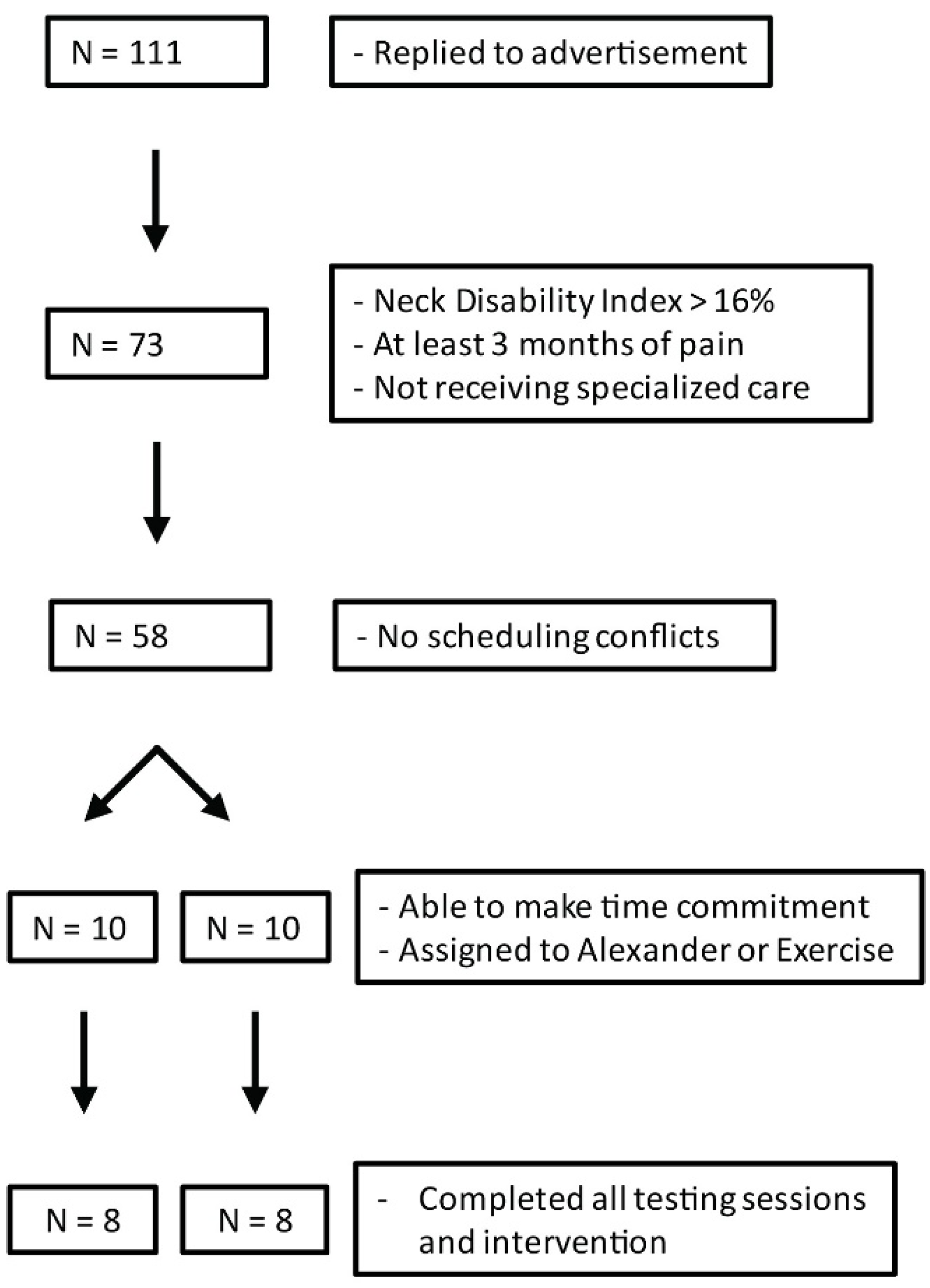
3.1. Recruitment, Screening, and Attendance
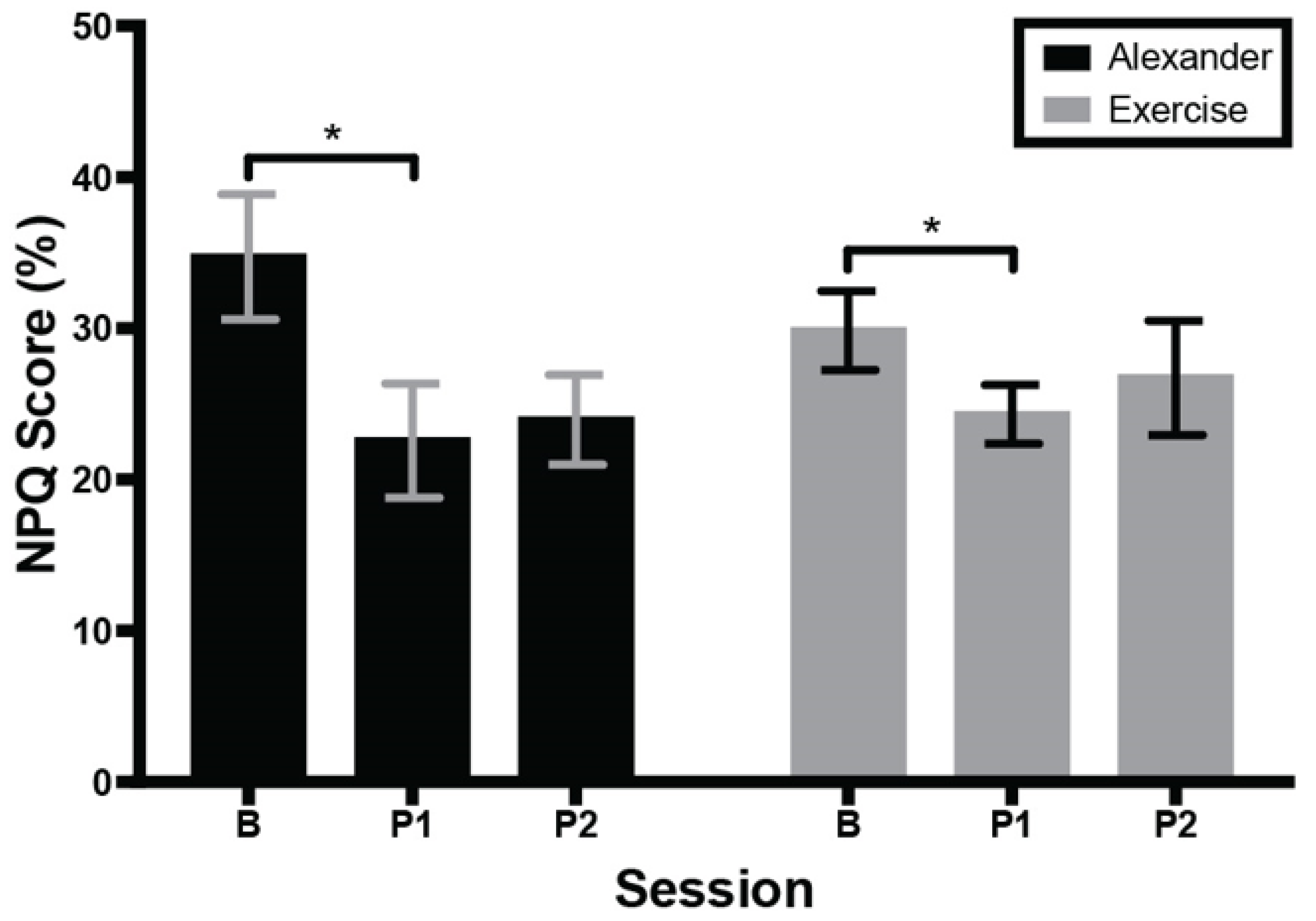
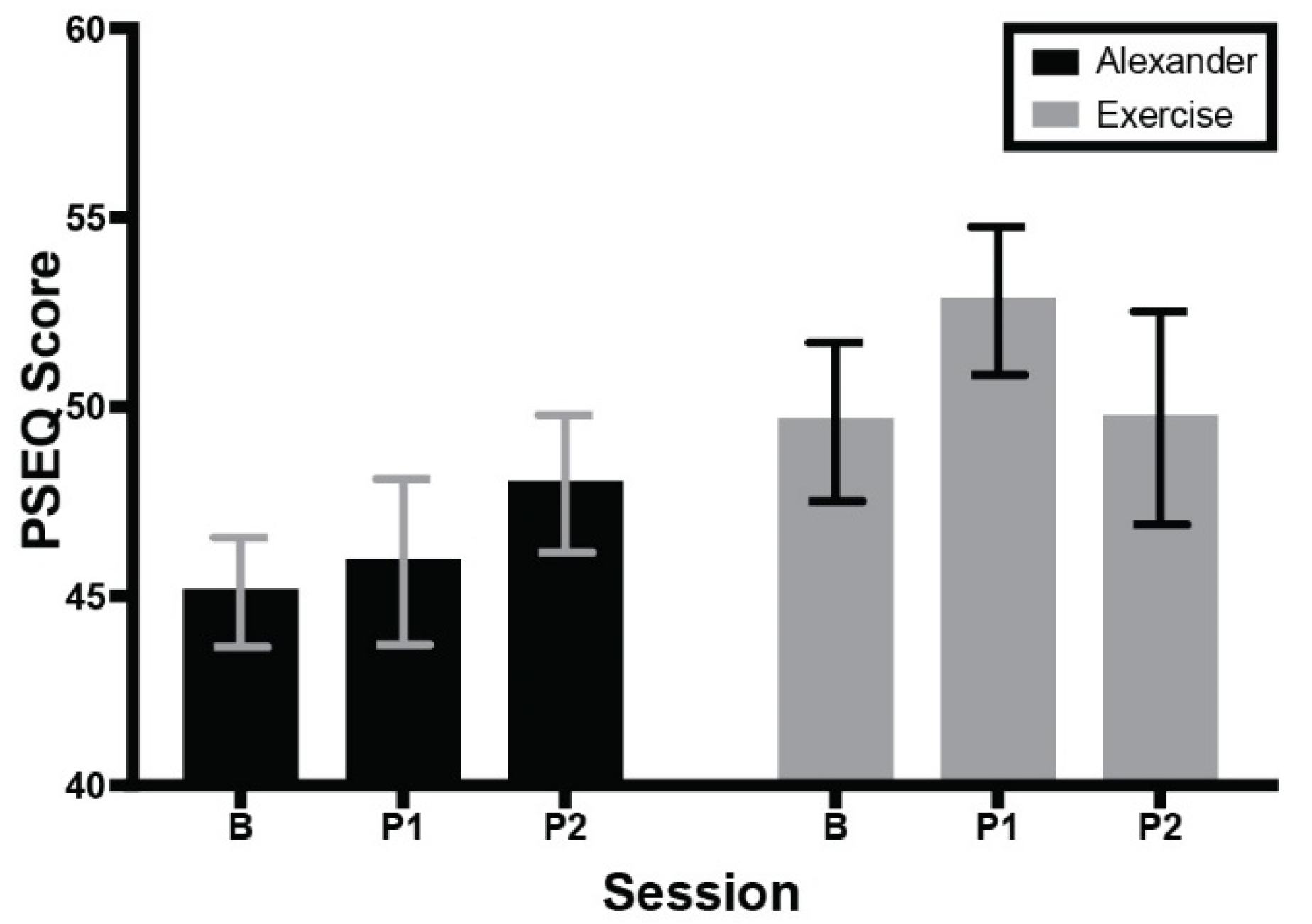
3.2. Self-Reports: Neck Pain, Pain Self-Efficacy, and Course Surveys
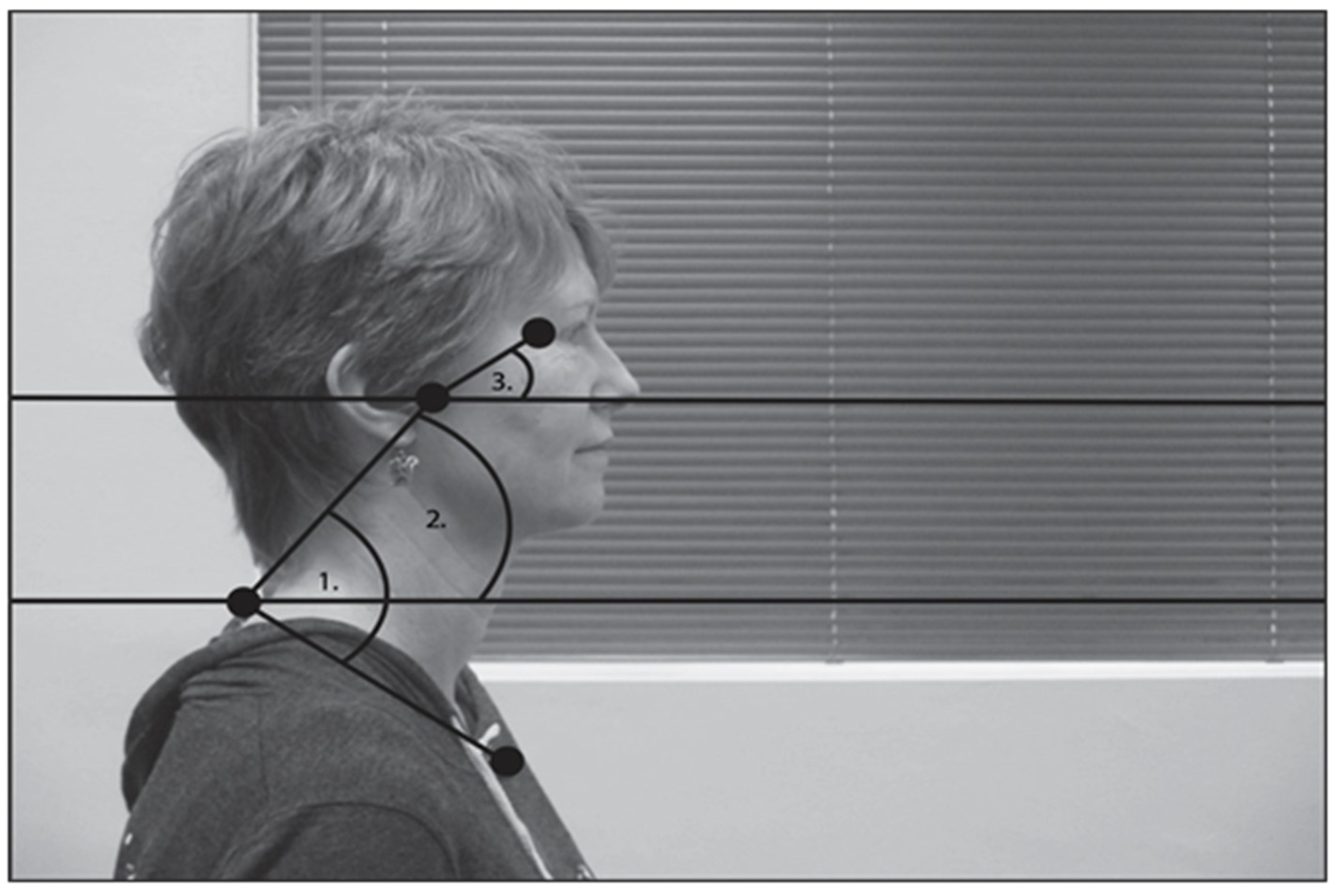
3.3. Posture
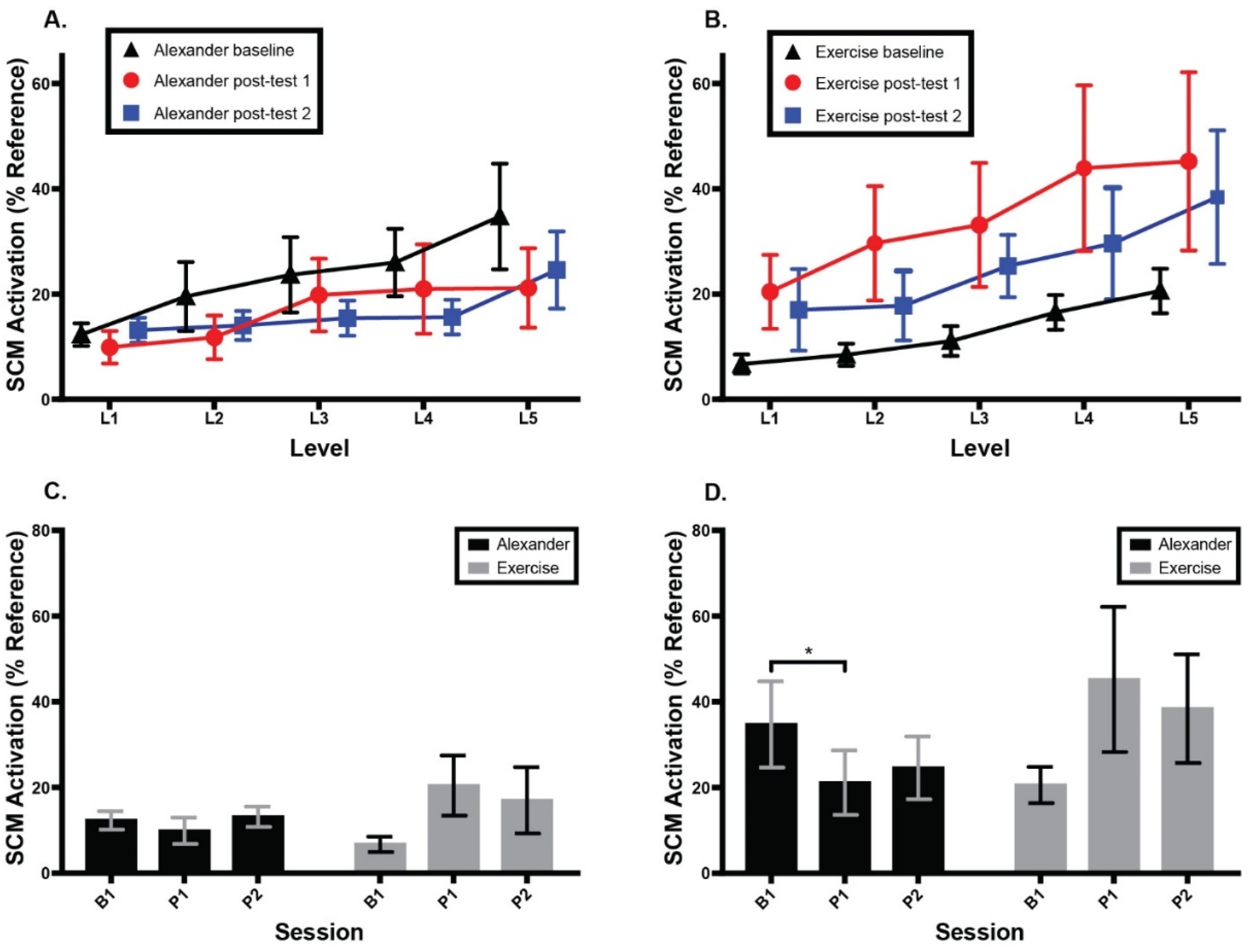
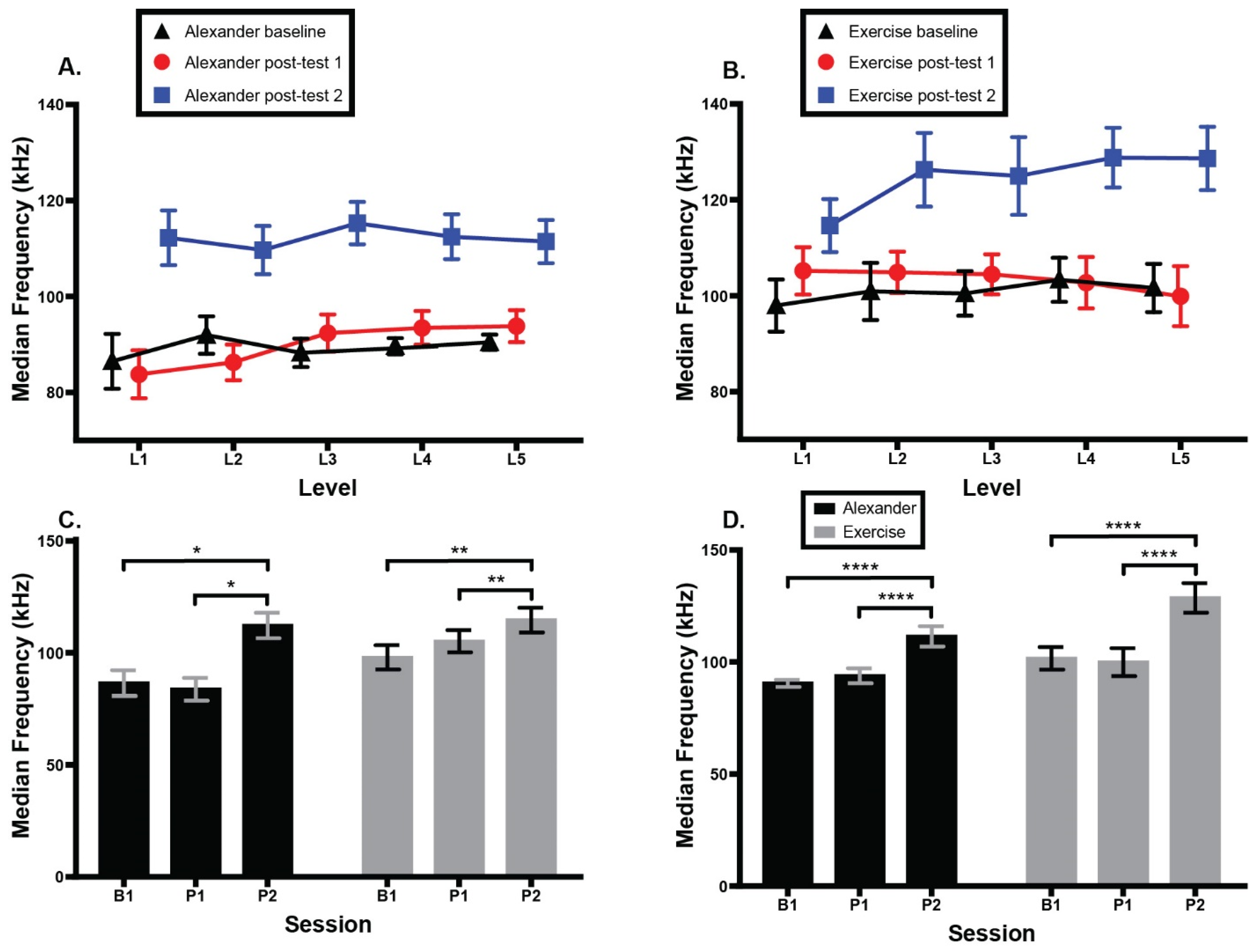
3.4. Sternocleidomastoid Activation
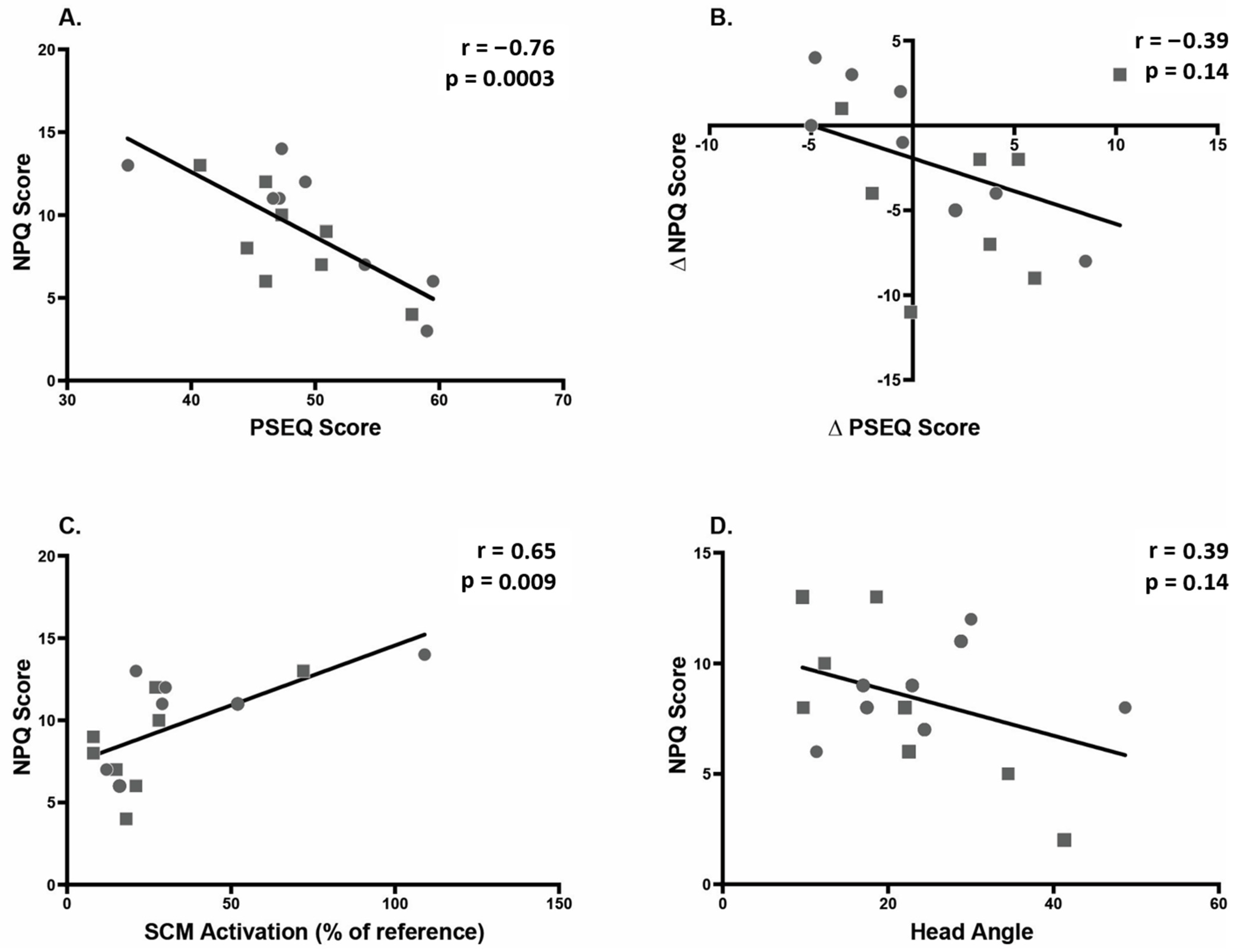
3.5. Correlations
4. Discussion
4.1. Summary of Results
4.2. Relation to Prior Work
4.3. Strengths, Limitations, and Future Directions
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Haldeman, S.; Carroll, L.; Cassidy, J.D. Findings from the bone and joint decade 2000 to 2010 task force on neck pain and its associated disorders. J. Occup. Environ. Med. 2010, 52, 424–427. [Google Scholar] [CrossRef]
- Murray, C.J.; Abraham, J.; Ali, M.K.; Alvarado, M.; Atkinson, C.; Baddour, L.M.; Bartels, D.H.; Benjamin, E.J.; Bhalla, K.; Birbeck, G.; et al. The state of US health, 1990–2010: Burden of diseases, injuries, and risk factors. JAMA 2013, 319, 591–606. [Google Scholar] [CrossRef] [PubMed]
- Dieleman, J.L.; Baral, R.; Birger, M.; Bui, A.L.; Bulchis, A.; Chapin, A.; Hamavid, H.; Horst, C.; Johnson, E.K.; Joseph, J.; et al. US Spending on Personal Health Care and Public Health, 1996–2013. JAMA 2016, 316, 2627–2646. [Google Scholar] [CrossRef]
