Investigation of the Correlation between Factors Influencing the Spectrum of Center of Pressure Measurements Using Dynamic Controlled Models of the Upright Stand and Subject Measurements

Abstract
1. Introduction
2. Materials and Methods
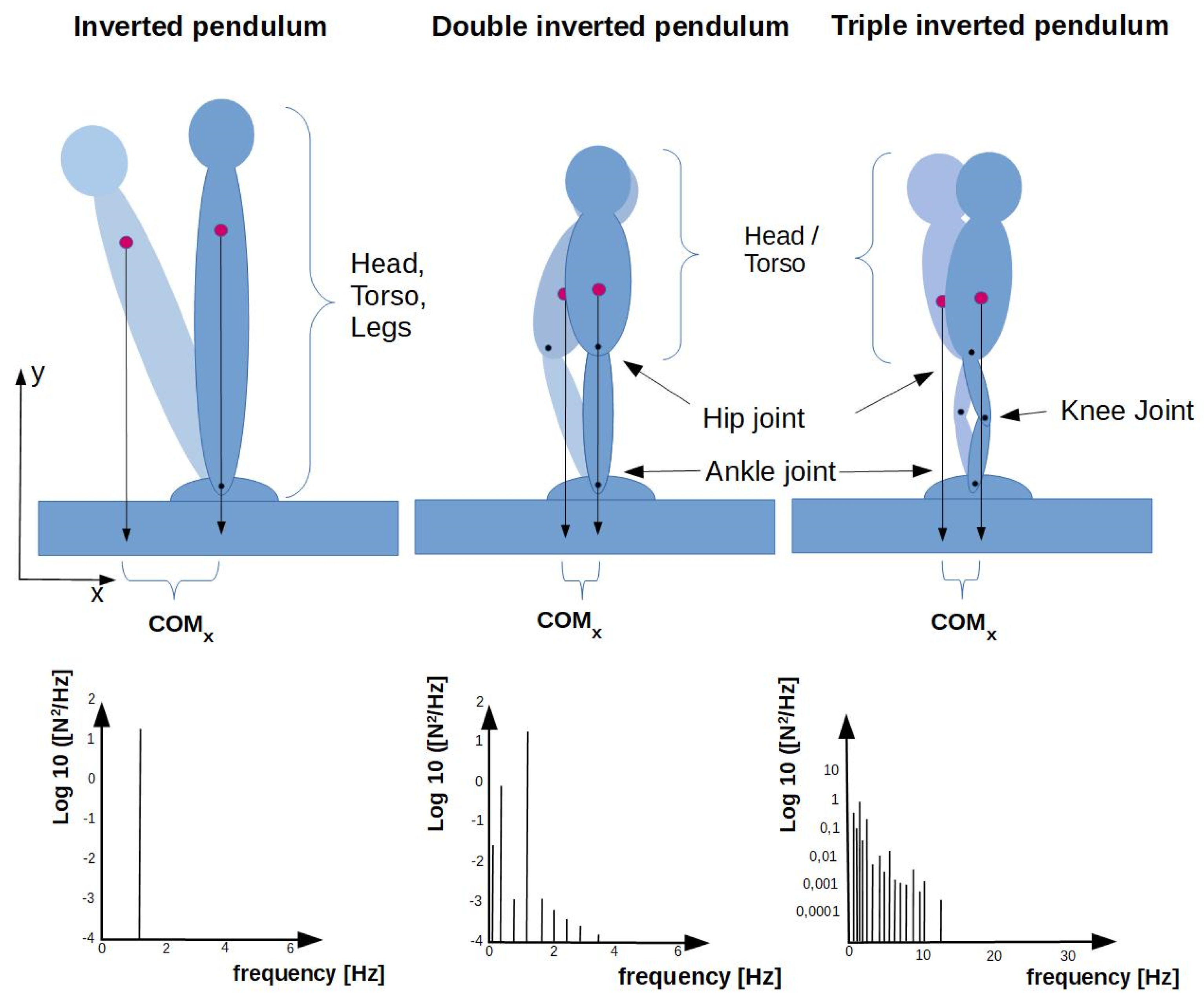
2.1. Structure of the Triple Inverted Pendulum
2.2. Studies on Test Persons
2.3. Data Analysis
3. Results
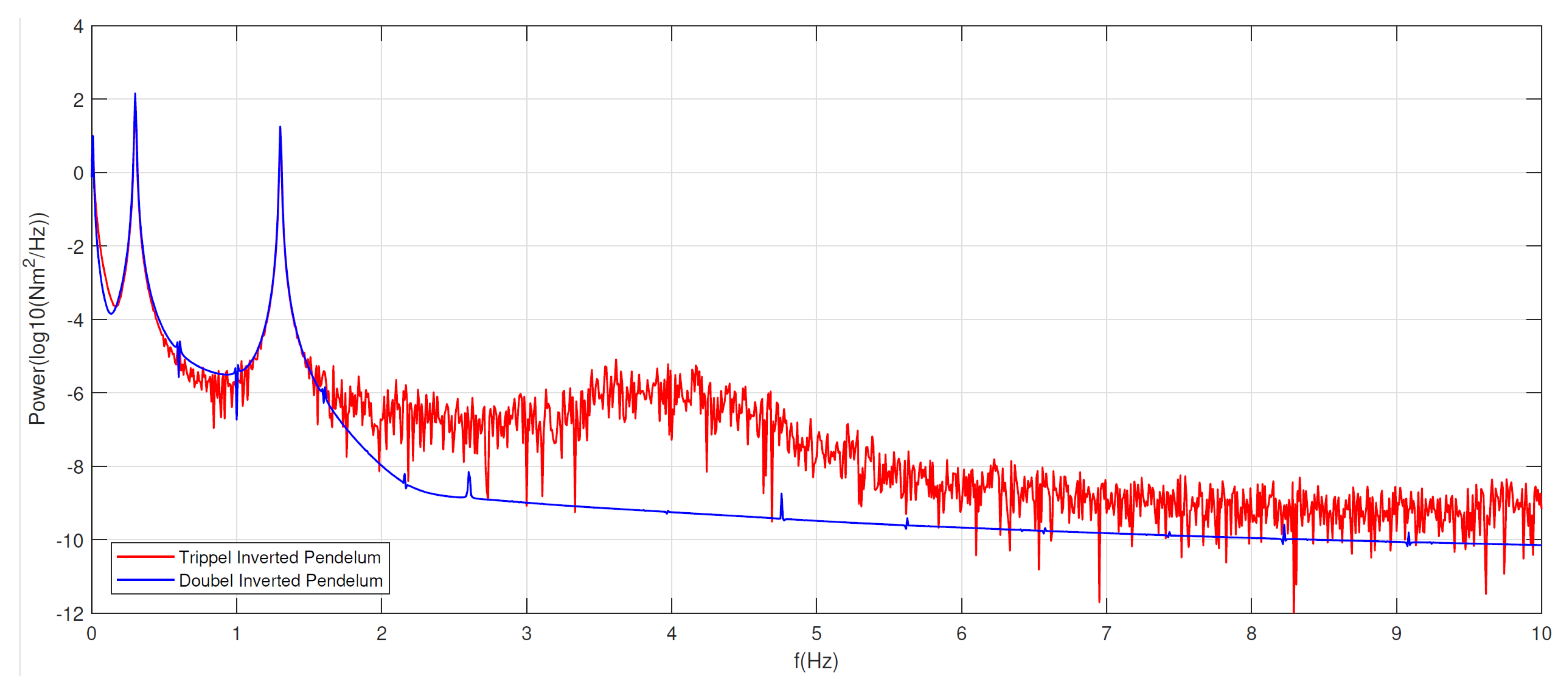
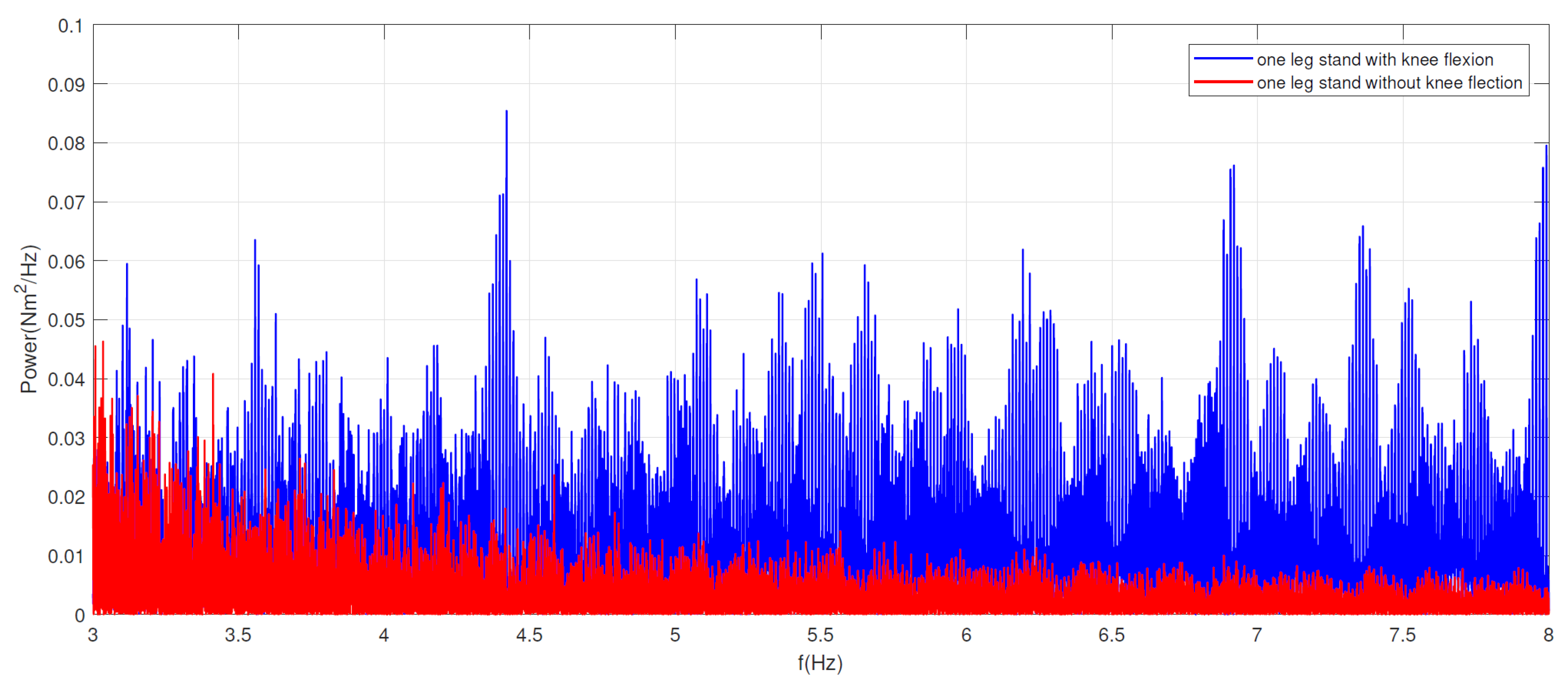
3.1. Frequency Analysis Model Versus Healthy Subjects
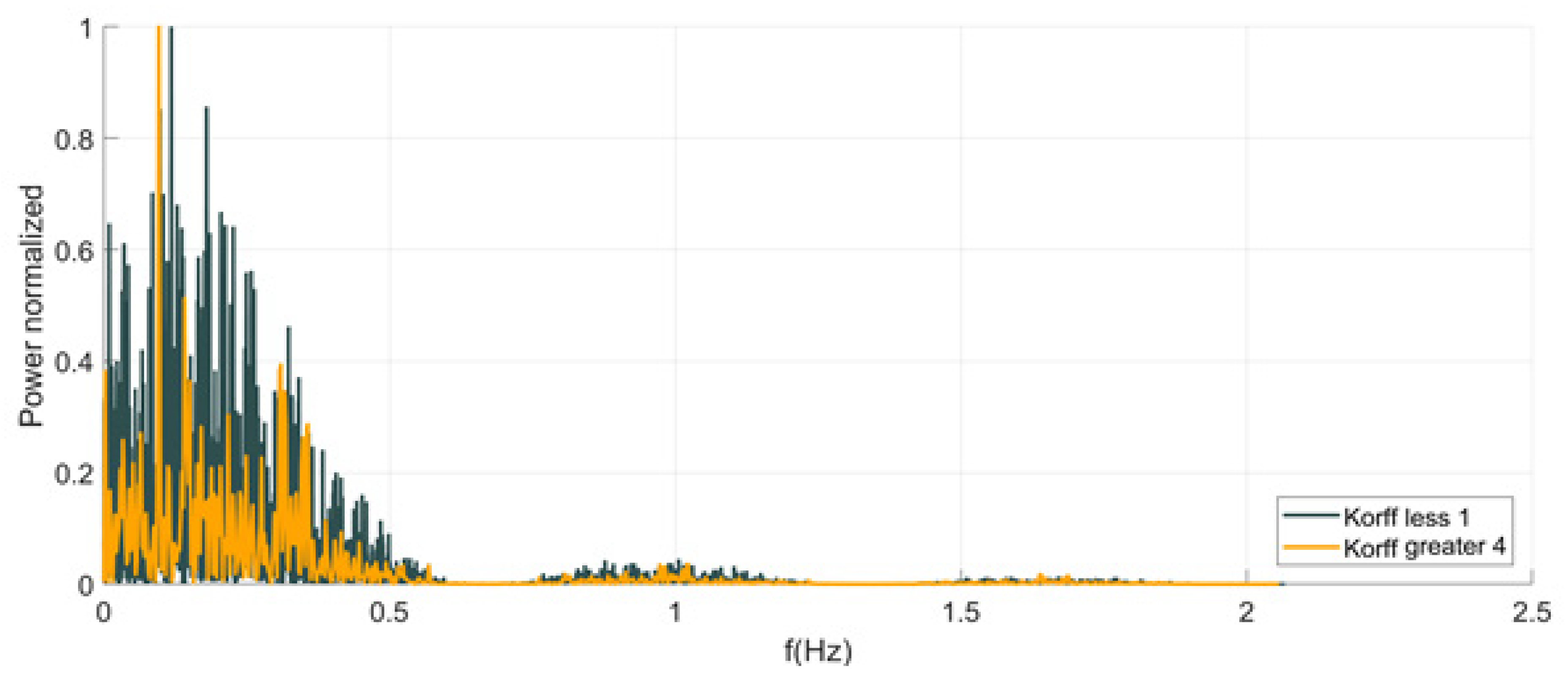
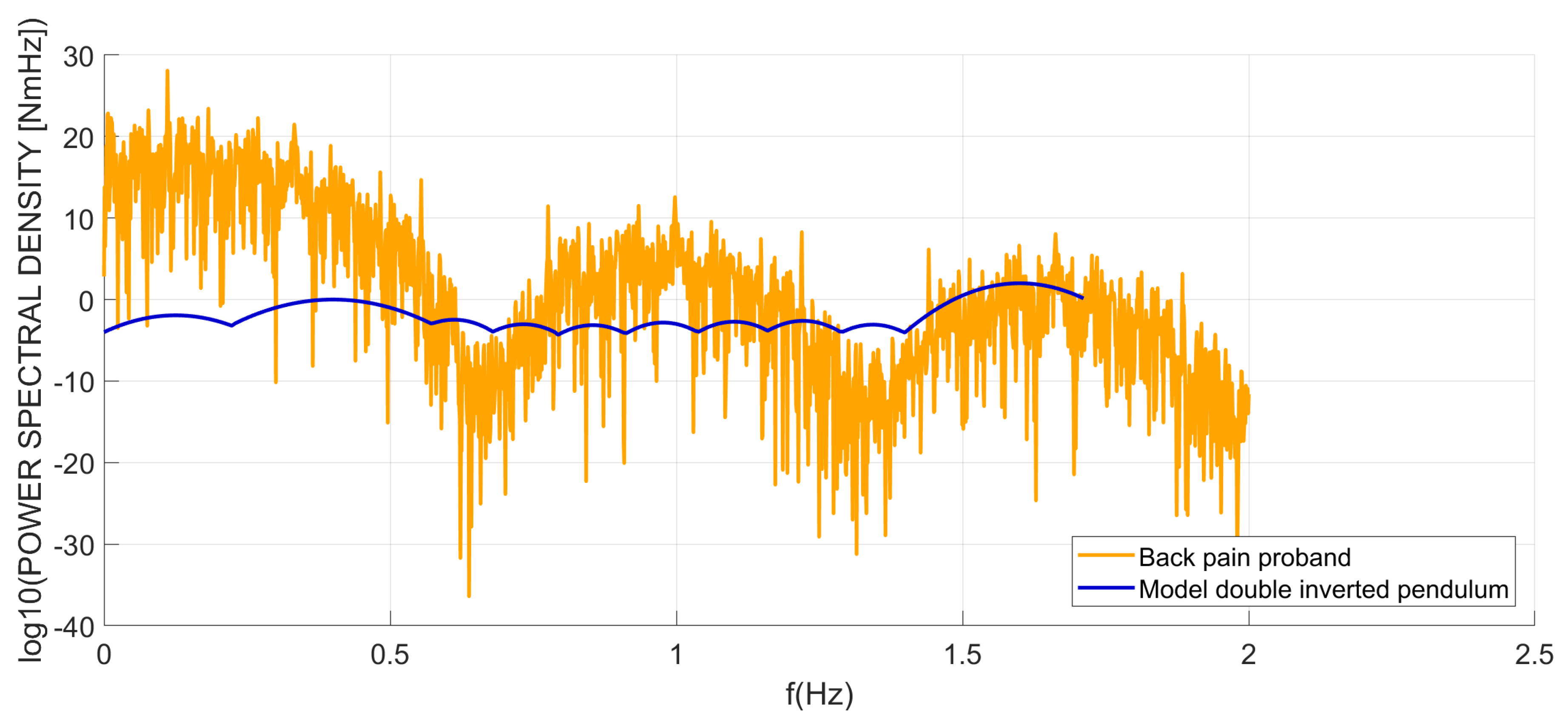
3.2. Test Persons with Back Pain
4. Discussion
4.1. Frequency Distribution in Healthy Volunteers
4.2. Test Persons with Low Back Pain
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Murray, M.; Seireg, A.; Scholz, R. Centre of gravity, centre of pressure and supportive. J. Appl. Physiol. 1967, 23, 831–838. [Google Scholar] [CrossRef] [PubMed]
- Gurfinkel, V.; Osevets, M. Dynamics of the vertical posture in man. Biophysics 1972, 17, 496–506. [Google Scholar]
