
Occupational Radiation Dose, Especially for Eye Lens: Hp(3), in Medical Staff Members Involved in Computed Tomography Examinations

 ,
,  ,
, 
Abstract
1. Introduction
2. Materials and Methods
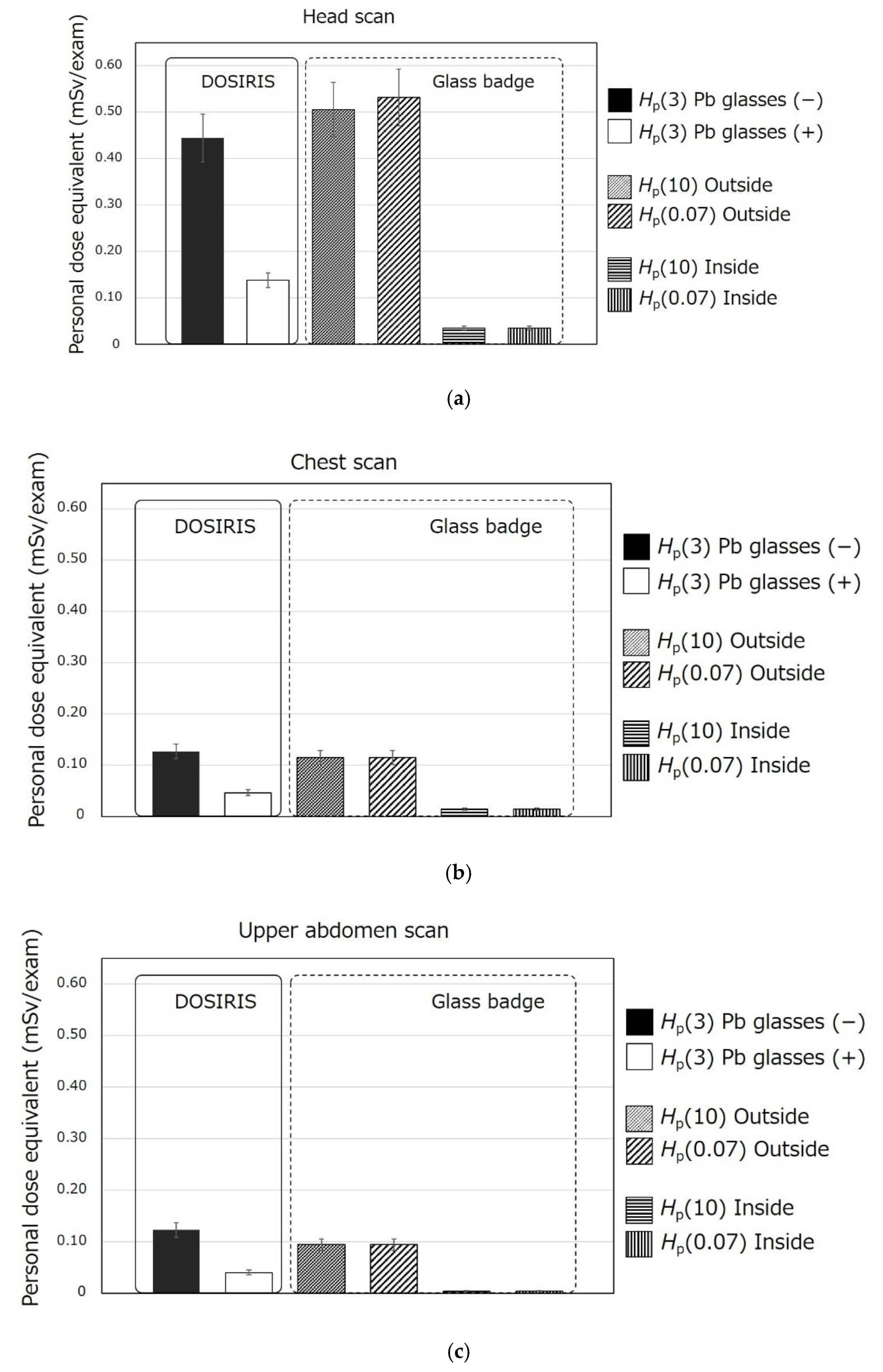
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Theumann, N.H.; Verdun, F.R.; Valley, J.F.; Capasso, P.; Schnyder, P.; Meuli, R.A. Radiation doses delivered to radiologists during contrast-enhanced helical-CT examinations. Eur. Radiol. 1999, 9, 1919–1922. [Google Scholar] [CrossRef] [PubMed]
- Al-Haj, A.N.; Lobriguito, A.M.; Lagarde, C.S. Occupational doses during the injection of contrast media in paediatric CT procedures. Radiat. Prot. Dosim. 2003, 103, 169–172. [Google Scholar] [CrossRef] [PubMed]
- Mori, H.; Koshida, K.; Ishigamori, O.; Matsubara, K. Investigation of qualitative and quantitative factors related to radiological exposure to nursing staff during computed tomography examinations. Health Phys. 2014, 107, S202–S210. [Google Scholar] [CrossRef] [PubMed]
- Heilmaier, C.; Mayor, A.; Zuber, N.; Fodor, P.; Weishaupt, D. Improving radiation awareness and feeling of personal security of non-radiological medical staff by implementing a traffic light system in computed tomography. Rofo 2016, 188, 280–287. [Google Scholar] [CrossRef] [PubMed]
