1. Introduction
Sepsis is usually defined as a clinical syndrome characterised by systemic signs of infection and the concomitant positivity of blood culture to the presence of pathogenic microorganisms. Sepsis is divided into two main categories: (i) early-onset sepsis (EONS) and (ii) late-onset sepsis (LONS), according to the period of onset, which can be within the first 72 h of life or after, respectively [
1]. This pathology particularly affects infants in neonatal intensive care units (NICU), especially if they are preterm and low birth weight, with an incidence in the literature ranging between 1 and 40%, varying according to the onset period. A recent review reported an incidence rate of EONS in very low birth weight (VLBW) neonates of about 1.5–2% and an incidence rate equal to 2.1% in extremely low birth weight (ELBW) neonates [
2].
To date, there is still no globally recognised consensus about the correct definition of neonatal sepsis. The presence of a positive blood culture represents the gold standard for its diagnosis, but negative blood cultures in neonatal care do not exclude sepsis, especially when other clinical and/or laboratory signs that support the suspicion of sepsis are present [
3,
4,
5]. Therefore in newborns, especially in premature ones, the diagnosis of sepsis is not entrusted to the outcome of blood culture. The main problem in dealing with clinically evident sepsis is to suspect the diagnosis as early as possible.
For the reason reported above, in this work, we will use the term sepsis to refer to a clinically manifest infection with systemic inflammatory response syndrome (SIRS) even when the result of the culture for pathogens is not yet available.
This study focuses on LONS, which is the first cause of death of VLBW neonates who survive the first week of life. This pathology can be subtle or explosive and entails mortality ranging from 10 to 30% depending on the patient’s vulnerability and the virulence of the germ [
6].
From a clinical point of view, the strategy to combat sepsis includes three main steps, namely prevention, early diagnosis and treatment. Prevention and early diagnosis are clearly preparatory for the treatment and condition its timeliness. Prevention is the most effective measure against sepsis, especially the scrupulous hand hygiene of the clinical operators [
7]. Early diagnosis of sepsis would allow timely antibiotic therapy, which is essential to reduce the severity and duration of the disease, as well as lead to more favourable outcomes. In the literature, the effectiveness of the early administration of antibiotics is clearly described; even just an hour can reduce the mortality rate of sepsis [
7,
8]. Early diagnosis is based on a screening test that is performed with biomarkers, such as reactive C-protein and procalcitonin, which do not have strong specificity and often reveal positivity late, concurrently or even after the clinical onset. Conversely, the search of pathogens’ DNA is a costly and not always available method. Finally, blood culture can produce false-negatives and does not have rapid response times. All these methods, therefore, do not satisfy the need to be able to diagnose sepsis early [
9]. Hence, more appropriate tests are needed, which should be highly sensitive, predictive, fast to perform and safe for this fragile category of babies.
In the scenario just described, the development of the HeRO (Heart Rate Observation) monitor was prompted by the observation that physiological perturbations in the early phase of sepsis are reflected by subtle, complex changes in heart rate characteristics. Decreased heart rate variability and transient repetitive heart rate decelerations occur in neonatal sepsis, often before a patient shows obvious clinical signs. The HeRO monitor shows a number, or score, which represents the risk that a patient will experience a clinical deterioration consistent with clinical or blood culture-proven sepsis in the next 24 h. However, it is worth reporting that there are a number of pathophysiological situations other than sepsis that can lead to a depression of heart rate variability without the presence of a sepsis episode [
10] and that therefore can cause an increase in the HeRO score. Thus, for an accurate early diagnosis of sepsis, the HeRO score must be analysed also considering a larger set of parameters and clinical manifestations.
Based on the previous premises, the purpose of this work is to give the clinician a high individualised decision support on each individual patient through an intelligent system capable of acquiring a series of detailed information and perform an accurate early diagnosis of sepsis, thus minimising errors of false positivity/negativity of the HeRO score and the use of unnecessary and/or protracted antibiotic therapy. Therefore, the research problem consists of responding to the need to develop a diagnostic system that allows considering both the HeRO score and several parameters and clinical manifestations with which the neonatologist is absolutely familiar.
The present study was conducted in collaboration with the clinicians of the Di Venere Hospital’s NICU from Bari (Italy) and aimed at:
investigating and confirming the diagnostic predictive ability of sepsis of the HeRO score computed by the innovative HeRO duet device (
https://www.heroscore.com/) according to the literature results [
11,
12];
developing an intelligent decision support system that, based on the newborn’s current clinical situation, including the HeRO score as well, can support the clinician in deciding the administration of early antibiotic treatment in the case of doubt regarding sepsis. This would allow for a refined early diagnosis that would enable a targeted antibiotic treatment, avoiding often superfluous, or prolonged, treatments, which could cause the phenomena of antibiotic resistance, as well as causing harm to or side-effects for such fragile babies [
13].
2. The HeRO Score and the Risk of Incorrect Sepsis Diagnosis
This section describes and discusses how the HeRO duet manages to detect the early signs of sepsis, with the aim to understand better the aspects related to the false positivity/negativity of the HeRO score. The HeRO device can analyse the infant’s heart rate variability without direct contact. It acquires the heart rate data from a multi-parameter monitor connected to the infant via electrodes.
