Abstract
In recent years, the Body Weight Support system has been considered to be an indispensable component in gait training systems, which be used to improve the ability to walk of hemiplegic, stroke, and spinal cord injury patients. Previous studies investigated the influence of the Body Weight Support system on gait parameters were based on the implementation with healthy subjects or patients with high assistance. Consequently, the influences of the Body Weight Support systems on gait rehabilitation in clinical practice are still unclear and need further investigation. In this study, we investigated the effects of the two Body Weight Support systems, the active body weight support system and the Counter Weight system, on an abnormal gait, which was generated by restriction of the right knee joint and 3 kg-weight on the right ankle joint. Both Body Weight Support systems improve the gait parameters of the abnormal gait such as the center of mass, the center of pressure, margin of stability, and step parameters. The active Body Weight Support system with the unloading force modulation showed more advanced and better behavior in comparison with the Counter Weight system. The results suggested the applicability of two Body Weight Support systems in clinical practice as a recovered gait intervention.
1. Introduction
Hemiparesis and impaired ambulation are commonly resultant of spinal cord injury and stroke [1,2]. According to the National Spinal Cord Injury Statistical Center (the United States (US)), the estimated number of people with SCI living in the United States is approximately 291,000 persons, with a range from 249,000 to 363,000 persons, about 17,730 new SCI cases (equivalent to 54 cases/million population) each year [3]. The number of incidents per million people per year varies widely by country, such as 27 in Japan [4], 13.4 in Switzerland [5], 12.7 in France [6], and 57.8 in Portugal [7]. Also, a report from the American Heart Association showed that an estimated 7.0 million Americans ≥20 years of age had a stroke [8]. The ratio of patients be able to walk again after recovery from SCI is only from one fourth to one third [9,10,11,12]. In terms of stroke patients, the new sufferers of stroke in the US are from 795,000 cases, about 26% remained disabled in necessary activities of daily living, and about 50% have reduced mobility due to hemiparesis [2]. Hemiparesis, locomotor disability, and impaired ambulation made an adverse impact on the daily life quality of the patient and cost up to billions of dollars for health care expenditures [2,13].
In recent studies, the Body Weight Support (BWS) system was considered to be an indispensable component in gait training systems that have been used to improve the ability to walk of hemiplegic, stroke, and spinal cord injury patients. The BWS system was used in many locomotion rehabilitation systems regardless of whether treadmill-based systems [14] or ground-based systems [15]. The evolution of the BWS system for gait training was based on the observation of the recovery of spinal cord cutting cats when implementation gait training for them with the weight-support and the full weight [16,17]. The application of the treadmill BWS system was then extended for the human gait training. Finch et al. investigated the influence of BWS on human gait [18]. Their findings showed that the Treadmill BWS system expressed the advantaged behaviors in every examined aspect and had potential extensive applicability in clinical gait training. The application of Martha Visintin et al. examined the differences between weight support and full weight-bearing in locomotor rehabilitation with 100 stroke-patient participation [19]. The results confirmed that gait training for a patient who was supported by the BWS provided walking ability better than the patient training with bearing full weight. The BWS system, then, is widely applied in locomotor rehabilitation from the laboratory to clinical [15,20,21,22,23,24] for both overground walking training [15,25,26] and treadmill walking training [23,27,28,29]. In recent years, the Treadmill BWS system in conjugation with orthosis robots was applied for many gait training systems to reduce the therapy cost and labor [30,31,32,33,34].
The BWS system, currently, was theoretically considered to be a clinical intervention in neuro-rehabilitation [35,36]. The principle of BWS training as an intervention is to improve motor performance by supplying the injured nervous system with the appropriate sensory input [37]. The influence of the BWS system on gait parameters while training has been investigated, such that the BWS system showed promise and potential as a clinical treatment that improves the locomotor function and ability to walk of hemiplegic, stroke, and spinal cord injury patients [15,19,21,22]. For example, Vinsintin et al. indicated that patients with stroke could walk better while their weight was supported [19]. Schindl MR et al. showed that the walking ability of the nonambulatory patients with cerebral palsy was improved after walking training on the treadmill with a part of body weight supported [27]. Walking speeds of the spinal cord injury patients were improved after training with the BWS system and electrical stimulation [38].
The implementation of the BWS system on the gait training would change the gait parameters and impact to the gait therapeutic effect. Previous studies investigated the influence of the BWS system on gait parameters were based on the implementation of healthy subjects [23,39,40,41]. The results of the implementation of the BWS system on the healthy subject just presented how the effect of the BWS system on the normal gait parameters or how gait parameters of the healthy subject changed while walking under the BWS system. In contrast, the improvement of the locomotor functionality after gait training under the BWS system has been shown clinically for hemiplegic, stroke, and spinal cord injury patients [15,19,21,22,28,29,35,38]. The gait parameters, in clinical, in which the BWS system implemented on gait training for the disorder patient may impact by many external factors such as the treadmill, the support of the therapist, or robotic. Therefore, the contribution of the BWS system on gait rehabilitation as an intervention in clinical is still unclear and needs further investigation.
In the present study, we investigate the influence of the unmodulated BWS system based on the Counter Weight (CW) system and modulated BWS system power by the Pneumatic Muscle Actuator (called active Body Weight Support system) on the gait characteristics of abnormal gait during walking on the treadmill. The abnormal gait was generated by a healthy subject walking on the treadmill; however, the knee motion on one side was restricted. We hypothesis that the active Body Weight Support (ABWS) system may improve the gait characteristics and provide better behavior in comparison with the CW system.
2. Materials and Methods
2.1. Apparatus
Two BWS systems were used to implement in this study: the ABWS system power by the pneumatic artificial muscles (PAMs) and the CW system. A detailed description of the ABWS system was described in the previous study [42]. Basically, the AWBS system contains four PAMs connected directly to the subject body via a harness. Four proportional pressure regulators drove the four PAMs. The unloading force was measured by load-cells and controlled actively by the controller. The principal scheme of the ABWS is shown in Figure 1A. Because of the flexibility of four PAMs, the therapist can apply many weight support strategies in gait training such as one-side support [43], or center of pressure (COP) tracking by the supported force. In this paper, the weight support strategy was implemented similarly as the previous study [42]. Such that the supported force from the ABWS system would follow the movement of COP. When the COP moves from left to right, the support force will decrease on the left side and increase on the right side. Inversely, when the COP moves from right to left, the supported force amplitude will decrease on the right side and increase on the left side.