- United States Bone and Joint Initiative. Burden of Musculoskeletal Diseases in the United States: Prevalence, Societal and Economic Cost, 3rd ed.; United States Bone and Joint Initiative: Rosemont, IL, USA, 2014. [Google Scholar]
- Jensen, M.P.; Solé, E.; Castarlenas, E.; Racine, M.; Roy, R.; Miró, J.; Cane, D. Behavioral inhibition, maladaptive pain cognitions, and function in patients with chronic pain. Scand. J. Pain 2017, 17, 41–48. [Google Scholar] [CrossRef] [PubMed]
- Jull, G.; Sterling, M. Bring back the biopsychosocial model for neck pain disorders. Man. Ther. 2009, 14, 117–118. [Google Scholar] [CrossRef]
- Miles, C.L.; Pincus, T.; Carnes, D.; Taylor, S.J.; Underwood, M. Measuring Pain Self-efficacy. Clin. J. Pain 2011, 27, 461–470. [Google Scholar] [CrossRef]
- Ahmed, S.A.; Shantharam, G.; Eltorai, A.E.; Hartnett, D.A.; Goodman, A.; Daniels, A.H. The effect of psychosocial measures of resilience and self-efficacy in patients with neck and lower back pain. Spine J. 2019, 19, 232–237. [Google Scholar] [CrossRef] [PubMed]
- Mahmoud, N.F.; Hassan, K.A.; Abdelmajeed, S.F.; Moustafa, I.M.; Silva, A.G. The Relationship Between Forward Head Posture and Neck Pain: A Systematic Review and Meta-Analysis. Curr. Rev. Musculoskelet. Med. 2019, 12, 562–577. [Google Scholar] [CrossRef]
