1. Introduction
Spastic diplegic cerebral palsy (CP) is characterized by impaired motor control on both sides of the body with shortened or improperly developed muscles, and impaired joint movement in both lower extremities [
1,
2,
3,
4,
5,
6]. These impairments impact directly on the body’s mobility and stability throughout the gait cycle [
7], not only for body-weight support during single-limb support (SLS), but also for body-weight transfer during double-limb support (DLS). In particular, during DLS, both limbs are on the ground, forming a closed kinetic chain. Thus, well-coordinated joint controls, both intra- and inter-limb, are needed for smooth and stable body-weight transfer and balance control during gait. Since the lower limbs exchange the roles of leading and trailing limbs between DLS phases, bilateral symmetry of the lower limb kinematics and kinetics is essential for walking. Tendon release surgery (TRS) lengthens the affected muscle-tendon unit to treat the motor dysfunctions and has been shown to help improve ranges of motion of lower limb joints during gait in children with spastic diplegic CP [
8,
9,
10,
11]. Evaluation of the efficacy of the TRS on the inter-limb coordination and bilateral symmetry in body-weight transfer and balance control during CP gait is needed.
Motion analysis technologies have been used to identify the deviations of pathological gait, as well as treatment effects on the affected limb during different phases of gait [
8,
9,
10,
11]. Generally, deviations in CP gait involve complex interactions of the lower limb joints that are affected by factors such as muscle tightness, bony deformity and impaired motor control. Evaluating the disease progression and treatment efficacy in terms of deviations of individual joints can be very challenging [
12], especially when attempting to identify the between-limb interactions. Thus, very few studies have examined how the lower limbs coordinate with each other for the observed gait patterns, especially during weight transfer between limbs in DLS. Previous studies have shown that leg stiffness, incorporating information of both the kinematics and kinetics of the lower limb joints, is a useful measure and should be included in future clinical gait analysis for a more complete assessment of gait in children with CP [
13,
14,
15]. For assessing the effects of pathology and the efficacy of TRS on the inter-limb coordination and bilateral symmetry in body-weight transfer and balance control during CP gait, quantitative analysis of leg stiffness during the phases of gait for both limbs can be a useful approach.
The control of the lower limbs as a whole in supporting the body during gait can be modeled as a mass-spring system with a point body-mass supported by the leg simulated as a non-linear spring. To support the body against collapse and to meet the demands of movement during the stance phase of gait, the stiffness of the spring (called leg stiffness) can be controlled by changing the joint torques provided by the musculotendinous units (i.e., net internal moments) and thus the skeletal alignment of the lower limb. The changes in the leg stiffness describe the modulation of the motions and joint loads of the lower limbs, and thus are useful in assessing pathology and treatment efficacy [
15,
16,
17]. For example, leg stiffness has been used to study the effects of disease on the control of the lower limbs as a whole during walking [
15,
16,
17], and the efficacy of treatment in children with CP, showing unaltered leg stiffness but significantly decreased joint stiffness at the hip and knee after TRS [
13]. The improvement in the joint kinematics and kinetics of the lower limb may either change the coordination between limbs (change of biomechanical condition) or remain unchanged (maintain walking habits), which are not easily revealed through traditional gait analysis variables. Quantifying the inter-limb sharing during DLS phases of gait and bilateral symmetry of the total leg stiffness will be useful for assessing the overall effects of TRS on gait performance and lower limb control in children with diplegic CP. However, no such study has been reported in the literature.
The purposes of this study were to quantify the inter-limb sharing and bilateral symmetry of the total leg stiffness during gait in children with diplegic CP, and to identify the changes of such features of total leg stiffness before and after TRS. It was hypothesized that the CP group would show altered inter-limb sharing of total leg stiffness with bilateral asymmetry during weight-transfer during gait, which would be improved to be similar to controls after TRS.
2. Materials and Methods
2.1. Subjects
Ten boys with spastic diplegic cerebral palsy (CP group, age: 10.3 ± 5.7 years; height: 123.8 ± 24.8 cm; mass: 30.0 ± 15.0 kg) from the outpatient orthopedic clinic, and ten healthy controls (Control group, age: 11.2 ± 2.5 years; height: 142.3 ± 12.6 cm; mass: 35.2 ± 9.4 kg) were recruited between August 2016 and July 2019 to participate in the current study. Informed written consent signed by the subject and his legal guardians was obtained from all subjects, as approved by the Institutional Review Board. A subject was included in the CP group if he was graded I–III in the Gross Motor Function Classification System (GMFCS) with moderate to normal muscle strength and mild to normal muscle tone and was able to walk independently without an assistive device. A subject was excluded if he had noticeable leg length discrepancy, serious muscle contractures, joint deformities, or any other pathological conditions that might affect gait. Each subject in the CP group received TRS on the gastrocnemius and hamstrings performed by a senior orthopedic surgeon (T.M. Wang). The healthy controls were all free from any musculoskeletal, neurological or cardiovascular disorders. Power analysis based on pilot results using GPOWER [
18] for the comparison of the leg stiffness for two-group independent
t-tests showed that a projected sample size of seven subjects would be needed for each group for a power of 0.8 and a large effect size (Cohen’s d = 0.88) at α = 0.05. Thus, ten subjects for each group were considered adequate for the current study.
