The Effect of Insertion Angles and Depths of Dental Implant on the Initial Stability


Abstract
1. Introduction
2. Materials and Methods
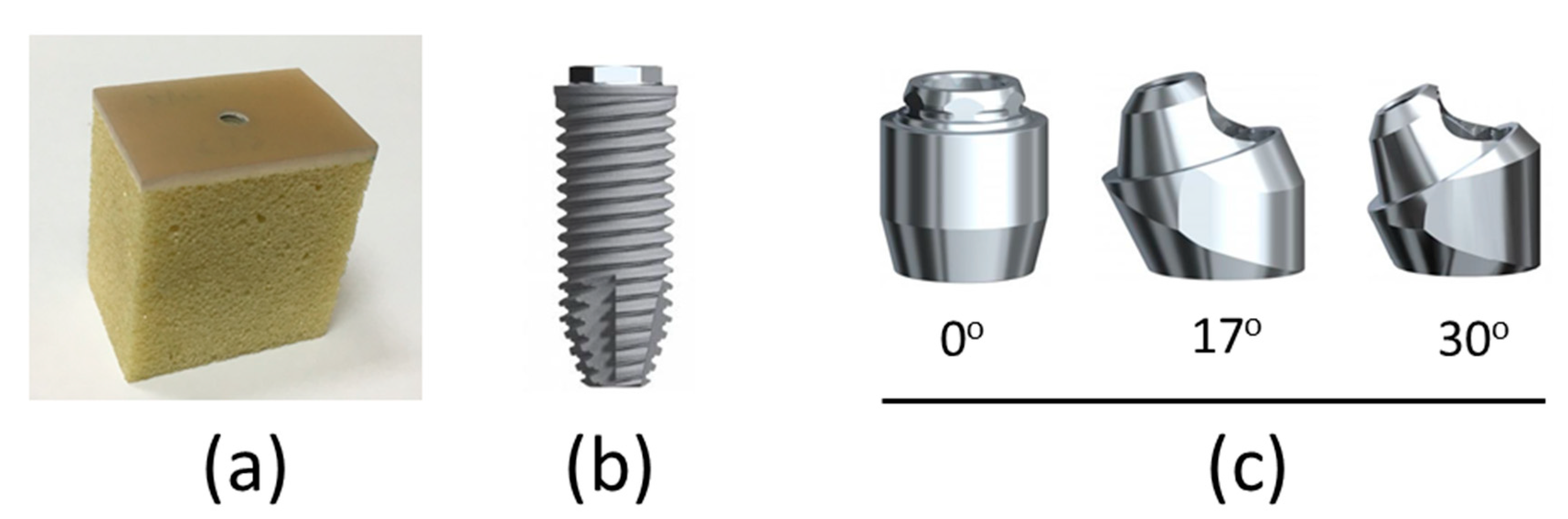
2.1. Preparation of the Artificial Foam Bone Specimen and Dental Implant Components
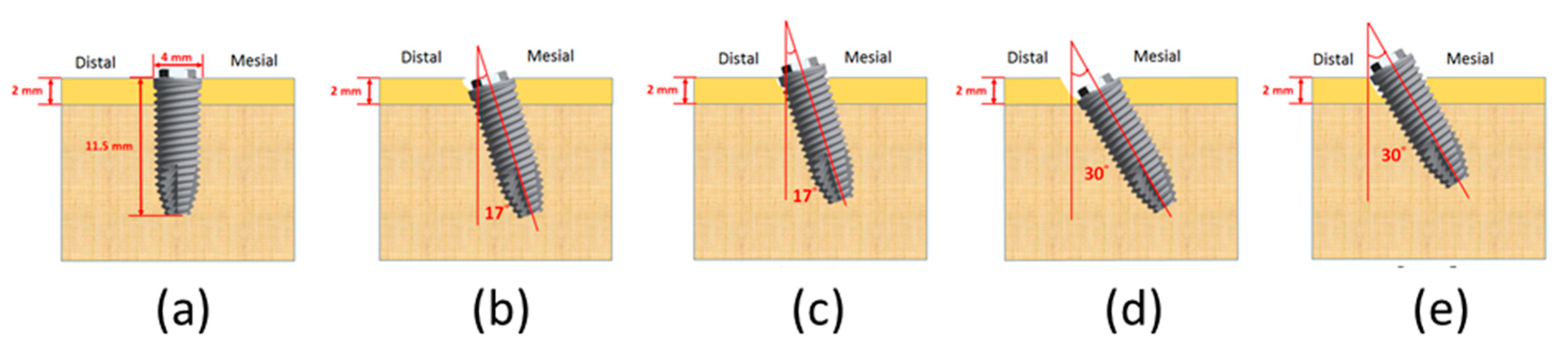
2.2. Insertion of the Dental Implant at Various Angulations and Depths