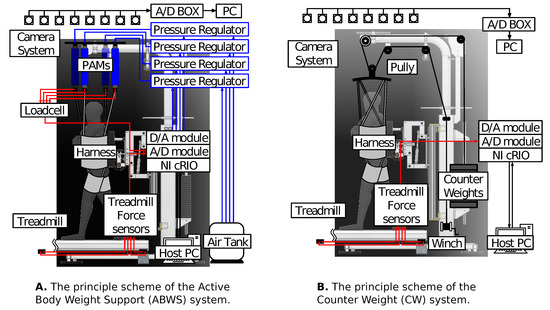
Figure 1.
The principle scheme of the Active Body Weight Support (ABWS) system (A) and the Counter Weight (CW) system (B) which integrated with the treadmill for gait rehabilitation.
In contrast with the working principle of the ABWS system, the CW system passively provides the supported force by a counter-weight. The principal scheme of the CW system is presented in Figure 1B. The structure of the CW system contains several counter-weights connecting with the subject body through the rope-pulley mechanism. The amount of supported force will equivalent to the number of counter-weights set in the backside. In the CW system, without the adjustment actuator, the supported force cannot be changed during gait training. In Figure 1, both the ABWS and CW systems are integrated with a treadmill for gait training.
2.2. Experiment Protocol
Ten healthy subjects (all subjects were male with age= 24.2 ± 3.2 (mean ± SD), height = 172.1 ± 6.1, and weight = 61.5 ± 6.51) volunteered to participate in the experiment. All subjects were free of any neurological pathology or musculoskeletal disorder and no prehistoric disability. Each subject received all information on the experiment procedure and provided the written informed consent prior to joining our experiment. Each subject walked on the treadmill under four conditions in this experiment. Firstly, the subject implemented the normal walking in which subject walking on the treadmill without any constraint. Secondly, the subject implemented the abnormal walking in which the right knee joint motion was restricted with two braces. Furthermore, the subject carried a load of three kg on the right ankle joint while walking on the treadmill. With two constraints, as shown in Figure 2, subjects reproduced the gait pattern of hemiplegia, and this walking condition was called abnormal walking. In the third condition, subjects implemented the abnormal walking on the treadmill with the weight supported by using the ABWS system with the unloading force level at 30%, 50%, and 70% of the subject weight. Finally, the subject implemented the abnormal walking on the treadmill under the CW system with the unloading force level at 30%, 50%, and 70% of the subject weight. The treadmill speed ramped from zero to two km/h by step of 0.1 km/h and kept steadily at 2 km/h. Subjects adapted to the steadied speed in one minute before recording data. The experiment protocol was approved by the ethical committee of the Shibaura Institute of Technology before implementation.

Figure 2.
The reproduction of the hemiplegia by restricted the knee joint motion and a load of 3 kg on the ankle joint.
2.3. Data Collection
Sixteen reflective markers placed bilaterally on the first metatarsal, the fifth metatarsal, lateral malleolus, calcaneus, lateral condyle, greater trochanter, pelvis, and acromion to collect the kinematic data. All markers coordinations were recorded by the motion capture system (Motion Analysis, Santa Rosa, CA, USA) with eight with cameras with sampling frequency at 200 Hz. Also, data from four force sensors embedded under the treadmill was recorded with sampling frequency 1000 Hz. The data from force sensors were synchronized with the marker data and were used to calculate the COP coordination during subject walking.
2.4. Data Processing
The discrete marker positions recorded by the motion capture system were manually corrected frame by frame and smoothed with a second-order low-pass filter with a cutoff frequency at six Hz. The sensor signals from the embedded force sensors under the treadmill were smoothed with the second-order low-pass filter with the cutoff frequency at 10 Hz. The smoothed data was cut to be every single gait cycle using the heel strike (HS). The gait events, the heel strike (HS) and the toe-off (TO), were found by the vertical component of the speed of the markers located at the calcaneus and the first metatarsal, respectively. All single gait cycles were finally normalized to 100% of one gait cycle.
The MATLAB (The MathWorks, Inc., Natick, MA, USA ) routines were developed to calculate the COM and the margin of stability (MOS), and the COP. The COM trajectories of the total subject body were calculated as the summation of the weighted COP coordinations of each body segment in three dimensions [44]. The trajectory COP, however, depended on both the ground reaction force and the COM could be calculated based on the force sensors data. The MOS represents the dynamic stability during gait and can be determined using the base of support (BOS) and the extrapolated center of mass (XcoM) [45]. The MOS and XcoM are shown by
in which represents for the BOS boundary, x and v represents the COM in frontal direction and its velocity, respectively. represents the natural frequency, which is calculated base on the pendulum model with the rotation axis at the foot and the pendulum at the COM. In Equation (1), the BOS boundary was determined using the distance between the markers on the left and right fifth metatarsal bones during the double support phase [45,46]; however, it was adjusted as the distance between the markers on the fifth metatarsal bone and the first metatarsal bone during the single support phase [47]. The definition of the BOS boundary is given in Figure 3.
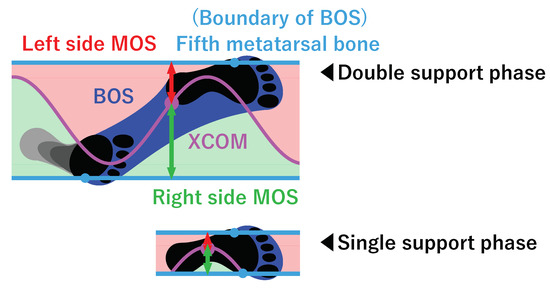
Figure 3.
