Three-Dimensional Analysis of Root Anatomy and Root Canal Curvature in Mandibular Incisors Using Micro-Computed Tomography with Novel Software


 , ,
, , 

Abstract
1. Introduction
2. Materials and Methods
2.1. Image Analysis
2.2. Statistical Analysis
3. Results
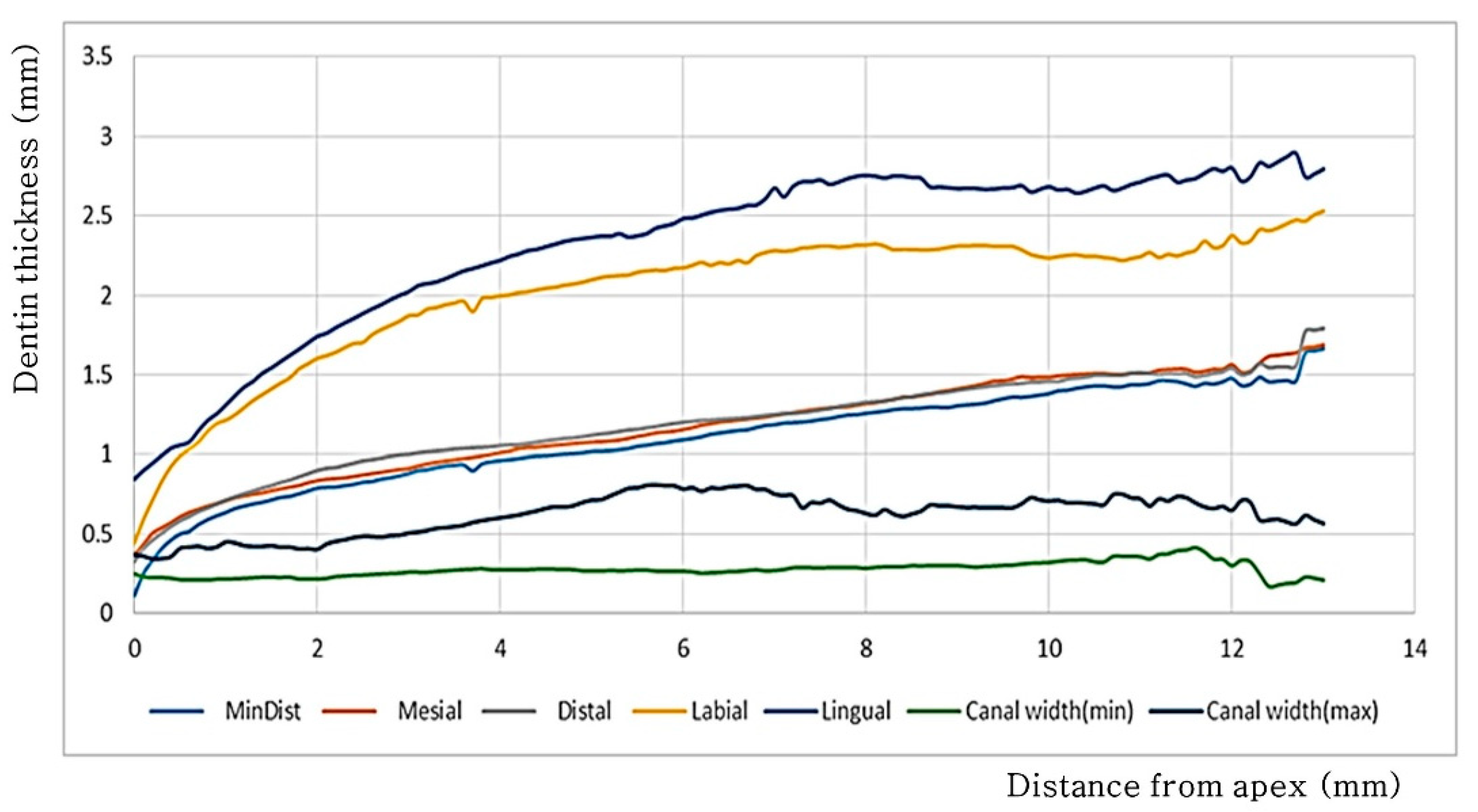
3.1. Dentin Thickness
3.2. Measurement of the Thinnest Dentin
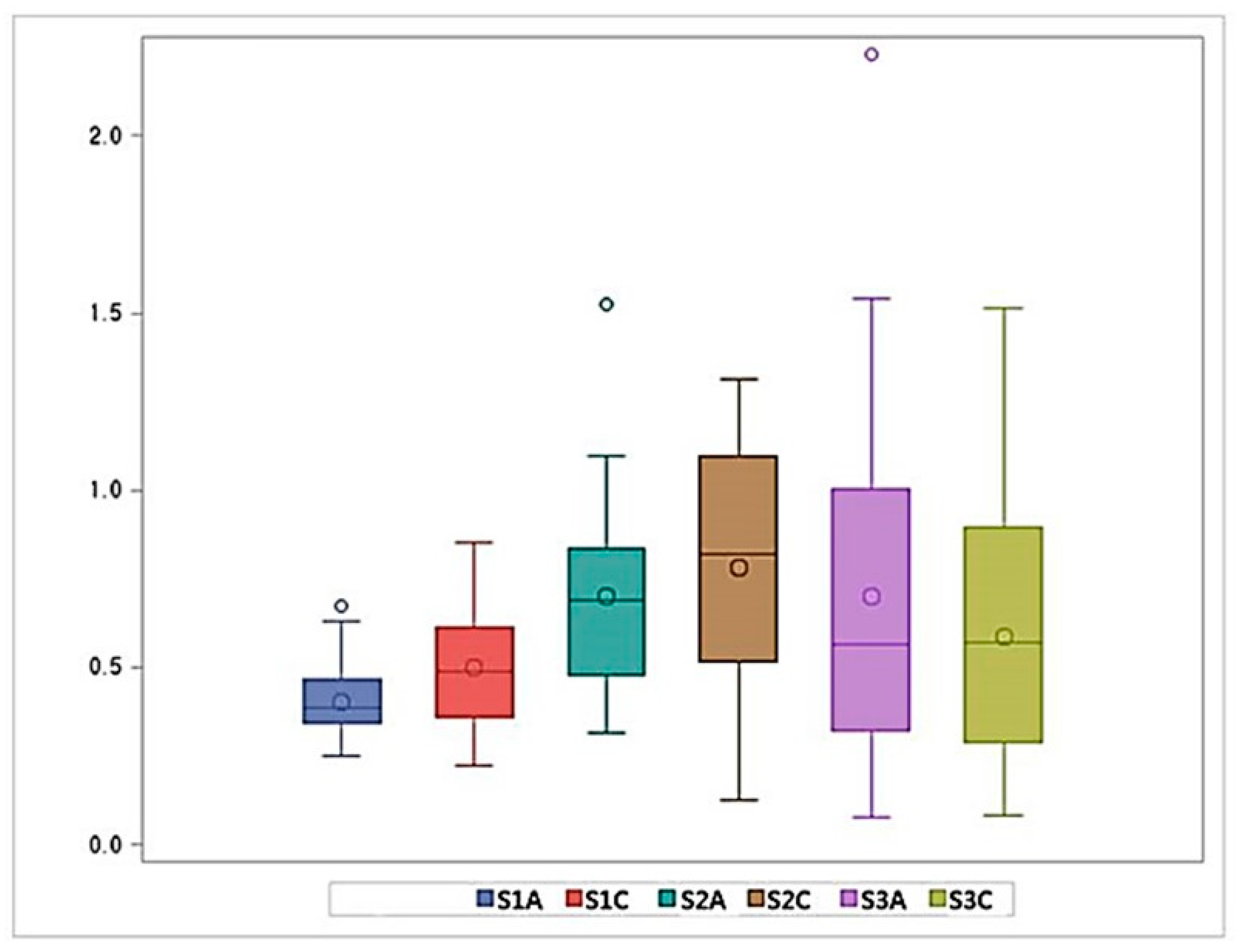
3.3. Canal Width
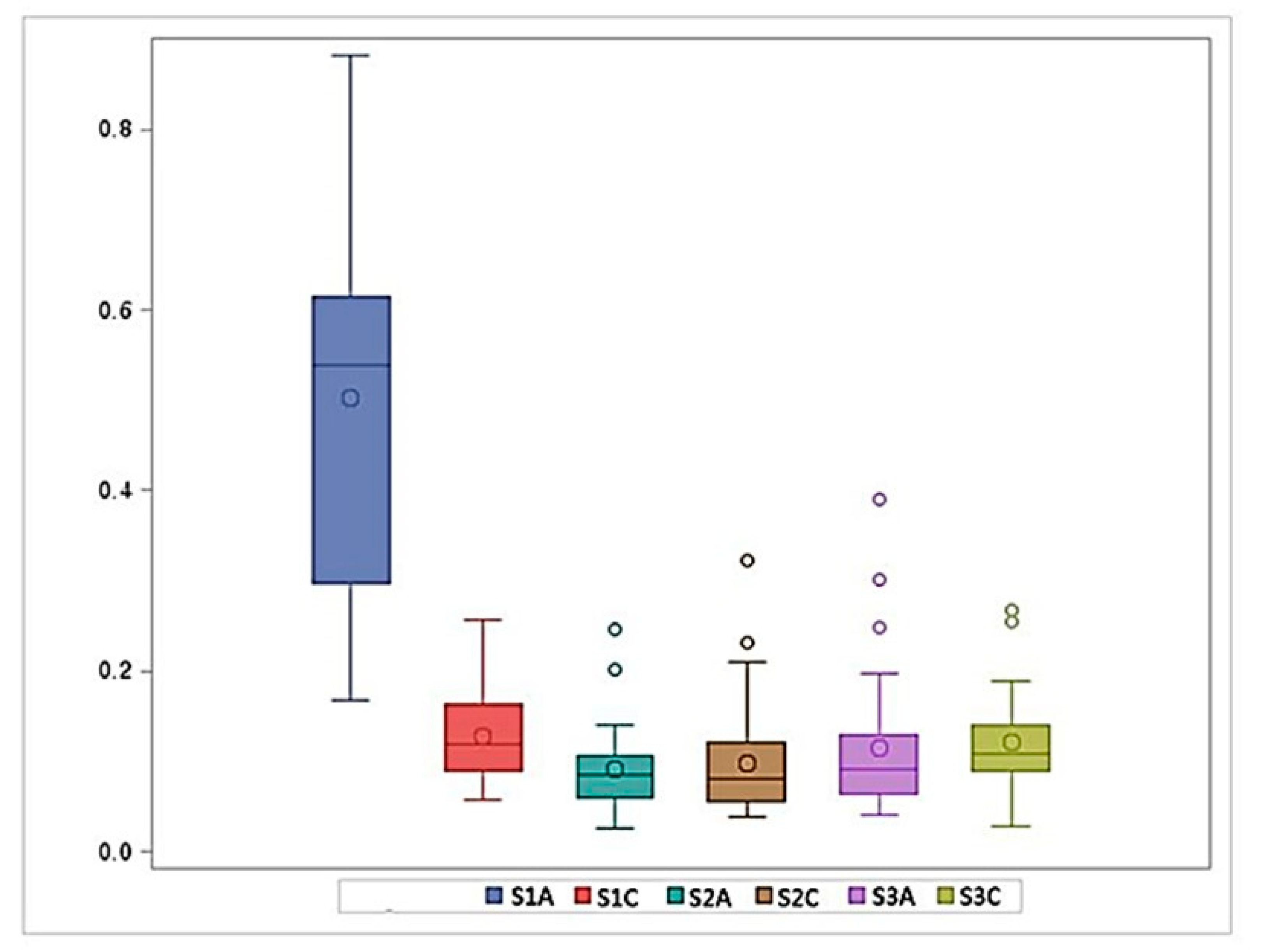
3.4. Canal Curvature
4. Discussion
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Leoni, G.B.; Versiani, M.A.; Pecora, J.D.; Damiao de Sousa-Neto, M. Micro-computed tomographic analysis of the root canal morphology of mandibular incisors. J. Endod. 2014, 40, 710–716. [Google Scholar] [CrossRef] [PubMed]
- Liu, J.; Luo, J.; Dou, L.; Yang, D. CBCT study of root and canal morphology of permanent mandibular incisors in a Chinese population. Acta Odontol. Scand. 2014, 72, 26–30. [Google Scholar] [CrossRef] [PubMed]
- Hargreaves, K.; Cohen, S. Pathways of the Pulp, 10th ed.; Mosby: Maryland Heights, MO, USA, 2011. [Google Scholar]
- Chang, S.W.; Lee, J.K.; Lee, Y.; Kum, K.Y. In-depth morphological study of mesiobuccal root canal systems in maxillary first molars: Review. Restor. Dent. Endod. 2013, 38, 2–10. [Google Scholar] [CrossRef] [PubMed]
- Lee, J.K.; Ha, B.H.; Choi, J.H.; Heo, S.M.; Perinpanayagam, H. Quantitative three-dimensional analysis of root canal curvature in maxillary first molars using micro-computed tomography. J. Endod. 2006, 32, 941–945. [Google Scholar] [CrossRef] [PubMed]