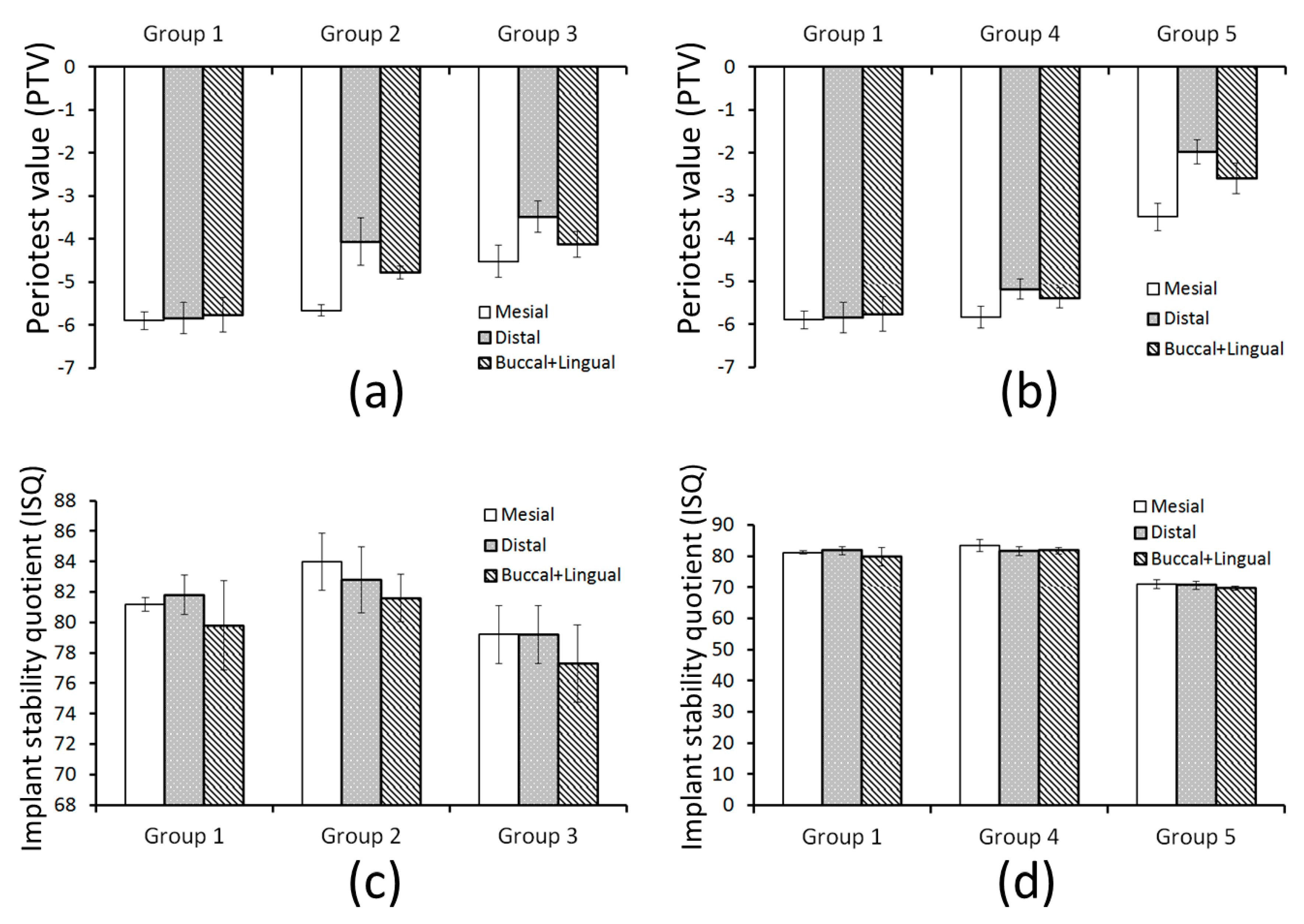
- Group 1:
- Vertical implant in an evencrestal position.
- Group 2:
- 17° tilted implant in a distal subcrestal position.
- Group 3:
- 17° tilted implant in a mesial supracrestal position.
- Group 4:
- 30° tilted implant in a distal subcrestal position.
- Group 5:
- 30° tilted implant in a mesial supracrestal position.