In the literature, it is described how a reduced variability and transient decelerations of the heart rate (HR) can be present in the hours or days preceding the diagnosis of sepsis [
11]. In fact, sepsis involves the proliferation of pathogens that can depress the variability of the heart rate through both direct stimulation of the vagus nerve and the release of cytokines [
14,
15]. The mechanism underlying the direct vagus nerve stimulation by pathogens is not yet well known. A direct stimulation of neuronal receptors located either peripherally or at the ganglion level is hypothesised [
14]. In addition, the mechanism by which cytokines (in particular interleukin 6) induce a reduced variability of HR even in the hours preceding the onset of sepsis to date is not yet clear. Interleukin 6 is supposed to induce electrophysiological changes in the myocardiocytes, which lead to an electrical remodelling of the heart, which could predispose to corrected QT (QTc) interval prolongation and ventricular arrhythmia. Such a mechanism would imply a compromise of the potassium channels and an enhancement of the function of the calcium channels of the cardiomyocytes with consequent prolongation of the duration of the membrane action potential of the myocardiocytes [
16,
17].
The reduced heart rate variability induced early in the initial stages of sepsis, often when the inflammation indexes are negative and the symptoms fade, is recorded by HeRO, which, by analysing the changes in the HR, is able to predict in advance (in the previous 24 h or even earlier) the onset of the infection episode [
18]. However, there are some pathophysiological conditions beyond sepsis that can involve the release of cytokines or the stimulation of the vagus nerve and that can affect the HeRO score outcome [
15]. The knowledge of these conditions can help clinicians to orient themselves by attributing a correct meaning to the HeRO score. However, the decision whether to treat the neonate with antibiotic therapy gets more difficult if considering only the HeRO score. In fact, all newborns with a positive score would be treated with antibiotic therapy with all the risks that this entails in such small infants. As an example, the results of a study conducted on 3003 VLBW neonates were reported in Mooman et al. [
19]. The authors of this study considered two groups of neonates: one group was treated with the knowledge of the HeRO score and the second one without access to the HeRO monitor. The results showed that in the first group of infants, there was a 22% drop in mortality, which rose to 26% if we consider only ELBW. However, in the first group of newborns, an increase in deafness was observed, which could perhaps be correlated with the greater number of days of antibiotic therapy [
20].
3. Materials And Methods
3.1. Patients
This retrospective study was conducted from February 2019 to September 2020 and involved 21 premature VLBW neonates, almost equally distributed between males and females, gestational age between 23 and 32 weeks and weight between 480 and 1500 g (
Table 1 reports the precise details about the neonates’ characteristics). All babies were at high risk of contracting sepsis because of the hospitalisation in the NICU, prematurity and low birth weight. The study was conducted in accordance with the Declaration of Helsinki.
The presented work is a retrospective observational study, and the processed data came exclusively from the collection from the medical records of patients whose parents at the time of admission had authorized their use. According to the policy of the Di Venere Hospital, consent from the ethics committee is not required in the case of retrospective observational studies. In these cases, the investigators simply notify the the ethics committee about the study, without waiting for its approval.
3.2. Data Collection
Clinical data used in this study were obtained from each patient’s electronic medical records and included the following parameters:
birth weight;
gestational age;
general aspect of the patient;
presence of sepsis symptoms: body temperature (fever, hypothermia), cardiovascular instability (bradycardia or tachycardia, rhythm irregularity, urine amount < 1 //, hypotension, impaired peripheral perfusion), skin and subcutaneous lesions (petechiae, sclerema), respiratory instability (apnea or tachypnea, increased oxygen demand, increased need for ventilation support), gastrointestinal (food intolerance, abdominal distension), non-specific (irritability lethargy, hypotonia);
positive culture for pathogens until 7 days before the suspicion of sepsis: LONS pathogens, i.e., coagulase, negative staphylococci, Staphylococcus aureus, group B Streptococcus, Enterococcus spp., Escherichia coli, Klebsiella spp, Serratia spp., Enterobacter spp., Pseudomonas spp., Acinetobacter baumannii, Candida spp.;
value of C-reactive protein (CRP);
value of procalcitonin (PCT);
metabolic acidosis (blood gas pH);
days with central venous catheter (CVC);
patient intubation;
HeRO score acquired every hour.
The authors found it interesting to include data related to the presence in NICU of patients with positive cultures for aggressive pathogens, notoriously responsible for late onset sepsis, both at the time of the suspicious episode and up to 7 days before. This is for the purpose of considering as a risk factor the microbiological data of the patient and more generally the pathogenic flora present in the NICU.