- Peolsson, A.; Marstein, E.; McNamara, T.; Nolan, D.; Sjaaberg, E.; Peolsson, M.; Jull, G.; O’Leary, S. Does posture of the cervical spine influence dorsal neck muscle activity when lifting? Man. Ther. 2014, 19, 32–36. [Google Scholar] [CrossRef] [PubMed]
- Cheng, C.-H.; Chien, A.; Hsu, W.-L.; Chen, C.P.-C.; Cheng, H.-Y.K. Investigation of the differential contributions of superficial and deep muscles on cervical spinal loads with changing head postures. PLoS ONE 2016, 11, e0150608. [Google Scholar] [CrossRef]
- Lee, K.-J.; Han, H.-Y.; Cheon, S.-H.; Park, S.-H.; Yong, M.-S. The effect of forward head posture on muscle activity during neck protraction and retraction. J. Phys. Ther. Sci. 2015, 27, 977–979. [Google Scholar] [CrossRef]
- Jull, G.A.; O’Leary, S.P.; Falla, D.L. Clinical Assessment of the Deep Cervical Flexor Muscles: The Craniocervical Flexion Test. J. Manip. Physiol. Ther. 2008, 31, 525–533. [Google Scholar] [CrossRef] [PubMed]
- Falla, D.L.; Jull, G.A.; Hodges, P. Patients With Neck Pain Demonstrate Reduced Electromyographic Activity of the Deep Cervical Flexor Muscles During Performance of the Craniocervical Flexion Test. Spine 2004, 29, 2108–2114. [Google Scholar] [CrossRef]
- Sihawong, R.; Sitthipornvorakul, E.; Paksaichol, A.; Janwantanakul, P. Predictors for chronic neck and low back pain in office workers: A 1-year prospective cohort study. J. Occup. Health 2016, 58, 16–24. [Google Scholar] [CrossRef] [PubMed]