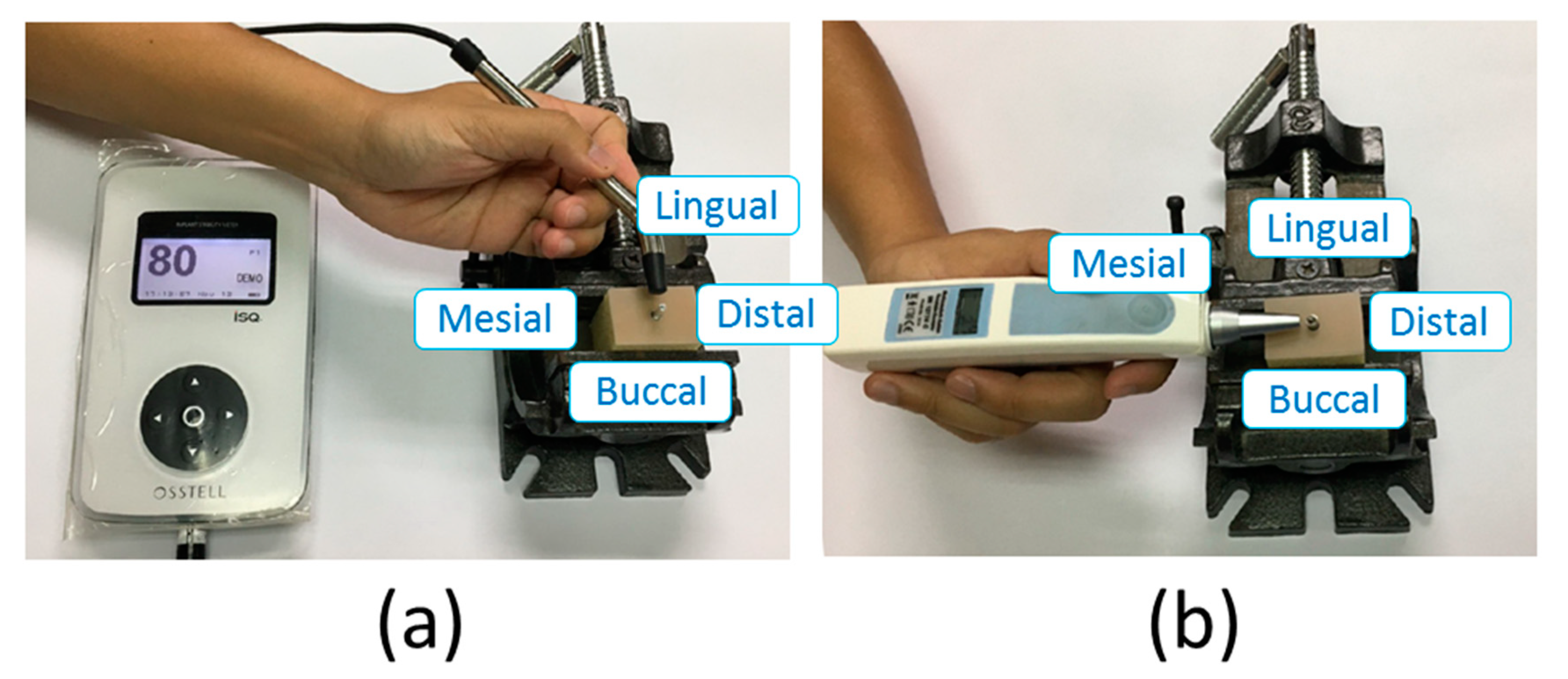
2.3. Measuring the PTV and ISQ
2.4. Statistical Analysis
3. Results
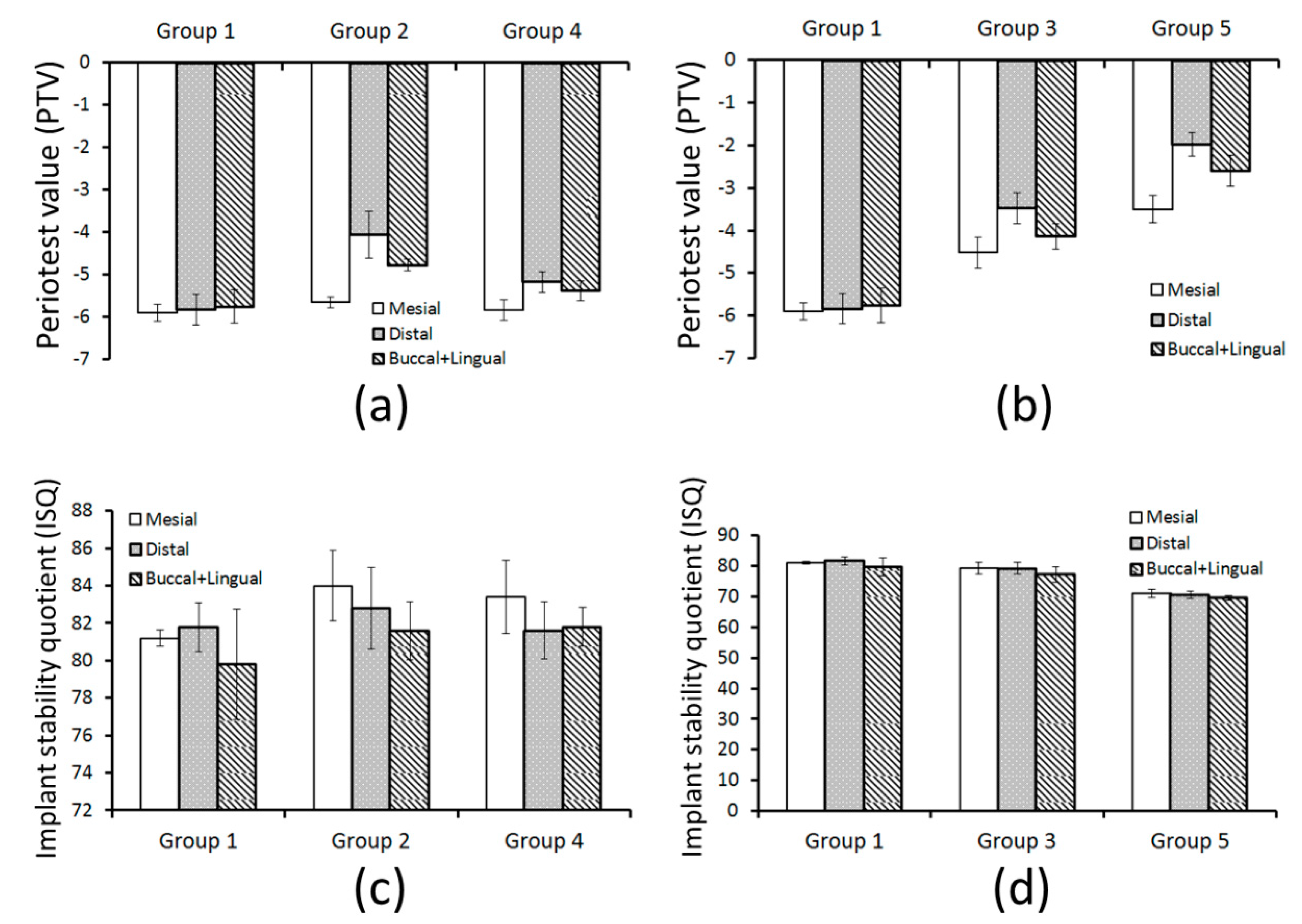
3.1. Differences and Correlations among the Four Measurement Directions of the PTV and ISQ
3.2. Differences of PTV and ISQ among the Three Inserted Angulation
3.3. Differences of PTV and ISQ among the Three Inserted Depth
4. Discussion
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Bouchard, P.; Renouard, F.; Bourgeois, D.; Fromentin, O.; Jeanneret, M.; Beresniak, A. Cost-effectiveness modeling of dental implant vs. bridge. Clin. Oral Implant. Res. 2009, 20, 583–587. [Google Scholar] [CrossRef]
- Branemark, P.-I. Osseointegrated implants in the treatment of the edentulous jaw. Experience from a 10-year period. Scand. J. Plast. Reconstr. Surg. Suppl. 1977, 2, 16. [Google Scholar]
- Hebel, K.; Gajjar, R.; Hofstede, T. Single-tooth replacement: Bridge vs. implant-supported restoration. J. Can. Dent. Assoc. 2000, 66, 435–438. [Google Scholar]
- Javed, F.; Ahmed, H.B.; Crespi, R.; Romanos, G.E. Role of primary stability for successful osseointegration of dental implants: Factors of influence and evaluation. Interv. Med. Appl. Sci. 2013, 5, 162–167. [Google Scholar] [CrossRef]
- Lioubavina-Hack, N.; Lang, N.P.; Karring, T. Significance of primary stability for osseointegration of dental implants. Clin. Oral Implant. Res. 2006, 17, 244–250. [Google Scholar] [CrossRef]
- Javed, F.; Romanos, G.E. The role of primary stability for successful immediate loading of dental implants. A literature review. J. Dent. 2010, 38, 612–620. [Google Scholar] [CrossRef]
- Atsumi, M.; Park, S.-H.; Wang, H.-L. Methods used to assess implant stability: Current status. Int. J. Oral Maxillofac. Implant. 2007, 22, 743–754. [Google Scholar]
- Mistry, G.; Shetty, O.; Shetty, S.; Singh, R.D. Measuring implant stability: A review of different methods. J. Dent. Implant. 2014, 4, 165. [Google Scholar] [CrossRef]
- Atwood, D.A. Reduction of residual ridges: A major oral disease entity. J. Prosthet. Dent. 1971, 26, 266–279. [Google Scholar] [CrossRef]
- Barão, V.; Delben, J.; Lima, J.; Cabral, T.; Assunção, W.G. Comparison of different designs of implant-retained overdentures and fixed full-arch implant-supported prosthesis on stress distribution in edentulous mandible–a computed tomography-based three-dimensional finite element analysis. J. Biomech. 2013, 46, 1312–1320. [Google Scholar] [CrossRef]