- Geursen, J.; Altena, D.; Massen, C.; Verduin, M. model of standing man for the description. Agressologie 1976, 17, 63–69. [Google Scholar] [PubMed]
- Mergner, T.; Maurer, C.; Peterka, R. Controlling balance during quiet standing: Proportional and derivative controller generates preceding motor command to body sway position observed in experiments. Gait Posture 2006, 23, 164–172. [Google Scholar]
- Winter, D.; Patla, A.; Ishac, M.; Gage, W. Motor mechanisms of balance during quietstanding. J. Electromyogr. Kinesiol. 2003, 13, 49–456. [Google Scholar] [CrossRef]
- Gage, W.; Winter, D.; Frank, J.; Adkin, A. Kinematic and kinetic validity of the inverted pendulum model in quiet standing. Gait Posture 2004, 19, 124–132. [Google Scholar] [CrossRef]
- Kiemel, T.; Oie, K.; Jeka, J. Slow dynamics of postural sway are in the feedback loop. J. Neurophysiol. 2006, 95, 1410–1418. [Google Scholar] [CrossRef]
- Madigan, M.; Davidson, B.; Nussbaum, M. Postural sway and joint kinematics during quiet standing are affected by lumbar extensor fatigue. Hum. Mov. Sci. 2006, 25, 788–799. [Google Scholar] [CrossRef]
- Edwards, A.S. The measurement of static ataxia. Am. J. Psychol. 1941, 55, 171–188. [Google Scholar] [CrossRef]