- Kim, Y.; Perinpanayagam, H.; Lee, J.K.; Yoo, Y.J.; Oh, S.; Gu, Y.; Lee, S.P.; Chang, S.W.; Lee, W.; Baek, S.H.; et al. Comparison of mandibular first molar mesial root canal morphology using micro-computed tomography and clearing technique. Acta Odontol. Scand. 2015, 73, 427–432. [Google Scholar] [CrossRef] [PubMed]
- Lee, J.K.; Yoo, Y.J.; Perinpanayagam, H.; Ha, B.H.; Lim, S.M.; Oh, S.R.; Gu, Y.; Chang, S.W.; Zhu, Q.; Kum, K.Y. Three-dimensional modelling and concurrent measurements of root anatomy in mandibular first molar mesial roots using micro-computed tomography. Int. Endod. J. 2015, 48, 380–389. [Google Scholar] [CrossRef] [PubMed]
- Park, P.S.; Kim, K.D.; Perinpanayagam, H.; Lee, J.K.; Chang, S.W.; Chung, S.H.; Kaufman, B.; Zhu, Q.; Safavi, K.E.; Kum, K.Y. Three-dimensional analysis of root canal curvature and direction of maxillary lateral incisors by using cone-beam computed tomography. J. Endod. 2013, 39, 1124–1129. [Google Scholar] [CrossRef] [PubMed]
- Park, J.W.; Lee, J.K.; Ha, B.H.; Choi, J.H.; Perinpanayagam, H. Three-dimensional analysis of maxillary first molar mesiobuccal root canal configuration and curvature using micro-computed tomography. Oral Surg. Oral Med. Oral Pathol. Oral Radiol. Endod. 2009, 108, 437–442. [Google Scholar] [CrossRef] [PubMed]
- Pineda, F.; Kuttler, Y. Mesiodistal and buccolingual roentgenographic investigation of 7,275 root canals. Oral Surg. Oral Med. Oral Pathol. 1972, 33, 101–110. [Google Scholar] [CrossRef]
- Madeira, M.C.; Hetem, S. Incidence of bifurcations in mandibular incisors. Oral Surg. Oral Med. Oral Pathol. 1973, 36, 589–591. [Google Scholar] [CrossRef]