- Miyajima, R.; Fujibuchi, T.; Miyachi, Y.; Tateishi, S.; Uno, Y.; Amakawa, K.; Ohura, H.; Orita, S. Effective techniques to reduce radiation exposure to medical staff during assist of X-ray computed tomography examination. Nihon Hoshasen Gijutsu Gakkai Zasshi 2018, 74, 326–334. (In Japanese) [Google Scholar] [CrossRef] [PubMed]
- Radiation Council. Secretariat of Nuclear Regulation Authority of Japan. 2017. Available online: https://www.nsr.go.jp/data/000209654.pdf (accessed on 19 March 2021).
- Ono, K.; Yoshitake, T.; Hasegawa, T.; Ban, N.; Kai, M. Estimation of the number of CT procedures based on a nationwide survey in Japan. Health Phys. 2011, 100, 491–496. [Google Scholar] [CrossRef] [PubMed]
- Rehani, M.M.; Hauptmann, M. Estimates of the number of patients with high cumulative doses through recurrent CT exams in 35 OECD countries. Phys. Med. 2020, 76, 173–176. [Google Scholar] [CrossRef] [PubMed]
- 2-3 Patient Assistance in X-ray Examination Room. Guideline for Radiation Safety of Medical Staff (Provisional Translation). 2020. Available online: https://www.jsrt.or.jp/data/wp-content/uploads/2020/10/suisyoutai_pdf2020.10.1.pdf (accessed on 19 March 2021).