- Chen, J.; Ahmad, R.; Suenaga, H.; Li, W.; Swain, M.; Li, Q. A comparative study on complete and implant retained denture treatments–a biomechanics perspective. J. Biomech. 2015, 48, 512–519. [Google Scholar] [CrossRef]
- De Vico, G.; Bonino, M.; Spinelli, D.; Schiavetti, R.; Sannino, G.; Pozzi, A.; Ottria, L. Rationale for tilted implants: FEA considerations and clinical reports. ORAL Implantol. 2011, 4, 23. [Google Scholar]
- Sivolella, S.; Stellini, E.; Testori, T.; Di Fiore, A.; Berengo, M.; Lops, D. Splinted and unsplinted short implants in mandibles: A retrospective evaluation with 5 to 16 years of follow-up. J. Periodontol. 2013, 84, 502–512. [Google Scholar] [CrossRef]
- Silva, L.D.; De Lima, V.; Faverani, L.; De Mendonca, M.; Okamoto, R.; Pellizzer, E. Maxillary sinus lift surgery—With or without graft material? A systematic review. Int. J. Oral Maxillofac. Surg. 2016, 45, 1570–1576. [Google Scholar] [CrossRef]
- Aparicio, C.; Manresa, C.; Francisco, K.; Claros, P.; Alández, J.; González-Martín, O.; Albrektsson, T. Zygomatic implants: Indications, techniques and outcomes, and the zygomatic success code. Periodontol. 2000 2014, 66, 41–58. [Google Scholar] [CrossRef]
- Krekmanov, L.; Kahn, M.; Rangert, B.; Lindström, H. Tilting of posterior mandibular and maxillary implants for improved prosthesis support. Int. J. Oral Maxillofac. Implant. 2000, 15, 405–414. [Google Scholar]
- Chrcanovic, B.R.; Albrektsson, T.; Wennerberg, A. Tilted versus axially placed dental implants: A meta-analysis. J. Dent. 2015, 43, 149–170. [Google Scholar] [CrossRef]
- Maló, P.; Rangert, B.; Nobre, M. “All-on-Four” immediate-function concept with Brånemark System® implants for completely edentulous mandibles: A retrospective clinical study. Clin. Implant Dent. Relat. Res. 2003, 5, 2–9. [Google Scholar] [CrossRef]
- Degidi, M.; Perrotti, V.; Shibli, J.A.; Novaes, A.B.; Piattelli, A.; Iezzi, G. Equicrestal and subcrestal dental implants: A histologic and histomorphometric evaluation of nine retrieved human implants. J. Periodontol. 2011, 82, 708–715. [Google Scholar] [CrossRef]
- Barros, R.R.; Novaes, A.B., Jr.; Muglia, V.A.; Iezzi, G.; Piattelli, A. Influence of interimplant distances and placement depth on peri-implant bone remodeling of adjacent and immediately loaded Morse cone connection implants: A histomorphometric study in dogs. Clin. Oral Implant. Res. 2010, 21, 371–378. [Google Scholar] [CrossRef]