- Vertucci, F.J. Root canal anatomy of the human permanent teeth. Oral Surg. Oral Med. Oral Pathol. 1984, 58, 589–599. [Google Scholar] [CrossRef]
- Caliskan, M.K.; Pehlivan, Y.; Sepetcioglu, F.; Turkun, M.; Tuncer, S.S. Root canal morphology of human permanent teeth in a Turkish population. J. Endod. 1995, 21, 200–204. [Google Scholar] [CrossRef]
- Milanezi de Almeida, M.; Bernardineli, N.; Ordinola-Zapata, R.; Villas-Boas, M.H.; Amoroso-Silva, P.A.; Brandao, C.G.; Guimaraes, B.M.; Gomes de Moraes, I.; Hungaro-Duarte, M.A. Micro-computed tomography analysis of the root canal anatomy and prevalence of oval canals in mandibular incisors. J. Endod. 2013, 39, 1529–1533. [Google Scholar] [CrossRef] [PubMed]
- Tasdemir, T.; Aydemir, H.; Inan, U.; Unal, O. Canal preparation with Hero 642 rotary Ni-Ti instruments compared with stainless steel hand K-file assessed using computed tomography. Int. Endod. J. 2005, 38, 402–408. [Google Scholar] [CrossRef] [PubMed]
- Moore, J.; Fitz-Walter, P.; Parashos, P. A micro-computed tomographic evaluation of apical root canal preparation using three instrumentation techniques. Int. Endod. J. 2009, 42, 1057–1064. [Google Scholar] [CrossRef] [PubMed]
- Gergi, R.; Rjeily, J.A.; Sader, J.; Naaman, A. Comparison of canal transportation and centering ability of twisted files, Pathfile-ProTaper system, and stainless steel hand K-files by using computed tomography. J. Endod. 2010, 36, 904–907. [Google Scholar] [CrossRef] [PubMed]