The BOS boundary was defined as the distance between the left and right Fifth metatarsal bones and the distance between the fifth metatarsal bone, and the first metatarsal bone for the double support phase, and the single support phase, respectively.
The range of motion (ROM) of the hip, knee, and ankle angles was considered in the anterior-posterior (AP) direction only. The definition of the hip, knee, and ankle angles are shown in Figure 4 and are calculated using the relative leg segments coordinations as in Equation (3). In addition, the step width, step length, and stride length were calculated using the detected HS and TO gait events. The quantitative parameters of each subject were standardized to the parameters of the normal walking condition. All quantitative data of each subject were standardized to mean values of the normal walking condition before combining together and analysis. The one-way analysis of variance (ANOVA) on ranks method was used to investigate the differences among walking conditions of the combination data of all subjects.
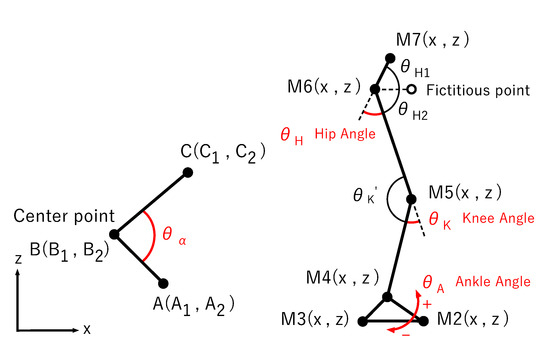
Figure 4.
The range of motions (ROM) of the hip, knee, and ankle angle were calculated using the relative leg segments coordinations.
3. Results
3.1. COM Movement
Figure 5 shows the comparison of the COM trajectories while subjects walked on the treadmill with different conditions. All the trajectories of all subjects were normalized, such that the gait cycle from 0% to 100%. In Figure 5, the mean trajectories are shown as the bold strokes, while the blurred area surrounding represents the variance of the COM trajectories (standard deviation). Row (a) shows the comparisons of the COM trajectories between normal walking and abnormal walking in the sagittal, horizontal, and vertical direction, respectively. The row (b), (c), and (d) represent the comparisons of the COM trajectories between the ABWS system and the CW system at the unloading level of 30%, 50% and 70%, respectively. The final row, row e, shows the comparisons of the maximum displacements of the COM in three directions: sagittal direction (anterior-posterior), horizontal direction (lateral), and vertical direction. From Figure 5, we can observe that the COM trajectories are modified due to hard walking under abnormal walking conditions. In the horizontal and vertical direction, the peak values of the COM trajectories appear sooner than the normal walking condition. The same results can also be observed in walking under the ABWS and CW system at all unloading force levels. In terms of the maximum displacements of the COM, the significant differences are observed in normal walking conditions for all directions (p < 0.001). The maximum displacements of COM during walking under the abnormal condition were significantly different from the walking under ABW and CW system in both horizontal and vertical directions at all unloading force levels. In the sagittal direction, only at 30%, the significant difference of the abnormal walking versus unloading systems cannot be found (p = 0.19 for ABWS and 0.99 for the CW system). In comparison between the ABWS and CW system, we found that the maximum displacements of COM in sagittal direction are not significantly different. However, the significant differences are found in both horizontal and vertical directions (p = 0.045 at 30% unloading force in the horizontal direction, p < 0.001 in other cases).
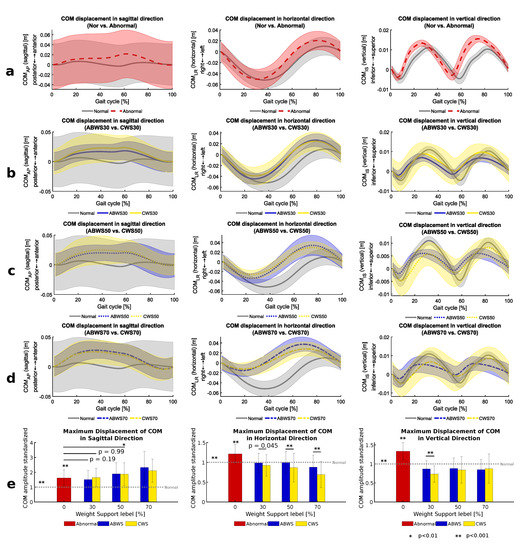
Figure 5.
Comparison of the COM trajectories: normal vs abnormal walking (a), ABWS and CW system unload 30% (b), ABWS and CW system unload 50% (c), ABWS and CW system unload 70% (d). (e) showed the comparison of the maximum displacement of COM in sagittal, horizontal and vertical direction. The significant value (p) was selected as 0.05. * and ** show that p is less than 0.01, and 0.001, respectively.
3.2. COP Movement
Figure 6 shows the COP trajectories of all walking conditions with the mean trajectories (the butterfly curves) and standard deviation bars in both sagittal and horizontal direction. Figure 7 shows the comparisons of the COP trajectories in the sagittal direction (a), and in the horizontal direction (b), and the comparisons of the maximum displacements of COP sagittal and horizontal directions (c). In Figure 6, the trajectory of the COP in the abnormal walking case is asymmetrical between the left side and right side. The improvement of the COP trajectories can be observed in the case of walking under the ABWS system at 30% and 50% weight support since the trajectories are more symmetry than the case of the CW system. The COP trajectories while walking under the CW system are deformed, and the range of COP movements decreases while increasing the weight support level.
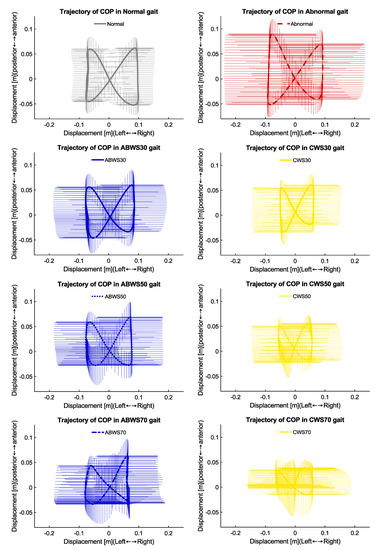
Figure 6.