- Todescan, F.F.; Pustiglioni, F.E.; Imbronito, A.V.; Albrektsson, T.; Gioso, M. Influence of the microgap in the peri-implant hard and soft tissues: A histomorphometric study in dogs. Int. J. Oral Maxillofac. Implant. 2002, 17, 467–472. [Google Scholar]
- Rojas-Vizcaya, F.; Zadeh, H.H. Minimizing the discrepancy between implant platform and alveolar bone for tilted implants with a sloped implant platform: A clinical report. J. Prosthet. Dent. 2018, 119, 319–324. [Google Scholar] [CrossRef]
- Maló, P.; de Araújo Nobre, M.; Lopes, A.; Francischone, C.; Rigolizzo, M. “All-on-4” immediate-function concept for completely edentulous maxillae: A clinical report on the medium (3 years) and long-term (5 years) outcomes. Clin. Implant Dent. Relat. Res. 2012, 14, e139–e150. [Google Scholar] [CrossRef]
- Barikani, H.; Rashtak, S.; Akbari, S.; Badri, S.; Daneshparvar, N.; Rokn, A. The effect of implant length and diameter on the primary stability in different bone types. J. Dent. 2013, 10, 449. [Google Scholar]
- Hong, J.; Lim, Y.J.; Park, S.O. Quantitative biomechanical analysis of the influence of the cortical bone and implant length on primary stability. Clin. Oral Implant. Res. 2012, 23, 1193–1197. [Google Scholar] [CrossRef]
- Huang, H.L.; Chang, Y.Y.; Lin, D.J.; Li, Y.F.; Chen, K.T.; Hsu, J.T. Initial stability and bone strain evaluation of the immediately loaded dental implant: An in vitro model study. Clin. Oral Implant. Res. 2011, 22, 691–698. [Google Scholar] [CrossRef]
- Pommer, B.; Hof, M.; Fädler, A.; Gahleitner, A.; Watzek, G.; Watzak, G. Primary implant stability in the atrophic sinus floor of human cadaver maxillae: Impact of residual ridge height, bone density, and implant diameter. Clin. Oral Implant. Res. 2014, 25, e109–e113. [Google Scholar] [CrossRef]
- Mattsson, T.; Köndell, P.-Å.; Gynther, G.W.; Fredholm, U.; Bolin, A. Implant treatment without bone grafting in severely resorbed edentulous maxillae. J. Oral Maxillofac. Surg. 1999, 57, 281–287. [Google Scholar] [CrossRef]
- Rosén, A.; Gynther, G. Implant treatment without bone grafting in edentulous severely resorbed maxillas: A long-term follow-up study. J. Oral Maxillofac. Surg. 2007, 65, 1010–1016. [Google Scholar] [CrossRef]