- Jull, G.; Falla, D.; Vicenzino, B.; Hodges, P. The effect of therapeutic exercise on activation of the deep cervical flexor muscles in people with chronic neck pain. Man. Ther. 2009, 14, 696–701. [Google Scholar] [CrossRef] [PubMed]
- Bertozzi, L.; Gardenghi, I.; Turoni, F.; Villafañe, J.H.; Capra, F.; Guccione, A.A.; Pillastrini, P. Effect of therapeutic exercise on pain and disability in the management of chronic nonspecific neck pain: Systematic review and meta-analysis of randomized trials. Phys. Ther. 2013, 93, 1026–1036. [Google Scholar] [CrossRef]
- Campbell, R.; Evans, M.; Tucker, M.; Quilty, B.; Dieppe, P.; Donovan, J.L. Why don’t patients do their exercises? Understanding non-compliance with physiotherapy in patients with osteoarthritis of the knee. J. Epidemiol. Community Health 2001, 55, 132–138. [Google Scholar] [CrossRef] [PubMed]
- Preece, S.J.; Jones, R.K.; Brown, C.A.; Cacciatore, T.W.; Jones, A.K.P. Reductions in co-contraction following neuromuscular re-education in people with knee osteoarthritis. BMC Musculoskelet. Disord. 2016, 17, 1–12. [Google Scholar] [CrossRef]
- Cacciatore, T.W.; Gurfinkel, V.S.; Horak, F.B.; Day, B.L. Prolonged weight-shift and altered spinal coordination during sit-to-stand in practitioners of the Alexander Technique. Gait Posture 2011, 34, 496–501. [Google Scholar] [CrossRef]