The mean and the variance of COP trajectory of all subjects while walking under different conditions.
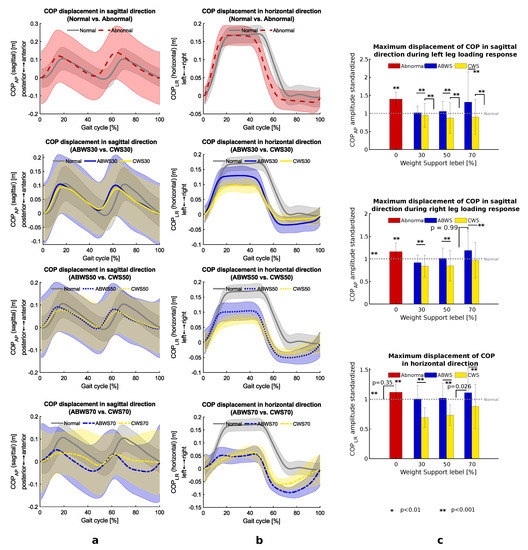
Figure 7.
The analyzing of the COP trajectories in sagittal, horizontal direction, column (a,b) respectively. Comparison of the maximum displacements of COP while left leg response, right leg response and horizontal direction present on column (c). The significant value (p) was selected as 0.05. * and ** show that p is less than 0.01, and 0.001, respectively.
The details analyzing of the COP trajectories are shown in Figure 7. The column (a) and (b) show the comparison of the COP trajectories in the sagittal and horizontal direction in the gait cycle, respectively. From top to bottom, column (a) and (b) show the comparison of the trajectories between the normal walking versus abnormal walking under ABWS and CW system at 30%, 50%, and 70% unloading force. In Figure 7, the COP trajectories in the sagittal plane show two peaks, which represented two times step for the left and right foot. The COP trajectories in horizontal direction commonly have two steady stages at bottom and top, which served for the left and right stance phase. The COP trajectory variances in terms of the abnormal walking condition and abnormal walking under the unload system (ABWS and CW system) are higher than the normal walking case. The shape of the COP trajectories was still maintained at 30% and 50% unloading force and more distorted at 70% of unloading force. The further quantities of the maximum displacement of COP are shown in the column (c). The COP maximal values in both the sagittal and horizontal direction of the abnormal walking condition significantly differed from the abnormal walking under the ABWS and CW system (p < 0.001). During the left leg loading response, no significant difference was found of the maximum values of COP of the ABWS system and the normal walking condition in the sagittal plane (p = 0.149 at 30% weight support, 0.656 at 50% weight support, and 0.670 at 70% weight support). In contrast, the maximum COP values of abnormal walking under the CW system significantly differ from the normal walking condition. The significant differences could also be observed of the maximum displacements of the COP between normal walking versus abnormal walking under the ABWS and CW system during the right leg loading response in both sagittal and horizontal direction (p < 0.001). However, the mean value of the maximum displacement of COP of the abnormal walking under the ABWS system was higher than the cases of using the CW system, and closer the normal walking case.
3.3. Margin of Stability
Figure 8a shows comparisons of the average MOS of all subjects varied in a gait cycle while walking at different conditions, from to bottom, normal walking and abnormal walking, abnormal walking under the ABWS, and CW system at 30%, 50%, and 70% weight support. The MOS of the abnormal walking kept the same shape as the normal walking; however, the MOS was more profound in the negative side. When comparing the ABWS and CW system at 30%, 50%, and 70% weight support, the MOS was mostly similar. Figure 8b presents the detailed comparison of the minimum at four gait events, the first double support, the single right support, the other single support, and the left single support phase. From The Figure 8b, the significant differences of the minimum MOS of the abnormal waking with the walking under ABWS and CW system were observed. The MOS of the abnormal waking was also significantly higher the normal walking at the first double support and the right single support phase (p < 0.001), smaller in the second single support phase (p < 0.001), and no significant difference at the left single support phase (p = 0.94). The statistical analysis indicated that MOS of the abnormal walking under the ABWS significantly differed from the CW case at the second double support phase and the left single support phase.
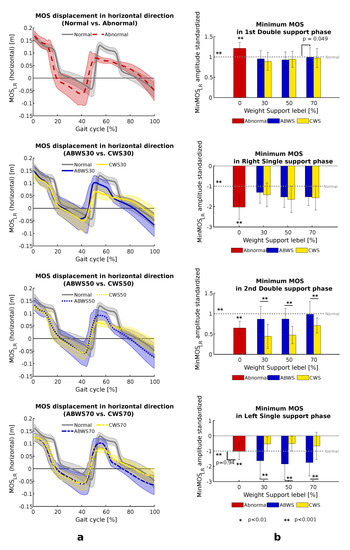
Figure 8.
The column (a) shows comparisons of the MOS in horizontal direction. The column (b) shows comparison of the minimum MOS at single support and double support among all walking conditions. The significant value (p) was selected as 0.05. * and ** show that p is less than 0.01, and 0.001, respectively.
3.4. The Range of Motion
Figure 9 shows the comparison of the range of motion of the hip, knee, and ankle angle. In Figure 9, row (a) shows the comparison of the hip, knee, and ankle joint movement between normal walking and abnormal walking. The row (b), (c), and (d) represent the comparison of ROM of the abnormal walking under the ABWS and CW system at 30%, 50%, and 70%, respectively. In Figure 9 we show that the angle pattern of the hip joint of the abnormal walking condition and walking under the ABWS and CW system still maintained the same shape as the normal walking; however, the knee and ankle angles were distorted due to the restriction of the right knee joint and 3 kg-weight on the right ankle angle.
