Oral Manifestations in Patients with Glycogen Storage Disease: A Systematic Review of the Literature


 ,
,  ,
,  , ,
, ,  ,
, 
Abstract
1. Introduction
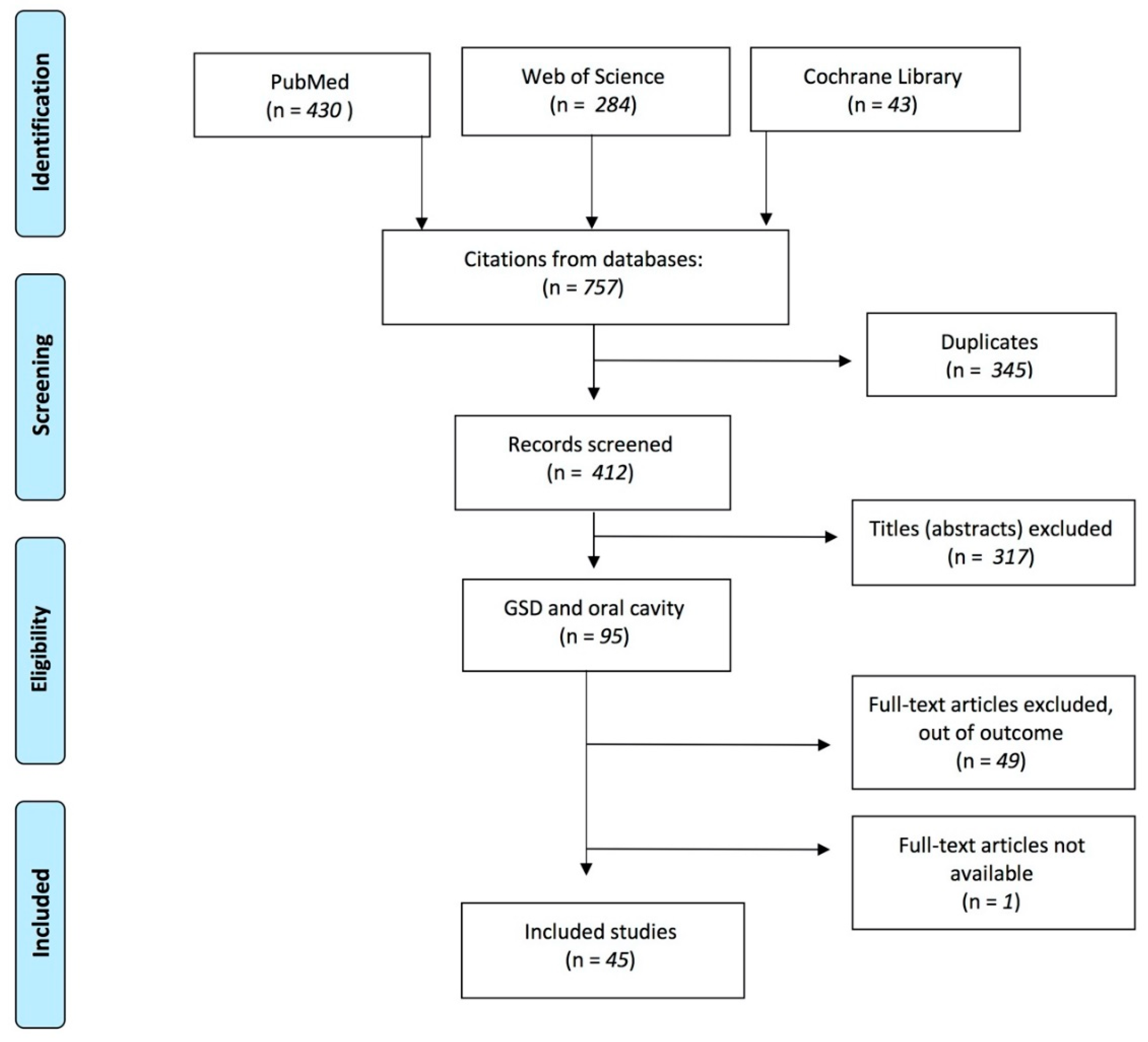
2. Materials and Methods
3. Results
3.1. Risk of Bias in Individual Studies
3.2. GSD Ia
3.3. GSD Ib
3.4. GSD II
3.5. GSD III
3.6. GSD V
3.7. GSD XIV
4. Discussion
Limitations of the Study
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Zhang, X.; Lerman, L.O. The metabolic syndrome and chronic kidney disease. Transl. Res. 2017, 183, 14–25. [Google Scholar] [CrossRef] [PubMed]
- Vega, A.I.; Medrano, C.; Navarrete, R.; Desviat, L.R.; Merinero, B.; Rodríguez-Pombo, P.; Vitoria, I.; Ugarte, M.; Pérez-Cerdá, C.; Pérez, B. Molecular diagnosis of glycogen storage disease and disorders with overlapping clinical symptoms by massive parallel sequencing. Genet. Med. 2016, 18, 1037–1043. [Google Scholar] [CrossRef] [PubMed]
- Saudubray, J.-M.; Baumgartner, M.R.; Walter, J. Inborn Metabolic Diseases; Springer: Berlin/Heidelberg, Germany, 2016. [Google Scholar]
- Farrington, F.H.; Duncan, L.L.; Roth, K.S. Looking a gift horse in the mouth: Effects of cornstarch therapy and other implications of glycogen storage disease on oral hygiene and dentition. Pediatric. Dent. 1995, 17, 311–314. [Google Scholar]
- Horvath, J.J.; Austin, S.L.; Case, L.E.; Greene, K.B.; Jones, H.N.; Soher, B.J.; Kishnani, P.S.; Bashir, M.R. Correlation between quantitative whole-body muscle magnetic resonance imaging and clinical muscle weakness in pompe disease. Muscle Nerve 2015, 51, 722–730. [Google Scholar] [CrossRef] [PubMed]
- Mortellaro, C.; Garagiola, U.; Carbone, V.; Cerutti, F.; Marci, V.; Bonda, P.L.F. Unusual Oral Manifestations and Evolution in Glycogen Storage Disease Type Ib. J. Craniofacial Surg. Surg. 2005, 16, 45–52. [Google Scholar] [CrossRef] [PubMed]
- Minozzi, S.; Cinquini, M.; Gianola, S.; Castellini, G.; Gerardi, C.; Banzi, R. Risk of bias in nonrandomized studies of interventions showed low inter-rater reliability and challenges in its application. J. Clin. Epidemiol. 2019, 112, 28–35. [Google Scholar] [CrossRef]
- Avsar, A. Dental findings in a child with glycogen storage disease type IA. Quintessence Int. 2007, 38, e36–e40. [Google Scholar]
- Iinger, T.M.D.; Livingston, H.M.; Holder, R.; Streckfus, C.F. Glycogen storage disease and von Willebrand’s disease implications for dental treatment: Dental management of a pediatric patient. Spec. Care Dent. 1998, 18, 243–246. [Google Scholar] [CrossRef]
- Duplan, M.B.; Hubert, A.; le Norcy, E.; Louzoun, A.; Perry, A.; Chaussain, C.; Labrune, P. Dental and periodontal manifestations of glycogen storage diseases: A case series of 60 patients. J. Inherit. Metab. Dis. 2018, 41, 947–953. [Google Scholar] [CrossRef]
- Prasad, R.; Estrella, J.; Christodoulou, J.; McKellar, G.; Tchan, M.C. A Third Case of Glycogen Storage Disease IB and Giant Cell Tumour of the Mandible: A Disease Association or Iatrogenic Complication of Therapy. In JIMD Reports; Springer: Berlin/Heidelberg, Germany, 2017; Volume 42, pp. 5–8. [Google Scholar]