- Cacciatore, T.W.; Johnson, P.M.; Cohen, R.G. Potential Mechanisms of the Alexander Technique: Toward a Comprehensive Neurophysiological Model. Kinesiol. Rev. 2020, 9, 1–15. [Google Scholar] [CrossRef]
- Little, P.; Lewith, G.; Webley, F.; Evans, M.; Beattie, A.; Middleton, K.; Barnett, J.; Ballard, K.; Oxford, F.; Smith, P.; et al. Randomised controlled trial of Alexander technique lessons, exercise, and massage (ATEAM) for chronic and recurrent back pain. BMJ 2008, 337, a884. [Google Scholar] [CrossRef]
- MacPherson, H.; Tilbrook, H.; Richmond, S.; Woodman, J.; Ballard, K.; Atkin, K.; Bland, M.; Eldred, J.; Essex, H.; Hewitt, C.; et al. Alexander technique lessons or acupuncture sessions for persons with chronic neck pain: A randomized trial. Ann. Intern. Med. 2015, 163, 653–662. [Google Scholar] [CrossRef]
- Batson, G.; Barker, S. Feasibility of group delivery of the Alexander technique on balance in the community-dwelling elderly: Preliminary findings. Act. Adapt. Aging 2008, 32, 103–119. [Google Scholar] [CrossRef]
- Becker, J.J.; Copeland, S.L.; Botterbusch, E.L.; Cohen, R.G. Preliminary evidence for feasibility, efficacy, and mechanisms of Alexander technique group classes for chronic neck pain. Complement. Ther. Med. 2018, 39, 80–86. [Google Scholar] [CrossRef]
- Cacciatore, T.; Gurfinkel, V.; Horak, F.; Cordo, P.; Ames, K. Increased dynamic regulation of postural tone through Alexander Technique training. Hum. Mov. Sci. 2011, 30, 74–89. [Google Scholar] [CrossRef]