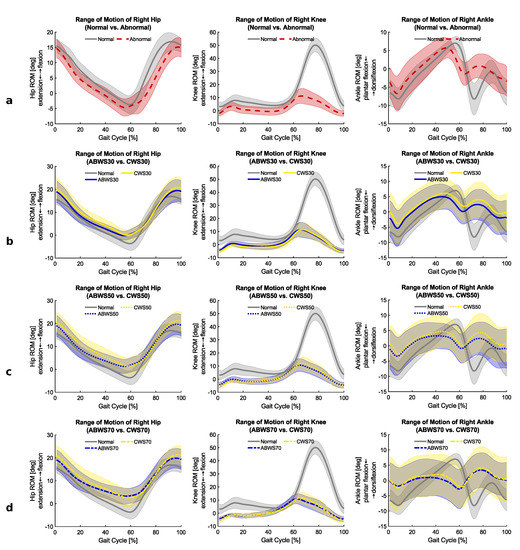
Figure 9.
The comparison of the ROS of the hip, knee and ankle joint on the right side. (a) represents the comparison of the hip, knee and ankle joint movement between normal walking and abnormal walking. (b–d) represent the comparison of ROM of the abnormal walking under the ABWS and CW system at 30%, 50% and 70%, respectively.
3.5. The Stride Length, Step Width, and Step Length
Table 1 represents the comparison of the standardized values of the stride length, the step width, the step length of the left and right sides. When comparing the stride length, the statistical analysis indicated that the abnormal walking condition significantly differed from the normal walking, walking under the ABWS system at all unloading force levels, and the walking under the CW system at 70% (p < 0.001). When the comparison between the walking under ABWS and CW systems, the significant differences were also observed (p < 0.01 at 30% and 70% unloading levels, p < 0.001 at 50% unloading level). The stride lengths of the walking under the ABWS system 50% and 70% unloading levels were not significantly different from the normal walking case (p = 0.958, and p = 0.975 at 50% and 70% unloading levels respectively). In contrast, the stride lengths while walking under the CW system at 30% and 50% unloading levels did not significantly differ from the abnormal walking case (p = 0.814, and p = 0.094 at 30% and 50% unloading levels respectively). From Table 1, the statistical analysis indicated that the step width of the abnormal walking condition significantly differed from all step widths of the other walking conditions (p = 0.027 when compared to normal walking, less than 0.001 when comparing with others). The significant differences were also found when comparing the normal walking case with walking both under the ABWS and CW system at all weight support levels (p < 0.001). Furthermore, significant differences were also seen in the comparison of the step width between walking under the ABWS and CW system at all unloading levels. In terms of the step length of the left side (the normal side), there was no significant difference from the abnormal walking and normal walking (p = 0.77). The step length of the left side in case of abnormal walking was significantly smaller than the ABWS and CW systems (p < 0.001) excepted at the 30% unloading level of the ABWS system. When comparing the step length of the right side (the restricted side), the abnormal walking showed the significant difference from the normal walking case (p < 0.001)and all other conditions (p < 0.001 for ABWS system at all unloading levels, and p < 0.05 for CW system). Comparison of the right step length between the ABWS and CW system, the significant differences were found at 30% and 70% of unloading force (p < 0.05).

Table 1.
The comparison of the standardized values of stride length, step width, the step length of the left and right side. The data of 30s walking in each walking condition of each subject, which was equivalent around 36 gait cycles, was selected. The number of gait cycles in each walking condition is 367 gait cycles for all subjects. The significance level was selected at 0.05.
4. Discussion
In this study, we aimed to examine and evaluate the effects of the ABWS and CW systems on an abnormal gait that looked like a hemiplegic patient. The abnormal gait was generated by restriction movement of the knee joint and 3 kg-weight on the ankle. Previous research has been shown the influence of the BWS system on healthy subjects, which only represented the changes of gait parameters of the healthy person during ambulation [23,39,40,41]. Furthermore, the gait parameters were impacted by many external factors while implementation of the BWS in clinical of hemiplegic, stroke, and spinal cord injury patients such as assistance device, the support of the therapist, etc [15,19,21,22,28,29,35,38]. Evaluation of the changes in the gait parameter during abnormal gait under the BWS system would be necessary and provide useful information for clinical practice.
The hypothesis assumed that the BWS system plays a role as a clinical intervention such that the BWS system would influence the gait patterns and parameters during rehabilitation. The assistance of the stepping movement by the BWS system, which changes the gait patterns and parameters of the abnormal walking, may alter and activate the sensory feedback, therefore, improve the ambulation functionality [20,35,37]. Our results confirmed that the BWS system would strongly alter the abnormal walking gait pattern and could play an important role in the clinical implementation of gait rehabilitation of the lower extremity. The ABWS and CW system generally cannot correct the extreme abnormal gait since the significant differences from the normal walking condition can be observed. However, the modification and improvement of the abnormal walking under the ABWS and CW system can be found. The results in Figure 5 and Figure 7 indicated that the ABWS system improved the gait parameters of abnormal walking in terms of COM, COP. The improvement was significant in the horizontal direction of COM and both sagittal and horizontal of COP. The CW system also improved the COM in the horizontal direction; however, it did not provide good result in term of COP. These improvements of stride length and the right step length can also be observed while using the ABWS system. These results agree with the previous research that the improvements in gait training could be achieved during weight supported by the BWS system [15,22,26,28,29,38].
When comparing gait parameters between the ABWS system and the CW, the ABWS system provided better behavior in most cases. Currently, only a few studies conducted an experimental comparison between the active and passive unloading system [42,48]. In this present study, the maximum displacements of the COM in the horizontal direction of the ABWS were significantly higher and closer to the normal walking condition, as shown in Figure 5e. In Figure 6, The mean COP trajectory shapes of the walking under the ABWS system were more symmetry, the COP trajectories of walking under the CW system, contrarily, were more distorted and could not replicate the COP trajectory of the normal walking case. The quantifies of the maximum displacements of the COP while walking under the ABWS system was better and closer to the normal case. The CW system even provided the worse results of the maximum displacement of the COP during the right leg loading response and in the horizontal direction. This result confirmed the previous study such that the unloading force of the ABWS system with the COP tracking could provide better gait trajectories in comparison with the case of using the CW system with a constant counterweight [42]. These results could be explained that the lateral force in the pendulum effect by using the CW system pulled subject COM to the vertical center axis [23,49]. Consequently, the COP in the horizontal direction would distort while walking under the CW system, especially at the high level of unloading force (see Figure 6). In contrast, the better results of the COM and COP while waking under the ABWS system suggest that the lateral force in the pendulum effect was reduced. These results would be meaningful in implementing the ABWS system with higher unloading force in gait training and indicated that the modulated body weight unloading system type on the treadmill shows potential advantages in clinical implementation of gait training when comparing with the passive unmodulated body weight unloading.