- Kapteyn, T.S. Data processing of posturographic curves. Agressologie 1972, 13, 29–34. [Google Scholar]
- Loram, I.; Lakie, M. Human balancing of aninverted pendulum: Position control by small, ballistic-like, throw and catch movements. J. Physiol. 2002, 540, 1111–1124. [Google Scholar] [CrossRef] [PubMed]
- Loram, I.; Maganaris, C.; Lakie, M. Human postural sway results from frequent, ballistic bias impulses by soleus and gastrocnemius. J. Physiol. 2005, 564, 295–311. [Google Scholar] [CrossRef] [PubMed]
- Day, B.; Steiger, M.; Thompson, P.; Marsden, C. Effect of vision and stance width on human body motion when standing: Implications for afferent control of lateral sway. J. Physiol. 1993, 469, 479–499. [Google Scholar] [CrossRef]
- Hsu, W.; Scholz, J.; Schöner, G.; Jeka, J.; Kiemel, T. Control and estimation of posture during quiet stance depends on multi joint coordination. J. Neurophysiol. 2007, 97, 3024–3035. [Google Scholar] [CrossRef]
- Günther, M.; Müller, O.; Blickhan, R. Watching quiet human stance to shake off its straitjacket. Arch. Appl. Mech. 2011, 81, 283–302. [Google Scholar] [CrossRef]