One or more clinical cases have been extracted from patient data according to the manifestations of at least one of the following events that raised the suspicion of sepsis:
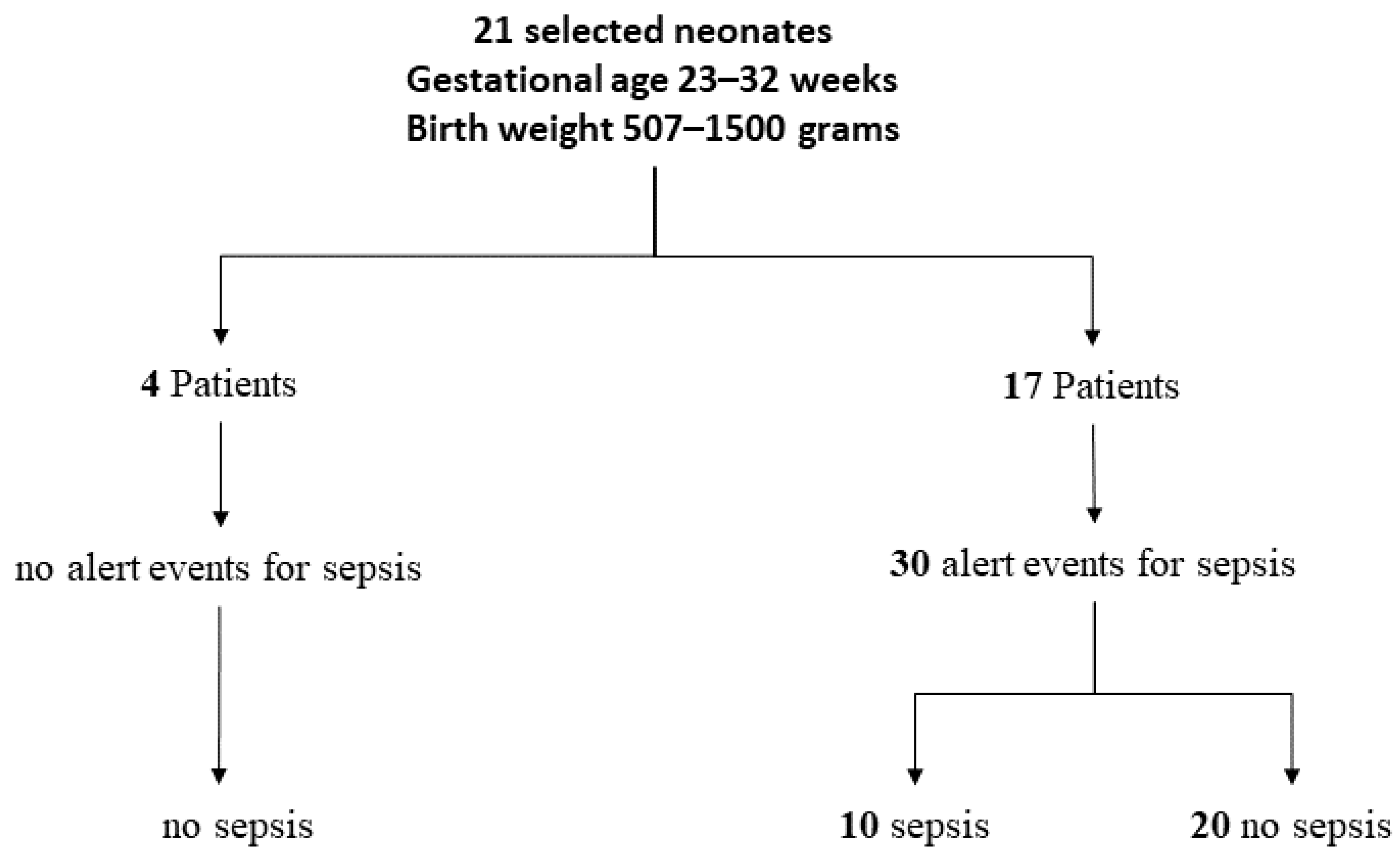
In particular, if the event was the positivity of the HeRO score, all analysed parameter values were referred to the next 24 h, whereas if the event was the presence of symptoms and/or the positivity of the inflammation indexes, all analysed parameters values were referred to the previous 24 h. In 17 patients out of 21, alerts were observed that raised the suspicion of sepsis for a total of 30 alerts (or clinical cases). In 10 clinical cases out of 30, sepsis diagnosis was then confirmed. The studied cohort also included four patients that neither presented any signs of sepsis, nor were affected by sepsis.
Figure 1 reports the distribution of the studied clinical cases.
The HeRO Duet Device
The HeRO duet is a medical device that supports medical personnel in diagnosis with high predictivity if it is used together with anamnestic and laboratory clinical findings. It allows intervening with antibiotic therapies also in correspondence with one of the first reported peaks, thus preventing short- and long-term complications associated with serious sepsis. In fact, as is well known in the literature, the first antibiotic administration, being always the most effective, would lead to a decisive intervention on the patient, if carried out in a timely manner [
19].