- do Amaral, F.R.; Carvalho, V.M.; Fraga, M.G.; Amaral, T.M.P.; Gomes, C.C.; Gomez, R.S. Oral Giant Cell Granuloma in a Patient with Glycogen Storage Disease. Open Dent. J. 2009, 3, 144–146. [Google Scholar] [CrossRef][Green Version]
- Dieckgraefe, B.; Korzenik, J.; Husain, A.; Dieruf, L. Association of glycogen storage disease 1b and Crohn disease: Results of a North American survey. Eur. J. Pediatrics 2002, 161, S88–S92. [Google Scholar] [CrossRef]
- Jones, H.N.; Muller, C.W.; Lin, M.; Banugaria, S.G.; Case, L.E.; Li, J.S.; O’Grady, G.; Heller, J.H.; Kishnani, P.S. Oropharyngeal dysphagia in infants and children with infantile Pompe disease. Dysphagia 2010, 25, 277–283. [Google Scholar] [CrossRef] [PubMed]
- Kishnani, P.S.; Boney, A.; Chen, Y.T. Nutritional deficiencies in a patient with glycogen storage disease type Ib. J. Inherit. Metab. Dis. 1999, 22, 795–801. [Google Scholar] [PubMed]
- Wendel, U.; Schroten, H.; Burdach, S.; Wahn, V. Glycogen storage disease type Ib: Infectious complications and measures for prevention. Eur. J. Pediatrics 1993, 152, 49–51. [Google Scholar] [CrossRef] [PubMed]
- Schroeder, T.; Hildebrandt, B.; Mayatepek, E.; Germing, U.; Haas, R. A patient with glycogen storage disease type Ib presenting with acute myeloid leukemia (AML) bearing monosomy 7 and granulocyte colony-stimulating factor (G-CSF): A case report. J. Med. Case Rep. 2008, 5, 1–5. [Google Scholar]
- Bhattacharya, K.; Heaton, N.; Rela, M.; Walter, J.H.; Lee, P.J. The benefits of liver transplantation in glycogenosis type Ib. J. Inherit. Metab. Dis. 2004, 27, 539–540. [Google Scholar] [CrossRef]
- Ma, R.; Vaziri, F.M.; Sabino, G.J.; Sarmast, N.D.; Zove, S.M.; Iacono, V.J.; Carrion, J.A. Glycogen storage disease IB and severe periodontal destruction: A case report. Dent. J. 2018, 6, 53. [Google Scholar]
- Salapata, Y.; Laskaris, G.; Drogari, E.; Harokopos, E.; Messaritakis, J. Oral manifestations in glycogen storage disease type 1b. J. Oral Pathol. Med. 1995, 24, 136–139. [Google Scholar]
- Barrett, A.P.; Buckley, D.J.; Katelaris, C.H. Oral complications in type 1B glycogen storage disease. Oral Surg. Oral Med. Oral Pathol. 1990, 69, 174–176. [Google Scholar]
- Dougherty, N.; Gataletto, M.A. Oral sequelae of chronic neutrophil defects: Case report of a child with glycogen storage disease type 1b. Pediatrics Dent. 1995, 17, 224–229. [Google Scholar]
- Bartoli, A.; Bossù, A.; Sfasciotti, G.; Polimeni, A. Glycogen Storage Disease type Ib: A paediatric case report. Eur. J. Pediatrics Dent. 2006, 7, 192–198. [Google Scholar]
- Katz, J. Oral manifestations and anesthesia considerations in a child with glycogen storage disease type 1b: Case report. Pediatrics Dent. 1997, 19, 123–126. [Google Scholar]