- Nashner, L.; McCollum, G. The organization of human postural movements: A formal basis and experimental synthesis. Behav. Brain Sci. 1985, 8, 135–172. [Google Scholar] [CrossRef]
- Horak, F.; Nashner, L.M. Central programming of postural movements: Adaption to alteredsupport configurations. J. Neurophysiol. 1986, 55, 1369–1381. [Google Scholar] [CrossRef]
- Wilson, E.; Madigan, M.; Davidson, B.; Nussbaum, M. Postural strategy changes with fatigue of the lumbar extensor muscles. Gait Posture 2006, 23, 348–354. [Google Scholar] [CrossRef]
- Berger, W.; Dietz, V.; Hufschmidt, A.; Jung, R.; Mauritz, K.H.; Schmidtbleicher, D. Haltung und Bewegung beim Menschen: Physiologie, Pathophysiologie, Gangentwicklung und Sporttraining; Springer Verlag: Berlin/Heidelberg, Germany, 1984. [Google Scholar]
- Kuo, A. An optimal state estimation model of sensory integration in human postural balance. J. Neural. Eng. 2005, 2, 235–249. [Google Scholar] [CrossRef]
- Saffer, M.; Kiemel, T.; Jeka, J. Coherence analysis of muscle activity during quietstance. Exp. Brain Res. 2008, 185, 215–226. [Google Scholar] [CrossRef]