2.2. Experimental Protocol
In a gait laboratory, each subject walked at his preferred speed on a 10 m walkway while wearing 39 retro-reflective markers placed on specific anatomical landmarks to track the motions of the body segments [
19]. The 3D trajectories of the markers were measured at 200 Hz using an 8-camera optical tracking system (Vicon T-40, OMG, Oxford, UK), and three forceplates (OR6-7-2000, AMTI, Watertown, MA, USA) were used to measure the ground reaction forces (GRF) at 2000 Hz [
20,
21]. For subsequent analysis, data of six gait cycles (three for each limb) were obtained from the Control group and from the CP group before TRS and an average of ten months (±1 month) after TRS.
2.3. Data Analysis
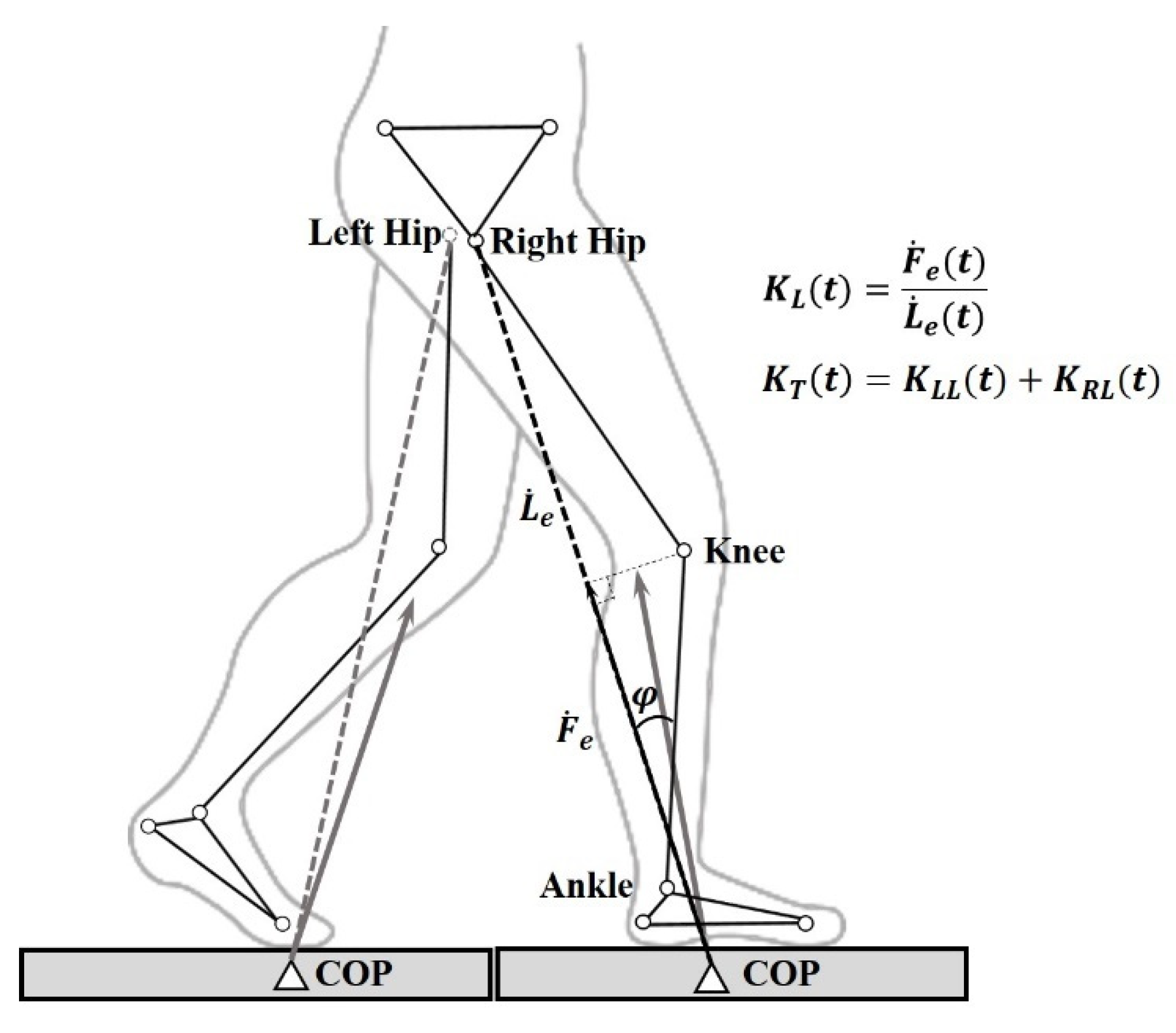
For calculating the leg stiffness (
KL), the lower limb was modeled as a non-linear spring, connecting the center of pressure (COP) of the GRF and the hip joint center (