In Figure 9, the lost peak can be seen in the range of motion of the knee joint for the abnormal walking condition and abnormal walking under both the ABWS and CW system at all unloading weight supported levels. The ankle angle patterns of all abnormal walking conditions were distorted and differed from the normal walking condition. The ranges of motion of the abnormal walking condition showed the analog shapes of the gait pattern of hemiplegia which were reported in previous studies [50,51,52]. These results suggested that the successful reproduction of the gait pattern of hemiplegia as the abnormal walking condition. One can see that the improvement in terms of ROM was not observed in this present study. The reason is that the experiment was carried out in the difficult conditions of abnormal walking with the rigid fixation of the right knee joint and the 3 kg-weight on the ankle joint. In Figure 8, the improvement of the MOS while walking under the ABWS system can be seen during the first double support phase, right single support phase, and the second double support phase. The CW system only improved the MOS at the first double support and the right single support phases. One should notice that the second double support phase is the transition phase from the abnormal side to the normal side. Therefore, the increment in the MOS while walking under the ABWS would be meaningful and help the subject walking more stable than in case of using the CW system. The negative MOS happened at the end of the single support phase, which represented for the unstable stage during dynamic walking, and the COM movement switched from the left to right and vice verse [47]. Hajime Ohtsu et al. indicated that the higher negative MOS might representation for the fast gait during dynamic walking [47]. The higher value of the negative MOS while walking under the ABWS may suggest a sign of the faster walking speed in comparison with the case of the CW system.
In Table 1, the ABWS improved the stride length, step width, and right step length. The no significant difference of stride length and step length on the right between abnormal walking under the ABWS system and normal walking at 30% and 70% unloading levels indicated the successful correction of the gait kinematic. The CW system only improved the stride length and the right step length; however, the successful correction gait kinematic was not be found. When considering the stride length, step width, and step length, the ABWS system again showed better behavior in comparison with that CW system.
The gait training process for the incomplete patient could be executed in the early stage and undergone many periods depending on the situation of the patient. Jørgensen HS et al. indicated that a valid prognosis of walking function in patients with the leg paresis on admission could be made in 3 weeks, and the recovery of walking function mainly occurs within the first 11 weeks after stroke; patients who experience functional recovery after that time are in fact few [1]. In the situation of the early stage of the gait training procedure, the high level of weight support would be necessary due to the frailty of the ability bearing the patient’s full weight. Previous studies mostly implemented the unloading level up to 40% for the healthy subject and walking impaired patient [15,19,22,36,39]. Only a few studies investigated the effect of unloading force on gait at a high level (higher than 50% subject weight) [23,36]. The possible reason for the uncommon implementation of high unloading force levels would be the distortion and significant changes in the gait pattern. In this study, the high distortion of the COP trajectory of the abnormal walking under the unloading system at the high weight supported level confirmed this assumption. Nevertheless, the improvement of the gait patterns and kinematic parameters of the abnormal walking under the ABWS system suggested the potential implementation and the high performance of the modulated active BWS system in clinical practice.
5. Conclusions
In this research, the abnormal gait, which was generated by the restricted knee joint movement and 3 kg-weight on ankle joint, would be like a pretend hemiplegic patient. The implement of the BWS system on the abnormal gait indicated the difficulty to correct gait parameters of the extreme abnormal walking. However, the improvement of the BWS system on the abnormal gait suggested the high potential application of the BWS system as a clinical intervention to recover the locomotion function. A comparison of the ABWS system and the CW system stand out the higher performance of the ABWS system since it showed better behavior than the CW system. In future work, the authors will focus on analyzing the effects of the BWS system in terms of kinetic and energy consumptions. Furthermore, implementation of the ABWS and CW system on patients such as hemiplegia, patients after spinal cord injury will be considered to observe the changes of the gait parameters and improve the ambulation functionality of patients.
Author Contributions
For research articles with several authors. V.-T.T. conceived the methodology prepare and conducted the experiment, he also analyzed data and wrote the paper. K.S. conducted the experiment and analyzed data. S.-i.Y. led the research efforts and led the preparation of this paper. All authors have read and agreed to the published version of the manuscript.
Funding
This research received funding by Kakenhi grant for Early-Career Scientists:18K18423.
Conflicts of Interest
The authors declare no conflict of interest.
References
- Jørgensen, H.S.; Nakayama, H.; Raaschou, H.O.; Olsen, T.S. Recovery of walking function in stroke patients: The Copenhagen Stroke Study. Arch. Phys. Med. Rehabil. 1995, 76, 27–32. [Google Scholar] [CrossRef]
- Katan, M.; Luft, A. Global Burden of Stroke. Semin. Neurol. 2018, 38, 208–211. [Google Scholar] [CrossRef]
- National Spinal Cord Injury Statistical Center at UAB. Spinal Cord Injury: Facts and Figures at a Glance. Available online: https://www.nscisc.uab.edu/ (accessed on 26 January 2020).