- Dagli, A.I.; Lee, P.J.; Correia, C.E.; Rodriguez, C.; Bhattacharya, K.; Steinkrauss, L.; Stanley, C.A.; Weinstein, D.A. Pregnancy in glycogen storage disease type Ib: Gestational care and report of first successful deliveries. J. Inherit. Metab. Dis. 2010, 33, 151–157. [Google Scholar] [CrossRef]
- Jones, H.N.; Crisp, K.D.; Asrani, P.; Sloane, R.; Kishnani, P.S. Quantitative assessment of lingual strength in late-onset Pompe disease. Muscle Nerve 2015, 51, 731–735. [Google Scholar] [CrossRef] [PubMed]
- Margolis, M.L.; Howlett, P.; Goldberg, R.; Eftychiadis, A.; Levine, S. Obstructive Sleep Apnea Syndrome in Acid Maltase Deficiency. Chest 1994, 105, 947–949. [Google Scholar] [CrossRef] [PubMed]
- Huie, M.L.; Kasper, J.S.; Arn, P.H.; Greenberg, C.R.; Hirschhorn, R. Increased occurrence of cleft lip in glycogen storage disease type II (GSDII): Exclusion of a contiguous gene syndrome in two patients by presence of intragenic mutations (Am J Med Genet 85: 5-8(1999)). Am. J. Med. Genet. Part A 2005, 137A, 114. [Google Scholar]
- Pichiecchio, A.; Rossi, M.; Cinnante, C.; Colafati, G.S.; de Icco, R.; Parini, R.; Menni, F.; Furlan, F.; Burlina, A.; Sacchini, M.; et al. Muscle MRI of classic infantile pompe patients: Fatty substitution and edema-like changes. Muscle Nerve 2017, 55, 841–848. [Google Scholar]
- Maggi, L.; Salerno, F.; Bragato, C.; Saredi, S.; Blasevich, F.; Maccagnano, E.; Pasanisi, B.; Danesino, C.; Mora, M.; Morandi, L. Familial adult-onset Pompe disease associated with unusual clinical and histological features. Acta Myol. 2013, 32, 85–90. [Google Scholar]
- Horvath, J.J.; Austin, S.L.; Jones, H.N.; Drake, E.J.; Case, L.E.; Soher, B.J.; Bashir, M.R.; Kishnani, P.S. Bulbar muscle weakness and fatty lingual in fi ltration in glycogen storage disorder type IIIa. Mol. Genet. Metab. 2012, 107, 496–500. [Google Scholar]
- Fecarotta, S.; Ascione, S.; Montefusco, G.; della Casa, R.; Villari, P.; Romano, A.; del Giudice, E.; Andria, G.; Parenti, G. Improvement of dysphagia in a child affected by Pompe disease treated with enzyme replacement therapy. Ital. J. Pediatrics 2013, 39, 30. [Google Scholar]
- Dubrovsky, A.; Corderi, J.; Lin, M.; Kishnani, P.S.; Jones, H.N. Expanding the phenotype of late-onset pompe disease: Tongue weakness: A new clinical observation. Muscle Nerve 2011, 44, 897–901. [Google Scholar] [CrossRef] [PubMed]
- Szklanny, K. Analysis of voice quality in patients with late-onset Pompe disease. Orphanet J. Rare Dis. 2016, 11, 1–9. [Google Scholar] [CrossRef] [PubMed]
- de Pinto, W.B.V.; de Souza, P.V.S.; Bortholin, T.; Naylor, F.G.M.; Oliveira, A.S.B. Abnormal tongue features as a clinical clue for late-onset Pompe’s disease. Arq. Neuro-Psiquiatria 2017, 75, 835–836. [Google Scholar] [CrossRef] [PubMed]
- Felice, K.J.; Alessi, A.G.; Grunnet, M.L. Clinical variability in adult-onset acid maltase deficiency: Report of affected sibs and review of the literature. Medicine 1995, 74, 131–135. [Google Scholar] [CrossRef]
- Milisenda, J.C.; Pujol, T.; Grau, J.M. Not only bright tongue sign in Pompe disease. Neurology 2016, 87, 1629–1630. [Google Scholar] [CrossRef]