- International Commission on Radiological Protection. Statement on Tissue Reactions. 2011; ICRP Ref 4825-3093-1464. [Google Scholar]
- International Commission on Radiological Protection. Publication 118: ICRP Statement on Tissue Reactions/Early and Late Effects of Radiation in Normal Tissues and Organs-Threshold Doses for Tissue Reactions in a RADIATION Protection Context; Annual of ICRP; Elsevier Ltd: Amsterdam, 2012. [Google Scholar]
- Kobayashi, M.; Koshida, K.; Suzuki, S.; Katada, K. Evaluation of patient dose and operator dose in swallowing CT studies performed with a 320-detector-row multislice CT scanner. Radiol. Phys. Technol. 2012, 5, 148–155. [Google Scholar] [CrossRef] [PubMed][Green Version]
- Haga, Y.; Chida, K.; Kaga, Y.; Sota, M.; Meguro, T.; Zuguchi, M. Occupational eye dose in interventional cardiology procedures. Sci. Rep. 2017, 7, 569. [Google Scholar] [CrossRef] [PubMed]
- Kato, M.; Chida, K.; Ishida, T.; Toyoshima, H.; Yoshida, Y.; Yoshioka, S.; Moroi, J.; Kinoshita, T. Occupational radiation exposure of the eye in neurovascular interventional physician. Radiat. Prot. Dosim. 2019, 185, 151–156. [Google Scholar] [CrossRef] [PubMed]
- Yokoyama, S.; Suzuki, S.; Toyama, H.; Arakawa, S.; Inoue, S.; Kinomura, Y.; Kobayashi, I. Evaluation of eye lens doses of interventional cardiologists. Radiat. Prot. Dosim. 2017, 173, 218–222. [Google Scholar] [CrossRef] [PubMed]
- Osanai, M.; Saito, Y.; Oyu, K.; Ishida, J.; Sato, M.; Sasaki, T. Image quality and radiation dose with low tube voltage in coronary CT angiography: An experimental study with normal type and soft plaque phantom. Hirosaki Med. J. 2013, 64, 15–28. [Google Scholar]
- Ishii, H.; Chida, K.; Satsurai, K.; Haga, Y.; Kaga, Y.; Abe, M.; Inaba, Y.; Zuguchi, M. A phantom study to determine the optimal placement of eye dosemeters on interventional cardiology staff. Radiat. Prot. Dosim. 2019, 185, 409–413. [Google Scholar] [CrossRef] [PubMed]
- Osanai, M.; Kudo, K.; Hosoda, M.; Tazoe, H.; Akata, N.; Kitajima, M.; Tsushima, M.; Komiya, N.; Kudo, M.; Tsujiguchi, T.; et al. The impact on the eye lens of radiation emitted by natural radionuclides (lead-210) present in radiation protection glasses. Radiat. Prot. Dosim. 2020, 188, 13–21. [Google Scholar] [CrossRef] [PubMed]
- Maki, D.; Ube, M.; Nagashima, Y.; Shinozaki, W.; Ueno, S.; Koguchi, Y.; Takeuchi, N. Development of the new glass badge. Radiat. Prot. Dosim. 2016, 171, 337–345. [Google Scholar] [CrossRef] [PubMed]
- Japan Accreditation Board. Available online: https://www.jab.or.jp/system/service/upload/RTL04590/RTL04590-en.pdf (accessed on 30 April 2021).
- Chiyoda Technol Corporation. Available online: https://www.c-technol.co.jp/eng/e-reason (accessed on 9 April 2021).
- Ishii, H.; Haga, Y.; Sota, M.; Inaba, Y.; Chida, K. Performance of the DOSIRIS™ eye lens dosimeter. J. Radiol. Prot. 2019, 39, N19–N26. [Google Scholar] [CrossRef] [PubMed]
- Japan Network for Research and Information on Medical Exposure. National Diagnostic Reference Levels in Japan (2020)—Japan DRLs 2020. 2020. Available online: http://www.radher.jp/J-RIME/report/DRL2020_Engver.pdf (accessed on 19 March 2021).
- Ministry of Health, Labour and Welfare. Notice No 254. 2001. Available online: https://www.mhlw.go.jp/content/11300000/000689300.pdf (accessed on 19 March 2021).