Figure 1). During walking, the varying
KL was calculated as the gradients of the force-deformation curve [
15]. The total leg stiffness (
KT) was then obtained as the sum of the leg stiffness values of both sides, and the proportional share of the total leg stiffness (
KS) by a lower limb over time was calculated during the double-limb support phases of gait (i.e., loading response, LR, and pre-swing, PS) as follows (
Figure 1 and
Figure 2):
The proportional share,
KS(
t), was then time-averaged over the double-limb support phases of gait (i.e., LR and PS). The symmetry index (SI (%)) of bilateral
KL was calculated for each gait phase as follows:
where
KLL was the leg stiffness of the left leg,
KRL was the leg stiffness of the right leg and the integrations were over the subphases of loading response (LR or initial DLS), mid-stance (MS), terminal stance (TS) and pre-swing (PS or terminal DLS) (
Figure 2). While an SI of zero indicated perfect bilateral symmetry, the greater the SI value, the greater the bilateral asymmetry in leg stiffness. Temporal-spatial parameters were also obtained, namely gait speed (normalized to leg length), cadence, stride time, stride length (normalized to leg length) and step width.
2.4. Statistical Analysis
Independent t-tests were performed to compare the variables between Control and CP groups, before TRS (Control vs. Pre-OP) and after TRS (Control vs. Post-OP). Paired t-tests were used to compare variables of the CP group between Pre-OP and Post-OP. A significance level of 0.05 was set for all the tests. All the statistical analyses were performed using SPSS version 20.0 (SPSS Inc., IBM, Armonk, NY, USA).
3. Results