The HeRO duet was designed to non-invasively predict neonatal sepsis and works by getting data from a generic device used to monitor vital functions. The HeRO duet detects the data concerning the ECG waveforms from the physiological monitor, which are subsequently transmitted in the form of an analogue signal via a cable connected to the AD2-DAD data acquisition device. The Dräger C500 monitor(
www.draeger.com) was used in this study. HeRO duet can acquire and analyse the electrocardiogram signal in order to compute the heart rate variability based on the R-R interval duration. A complex model based on the observations of the heart rate variability is then used to generate the HeRO index, which represents a factor associated with the increased risk of sepsis [
11].
HeRO was developed as an alert system for sepsis in preterm infants in intensive care. Researchers from the University of Virginia, in fact, observing patients and noting abnormal heart rate characteristics (HRCs) before and at the clinical moment of the pathology, devised an algorithm that is based on the dependence of HRCs on variables such as the standard deviation of R-R intervals, sample asymmetry and sample entropy. Sample asymmetry refers to the relative rate of heart rate acceleration and deceleration. The entropy of the sample, instead, measures the irregularity of the sample, which can be interpreted as signalling for systemic inflammatory response syndrome (SIRS). Calculating the following information, therefore, through the final algorithm, which is based on the logistic regression adapted for repeated measures, the result is obtained, as well as the index of the increased factor for the risk of sepsis in the following 24 h [
20]. Precisely, based on this scientific evidence, the HeRO duet device is capable of generating a new score every hour taking into account the variation of the patient’s cardiac variability in the last 12 h. The HeRO index computation procedure is described within the HeRO duet manual. The risk of contracting sepsis is classified as:
low if the score is lower than 1;
intermediate if the score ranges between 1 and 2;
high if the score is higher than 2.
It is worth mentioning that patients featuring a high HeRO score are six times more likely to contract sepsis than patients with a low HeRO score value [
21]. For each monitored patient, the device’s display (an example view is shown in
Figure 2) shows both the current score and the trend of the previous scores computed in the last five days. One HeRO duet device can simultaneously monitor up to two patients. A list of the information that is shown on the screen follows:
bed identifier;
trend of the signal over time;
graph indicating the current score;
current score value;
alarm symbol that appears only in correspondence with a high score;
status indicator, which turns green in the case of the detection of the R-R intervals, grey in the opposite case.
3.3. ANN Classifier
The intelligent neonatal sepsis early diagnosis system (I.N.E.S.) proposed in this work allows the early detection of sepsis by using an appropriate artificial neural network, processing input data and deciding if the input pattern would lead to the sepsis condition or not. The following paragraphs describe the input data processed by the neural classifier, the ANN topology design strategy and the metrics for evaluating the classification performance.
3.4. ANN Design
In order to design the ANN topology, in this work, an evolutionary approach based on a single-objective genetic algorithm (GA) was employed for selecting the optimal combination in terms of the number of hidden layers, the number of neurons per layer and the activation function for each hidden layer, as in previous works of some of the authors, which was revealed to be a suitable approach for solving problems in several clinical domains [
23,
24,
25]. The MATLAB
® framework was employed for designing and implementing both the neural models and the optimisation algorithm.
The GA searched for the optimal ANN topology by maximizing the mean accuracy (Equation (
1)), measured on the test set, over 100 iterations of training, validation and testing of the ANN. To do this, each individual in the GA population, namely each candidate ANN topology, was trained, validated and tested 100 times considering random permutations of the input dataset, splitting it into 60–10–30% for training, validation and test sets, respectively. Each ANN could be constituted by at least one hidden layer, up to three, with at maximum 256 neurons per layer. The GA also evaluated several activation functions (each hidden layer shared the same transfer function for all the neurons of the layer), namely the hyperbolic tangent sigmoid transfer function (
tansig), the log-sigmoid transfer function (
logsig), the linear transfer function (
purelin) and the symmetric saturating linear transfer function (
satlins). The output layer was always characterised by a tansig transfer function, whereas the ANN training was performed with resilient propagation [
26]. Although in Bevilacqua et al., the 60-20-20 percentages were used for splitting the dataset [
23], in this work, due to a limited number of samples, ten percent only was employed for the validation set, since it was used for evaluating the early-stopping of the network training in order to avoid over-fitting.
Furthermore, since the input data were unbalanced between the positive and negative classes, the adaptive synthetic (ADASYN) approach was considered for generating synthetic data for the class with fewer samples [
22]. In this way, the final dataset was constituted by 46 samples (24 negative and 22 positive), described by 11 features.
4. Results
In this section, the results obtained in the detection of sepsis condition in the considered subjects are reported.
4.1. HeRO-Based Results, Clinical Manifestations, Indexes and Therapy
As the first step, the predictivity of the HeRO score was analysed considering that a patient would have contracted the disease after 24 h of a HeRO peak higher than one.
Figure 4 shows a summary scheme of the diagnostic results.