- Pancko, F.; Dyer, J.; Weisglass, S.; Kraut, R.A. Use of tilted implants in treatment of the atrophic posterior mandible: A preliminary report of a novel approach. J. Oral Maxillofac. Surg. 2010, 68, 407–413. [Google Scholar] [CrossRef]
- Maló, P.; de Araújo Nobre, M.; Lopes, A.; Ferro, A.; Gravito, I. A ll-on-4® Treatment Concept for the Rehabilitation of the Completely Edentulous Mandible: A 7-Year Clinical and 5-Year Radiographic Retrospective Case Series with Risk Assessment for Implant Failure and Marginal Bone Level. Clin. Implant Dent. Relat. Res. 2015, 17, e531–e541. [Google Scholar]
- Elfar, J.; Stanbury, S.; Menorca, R.M.G.; Reed, J.D. Composite bone models in orthopaedic surgery research and education. J. Am. Acad. Orthop. Surg. 2014, 22, 111. [Google Scholar]
- Singh, A.; Sharma, R.; Sharma, R.; Musmade, D. Challenges in cadaver availability for learning and research in medical sciences. Int. J. Med. Clin. Res. 2011, 2, 67–71. [Google Scholar]
- Engelke, W.; Decco, O.A.; Cura, A.C.; Maldonado, I.; Crippa, F.G. Influence of implant diameter in the displacement of dental implants in trabecular bovine bone under a static lateral load: Experimental results and computational modeling. Implant Dent. 2014, 23, 635–640. [Google Scholar] [CrossRef]
- Manresa, C.; Bosch, M.; Echeverría, J.J. The comparison between implant stability quotient and bone-implant contact revisited: An experiment in B eagle dog. Clin. Oral Implant. Res. 2014, 25, 1213–1221. [Google Scholar] [CrossRef]
- Hsu, J.T.; Fuh, L.J.; Tu, M.G.; Li, Y.F.; Chen, K.T.; Huang, H.L. The effects of cortical bone thickness and trabecular bone strength on noninvasive measures of the implant primary stability using synthetic bone models. Clin. Implant Dent. Relat. Res. 2013, 15, 251–261. [Google Scholar] [CrossRef]
- Liu, C.; Tsai, M.-T.; Huang, H.-L.; Chen, M.Y.-C.; Hsu, J.-T.; Su, K.-C.; Chang, C.-H.; Wu, A.Y.-J. Relation between insertion torque and bone–implant contact percentage: An artificial bone study. Clin. Oral Investig. 2012, 16, 1679–1684. [Google Scholar] [CrossRef]
- American Society for Testing and Materials A. ASTM F1839-08 Standard Specification for Rigid Polyurethane Foam for Use as a Standard Material for Testing Orthopedic Devices and Instruments. Available online: https://www.techstreet.com/standards/astm-f1839-08-2016?product_id=1931970 (accessed on 29 March 2020).