- Creath, R.; Kiemel, T.; Horak, F.; Peterka, R.; Jeka, J. unified view of quietand perturbed stance: Simultaneous co-existing excitable modes. Neurosci. Lett. 2005, 377, 75–80. [Google Scholar] [CrossRef] [PubMed]
- Edwards, W. Effect of joint stiffness on standing stability. Gait Posture 2007, 25, 432–439. [Google Scholar] [CrossRef] [PubMed]
- Grimmer, S.; Ernst, M.; Günther, M.; Blickhan, R. Running on uneven ground: Leg adjustment to vertical steps and self-stability. J. Exp. Biol. 2008, 211, 2989–3000. [Google Scholar] [CrossRef] [PubMed]
- Blickhan, R.; Seyfarth, A.; Geyer, H.; Grimmer, S.; Wagner, H.; Günther, M. Intelligence by mechanics. Philos. Trans. R. Soc. Lond. 2007, 365, 199–220. [Google Scholar] [CrossRef] [PubMed]
- van Soest, A.; Haenen, W.; Rozendaal, L. Stability of bipedal stance: The contribution of cocontraction and spindle feedback. Biol. Cybern. 2003, 8, 293–301. [Google Scholar] [CrossRef] [PubMed][Green Version]
- Rozendaal, L.; van Soest, A. Joint Stiffness Requirements in a Multi-Segment Stance Mode. In Proceedings of the 20th Congress of the International Society of Biomechanics. Cleveland Clinic Foundation, Cleveland, OH, USA, 31 July–5 August 2005. [Google Scholar]