- Paque, F.; Zehnder, M.; De-Deus, G. Microtomography-based comparison of reciprocating single-file F2 ProTaper technique versus rotary full sequence. J. Endod. 2011, 37, 1394–1397. [Google Scholar] [CrossRef] [PubMed]
- Rhodes, J.S.; Ford, T.R.; Lynch, J.A.; Liepins, P.J.; Curtis, R.V. Micro-computed tomography: A new tool for experimental endodontology. Int. Endod. J. 1999, 32, 165–170. [Google Scholar] [CrossRef] [PubMed]
- Gu, Y.; Lee, J.K.; Spangberg, L.S.; Lee, Y.; Park, C.M.; Seo, D.G.; Chang, S.W.; Hur, M.S.; Hong, S.T.; Kum, K.Y. Minimum-intensity projection for in-depth morphology study of mesiobuccal root. Oral Surg. Oral Med. Oral Pathol. Oral Radiol. Endod. 2011, 112, 671–677. [Google Scholar] [CrossRef] [PubMed]












{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| S1A | S1C | S2A | S2C | S3A | S3C | |
|---|---|---|---|---|---|---|
| Thinnest dentin thickness (mm) | 0.56 ± 0.12 | 0.86 ± 0.13 | 1.00 ± 0.15 | 1.14 ± 0.14 | 1.30 ± 0.15 | 1.41 ± 0.21 |
| Mesial dentin thickness (mm) | 0.66 ± 0.14 | 0.91 ± 0.14 | 1.07 ± 0.17 | 1.20 ± 0.16 | 1.37 ± 0.16 | 1.50 ± 0.19 |
| Distal dentin thickness (mm) | 0.66 ± 0.12 | 0.98 ± 0.14 | 1.11 ± 0.13 | 1.23 ± 0.13 | 1.36 ± 0.13 | 1.50 ± 0.16 |
| Labial dentin thickness (mm) | 1.13 ± 0.23 | 1.81 ± 0.22 | 2.06 ± 0.23 | 2.22 ± 0.24 | 2.29 ± 0.23 | 2.28 ± 0.23 |
| Lingual dentin thickness (mm) | 1.27 ± 0.29 | 1.97 ± 0.28 | 2.32 ± 0.36 | 2.57 ± 0.44 | 2.68 ± 0.34 | 2.71 ± 0.23 |
| Narrowest canal width(mm) | 0.22 ± 0.05 | 0.25 ± 0.05 | 0.27 ± 0.08 | 0.28 ± 0.13 | 0.31 ± 0.15 | 0.30 ± 0.16 |
| Widest canal width (mm) | 0.40 ± 0.11 | 0.50 ± 0.17 | 0.70 ± 0.27 | 0.78 ± 0.36 | 0.70 ± 0.50 | 0.59 ± 0.38 |