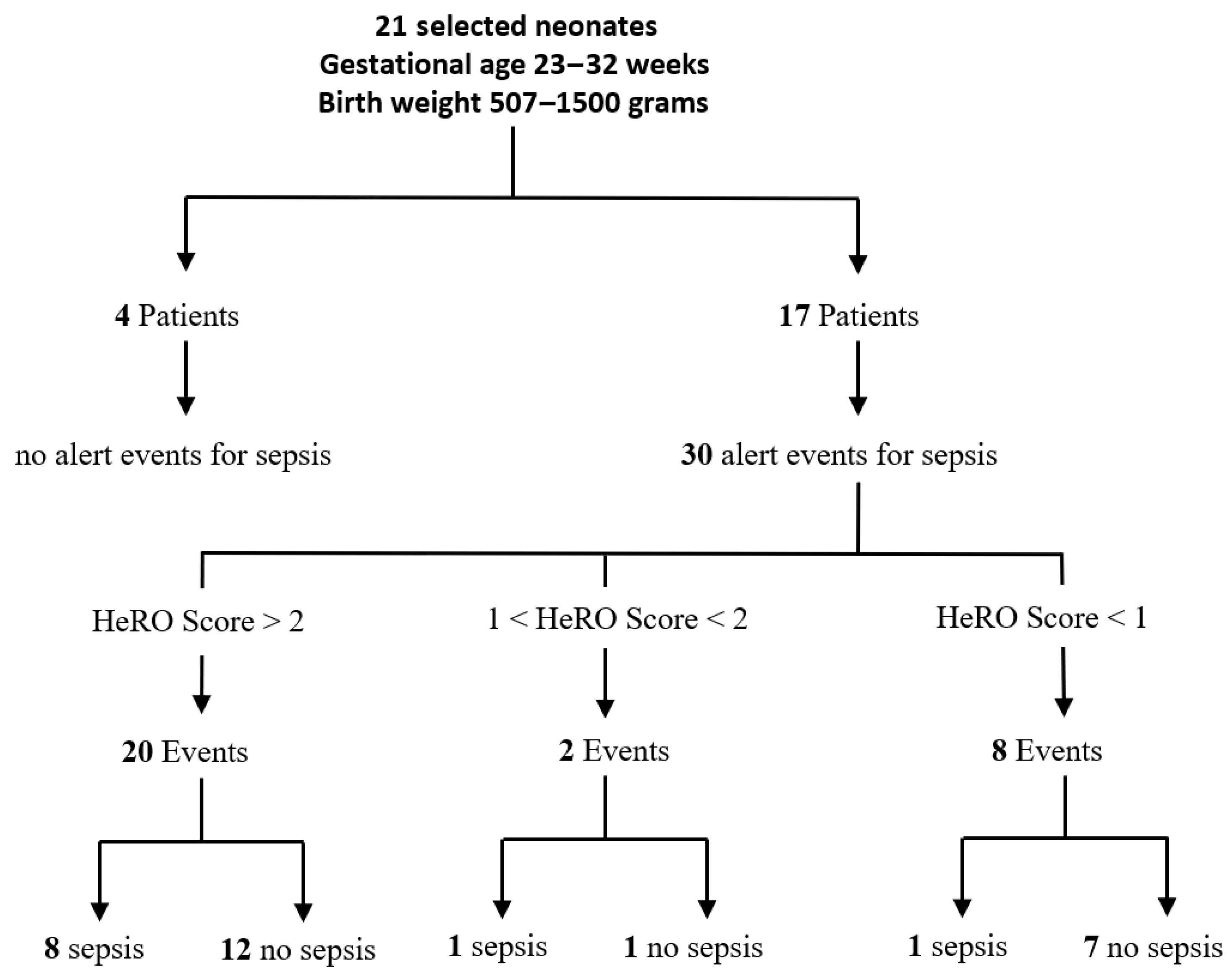
Considering the 30 suspicious clinical cases, the following results were observed according to the HeRO score:
Twenty clinical cases out of 30 were characterised by a positive HeRO score higher than two:
- -
In eight of these cases, the newborn developed sepsis, which the HeRO score was able to predict between 5 and 12 h in advance. In one case, the HeRO duet was connected to the patient’s monitor when there were full-blown symptoms; even though there was the need for intubation and the decay of the general conditions, the inflammation indexes were negative. Antibiotic therapy was initiated on the basis of both the positive HeRO score and the sepsis symptoms. A few hours later, the start of pneumonia was observed, and inflammation indexes became positive after about 24 h.
- -
In 12 clinical cases, the HeRO was positive (nine cases out of 12 had a clinical symptom or a slightly positive inflammation index), but they did not develop sepsis. Thus, no antibiotic therapy was started.
Two cases out of 30 were characterised by a HeRO score between one and two (specifically, 1.6). The baby developed signs of infection 5 h before the HeRO peak. In this specific case, the newborn was already on antibiotic therapy with a negative HeRO index and good conditions when he presented a slightly clinical and radiographic deterioration; an antibiotic change was necessary. In this case, the baby did not develop sepsis, but he had only moderate abdominal distension, then regressed without any therapy.
Eight cases out of 30 were characterised by a negative HeRO score, but slight positive signs of the infection indices (at least one) and/or one symptom-related to sepsis were detected in seven episodes. In one case, positive symptoms were observed. For all eight cases, no antibiotic therapy was initiated after continuous monitoring of the cases, which considered a series of blood samples. In one case, the HeRO score was negative, but the baby presented severe sepsis starting as pneumonia (in the case of localized infection, it described a possible negativity of the HeRO score; in fact, in the following days, the sepsis became generalized with the HeRO score, which became positive).