- Tusji, S.; Fujishama, H. Paraplegias, Clinical Statisitcs; Kyushu Rosai Hospital: Fukuoka, Japan, 1975. [Google Scholar]
- Gehrig, R.; Michaelis, L.S. Statistics of acute paraplegia and tetraplegia on a national scale. Switzerland 1960–1967. Paraplegia 1986, 6, 93–95. [Google Scholar]
- Minaire, P.; Castanier, M.; Girard, R.; Berard, E.; Deidier, C.; Bourret, J. Epidemiology of spinal-cord injury in Rhone-Alpes region. France, 1970–1975. Paraplegia 1978, 16, 76–87. [Google Scholar]
- Martins, F.; Freitas, F.; Martins, L.; Dartigues, J.F.; Barat, M. Spinal cord injuries—epidemiology in Portugal’s central region. Spinal Cord 1998, 35, 574–578. [Google Scholar] [CrossRef][Green Version]
- Benjamin, E.J.; Muntner, P.; Alonso, A.; Bittencourt, M.S.; Callaway, C.W.; Carson, A.P.; Chamberlain, A.M.; Chang, A.R.; Cheng, S.; Das, S.R.; et al. Heart Disease and Stroke Statistics—2019 Update: A Report From the American Heart Association. AHA J. 2019, 139, E56–E528. [Google Scholar] [CrossRef]
- Barbeau, H.; Ladouceur, M.; Norman, K.E.; Pépin, A.; Leroux, A. Walking after spinal cord injury: Evaluation, treatment, and functional recovery. Arch. Phys. Med. Rehabil. 1999, 80, 225–235. [Google Scholar] [CrossRef]
- Subbarao, J.V. Walking after spinal cord injury. Goal or wish? West. J. Med. 1991, 154, 612–614. [Google Scholar]
- Hasegawa, T.; Uchiyama, Y.; Uemura, K.; Harada, Y.; Sugiyama, M.; Tanaka, H. Physical impairment and walking function required for community ambulation in patients with cervical incomplete spinal cord injury. Spinal Cord 2014, 52, 396–399. [Google Scholar] [CrossRef]
- Menon, N.; Gupta, A.; Khanna, M.; Taly, A.B. Ambulation following spinal cord injury and its correlates. Ann. Indian Acad. Neurol. 2015, 18, 167–170. [Google Scholar]
- Noonan, V.; Fallah, N.; Park, S.; Dumont, F.; Leblond, J.; Cobb, J.; Noreau, L. Health care utilization in persons with traumatic spinal cord injury: The importance of multimorbidity and the impact on patient outcomes. Top. Spinal Cord Inj. Rehabil. 2014, 20, 289–301. [Google Scholar] [CrossRef] [PubMed]
- Combs, S.A.; Dugan, E.L.; Ozimek, E.N.; Curtis, A.B. Effects of body-weight supported treadmill training on kinetic symmetry in persons with chronic stroke. Clin. Biomech. 2012, 27, 887–892. [Google Scholar] [CrossRef]
- Sousa, C.O.; Barela, J.A.; Prado-Medeiros, C.L.; Salvini, T.F.; Barela, A.M. The use of body weight support on ground level: An alternative strategy for gait training of individuals with stroke. J. Neuroeng. Rehabil. 2009, 6, 43. [Google Scholar] [CrossRef] [PubMed]
- Lovely, R.G.; Gregor, R.J.; Roy, R.R.; Edgerton, V.R. Effects of training on the recovery of full-weight-bearing stepping in the adult spinal cat. Exp. Neurol. 1986, 92, 421–435. [Google Scholar] [CrossRef]
- Barbeau, H.; Rossignol, S. Recovery of locomotion after chronic spinalization in the adult cat. Brain Res. 1987, 412, 84–95. [Google Scholar] [CrossRef]
- Finch, L.; Barbeau, H.; Arsenault, B. Influence of body weight support on normal human gait: Development of a gait retraining strategy. Phys. Ther. 1991, 71, 842–855. [Google Scholar] [CrossRef]
- Visintin, M.; Barbeau, H.; Korner-Bitensky, N.; Mayo, N.E. A new approach to retrain gait in stroke patients through body weight support and treadmill stimulation. Stroke 1998, 29, 1122–1128. [Google Scholar] [CrossRef]
- Dietz, V. Body weight supported gait training: From laboratory to clinical setting. Brain Res. Bull. 2009, 78, I–VI. [Google Scholar] [CrossRef]
- Hesse, S.; Bertelt, C.; Jahnke, M.T.; Schaffrin, A.; Baake, P.; Malezic, M.; Mauritz, K.H. Treadmill training with partial body weight support compared with physiotherapy in nonambulatory hemiparetic patients. Stroke 1995, 26, 976–981. [Google Scholar] [CrossRef]
- Barbeau, H.; Visintin, M. Optimal outcomes obtained with body-weight support combined with treadmill training in stroke subjects. Arch. Phys. Med. Rehabil. 2003, 84, 1458–1465. [Google Scholar] [CrossRef]
- Dragunas, A.C.; Gordon, K.E. Body weight support impacts lateral stability during treadmill walking. J. Biomech. 2016, 49, 2662–2668. [Google Scholar] [CrossRef] [PubMed]
- Gama, G.L.; Celestino, M.L.; Barela, J.A.; Barela, A.M.F. Gait initiation and partial body weight unloading for functional improvement in post-stroke individuals. Gait Posture 2019, 68, 305–310. [Google Scholar] [CrossRef] [PubMed]
- Miller, E.W.; Quinn, M.E.; Seddon, P.G. Body weight support treadmill and overground ambulation training for two patients with chronic disability secondary to stroke. Phys. Ther. 2002, 82, 53–61. [Google Scholar] [CrossRef] [PubMed]
- Sousa, C.O.; Barela, J.A.; Prado-Medeiros, C.L.; Salvini, T.F.; Barela, A.M. Gait training with partial body weight support during overground walking for individuals with chronic stroke: A pilot study. J. Neuroeng. Rehabil. 2011, 8, 48. [Google Scholar] [CrossRef] [PubMed]
- Schindl, M.R.; Forstner, C.; Kern, H.; Hesse, S. Treadmill training with partial body weight support in nonambulatory patients with cerebral palsy. Arch. Phys. Med. Rehabil. 2000, 81, 301–306. [Google Scholar] [CrossRef]