- Hobson-webb, L.D.; Jones, H.N.; Kishnani, P.S. Oropharyngeal dysphagia may occur in late-onset Pompe disease, implicating bulbar muscle involvement. Neuromuscul. Disord 2013, 23, 319–323. [Google Scholar] [CrossRef]
- de Gijt, J.P.; van Capelle, C.I.; Oosterhuis, J.W.; van der Ploeg, A.T.; van der Wal, K.G.H. Gingival Overgrowth in Pompe Disease: A Case Report. J. Oral Maxillofac. Surg. 2011, 69, 2186–2190. [Google Scholar] [CrossRef]
- Baccetti, T.; Pierleoni, L.; Filippi, L.; Donati, M.A.; Tollaro, I.; Zammarchi, E. Dental and craniofacial findings in a child affected by glycogen storage disease type III. J. Clin. Pediatrics Dent. 1994, 19, 55–60. [Google Scholar]
- Cleary, M.A.; Walter, J.H.; Kerr, B.A.; Wraith, J.E. Facial appearance in glycogen storage disease type III. Clin. Dysmorphol. 2002, 11, 117–120. [Google Scholar] [CrossRef]
- Thornhill, M.H. Masticatory muscle symptoms in a patient with McArdle’s disease. Oral Surg. Oral Med. Oral Pathol. Oral Radiol Endodontol. 1996, 81, 544–546. [Google Scholar] [CrossRef]
- Kouwenberg, C.V.; Voermans, N.C.; Quinlivan, R.; van den Engel-Hoek, L. Mastication and Oral Motor Function in McArdle Disease: Patient Reported Complaints. J. Neuromuscul. Dis. 2018, 5, 353–357. [Google Scholar] [CrossRef] [PubMed]
- Wong, S.Y.-W.; Beamer, L.J.; Gadomski, T.; Honzik, T.; Mohamed, M.; Wortmann, S.B.; Holmefjord, K.S.B.; Mork, M.; Bowling, F.; Sykut-Cegielska, J.; et al. Defining the Phenotype and Assessing Severity in Phosphoglucomutase-1 Deficiency. J. Pediatrics 2016, 175, 130–136. [Google Scholar] [CrossRef] [PubMed]
- Loewenthal, N.; Haim, A.; Parvari, R.; Hershkovitz, E. Phosphoglucomutase-1 deficiency: Intrafamilial clinical variability and common secondary adrenal insufficiency. Am. J. Med. Genet. Part A 2015, 167, 3139–3143. [Google Scholar] [CrossRef] [PubMed]
- Nina Ondruskova, H.H.; Honzik, T.; Vondrackova, A.; Tesarova, M.; Zeman, J. Department. Glycogen storage disease-like phenotype with central nervous system involvement in a PGM1-CDG patient Nina. Neuroendocrinol. Lett 2014, 35, 137–141. [Google Scholar]
- Kidd, S.A.; Rademeyer, C.; Roberts, G.J.; Lee, P.J.; Lucas, V.S. Dental disease indices and caries-related microflora in children with glycogen storage disease. Int. J. Paediatr. Dent. 2002, 12, 8–13. [Google Scholar] [PubMed]
- Kishnani, P.S.; Austin, S.L.; Abdenur, J.E.; Arn, P.; Bali, D.S.; Boney, A.; Chung, W.K.; Dagli, A.I.; Dale, D.; Koeberl, D.; et al. Diagnosis and management of glycogen storage disease type I: A practice guideline of the American College of Medical Genetics and Genomics. Genet. Med. 2014, 16, 1–29. [Google Scholar] [CrossRef]
- Martinez, C.C.; Tonon, T.; Nalin, T.; Refosco, L.F.; de Souza, C.F.M.; Schwartz, I.V.D. Feeding Difficulties and Orofacial Myofunctional Disorder in Patients with Hepatic Glycogen Storage Diseases. In JIMD Reports; Springer: Berlin/Heidelberg, Germany, 2018; Volume 45, pp. 21–27. [Google Scholar]