- Günther, M.; Wagner, H. Dynamics of quiet human stance: Computer simulations of a triple inverted pendulum model. Comput Methods Diomech Biomed Enfin 2016, 19, 819–834. [Google Scholar] [CrossRef]
- Stoll, W. Posturographie in der Vestibularisdiagnostik- Prinzip, Interpretation und klinische Erfahrung. Laryngol. Rhinol. Otol. Stuttg. 1985, 64, 590–594. [Google Scholar] [CrossRef]
- Norre, M.E.; Forrez, G. Posture testing (Posturography) in the diagnosis of peripheral-Vestibular Pathology. Vestib. Pathol. 1986, 243, 186–189. [Google Scholar] [CrossRef]
- Aalto, M.; Pyykko, I.; Starck, J. Computerized Posturography, a development of the measuring system. Acta Otolaryngol. Suppl. Stock. 1988, 449, 71–75. [Google Scholar] [CrossRef]
- Hytönen, M.; Pyykkö, I.; Aalto, H.; Juhola, M.; Ramsay, H. Vestibulo-Ocular and Vestibulo- Spinal Reflexes in Evaluation of Vestibular Lesions. Acta Otolaryngol. Suppl. Stock. 1989, 486, 231–234. [Google Scholar] [CrossRef]
- Nashner, L.; Berthoz, A. Visual contribution to rapid motor responses during posturalcontrol. Brain Res. 1978, 150, 403–407. [Google Scholar] [CrossRef]