- Steinmetz, A.; Claus, A.; Hodges, P.W.; Jull, G.A. Neck muscle function in violinists/violists with and without neck pain. Clin. Rheumatol. 2016, 35, 1045–1051. [Google Scholar] [CrossRef] [PubMed]
- Cacciatore, T.W.; Horak, F.B.; Henry, S.M. Improvement in automatic postural coordination following Alexander Technique lessons in a person with low back pain. Phys. Ther. 2005, 85, 565–578. [Google Scholar] [CrossRef]
- Bjerken, T.; Mello, B.; Mello, R. Cultivating a lively use of tension: The synergy between acting and the Alexander Technique. Theatr. Danc. Perform. Train. 2012, 3, 27–40. [Google Scholar] [CrossRef]
- Leak, A.M.; Cooper, J.; Dyer, S.; Williams, K.A.; Turner-Stokes, L.; Frank, A.O. The Northwick Park Neck Pain Questionnaire, devised to measure neck pain and disability. Br. J. Rheumatol. 1994, 33, 469–474. [Google Scholar] [CrossRef] [PubMed]
- Nicholas, M.K. The pain self-efficacy questionnaire: Taking pain into account. Eur. J. Pain 2007, 11, 153–163. [Google Scholar] [CrossRef]
- Mayoux-Benhamou, M.A.; Revel, M.; Vallée, C.; Roudier, R.; Barbet, J.P.; Bargy, F. Longus colli has a postural function on cervical curvature. Surg. Radiol. Anat. 1994, 16, 367–371. [Google Scholar] [CrossRef]
- US Department of Labor. Working Safely with Video Display Terminals; Occupational Safety and Health Administration: Washington, DC, USA, 1997.