- Funao, H.; Ishii, K.; Momoshima, S.; Iwanami, A.; Hosogane, N.; Watanabe, K.; Nakamura, M.; Toyama, Y.; Matsumoto, M. Surgeons’ exposure to radiation in single-and multi-level minimally invasive transforaminal lumbar interbody fusion; a prospective study. PLoS ONE 2014, 9, e95233. [Google Scholar] [CrossRef] [PubMed]
- Komemushi, A.; Suzuki, S.; Sano, A.; Kanno, S.; Kariya, S.; Nakatani, M.; Yoshida, R.; Kono, Y.; Ikeda, K.; Utsunomiya, K.; et al. Radiation dose of nurses during IR procedures: A controlled trial evaluating operator alerts before nursing tasks. J. Vasc. Interv. Radiol. 2014, 25, 1195–1199. [Google Scholar] [CrossRef] [PubMed]
- Inoue, T.; Komemushi, A.; Murota, T.; Yoshida, T.; Taguchi, M.; Kinoshita, H.; Matsuda, T. Effect of protective lead curtains on scattered radiation exposure to the operator during ureteroscopy for stone disease: A controlled trial. Urology 2017, 109, 60–66. [Google Scholar] [CrossRef] [PubMed]
- International Commission on Radiological Protection. ICRP Publication 87: Managing Patient Dose in Computed Tomography; Annual of ICRP; Pergamon Press: Oxford, UK, 2000. [Google Scholar]
- International Commission on Radiological Protection. ICRP Publication 51: Data for Use in Protection against External Radiation; Annual of ICRP; Pergamon Press: Oxford, UK, 1987. [Google Scholar]
- Vlachos, I.; Tsantilas, X.; Kalyvas, N.; Delis, H.; Kandarakis, I.; Panayiotakis, G. Measuring scatter radiation in diagnostic X rays for radiation protection purposes. Radiat. Prot. Dosim. 2015, 165, 382–385. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
| Head | Chest | Upper Abdomen | |
|---|---|---|---|
| Tube voltage (kV) | 120 | 120 | 120 |
| Noise index | 2.8 | 9.0 | 9.9 |
| Set max. tube current (mA) | 300 | 440 | 440 |
| Scan mode | Axial | Helical | Helical |
| Rotation time (sec/rot) | 2.0 | 0.6 | 0.6 |
| Beam pitch | - | 0.875 | 1.35 |
| Beam collimation (mm) | 8 × 1.25 | 8 × 2.5 | 8 × 2.5 |
| CTDIvol (mGy) 1 | 83.03 | 6.15 | 10.63 |
| DLP (mGy cm) 2 | 1245.48 | 220.56 | 270.52 |
| Body Site of Scan | Effective Dose of Medical Staff (mSv/exam) |
|---|---|
| Head | 0.087 |
| Chest | 0.026 |
| Upper abdomen | 0.015 |
| Body Site of Scan | Hp(3) (mSv/DLP) 1 |
|---|---|
| Head | 3.6 × 10−4 |
| Chest | 7.4 ×10−4 |
| Upper abdomen | 7.3 × 10−4 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Osanai, M.; Sato, H.; Sato, K.; Kudo, K.; Hosoda, M.; Hosokawa, S.; Kitajima, M.; Tsushima, M.; Fujita, A.; Hosokawa, Y.; et al. Occupational Radiation Dose, Especially for Eye Lens: Hp(3), in Medical Staff Members Involved in Computed Tomography Examinations. Appl. Sci. 2021, 11, 4448. https://doi.org/10.3390/app11104448
Osanai M, Sato H, Sato K, Kudo K, Hosoda M, Hosokawa S, Kitajima M, Tsushima M, Fujita A, Hosokawa Y, et al. Occupational Radiation Dose, Especially for Eye Lens: Hp(3), in Medical Staff Members Involved in Computed Tomography Examinations. Applied Sciences. 2021; 11(10):4448. https://doi.org/10.3390/app11104448
Chicago/Turabian StyleOsanai, Minoru, Hidenori Sato, Kana Sato, Kohsei Kudo, Masahiro Hosoda, Shota Hosokawa, Maiko Kitajima, Megumi Tsushima, Akira Fujita, Yoichiro Hosokawa, and et al. 2021. "Occupational Radiation Dose, Especially for Eye Lens: Hp(3), in Medical Staff Members Involved in Computed Tomography Examinations" Applied Sciences 11, no. 10: 4448. https://doi.org/10.3390/app11104448
APA StyleOsanai, M., Sato, H., Sato, K., Kudo, K., Hosoda, M., Hosokawa, S., Kitajima, M., Tsushima, M., Fujita, A., Hosokawa, Y., & Saito, Y. (2021). Occupational Radiation Dose, Especially for Eye Lens: Hp(3), in Medical Staff Members Involved in Computed Tomography Examinations. Applied Sciences, 11(10), 4448. https://doi.org/10.3390/app11104448