- Kohen-Raz, R. Application of tetra-ataxiametric posturography in clinical and developmental diagnosis. Percept. Mot. Ski. 1991, 48, 635–665. [Google Scholar] [CrossRef] [PubMed]
- De Witt, G. Optic versus vestibular and propriozeption impulses, measured by posturometry. Aggressologie 1972, 13, 75–79. [Google Scholar]
- Kohen-Raz, R.; Himmelfarb, M.; Tzur, S.; Kohen-Raz, A.; Shub, Y. Perzeptual and Motor Skils An Initial Evaluation Of Work Fatigue And Circadian Changes By Multiplate Posturography. Percept. Mot. Ski. 1996, 82, 547–557. [Google Scholar] [CrossRef] [PubMed]
- Era, P.; Heikkinen, E. Postural sway during standing and unexpected disturbance of balance in random samples of men of different ages. J. Gerontol. 1985, 40, 287–295. [Google Scholar] [CrossRef]
- Maki, B.E.; Holliday, P.J.; Fernie, G.R. Aging and postural control. A comparison of spontaneous- and induced-sway balance tests. J. Am. Geriatr. Soc. 1990, 38, 1–9. [Google Scholar] [CrossRef]
- Basta, D. Posturografische Verfahren. In Gleichgewichtsstörungen; Basta, D., Ed.; Georg Thieme: Stuttgart, Germany, 2012. [Google Scholar]