Before TRS, the CP group walked at significantly decreased speed with increased step width when compared to Control. TRS tended to increase the gait speed in the CP group, with significantly increased stride time and decreased cadence (
p < 0.05) as compared to Control (
Table 1).
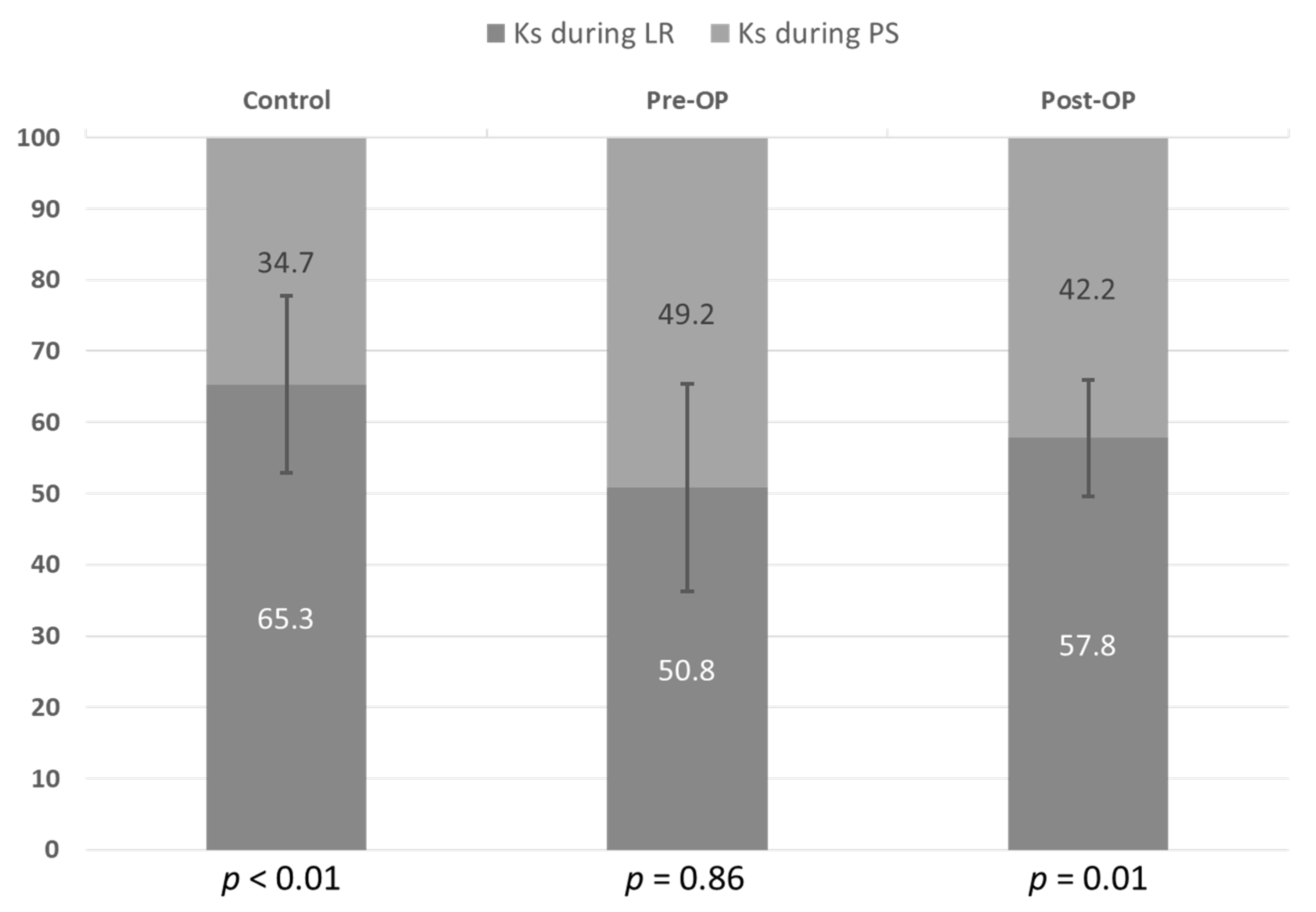
No significant differences in time-averaged values of
KL and
KT over LR and PS were found between CP and Control (
Table 2). In the healthy Controls, the limb shared greater
KT during LR than during PS (
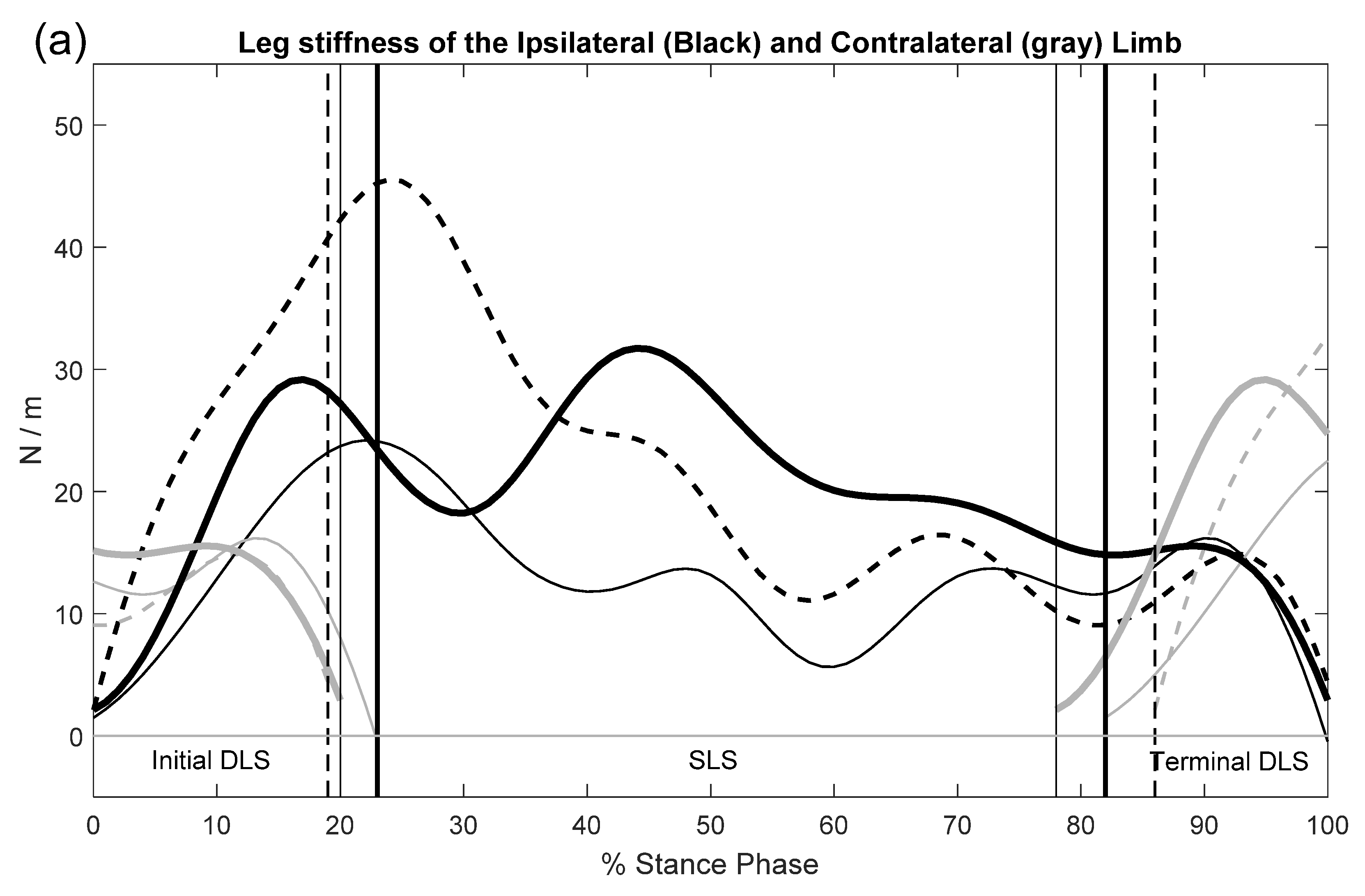
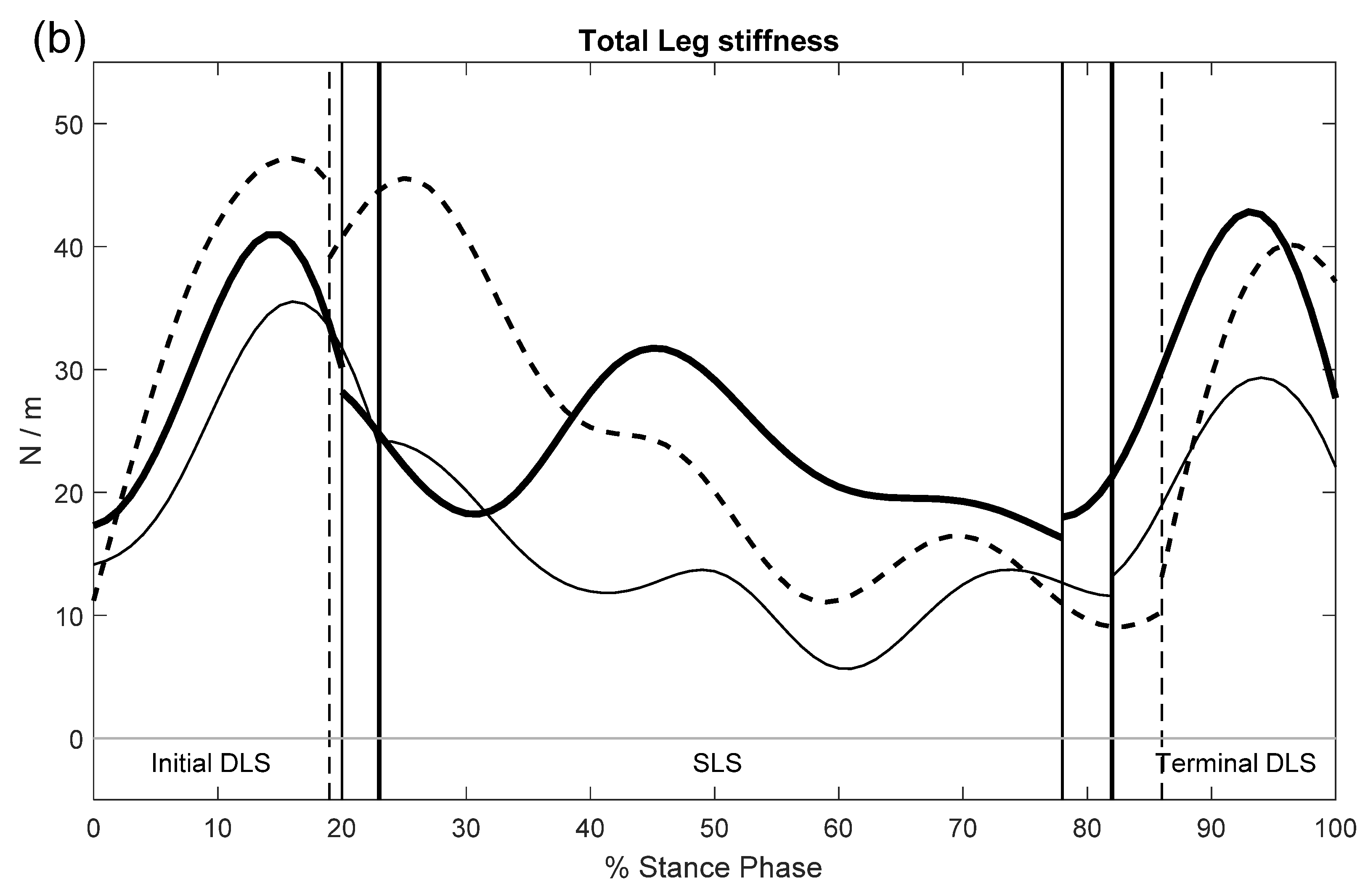
Figure 3 and
Figure 4a,b). Compared to Control, the CP group showed significantly decreased
KS during LR but increased
KS during PS before surgery (Pre-OP) (
Table 2), resulting in similar
KS between LR and PS within the CP group (
Figure 3 and
Figure 4a,b,
Table 2). After surgery, the CP group showed significantly greater
KS during LR than during PS (
Figure 3 and
Figure 4a,b,
Table 2).