{kind=link}
| # | Author | Study Population | Exposure | Outcome | Study Design | Oral Manifestations |
|---|---|---|---|---|---|---|
| 1 | Prasad R et al. (2017) | 1 (child) | GSD Ib | A Case of Glycogen Storage Disease IB and Giant Cell Tumour of the Mandible | Case report | Giant Cellular Tumour of the mandible; |
| 2 | Jones HN et al. (2015) | 30 (adults) | GSD II | Quantitative assessment of lingual strength in late-onset Pompe disease. | Retrospective study | Tongue Weakness |
| 3 | Fecarotta S et al. (2013) | 1 (child) | GSD II | Improvement of dysphagia in a child affected by Pompe disease treated with enzyme replacement therapy. | Case report | Macroglossia |
| 4 | Hobson-Webb LD et al. (2013) | 3 (adults) | GSD II | Oropharyngeal dysphagia in late-onset Pompe disease, implicating bulbar muscle involvement. | Case series | Tongue Weakness |
| 5 | Horvath JJ et al. (2012) | 3 (2 adults/1 child) | GSD IIIa | Bulbar muscle weakness and fatty lingual infiltration in glycogen storage disorder type IIIa. | Case series | Tongue Weakness |
| 6 | Gijt JP et al. (2011) | 1 (child) | GSD II | Gingival overgrowth in Pompe disease | Case report | Gingival overgrowth; Malocclusion (3rd class Angle) |
| 7 | Dagli Al et al. (2010) | 3 (adults) | GSD Ib | Pregnancy in glycogen storage disease type Ib. | Case series | Oral Ulcers |
| 8 | Jones HN et al. (2010) | 13 (children) | GSD II | Oropharyngeal dysphagia in infants and children with infantile Pompe disease. | Case series | Tongue thrust, oral dysmotility, lip incompetence, and oral disorganization in 3/13 subjects (23%) |
| 9 | Amaral Fr et al. (2009) | 1 (adult) | GSD Ib | Oral giant cell granuloma in a patient with glycogen storage disease. | Case report | Hyperplasic purplish lesion localized adjacent to the teeth 32, 33 and 34 |
| 10 | Melis D et al. (2009) | 7 (6 adults/1 child) | GSD Ib | Vitamin E supplementation improves neutropenia and reduces the frequency of infections in patients with glycogen storage disease type 1b. | Prospective study | Oral Ulcers |
| 11 | Avsar A (2007) | 1 (child) | GSD Ia | Dental findings in a child with glycogen storage disease type IA. | Case report | Delayed mixed dentition; tooth decay; taurodontism of both primary and permanent molars |
| 12 | Mortellaro C et al. (2005) | 1 (child) | GSD Ib | Unusual oral manifestations and evolution in glycogen storage disease type Ib. | Case report | Periodontitis; Oral ulcers |
| 13 | Dieckgraefe BK et al. (2002) | 36 (children) | GSD Ib | Association of glycogen storage disease 1b and Crohn disease | Retrospective study | 9 subjects (25%) had evidence of oral manifestations, including aphthous stomatitis, or periodontitis |
| 14 | Kidd SA et al. (2002) | 21 (children) | GSD Ia (6); GSD Ib(3); GSD IIII (12) | Dental disease indices and caries-related microflora in children with glycogen storage disease. | Case series | 3 children had caries experience in the primary teeth; 1 caries experience in both the primary and permanent teeth; visible plaque deposits were recorded in all children except one; Gengivitis was present in 62% of the children |