4.2. I.N.E.S. Results and Comparison with the HeRO-Based Diagnostic Outcomes
Considering the neural classifier, the optimised ANN allowed obtaining 94.1%, 80% and 100% for the accuracy, sensitivity and specificity, respectively. Conversely, these indices reached 58.8%, 80% and 50% for the HeRO score on the same set of clinical cases.
Considering
Table 4 and the confusion matrix reported in
Table 5, as well as computing the accuracy, sensitivity and specificity of the evaluated scores related to the clinical cases, it is clear that the I.N.E.S. score showed higher diagnostic performances with respect to the HeRO score. It has to be emphasised that the positivity/negativity of the I.N.E.S. score of the clinical cases reported in
Table 4 was obtained by a voting of the classifications performed by all 100 trained models, ensuring also that the considered entry for classification was not included in the training set of the model, as described in
Section 3.4. Lastly, in order to show the variability of the HeRO score respect to the sepsis diagnosis,
Figure 5 and
Figure 6 show two examples of the variation over time of the HeRO score for 4 different subjects. Specifically,
Figure 5 shows two cases correctly classified by both HeRO and I.N.E.S. scores;
Figure 6, instead, shows two false positives for the HeRO systems correctly classified by the I.N.E.S. score.
5. Discussion
The results of this study confirm what has already been highlighted in the literature about the prediction of the HeRO score with respect to the onset of sepsis. However, in all sepsis events announced early by the HeRO score, clinicians waited for at least one clinical and/or laboratory sign to appear before starting antibiotic therapy. In the literature, it is described how the early administration of antibiotics, even just an hour before, is useful in order to reduce mortality from sepsis [
5,
6].
In this study, concerning the positive clinical cases for sepsis, the positivity of the score alone, however correct and predicted, was not sufficient to activate the useful actions to intervene with the desired treatment. On the other hand, the finding of a negative HeRO score in patients with sepsis alerts about the presence of only one symptom and/or a slight positivity (CRP < 1 /; PCT < 1 /) of one of the two laboratory indices, after an attentive discussion of the single clinical case suggested to the clinicians to wait (it is worth noting that these events concerned newborns with birth weight and gestational age values at the upper limits), but with the activation of serious clinical and laboratory tests and accepting the risk of accentuating the physiological anaemia of prematurity.
In 12 out of 20 events overall, the HeRO score was positive, but the patient did not develop sepsis. In addition to the positive score, in 10 events, patients presented only one symptom and/or a mild positivity of one of the two laboratory indices, activating surveillance as in the previous cases. The company that produces HeRO and the most recent literature on the topic report a list of clinical situations and/or pharmacological therapies that might influence the increase in the HeRO score. In fact, the clinical situations involving an increased release of cytokines and/or a stimulus of the vagus nerve can cause an increase in the HeRO score. This explains why apneas, intraventricular and/or parenchymal haemorrhage, periventricular leukomalacia, a sudden deterioration of respiratory conditions, but also necrotising enterocolitis (NEC), some drugs administered in the post-surgical course (anaesthetics, anticholinergics) and anti-inflammatory drugs may affect the HeRO score.
It should also be borne in mind that sepsis often has an association with several of these pathologies: neonates with severe sepsis may have intra-ventricular haemorrhages (IVH) during sepsis, but also NEC, a sudden deterioration of respiratory conditions and other complications. All these conditions must be kept in mind and carefully evaluated when considering the HeRO score. One should also keep in mind what are the multiplicative risk factors of sepsis and that is a very low gestational age and birth weight (most are low factors), staying in the NICU (the longer the hospitalization, the greater the risk of sepsis) and the placement of central catheters (the more days from the positioning, the greater the risk of sepsis) [
6]. This suggests that all the team involved in caring for the neonate must be educated and trained on the functioning of the HeRO device and on all situations that can influence the HeRO score, thus highlighting a limitation of the HeRO score. In fact, it can be observed how, in case of doubt, the clinician activates a series of additional checks (clinical checks and a series of blood sampling) and how, in strongly suspicious cases, he, or she, tends to wait for other clinical or laboratory confirmation before changing or starting antibiotic therapy. It would therefore be necessary to have other instruments in relation to the score of HeRO. The manufacturer of the HeRO duet device proposes a composite score that takes into account the indices of infection and the clinic. However, such a set score is very generic and, in the authors’ opinion, is not very individualized as it does not take into account a series of factors (birth weight, gestational age, stay in NICU, etc.) that could be helpful in the evaluation, for example, of a false-positive score.