Compared to Control, the CP group showed significantly increased SI values during MS, TS and PS phases before TRS (Pre-OP). Generally, TRS tended to reduce the SI values during MS, TS and PS, reaching statistical significance for TS (
Table 3). After TRS, no significant differences in SI between Control and CP (Post-OP) were found throughout the whole gait cycle (
Table 3).
4. Discussion
The current study aimed to quantify the inter-limb sharing of the total leg stiffness, and the bilateral symmetry in leg stiffness, while supporting the body against collapse during the stance phase of gait in children with diplegic CP before and after TRS. Before TRS, the children with diplegic CP walked with a decreased share of total leg stiffness during weight-acceptance and increased bilateral leg stiffness asymmetry during single-limb support and weight-transfer during gait when compared to healthy Controls. The asymmetry in bilateral leg stiffness was significantly reduced in the CP group, especially in the terminal stance phase, with inter-limb sharing of total leg stiffness becoming similar to that of Controls. The results supported the hypothesis that the CP group would walk with improved, close-to-normal bilateral symmetry and inter-limb sharing of leg stiffness after tendon release surgery.
Double-limb support (DLS) is the key feature of human walking as opposed to running, enabling the body-weight transfer between the lower limbs for the subsequent single-limb support and swing of the contralateral limb for continuous progression of the body. Smooth and stable transfer of the body weight during DLS relies on the highly coordinated kinematic and kinetic interactions of the lower limbs, the quality of which could be used to evaluate the roles of the lower limbs in the control of the whole-body balance during gait. During loading response (weight-acceptance), the CP group showed a significantly decreased share of the total leg stiffness without a significant difference in the bilateral leg stiffness symmetry before TRS when compared to the Controls. The healthy Controls were expected to sustain greater stiffness and share of the total leg stiffness during weight-acceptance than the CP group was, which could be beneficial for preventing collapse when facing a sudden load during this phase of gait. However, the tightness of the musculotendinous units in the CP group led them to walk with more flexed lower limbs, and with an increased muscular effort (i.e., net internal joint moments) [
15], which appeared to contribute to the decrease in the total leg stiffness sharing in the weight-acceptance limb. TRS increased the total leg stiffness sharing during loading response, which may be related to previously reported benefits of TRS, including improvement of dynamic lower limb alignment, impact absorption, smoothness of body-weight transfer with reduced energy expenditure and improved endurance [
22,
23].
During pre-swing (weight-release), the task is to transfer the body weight from the support limb to the contralateral limb. Before TRS, the CP group showed a significantly increased share of the total leg stiffness and bilateral stiffness asymmetry when compared to the Controls. These results suggest that the patients kept the body weight more on the trailing support limb during pre-swing, showing a more cautious but less smooth pattern of weight transfer to the contralateral limb. After TRS, the stiffness-sharing was decreased and the transfer of the body weight to the leading stance limb became easier. The reduced asymmetry also suggests improved muscle and joint conditions between limbs, as well as overall gait improvement after TRS.
During SLS, the TRS was found to improve the symmetry of bilateral leg stiffness, which would help decrease the risk of collapse of the lower limbs when supporting the body weight for dynamic balance during gait in the children with diplegic CP. Generally, children with spastic diplegic CP showed reduced leg stiffness with increased joint stiffness during SLS, which was related to the more flexed posture of the stance limb [
15]. Variability of the degrees and severity of impairment of the muscles and joints often leads to bilateral mechanical asymmetry in children with spastic diplegic CP. The TRS improved the alignment and musculotendinous conditions of both the lower extremities, which in turn improved the bilateral symmetry in leg stiffness.
The current study was the first attempt to quantify the effects of TRS on the inter-limb sharing of the total leg stiffness during DLS and bilateral symmetry in the leg stiffness throughout the gait cycle in children with diplegic CP. Further study may be needed to test whether similar effects also exist in children with spastic hemiplegic CP. The gait data of patients were collected before and an average of 10 months after surgery. Similar time intervals post-surgery for gait analysis were also found in previous CP gait studies [
24,
25], as muscle weakness due to surgery would normally resolve within 6–9 months [
26]. Further gait analyses at different time intervals post-surgery may be needed for a more complete picture of how inter-limb sharing of the total leg stiffness and bilateral symmetry in leg stiffness would change over time.