- Georgakis, A.; Stergioulas, L.K.; Giakas, G. Fatigue analysis of the surface EMG signal in isometric constant force contractions using the averaged instantaneous frequency. IEEE Trans. Biomed. Eng. 2003, 50, 262–265. [Google Scholar] [CrossRef]
- Sim, J.; Jordan, K.; Lewis, M.; Hill, J.; Hay, E.M.; Dziedzic, K. Sensitivity to change and internal consistency of the Northwick Park neck pain questionnaire and derivation of a minimal clinically important difference. Clin. J. Pain 2006, 22, 820–826. [Google Scholar] [CrossRef]
- Woodman, J.; Ballard, K.; Hewitt, C.; MacPherson, H. Self-efficacy and self-care-related outcomes following Alexander Technique lessons for people with chronic neck pain in the ATLAS randomised, controlled trial. Eur. J. Integr. Med. 2018, 17, 64–71. [Google Scholar] [CrossRef] [PubMed]
- Slater, D.; Korakakis, V.; O’Sullivan, P.; Nolan, D.; O’Sullivan, K. ‘Sit Up Straight’: Time to Re-evaluate. J. Orthop. Sport. Phys. Ther. 2019, 49, 562–564. [Google Scholar] [CrossRef]
- Alexander, F.M.; Fischer, J.M.O. The Universal Constant in Living, 1st ed.; Re-Educational Publications:: Mouritz, London, UK, 2000. [Google Scholar]
- McLean, S.M.; Moffett, J.A.K.; Sharp, D.M.; Gardiner, E. A randomised controlled trial comparing graded exercise treatment and usual physiotherapy for patients with non-specific neck pain (the GET UP neck pain trial). Man. Ther. 2013, 18, 199–205. [Google Scholar] [CrossRef]
- Gross, M.; Ravichandra, R.; Cohen, R.; Mello, B. Alexander Technique (AT) Group Classes: Feasible Intervention for Care Partners of People Living With Parkinson’s. Arch. Phys. Med. Rehabil. 2019, 100, 42. [Google Scholar] [CrossRef]
- Gross, M.; Cohen, R.; Ravichandra, R.; Basye, M.; Norcia, M. Poised for Parkinson’s: Alexander Technique Course improves Balance, Mobility and Posture for People with PD. Arch. Phys. Med. Rehabil. 2019, 100, 193. [Google Scholar] [CrossRef]
- Falla, D.L.; Jull, G.; Hodges, P. Training the cervical muscles with prescribed motor tasks does not change muscle activation during a functional activity. Man. Ther. 2008, 13, 507–512. [Google Scholar] [CrossRef] [PubMed]
- Castanharo, R.; Duarte, M.; McGill, S. Corrective sitting strategies: An examination of muscle activity and spine loading. J. Electromyogr. Kinesiol. 2014, 24, 114–119. [Google Scholar] [CrossRef] [PubMed]
- May, S.; Johnson, R. Stabilisation exercises for low back pain: A systematic review. Physiotherapy 2008, 94, 179–189. [Google Scholar] [CrossRef]









{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| AT | EX | ||||
|---|---|---|---|---|---|
| Mean | SD | Mean | SD | p-Value | |
| Sex (F/M) | 4/4 | 5/3 | 0.61 | ||
| NPQ at baseline (%) | 34.7 | 11.7 | 29.9 | 7.4 | 0.34 |
| Sedentary (hrs/day) | 6.1 | 4.6 | 6.9 | 2.6 | 0.70 |
| Age (yrs) | 49.3 | 11.0 | 54.8 | 18.9 | 0.49 |
| Education (yrs past HS) | 5.3 | 3.4 | 7.5 | 3.3 | 0.21 |
| Classes (# attended) | 9.0 | 0.0 | 8.4 | 2.3 | 0.46 |
| AT | EX | p | |
|---|---|---|---|
| 1. The classes were enjoyable. | 9.1 | 8.3 | |
| 2. The material was presented in a clear and understandable way. | 8.3 | 9.0 | |
| 3. I learned about how my movements contribute to my neck pain. | 8.4 | 5.4 | 0.03 |