6. Conclusions
In this study, the authors demonstrated on a small cohort of patients how an intelligent neural network that processes the HeRO score along with a series of parameters strictly connected to the risk of sepsis can support the clinic in its decisions. The network developed thanks to the close collaboration between neonatologists and engineers gave very satisfactory results regarding the ability to screen patients for sepsis. I.N.E.S. gave even more accurate results in those cases (12/20) in which the HeRO score was frankly positive (index > 2), but the patient had no sepsis. It is worth underlining how having recognized the positive patients with a specificity of 100% for sepsis could have given clinicians a useful confirmation to activate the start of antibiotic therapy early. On the other hand, having recognized all negative cases for sepsis could give the clinician the peace of mind not to treat those cases that present a positive HeRO without any confirmation of clinical and/or laboratory sepsis. Regarding other events with the HeRO score completely negative, or rather less than one (one overall), only one patient had sepsis: in line with the manufacturer’s description, the HeRO score may not be reliable in the case of localized infection; this case resulted in being negative also for I.N.E.S. In two events, the HeRO score was between one and two: one case had mild symptoms, and only one index score resulted in sepsis; both cases were negative for I.N.E.S. Future studies will investigate the performance of the proposed neural network on a larger population of patients at risk in order to confirm its effectiveness and make any corrective measures, especially regarding the choice of input parameters.
Author Contributions
Conceptualization, V.B., A.D.V. and F.P.; methodology, A.B. and D.B.; software, F.T., A.B. and D.B.; validation, V.B. and F.P.; formal analysis, A.B. and D.B.; investigation, F.T., D.B. and F.P.; data curation, F.T. and F.P.; writing—original draft preparation, A.B., D.B. and F.P.; writing—review and editing, all authors; supervision, V.B. and F.P.; All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Informed Consent Statement
Informed consent was obtained from all subjects involved in the study.
Data Availability Statement
The data presented in this study are available on request from the corresponding author.
Conflicts of Interest
The authors declare no conflict of interest.
References
- Camacho-Gonzalez, A.; Spearman, P.W.; Stoll, B.J. Neonatal infectious diseases: Evaluation of neonatal sepsis. Pediatric Clin. N. Am. 2013, 60, 367. [Google Scholar] [CrossRef]
- Siegel, J.D. Neonatal sepsis. Pediatric Infect. Dis. J. 1982, 1, S39. [Google Scholar] [CrossRef]
- Wynn, J.L. Defining neonatal sepsis. Curr. Opin. Pediatric 2016, 28, 135. [Google Scholar] [CrossRef] [PubMed]
- Wynn, J.L.; Wong, H.R.; Shanley, T.P.; Bizzarro, M.J.; Saiman, L.; Polin, R.A. Time for a neonatal–specific consensus definition for sepsis. Pediatric Crit. Care Med. A J. Soc. Crit. Care Med. World Fed. Pediatric Intensive Crit. Care Soc. 2014, 15, 523. [Google Scholar] [CrossRef]
- Goldstein, B.; Giroir, B.; Randolph, A. International pediatric sepsis consensus conference: Definitions for sepsis and organ dysfunction in pediatrics. Pediatric Crit. Care Med. 2005, 6, 2–8. [Google Scholar] [CrossRef] [PubMed]
- Stoll, B.J.; Hansen, N. Infections in VLBW infants: Studies from the NICHD Neonatal Research Network. In Seminars in Perinatology; Elsevier: Amsterdam, The Netherlands, 2003; Volume 27, pp. 293–301. [Google Scholar]
- Kuti, B.P.; Ogunlesi, T.A.; Oduwole, O.; Oringanje, C.; Udoh, E.E.; Meremikwu, M.M. Hand hygiene for the prevention of infections in neonates. Cochrane Database Syst. Rev. 2019, 2019, CD013326. [Google Scholar] [CrossRef]
- Kumar, A.; Roberts, D.; Wood, K.E.; Light, B.; Parrillo, J.E.; Sharma, S.; Suppes, R.; Feinstein, D.; Zanotti, S.; Taiberg, L.; et al. Duration of hypotension before initiation of effective antimicrobial therapy is the critical determinant of survival in human septic shock. Crit. Care Med. 2006, 34, 1589–1596. [Google Scholar] [CrossRef]
- Clec’h, C.; Timsit, J.F.; De Lassence, A.; Azoulay, E.; Alberti, C.; Garrouste-Orgeas, M.; Mourvilier, B.; Troche, G.; Tafflet, M.; Tuil, O.; et al. Efficacy of adequate early antibiotic therapy in ventilator-associated pneumonia: Influence of disease severity. Intensive Care Med. 2004, 30, 1327–1333. [Google Scholar] [CrossRef]