| Canal Curvature (mm−1) | 0.50 ± 0.22 | 0.13 ± 0.05 | 0.09 ± 0.05 | 0.10 ± 0.07 | 0.11 ± 0.08 | 0.12 ± 0.06 |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Lee, J.; Lee, S.-H.; Hong, J.-R.; Kum, K.-Y.; Oh, S.; Al-Ghamdi, A.S.; Al-Ghamdi, F.A.; Mandorah, A.O.; Jang, J.-H.; Chang, S.W. Three-Dimensional Analysis of Root Anatomy and Root Canal Curvature in Mandibular Incisors Using Micro-Computed Tomography with Novel Software. Appl. Sci. 2020, 10, 4385. https://doi.org/10.3390/app10124385
Lee J, Lee S-H, Hong J-R, Kum K-Y, Oh S, Al-Ghamdi AS, Al-Ghamdi FA, Mandorah AO, Jang J-H, Chang SW. Three-Dimensional Analysis of Root Anatomy and Root Canal Curvature in Mandibular Incisors Using Micro-Computed Tomography with Novel Software. Applied Sciences. 2020; 10(12):4385. https://doi.org/10.3390/app10124385
Chicago/Turabian StyleLee, JongKi, Shin-Hoon Lee, Jong-Rak Hong, Kee-Yeon Kum, Soram Oh, Adel Saeed Al-Ghamdi, Fawzi Ali Al-Ghamdi, Ayman Omar Mandorah, Ji-Hyun Jang, and Seok Woo Chang. 2020. "Three-Dimensional Analysis of Root Anatomy and Root Canal Curvature in Mandibular Incisors Using Micro-Computed Tomography with Novel Software" Applied Sciences 10, no. 12: 4385. https://doi.org/10.3390/app10124385
APA StyleLee, J., Lee, S.-H., Hong, J.-R., Kum, K.-Y., Oh, S., Al-Ghamdi, A. S., Al-Ghamdi, F. A., Mandorah, A. O., Jang, J.-H., & Chang, S. W. (2020). Three-Dimensional Analysis of Root Anatomy and Root Canal Curvature in Mandibular Incisors Using Micro-Computed Tomography with Novel Software. Applied Sciences, 10(12), 4385. https://doi.org/10.3390/app10124385