- Wernig, A.; Müller, S. Laufband locomotion with body weight support improved walking in persons with severe spinal cord injuries. Spinal Cord 1992, 30, 229–238. [Google Scholar] [CrossRef]
- Werner, C.; Von Frankenberg, S.; Treig, T.; Konrad, M.; Hesse, S. Treadmill training with partial body weight support and an electromechanical gait trainer for restoration of gait in subacute stroke patients: A randomized crossover study. Stroke 2002, 33, 2895–2901. [Google Scholar] [CrossRef]
- Colombo, G.; Joerg, M.; Schreier, R.; Dietz, V. Treadmill training of paraplegic patients using a robotic orthosis. J. Rehabil. Res. Dev. 2000, 37, 693–700. [Google Scholar]
- Hornby, T.G.; Zemon, D.H.; Campbell, D. Robotic-assisted, body-weight-supported treadmill training in individuals following motor incomplete spinal cord injury. Phys Ther. 2005, 85, 52–66. [Google Scholar] [CrossRef]
- Beyl, P.; Knaepen, K.; Duerinck, S.; Van Damme, M.; Vanderborght, B.; Meeusen, R.; Lefeber, D. Safe and compliant guidance by a powered knee exoskeleton for robot-assisted rehabilitation of gait. Adv. Robot. 2011, 25, 513–535. [Google Scholar] [CrossRef]
- Srivastava, S.; Kao, P.C.; Kim, S.H.; Stegall, P.; Zanotto, D.; Higginson, J.S.; Agrawal, S.K.; Scholz, J.P. Assist-as-needed robot-aided gait training improves walking function in individuals following stroke. IEEE Trans. Neural Syst. Rehabil. Eng. 2014, 23, 956–963. [Google Scholar] [CrossRef] [PubMed]
- Fisher, S.; Lucas, L.; Thrasher, T.A. Robot-assisted gait training for patients with hemiparesis due to stroke. Top. Stroke Rehabil. 2011, 18, 269–276. [Google Scholar] [CrossRef]
- Smith, A.C.; Knikou, M. A review on locomotor training after spinal cord injury: Reorganization of spinal neuronal circuits and recovery of motor function. Neural Plast. 2016, 2016, 1216258. [Google Scholar] [CrossRef] [PubMed]
- Apte, S.; Plooij, M.; Vallery, H. Influence of body weight unloading on human gait characteristics: A systematic review. J. Neuroeng. Rehabil. 2018, 15, 53. [Google Scholar] [CrossRef] [PubMed]
- Kleim, J.A.; Jones, T.A. Principles of experience-dependent neural plasticity: Implications for rehabilitation after brain damage. J. Speech Lang. Hear. Res. 2008, 51, 225–239. [Google Scholar] [CrossRef]
- Field-Fote, E.C.; Tepavac, D. Improved intralimb coordination in people with incomplete spinal cord injury following training with body weight support and electrical stimulation. Phys. Ther. 2002, 82, 707–715. [Google Scholar] [CrossRef]
- Aaslund, M.K.; Moe-Nilssen, R. Treadmill walking with body weight support effect of treadmill, harness and body weight support systems. Gait Posture 2008, 28, 303–308. [Google Scholar] [CrossRef]
- Hwang, S.; Jeon, H.S.; Kwon, O.Y.; Yi, C.H. The effects of body weight on the soleus H-reflex modulation during standing. J. Electromyogr. Kinesiol. 2011, 21, 445–449. [Google Scholar] [CrossRef]
- You, Y.L.; Lee, S.Y.; Tsai, Y.J.; Lin, C.F.; Kuo, L.C.; Su, F.C. Effects of body weight support and pedal stance width on joint loading during pinnacle trainer exercise. Gait Posture 2019, 74, 45–52. [Google Scholar] [CrossRef]
- Van Thuc, T.; Yamamoto, S.-I. Development of a Body Weight Support System Using Pneumatic Muscle Actuators: Controlling and Validation. Adv. Mech. Eng. 2016, 8. [Google Scholar] [CrossRef]
- Furukawa, J.; Noda, T.; Teramae, T.; Morimoto, J. An EMG-Driven Weight Support System With Pneumatic Artificial Muscles. IEEE Syst. J. 2016, 10, 1026–1034. [Google Scholar] [CrossRef]
- Winter, D.A. Biomechanics and Motor Control of Human Movement; John Wiley & Sons: Hoboken, NJ, USA, 2009; pp. 101–149. [Google Scholar]
- Hof, A.L.; Gazendam, M.G.; Sinke, W.E. The condition for dynamic stability. J. Biomech. 2005, 38, 1–8. [Google Scholar] [CrossRef] [PubMed]
- Hof, A.L. The ’extrapolated center of mass’ concept suggests a simple control of balance in walking. Hum. Mov. Sci. 2008, 27, 112–125. [Google Scholar] [CrossRef] [PubMed]
- Ohtsu, H.; Yoshida, S.; Minamisawa, T.; Takahashi, T.; Yomogida, S.I.; Kanzaki, H. Investigation of balance strategy over gait cycle based on margin of stability. J. Biomech. 2019, 95. [Google Scholar] [CrossRef]
- Frey, M.; Colombo, G.; Vaglio, M.; Bucher, R.; Jorg, M.; Riener, R. A Novel Mechatronic Body Weight Support System. IEEE Trans. Neural Syst. Rehabil. Eng. 2006, 14, 311–321. [Google Scholar] [CrossRef]
- Pennycott, A.; Wyss, D.; Vallery, H.; Riener, R. Effects of added inertia and body weight support on lateral balance control during walking. In Proceedings of the 2011 IEEE International Conference on Rehabilitation Robotics, Zurich, Switzerland, 29 June–1 July 2011; pp. 1–5. [Google Scholar] [CrossRef]
- Winters, T.F.; Gage, J.R.; Hicks, R. Gait patterns in spastic hemiplegia in children and young adults. J. Bone Jt. Surg. Am. 1987, 69, 437–441. [Google Scholar]
- Olney, S.J.; Griffin, M.P.; McBride, I.D. Temporal, kinematic, and kinetic variables related to gait speed in subjects with hemiplegia: A regression approach. Phys. Ther. 1994, 74, 872–885. [Google Scholar] [CrossRef]
- Olney, S.J.; Richards, C. Hemiparetic gait following stroke. Part I: Characteristics. Gait Posture 1996, 4, 136–148. [Google Scholar] [CrossRef]
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).