- Russell, A.B.; Kumar, R. Early onset neonatal sepsis: Diagnostic dilemmas and practical management. Arch. Dis. Child.-Fetal Neonatal Ed. 2015, 100, F350–F354. [Google Scholar] [CrossRef]
- Fairchild, K.D.; Lake, D.E. Cross-correlation of heart rate and oxygen saturation in very low birthweight infants: Association with apnea and adverse events. Am. J. Perinatol. 2018, 35, 463. [Google Scholar]
- Schelonka, R.L.; Carlo, W.A.; Bauer, C.R.; Peralta-Carcelen, M.; Phillips, V.; Helderman, J.; Navarrete, C.T.; Moorman, J.R.; Lake, D.E.; Kattwinkel, J.; et al. Mortality and Neurodevelopmental Outcomes in the Heart Rate Characteristics Monitoring Randomized Controlled Trial. J. Pediatrics 2020, 219, 48–53. [Google Scholar] [CrossRef] [PubMed]
- Isaacs, D. Unnatural selection: Reducing antibiotic resistance in neonatal units. Arch. Dis. Child.-Fetal Neonatal Ed. 2006, 91, F72–F74. [Google Scholar] [CrossRef] [PubMed]
- Fairchild, K.D.; Srinivasan, V.; Randall Moorman, J.; Gaykema, R.P.; Goehler, L.E. Pathogen-induced heart rate changes associated with cholinergic nervous system activation. Am. J. Physiol.-Regul. Integr. Comp. Physiol. 2011, 300, R330–R339. [Google Scholar] [CrossRef] [PubMed]
- Sullivan, B.A.; Grice, S.M.; Lake, D.E.; Moorman, J.R.; Fairchild, K.D. Infection and other clinical correlates of abnormal heart rate characteristics in preterm infants. J. Pediatric 2014, 164, 775–780. [Google Scholar] [CrossRef]
- Kobayashi, H.; Kobayashi, Y.; Yokoe, I.; Kitamura, N.; Nishiwaki, A.; Takei, M.; Giles, J.T. Heart rate–Corrected QT interval duration in rheumatoid arthritis and its reduction with treatment with the interleukin 6 inhibitor tocilizumab. J. Rheumatol. 2018, 45, 1620–1627. [Google Scholar] [CrossRef]
- Lazzerini, P.E.; Capecchi, P.L.; Laghi-Pasini, F. Systemic inflammation and arrhythmic risk: Lessons from rheumatoid arthritis. Eur. Heart J. 2017, 38, 1717–1727. [Google Scholar] [CrossRef]
- Fairchild, K.D.; O’Shea, T.M. Heart rate characteristics: Physiomarkers for detection of late-onset neonatal sepsis. Clin. Perinatol. 2010, 37, 581–598. [Google Scholar] [CrossRef]
- Moorman, J.R.; Carlo, W.A.; Kattwinkel, J.; Schelonka, R.L.; Porcelli, P.J.; Navarrete, C.T.; Bancalari, E.; Aschner, J.L.; Walker, M.W.; Perez, J.A.; et al. Mortality reduction by heart rate characteristic monitoring in very low birth weight neonates: A randomized trial. J. Pediatric 2011, 159, 900–906. [Google Scholar] [CrossRef]
- King, W.E. A Case Study in Evaluating the Clinical Utility of Early Warning Systems: HeRO. Neonatal Intensive Care 2020, 33, 15. [Google Scholar]
- Griffin, M.P.; Lake, D.E.; Bissonette, E.A.; Harrell, F.E.; O’Shea, T.M.; Moorman, J.R. Heart rate characteristics: Novel physiomarkers to predict neonatal infection and death. Pediatrics 2005, 116, 1070–1074. [Google Scholar] [CrossRef]
- He, H.; Bai, Y.; Garcia, E.A.; Li, S. ADASYN: Adaptive synthetic sampling approach for imbalanced learning. In Proceedings of the 2008 IEEE International Joint Conference on Neural Networks (IEEE World Congress on Computational Intelligence), Hong Kong, China, 1–8 June 2008; pp. 1322–1328. [Google Scholar]
- Bevilacqua, V.; Brunetti, A.; Triggiani, M.; Magaletti, D.; Telegrafo, M.; Moschetta, M. An optimized feed-forward artificial neural network topology to support radiologists in breast lesions classification. In Proceedings of the 2016 on Genetic and Evolutionary Computation Conference Companion, Denver, CO, USA, 20–24 July 2016; pp. 1385–1392. [Google Scholar]
- Trotta, G.F.; Pellicciari, R.; Boccaccio, A.; Brunetti, A.; Cascarano, G.D.; Manghisi, V.M.; Fiorentino, M.; Uva, A.E.; Defazio, G.; Bevilacqua, V. A neural network-based software to recognise blepharospasm symptoms and to measure eye closure time. Comput. Biol. Med. 2019, 112, 103376. [Google Scholar] [CrossRef] [PubMed]
- Bevilacqua, V.; Brunetti, A.; Trotta, G.F.; Dimauro, G.; Elez, K.; Alberotanza, V.; Scardapane, A. A novel approach for hepatocellular carcinoma detection and classification based on triphasic CT protocol. In Proceedings of the 2017 IEEE Congress on Evolutionary Computation (CEC), San Sebastian, Spain, 5–8 June 2017; pp. 1856–1863. [Google Scholar]
- Riedmiller, M.; Braun, H. A direct adaptive method for faster backpropagation learning: The RPROP algorithm. In Proceedings of the IEEE International Conference on Neural Networks, San Francisco, CA, USA, 28 March–1 April 1993; pp. 586–591. [Google Scholar]
| Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).


 ,
, 









{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}