- Miyamoto, I.; Tsuboi, Y.; Wada, E.; Suwa, H.; Iizuka, T. Influence of cortical bone thickness and implant length on implant stability at the time of surgery—Clinical, prospective, biomechanical, and imaging study. Bone 2005, 37, 776–780. [Google Scholar] [CrossRef]
- Di Fiore, A.; Sivolella, S.; Stocco, E.; Favero, V.; Stellini, E. Experimental Analysis of Temperature Differences During Implant Site Preparation: Continuous Drilling Technique Versus Intermittent Drilling Technique. J. Oral Implantol. 2018, 44, 46–50. [Google Scholar] [CrossRef]
- Lucchiari, N.; Frigo, A.C.; Stellini, E.; Coppe, M.; Berengo, M.; Bacci, C. In vitro assessment with the infrared thermometer of temperature differences generated during implant site preparation: The traditional technique versus the single-drill technique. Clin. Implant Dent. Relat. Res. 2016, 18, 182–191. [Google Scholar] [CrossRef]
- Swami, V.; Vijayaraghavan, V.; Swami, V. Current trends to measure implant stability. J. Indian Prosthodont. Soc. 2016, 16, 124. [Google Scholar] [CrossRef] [PubMed]
- Wentaschek, S.; Hartmann, S.; Walter, C.; Wagner, W. Six-implant-supported immediate fixed rehabilitation of atrophic edentulous maxillae with tilted distal implants. Int. J. Implant Dent. 2017, 3, 35. [Google Scholar] [CrossRef]
- Han, H.-C.; Lim, H.-C.; Hong, J.-Y.; Ahn, S.-J.; Han, J.-Y.; Shin, S.-I.; Chung, J.-H.; Herr, Y.; Shin, S.-Y. Primary implant stability in a bone model simulating clinical situations for the posterior maxilla: An in vitro study. J. Periodontal Implant Sci. 2016, 46, 254–265. [Google Scholar] [CrossRef] [PubMed]
- Aparicio, C.; Perales, P.; Rangert, B. Tilted implants as an alternative to maxillary sinus grafting: A clinical, radiologic, and periotest study. Clin. Implant Dent. Relat. Res. 2001, 3, 39–49. [Google Scholar] [CrossRef]
- Di, P.; Lin, Y.; Li, J.-H.; Luo, J.; Qiu, L.-X.; Chen, B.; Cui, H.-Y. The All-on-Four implant therapy protocol in the management of edentulous Chinese patients. Int. J. Prosthodont. 2013, 26, 509–516. [Google Scholar] [CrossRef]
- Lopes, A.; Maló, P.; de Araujo Nobre, M.; Sanchez-Fernández, E. The N obel G uide® A ll-on-4® Treatment Concept for Rehabilitation of Edentulous Jaws: A Prospective Report on Medium-and Long-Term Outcomes. Clin. Implant Dent. Relat. Res. 2015, 17, e406–e416. [Google Scholar] [CrossRef]
- Lachmann, S.; Jäger, B.; Axmann, D.; Gomez-Roman, G.; Groten, M.; Weber, H. Resonance frequency analysis and damping capacity assessment: Part 1: An in vitro study on measurement reliability and a method of comparison in the determination of primary dental implant stability. Clin. Oral Implant. Res. 2006, 17, 75–79. [Google Scholar] [CrossRef]
- Elramady, M.M.; Sayed, A.M.; Awadalla, M.A.; Mohamed, F.S.; Nassef, T.M. Measuring primary stability for the inclined implants retaining mandibular overdenture using resonance frequency. In Proceedings of the 2014 Cairo International Biomedical Engineering Conference (CIBEC), Giza, Egypt, 11–13 December 2014; pp. 83–86. [Google Scholar]
- Bergkvist, G.; Nilner, K.; Sahlholm, S.; Karlsson, U.; Lindh, C. Immediate loading of implants in the edentulous maxilla: Use of an interim fixed prosthesis followed by a permanent fixed prosthesis: A 32-month prospective radiological and clinical study. Clin. Implant Dent. Relat. Res. 2009, 11, 1–10. [Google Scholar] [CrossRef]
- Cannizzaro, G.; Leone, M.; Consolo, U.; Ferri, V.; Esposito, M. Immediate functional loading of implants placed with flapless surgery versus conventional implants in partially edentulous patients: A 3-year randomized controlled clinical trial. Int. J. Oral Maxillofac. Implant. 2008, 23, 867–875. [Google Scholar]
- Romanos, G.E.; Aydin, E.; Gaertner, K.; Nentwig, G.H. Long-term results after subcrestal or crestal placement of delayed loaded implants. Clin. Implant Dent. Relat. Res. 2015, 17, 133–141. [Google Scholar] [CrossRef]