| 15 | Kishnani PS et al. (1999) | 1 (child) | GSD Ib | Nutritional deficiencies in a patient with glycogen storage disease type Ib. | Case report | Dry lips, Beefy red appearance of the tongue and mucous membranes |
| 16 | Dellinger TM et al. (1998) | 1 (child) | GSD Ia | Glycogen storage disease and von Willebrand’s disease implications for dental treatment: dental management of a pediatric patient. | Case report | multiple caries lesions; High levels of plaque; |
| 17 | Katz J et al. (1997) | 1 (child) | GSD Ib | Oral manifestations and anesthesia considerations in a child with glycogen storage disease type 1b. | Case report | Oral ulcers; Gingivitis; Delay in eruption time; Hypodontia of primary teeth |
| 18 | Thornhill MH (1996) | 1 (adult) | GSD V | Masticatory muscle symptoms in a patient with McArdle’s disease. | Case report | Tmj disfunction; massetere and temporal pain. |
| 19 | Dougherty N et al. (1995) | 1 (child) | GSD Ib | Oral sequelae of chronic neutrophil defects in a child with glycogen storage disease type 1b. | Case report | Early bone loss; Early primary tooth loss |
| 20 | Salapata Y et al. (1995) | 3 (children) | GSD Ib | Oral manifestations in glycogen storage disease type 1b. | Case series | Case 1: Oral ulcer; Geographic tongue. Case 2: Oral ulcers; Gingival recession; Gingival bleeding. Case 3: Narrow palate; Severe recurrent oral ulcers |
| 21 | Margolis ML et al. (1994) | 1 (adult) | GSD II | Obstructive sleep apnea syndrome in acid maltase deficiency. | Case report | Tongue Weakness |
| 22 | Baccetti T et al. (1994) | 1 (child) | GSD III | Dental and craniofacial findings in a child affected by glycogen storage disease type III. | Case report | Taurodontism of primary dentition; Malocclusion (II class Angle) |
| 23 | Wendel U et al. (1993) | 1 (adult) | GSD Ib | Glycogen storage disease type Ib: infectious complications and measures for prevention. | Case report | Oral abscesses; Oral ulcers; Periodontitis |
| 24 | Barrett AP et al. (1990) | 1 (adult) | GSD Ib | Oral complications in type 1B glycogen storage disease. | Case report | Fissure adjacent the right edentulous mandibular alveolar ridge; Browny swelling at the lower bord of the mandible; Traumatic ulceration corresponded to the buccal extention of the lower dentur; Ulceration on the dorsum of the tongue |
| 25 | Huie ML et al. (2005) | 2 (children) | GSD II | Increased occurrence of cleft lip in glycogen storage disease type II (GSDII). | Case series | 1/2 Bilateral severe cleft lip and palate |
| 26 | Cleary MA et al. (2002) | 2 (children) | GSD III | Facial appearance in glycogen storage disease type III. | Case series | Case 1: Midface hypoplasia; bow-shaped upper lip with a thin vermillon. Case 2: Short philtrum; Midface hypoplasia |