5. Conclusions
The modulation of the sharing of the total leg stiffness between the lower limbs during DLS and the bilateral symmetry in leg stiffness throughout the gait cycle in children with diplegic CP who had undergone TRS was revealed in the current study. Before TRS, the CP group had greater stiffness-sharing in the weight-release limbs and asymmetry between lower limbs during gait. The surgery seemed to improve their lower limb control and increased the bilateral limb symmetry during gait. The current results suggest that an analysis of the symmetry in bilateral leg stiffness and stiffness-sharing will be useful for a more complete gait assessment in children with CP.
Author Contributions
Conceptualization: T.-W.L. and C.-C.K.; Methodology: T.-W.L., T.-M.W. and H.-P.H.; Formal analysis and investigation: H.-Y.L. and T.-Y.C.; Writing—original draft preparation: T.-W.L. and H.-P.H.; Writing—review and editing: C.-C.K. and T.-M.W.; Funding acquisition: T.-M.W.; Resources: C.-C.K.; Supervision: T.-W.L. All authors have read and agreed to the published version of the manuscript.
Funding
This research was financially supported by the Ministry of Science and Technology of Taiwan (103-2221-E-002-169).
Institutional Review Board Statement
The study was conducted according to the guidelines of the Declaration of Helsinki and approved by the Research Ethics Committee of National Taiwan University Hospital (protocol code: 201605138RIND and date of approval: 28 June 2016).
Informed Consent Statement
Informed consent was obtained from all subjects involved in the study.
Data Availability Statement
The datasets used and/or analyzed during the current study are available from the corresponding author on reasonable request.
Conflicts of Interest
The authors declare no conflict of interest.
References
- Engsberg, J.R.; Ross, S.A.; Olree, K.S.; Park, T.S. Ankle spasticity and strength in children with spastic diplegic cerebral palsy. Dev. Med. Child Neurol. 2000, 42, 42–47. [Google Scholar] [CrossRef] [PubMed]
- Lin, C.J.; Guo, L.Y.; Su, F.C.; Chou, Y.L.; Cherng, R.J. Common abnormal kinetic patterns of the knee in gait in spastic diplegia of cerebral palsy. Gait Posture 2000, 11, 224–232. [Google Scholar] [CrossRef]
- McNee, A.E.; Shortland, A.P.; Eve, L.C.; Robinson, R.O.; Gough, M. Lower limb extensor moments in children with spastic diplegic cerebral palsy. Gait Posture 2004, 20, 171–176. [Google Scholar] [CrossRef]
- Carriero, A.; Zavatsky, A.; Stebbins, J.; Theologis, T.; Shefelbine, S.J. Correlation Between Lower Limb Bone Morphology and Gait Characteristics in Children With Spastic Diplegic Cerebral Palsy. J. Pediatr. Orthop. 2009, 29, 73–79. [Google Scholar] [CrossRef]
- Gaston, M.S.; Rutz, E.; Dreher, T.; Brunner, R. Transverse plane rotation of the foot and transverse hip and pelvic kinematics in diplegic cerebral palsy. Gait Posture 2011, 34, 218–221. [Google Scholar] [CrossRef]
- Goldberg, E.J.; Requejo, P.S.; Fowler, E.G. Joint moment contributions to swing knee extension acceleration during gait in individuals with spastic diplegic cerebral palsy. Gait Posture 2011, 33, 66–70. [Google Scholar] [CrossRef]
- Wu, S.K.; You, J.Y.; Chen, H.Y.; Lou, S.Z. Gastrocnemius Tightness Affects Hip and Pelvic Movement in Gait. Biomed. Eng.-Appl. Basis Commun. 2020, 32, 8. [Google Scholar] [CrossRef]
- Abel, M.F.; Damiano, D.L.; Pannunzio, M.; Bush, J. Muscle-tendon surgery in diplegic cerebral palsy: Functional and mechanical changes. J. Pediatr. Orthop. 1999, 19, 366–375. [Google Scholar] [CrossRef]
- Bialik, G.M.; Pierce, R.; Dorociak, R.; Lee, T.S.; Aiona, M.D.; Sussman, M.D. Iliopsoas Tenotomy at the Lesser Trochanter Versus at the Pelvic Brim in Ambulatory Children With Cerebral Palsy. J. Pediatr. Orthop. 2009, 29, 251–255. [Google Scholar] [CrossRef]