- Da Costa Valente, M.L.; de Castro, D.T.; Shimano, A.C.; Lepri, C.P.; dos Reis, A.C. Analysis of the influence of implant shape on primary stability using the correlation of multiple methods. Clin. Oral Investig. 2015, 19, 1861–1866. [Google Scholar] [CrossRef] [PubMed]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Group | Implant Angulations and Inserted Type | Measured Direction (Mean ± SD) | p Value * | Mean of the Four Direction | |||
|---|---|---|---|---|---|---|---|
| Mesial | Distal | Buccal | Lingual | ||||
| 1 | vertical implant with evencrestal position | 81.2 ± 0.447 | 81.8 ± 1.309 | 79.8 ± 2.95 | 79.8 ± 2.95 | 0.314 | 80.7 ± 1.91 |
| 2 | 17° tilted implant with distal subcrestal position | 84 ± 1.87 | 82.8 ± 2.168 | 81.4 ± 1.341 | 81.8 ± 1.789 | 0.149 | 82.5 ± 1.79 |
| 3 | 17° tilted implant with mesial supracrestal position | 79.2 ± 1.924 | 79.2 ± 1.924 | 77.4 ± 2.068 | 77.2 ± 2.49 | 0.346 | 78.3 ± 2.24 |
| 4 | 30° tilted implant with distal subcrestal position | 83.4 ± 1.949 | 81.6 ± 1.517 | 82.2 ± 1.303 | 82.6 ± 1.341 | 0.468 | 82.5 ± 1.6 |
| 5 | 30° tilted implant with mesial supracrestal position | 71 ± 1.414 | 70.6 ± 1.291 | 70.0 ± 0.0 | 70.2 ± 0.447 | 0.207 | 70.6 ± 0.86 |
| Group | Implant Angulations and Inserted Type | Measured Direction (Mean ± SD) | p Value * | ||
|---|---|---|---|---|---|
| Mesial (Mean ± SD) † | Distal (Mean ± SD) | Mean (B&L) (Mean ± SD) | |||
| 1 | vertical implant with evencrestal position | −5.9 ± 0.2 a | −5.84 ± 0.358 a | −5.76 ± 0.397 a | 0.922 |
| 2 | 17° tilted implant with distal subcrestal position | −5.66 ± 0.134 a | −4.06 ± 0.55 b | −4.78 ± 0.144 c | <0.001 |
| 3 | 17° tilted implant with mesial supracrestal position | −4.52 ± 0.37 a | −3.48 ± 0.35 b | −4.13 ± 0.297 a | 0.001 |
| 4 | 30° tilted implant with distal subcrestal position | −5.86 ± 0.251 a | −5.18 ± 0.239 b | −5.39 ± 0.238 b | 0.004 |
| 5 | 30° tilted implant with mesial supracrestal position | −3.5 ± 0.316 a | −1.98 ± 0.277 b | −2.6 ± 0.354 c | <0.001 |
| Group | Implant Angulations and Inserted Type | Correlation (r and p) between the ISQ and Different Measurement Direction of PTV | |||
|---|---|---|---|---|---|
| Mean of Four Direction | Mesial Direction | Distal Direction | Mean of Buccal and Lingual Directions | ||
| 1 | vertical implant with evencrestal position | r = −0.85 (p = 0.04) | |||
| 2 | 17° tilted implant with distal subcrestal position | r = 0.384 (p = 0.523) | r = 0.178 (p = 0.775) | r = −0.949 (p = 0.014) | |
| 3 | 17° tilted implant with mesial supracrestal position | r = −0.673 (p = 0.213) | r = −0.142 (p = 0.82) | r = −0.345 (p = 0.57) | |
| 4 | 30° tilted implant with distal subcrestal position | r = −0.968 (p = 0.007) | r = −0.711 (p = 0.178) | r = −0.636 (p = 0.249) | |
| 5 | 30° tilted implant with mesial supracrestal position | r = −0.200 (p = 0.747) | r = 0.285 (p = 0.642) | r = −0.292 (p = 0.634) | |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Wu, H.-C.; Tsai, M.-T.; Hsu, J.-T. The Effect of Insertion Angles and Depths of Dental Implant on the Initial Stability. Appl. Sci. 2020, 10, 3112. https://doi.org/10.3390/app10093112
Wu H-C, Tsai M-T, Hsu J-T. The Effect of Insertion Angles and Depths of Dental Implant on the Initial Stability. Applied Sciences. 2020; 10(9):3112. https://doi.org/10.3390/app10093112
Chicago/Turabian StyleWu, Hsiang-Chun, Ming-Tzu Tsai, and Jui-Ting Hsu. 2020. "The Effect of Insertion Angles and Depths of Dental Implant on the Initial Stability" Applied Sciences 10, no. 9: 3112. https://doi.org/10.3390/app10093112
APA StyleWu, H.-C., Tsai, M.-T., & Hsu, J.-T. (2020). The Effect of Insertion Angles and Depths of Dental Implant on the Initial Stability. Applied Sciences, 10(9), 3112. https://doi.org/10.3390/app10093112