| 27 | Pichiecchio A et al. (2017) | 9 (children) | GSD II | Muscle MRI of classic infantile pompe patients: Fatty substitution and edema-like changes. | Case series | 7 subjects with macroglossia; 6 subjects with tongue weakness |
| 28 | Horvath JJ et al. (2015) | 22,11 case and 11 control (10 adults/1 child) | GSD II | Correlation between quantitative whole-body muscle magnetic resonance imaging and clinical muscle weakness in Pompe disease. | Case-control study | 11 tongue weakness |
| 29 | Maggi L et al. (2013) | 1 (adult) | GSD II | Familial adult-onset Pompe disease associated with unusual clinical and histological features. | Case report | Tongue Weakness |
| 30 | Dubrovsky A et al. (2011) | 11 (adults) | GSD II | Expanding the phenotype of late-onset Pompe disease: tongue weakness. | Cross-sectional study | Tongue Weakness |
| 31 | Szklanny K et al. (2016) | 19 (5 children/14 adults) | GSD II | Analysis of voice quality in patients with late-onset Pompe disease. | Comparative study | 9 subjects had an excessive muscle tension of sub-mandibular areas, 2 subjects with short soft palate |
| 32 | Wong SY et al. (2016) | 27 (18 children/9 adults) | GSD XIV | Defining the Phenotype and Assessing Severity in Phosphoglucomutase-1 Deficiency. | Cross-sectional study | 70% cleft palate; 67% bifid uvula |
| 33 | Loewenthal N et al. (2015) | 7 (5 children/2 adults) | GSD XIV | Phosphoglucomutase-1 deficiency: intrafamilial clinical variability and common secondary adrenal insufficiency. | Retrospective study | 1 Pierre–Robin; 3 Cleft palate; 3 Bifid uvula |
| 34 | Ondruskova N et al. (2014) | 1 (child) | GSD XIV | Glycogen storage disease-like phenotype with central nervous system involvement in a PGM1-CDG patient. | Case report | Cleft palate |
| 35 | Bartoli A et al. (2006) | 1 (child) | GSD Ib | Glycogen Storage Disease type Ib in a paediatric case. | Case report | Oral candidiasis; Oral ulcers; Gingivitis; Bone difect; Periodontal index 4 |
| 36 | Farrington et al. (1995) | 1 (child) | GSD Ib | Effects of cornstarch therapy and other implications of glycogen storage disease on oral hygiene and dentition. | Case report | Oral ulcers; Enamel decalcification; Several posterior teeth had occlusal and interproximal decay; Hard swelling was noted in the left cheek and intraoral rednesss and swelling noted in the left mucobuccalfold in the area of the maxillary left primary canine and first primary molar |
| 37 | Schroeder T et al. (2008) | 1 (adult) | GSD Ib | A patient with glycogen storage disease type Ib presenting with acute myeloid leukemia (AML) bearing monosomy 7 and translocation t(3;8)(q26;q24) after 14 years of treatment with granulocyte colony-stimulating factor (G-CSF) | Case report | Aphthous ulcers; Mucosa bleeding |
| 38 | Kouwenberg CV et al. (2018) | 28 (adult) | GSD V | Mastication and Oral Motor Function in McArdle Disease: Patient Reported Complaints | Survey study | Difficulties with mastication; Cramps in muscles |