| 4. I was surprised by some of the things I learned. | 9.0 | 4.1 | 0.001 |
| 5. I learned some practical tools to be more comfortable in my body. | 8.5 | 6.6 | |
| 6. I am likely to remember what I learned. | 8.0 | 7.1 | |
| 7. I am likely to continue to practice what I learned. | 7.8 | 6.0 | |
| 8. I enjoyed the interaction with my fellow-students. | 8.9 | 8.2 | |
| 9. I would refer a friend to this class. | 8.8 | 6.9 | |
| 10. I would pay for continuing classes if they were available. | 6.1 | 4.0 | |
| 11. I would have preferred a private lesson format. | 1.9 | 3.6 | |
| 12. I would have preferred a class that met only once per week. | 3.0 | 3.9 | |
| 13. I would have preferred a class that met more than twice per week. | 1.0 | 3.1 | |
| 14. I would have preferred to meet in a more “healing” environment such as a yoga studio. | 3.4 | 3.1 | |
| 15. I would have preferred a class with a more structured format. | 1.5 | 2.8 |
| Never or A Few Times | Weekly or Every Few Days | Daily or More Often | p | ||
|---|---|---|---|---|---|
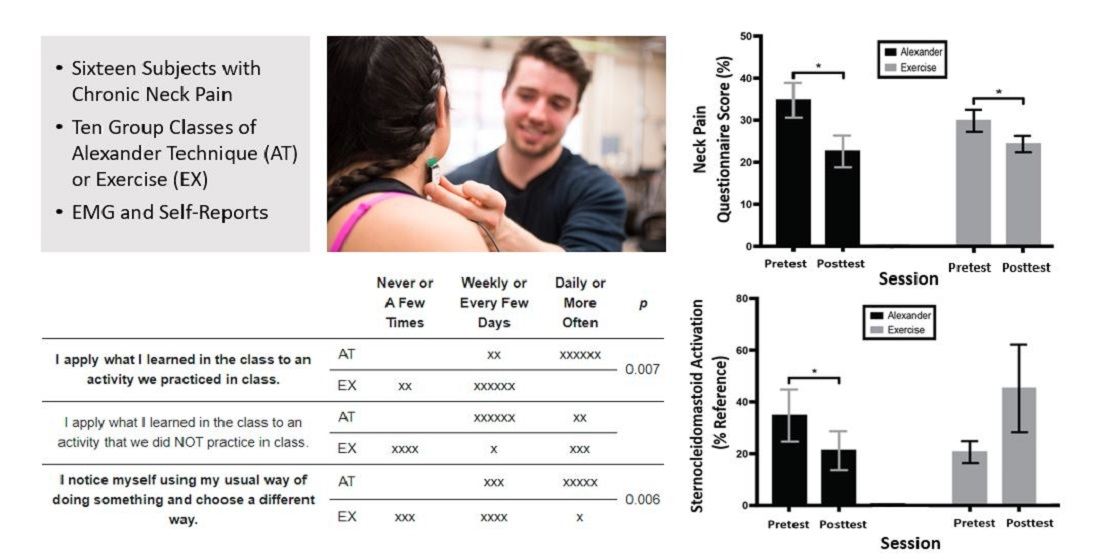
| I apply what I learned in the class to an activity we practiced in class. | AT | xx | xxxxxx | 0.007 | |
| EX | xx | xxxxxx | |||
| I apply what I learned in the class to an activity that we did NOT practice in class. | AT | xxxxxx | xx | ||
| EX | xxxx | x | xxx | ||
| I notice myself using my usual way of doing something and choose a different way. | AT | xxx | xxxxx | 0.006 | |
| EX | xxx | xxxx | x |
| Predictor | Correlation with NPQ at Baseline | Correlation with NPQ at Post-Test | Correlation of Change in NPQ with Change in Predictor |
|---|---|---|---|
| Pain self-efficacy | 0.04 (0.40) | P1: −0.38 (0.07) P2: −0.76 (0.0003) | P1-B1: 0.08 (0.40) P2-B1: −0.39 (0.14) |
| Head–torso angle | 0.06 (0.08) | P1:0.23 (0.39) P2: 0.15 (0.58) | P1-B1: −0.17 (0.58) P2-B1: −0.05 (0.85) |
| Head angle | −0.36 (0.17) | P1: −0.39 (0.14) P2: 0.07 (0.80) | P1-B1: 0.03 (0.90) P2-B1: 0.03 (0.90) |
| Neck angle | 0.13 (0.63) | P1: 0.25 (0.35) P2: −0.12 (0.65) | P1-B1: −0.04 (0.90) P2-B1: −0.08 (0.77) |
| Muscle amplitude | −0.04 (0.88) | P1: 0.23 (0.41) P2: 0.65 (0.009) | P1-B1: −0.08 (0.77) P2-B1: 0.19 (0.48) |
| Muscle frequency | −0.10 (0.72) | P1: 0.19 (0.50) P2: 0.21 (0.45) | P1-B1: 0.28 (0.31) P2-B1: 0.12 (0.67) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Becker, J.J.; McIsaac, T.L.; Copeland, S.L.; Cohen, R.G. Alexander Technique vs. Targeted Exercise for Neck Pain—A Preliminary Comparison. Appl. Sci. 2021, 11, 4640. https://doi.org/10.3390/app11104640
Becker JJ, McIsaac TL, Copeland SL, Cohen RG. Alexander Technique vs. Targeted Exercise for Neck Pain—A Preliminary Comparison. Applied Sciences. 2021; 11(10):4640. https://doi.org/10.3390/app11104640
Chicago/Turabian StyleBecker, Jordan J., Tara L. McIsaac, Shawn L. Copeland, and Rajal G. Cohen. 2021. "Alexander Technique vs. Targeted Exercise for Neck Pain—A Preliminary Comparison" Applied Sciences 11, no. 10: 4640. https://doi.org/10.3390/app11104640
APA StyleBecker, J. J., McIsaac, T. L., Copeland, S. L., & Cohen, R. G. (2021). Alexander Technique vs. Targeted Exercise for Neck Pain—A Preliminary Comparison. Applied Sciences, 11(10), 4640. https://doi.org/10.3390/app11104640