- Presedo, A.; Megrot, F.; Ilharreborde, B.; Mazda, K.; Pennecot, G.F. Rectus Femoris Distal Tendon Resection Improves Knee Motion in Patients With Spastic Diplegia. Clin. Orthop. Relat. Res. 2012, 470, 1312–1319. [Google Scholar] [CrossRef][Green Version]
- Vegvari, D.; Wolf, S.I.; Heitzmann, D.; Klotz, M.C.M.; Dreher, T. Does Proximal Rectus Femoris Release Influence Kinematics In Patients With Cerebral Palsy and Stiff Knee Gait? Clin. Orthop. Relat. Res. 2013, 471, 3293–3300. [Google Scholar] [CrossRef]
- Õunpuu, S.; Davis, R.B.; DeLuca, P.A. Joint kinetics: Methods, interpretation and treatment decision-making in children with cerebral palsy and myelomeningocele. Gait Posture 1996, 4, 62–78. [Google Scholar] [CrossRef]
- Kuo, C.C.; Huang, H.P.; Wang, T.M.; Hong, S.W.; Hung, L.W.; Kuo, K.N.; Lu, T.W. Tendon release reduced joint stiffness with unaltered leg stiffness during gait in spastic diplegic cerebral palsy. PLoS ONE 2021, 16, e0245616. [Google Scholar] [CrossRef] [PubMed]
- Huang, H.P.; Kuo, C.C.; Lu, T.W.; Wu, K.W.; Kuo, K.N.; Wang, T.M. Bilateral symmetry in leg and joint stiffness in children with spastic hemiplegic cerebral palsy during gait. J. Pediatr. Orthop. 2020, 38, 2006–2014. [Google Scholar] [CrossRef] [PubMed]
- Wang, T.M.; Huang, H.P.; Li, J.D.; Hong, S.W.; Lo, W.C.; Lu, T.W. Leg and Joint Stiffness in Children with Spastic Diplegic Cerebral Palsy during Level Walking. PLoS ONE 2015, 10, e0143967. [Google Scholar] [CrossRef]
- Silder, A.; Whittington, B.; Heiderscheit, B.; Thelen, D.G. Identification of passive elastic joint moment-angle relationships in the lower extremity. J. Biomech. 2007, 40, 2628–2635. [Google Scholar] [CrossRef]
- Shamaei, K.; Sawicki, G.S.; Dollar, A.M. Estimation of quasi-stiffness and propulsive work of the human ankle in the stance phase of walking. PLoS ONE 2013, 8, e59935. [Google Scholar] [CrossRef]
- Erdfelder, E.; Faul, F.; Buchner, A. GPOWER: A general power analysis program. Behav. Res. Methods Instrum. Comput. 1996, 28, 1–11. [Google Scholar] [CrossRef]
- Wu, K.W.; Wang, T.M.; Hu, C.C.; Hong, S.W.; Lee, P.A.; Lu, T.W. Postural adjustments in adolescent idiopathic thoracic scoliosis during walking. Gait Posture 2019, 68, 423–429. [Google Scholar] [CrossRef]
- Chien, H.L.; Lu, T.W.; Liu, M.W. Effects of long-term wearing of high-heeled shoes on the control of the body’s center of mass motion in relation to the center of pressure during walking. Gait Posture 2014, 39, 1045–1050. [Google Scholar] [CrossRef]
- Hsieh, H.-J.; Lu, T.-W.; Chen, S.-C.; Chang, C.-M.; Hung, C. A new device for in situ static and dynamic calibration of force platforms. Gait Posture 2011, 33, 701–705. [Google Scholar] [CrossRef] [PubMed]
- Dahlback, G.O.; Norlin, R. The Effect of Corrective Surgery on Energy-Expenditure during Ambulation in Children with Cerebral-Palsy. Eur. J. Appl. Physiol. Occup. Physiol. 1985, 54, 67–70. [Google Scholar] [CrossRef] [PubMed]
- Marconi, V.; Hachez, H.; Renders, A.; Docquier, P.L.; Detrembleur, C. Mechanical work and energy consumption in children with cerebral palsy after single-event multilevel surgery. Gait Posture 2014, 40, 633–639. [Google Scholar] [CrossRef] [PubMed]
- Ancillao, A.; van der Krogt, M.M.; Buizer, A.I.; Witbreuk, M.M.; Cappa, P.; Harlaar, J. Analysis of Gait Patterns Pre- and Post-Single Event Multilevel Surgery in children with Cerebral Palsy by means of Offset-Wise Movement Analysis Profile and Linear Fit Method. Hum. Mov. Sci. 2017, 55, 145–155. [Google Scholar] [CrossRef]
- Lee, E.H.; Goh, J.C.; Bose, K. Value of gait analysis in the assessment of surgery in cerebral palsy. Arch. Phys. Med. Rehabil. 1992, 73, 642–646. [Google Scholar]
- Ying, C.T.Q.; Hong, S.L.W.; Lee, B.H.; Thevendran, G. Return to physical activity after gastrocnemius recession. World J. Orthop. 2016, 7, 746–751. [Google Scholar] [CrossRef]
| Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).


 and
and 






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}