| 39 | Ma et al. (2018) | 1 (child) | GSD Ib | A case of GSD type Ib and its associated oral manifestations with microbial, immunological and histological appearances | Case report | Extensive generalized inflammation of the gingiva, erythema, ulceration, and generalized deep periodontal pocketing with bleeding on probing; severe horizontal bone loss. |
| 40 | Martinez et al. (2018) | 36 (children) | GSD Ia (22); GSD Ib1 (8); GSD III (2); GSD IXa (3); GSD IXc (1) | Prevalence of feeding difficulties (FDs) and orofacial myofunctional disorders (OMDs) | Cross-sectional study | FDs: 72.2% (26); OMDs: 1 mouth breathing (12) and oronasal-type breathing (12) |
| 41 | Pinto et al. (2017) | 1 (adult) | GSD II | Abnormal tongue features | Case report | Tongue weakness with fatty infiltration, diffuse tongue atrophy, bnormal fatty replacement of the tongue musculature resembling a “tumor-like” structure |
| 42 | Duplan et al. (2018) | 60 children/adults | GSD Ia (25); GSD Ib (4); GSD III (24); GSD IX (7) | Dental and periodontal manifestations of glycogen storage diseases | Cross-sectional study | Delayed tooth eruption, tooth agenesis, tooth shape abnormalities, severe periodontitis (GSD Ib and neutropenia) |
| 43 | Bhattacharya (2004) | 2 (children) | GSD Ib | How liver transplantation may lead to clinical improvement in patients with GSD Ib | Case report | Oral ulcers |
| 44 | Felice (1995) | 2 (adults) | GSD II | Increasing knowledge about clinical features of GSD II (AMD) | Case report | 1°: swallowing problems, macroglossia, moderate weakness of the tongue; 2°: no oral features |
| 45 | Milisenda (2016) | 1 (adult) | GSD II | Unusual finding in a patient with GSD II | Case report | Bright tongue (MRI); pseudohypertrophy of the tongue, tumor at right side of atrophic tongue |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Romano, A.; Russo, D.; Contaldo, M.; Lauritano, D.; Vella, F.d.; Serpico, R.; Lucchese, A.; Stasio, D.D. Oral Manifestations in Patients with Glycogen Storage Disease: A Systematic Review of the Literature. Appl. Sci. 2020, 10, 6720. https://doi.org/10.3390/app10196720
Romano A, Russo D, Contaldo M, Lauritano D, Vella Fd, Serpico R, Lucchese A, Stasio DD. Oral Manifestations in Patients with Glycogen Storage Disease: A Systematic Review of the Literature. Applied Sciences. 2020; 10(19):6720. https://doi.org/10.3390/app10196720
Chicago/Turabian StyleRomano, Antonio, Diana Russo, Maria Contaldo, Dorina Lauritano, Fedora della Vella, Rosario Serpico, Alberta Lucchese, and Dario Di Stasio. 2020. "Oral Manifestations in Patients with Glycogen Storage Disease: A Systematic Review of the Literature" Applied Sciences 10, no. 19: 6720. https://doi.org/10.3390/app10196720
APA StyleRomano, A., Russo, D., Contaldo, M., Lauritano, D., Vella, F. d., Serpico, R., Lucchese, A., & Stasio, D. D. (2020). Oral Manifestations in Patients with Glycogen Storage Disease: A Systematic Review of the Literature. Applied Sciences, 10(19), 6720. https://doi.org/10.3390/app10196720