- Saziorski, W.M.; Aruin, A.S.; Selujanow, W.M. Biomechanik des Menschlichen Bewegungsap-Parates; Sportverlag: Berlin, Germany, 1984. [Google Scholar]
- Basmajian, J.V.; De Luca, C.J. Muscles Alive: Their Functions Revealed by Electromyography; Lippincott Williams & Wilkins: Baltimore, MD, USA, 1985. [Google Scholar]
- von Korff, M.; Ormel, J.; Keefe, F.J. Grading the severity of chronic pain. Pain 1992, 50, 133–149. [Google Scholar] [CrossRef]
- Koltermann, J.J.; Gerber, M.; Beck, H.; Beck, M. Validation of Different Filters for Center of Pressure Measurements by a Cross-Section Study. Technologies 2019, 7, 68. [Google Scholar] [CrossRef]
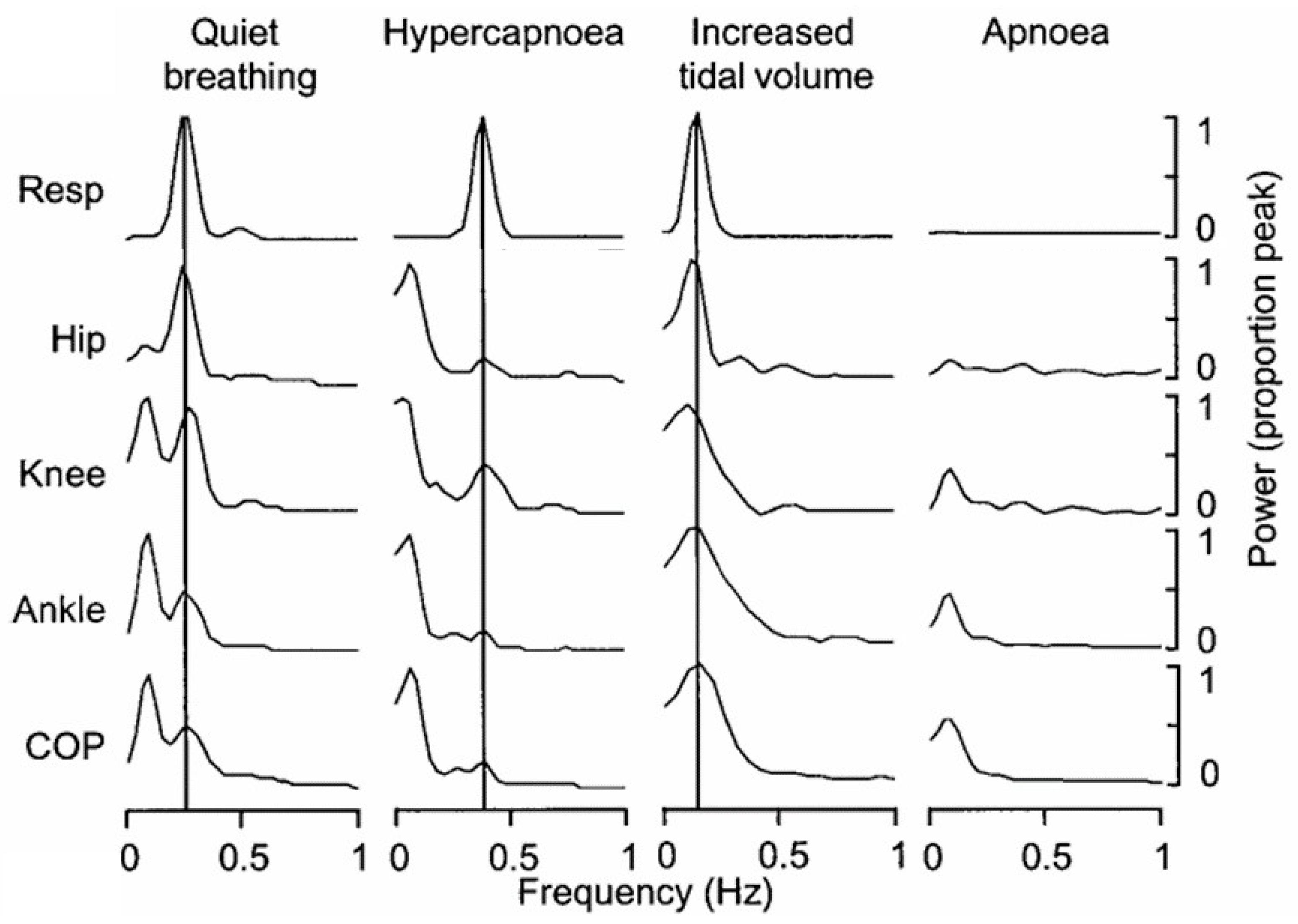
- Hodges, P.W.; Gurfinkel, V.S.; Brumagne, S.; Smith, T.C.; Cordo, P.C. Coexistence of stability and mobility in postural control: Evidence from postural compensation for respiration. Exp. Brain Res. 2002, 144, 293–302. [Google Scholar] [CrossRef]
- Chen, C.L.; Lou, S.Z.; Wu, H.W.; Wu, S.K.; Yeung, K.T.; Su, F.C. Effects of the type and direction of support surface perturbation on postural responses. J. Neuroeng. Rehabil. 2014, 11, 1–12. [Google Scholar] [CrossRef]
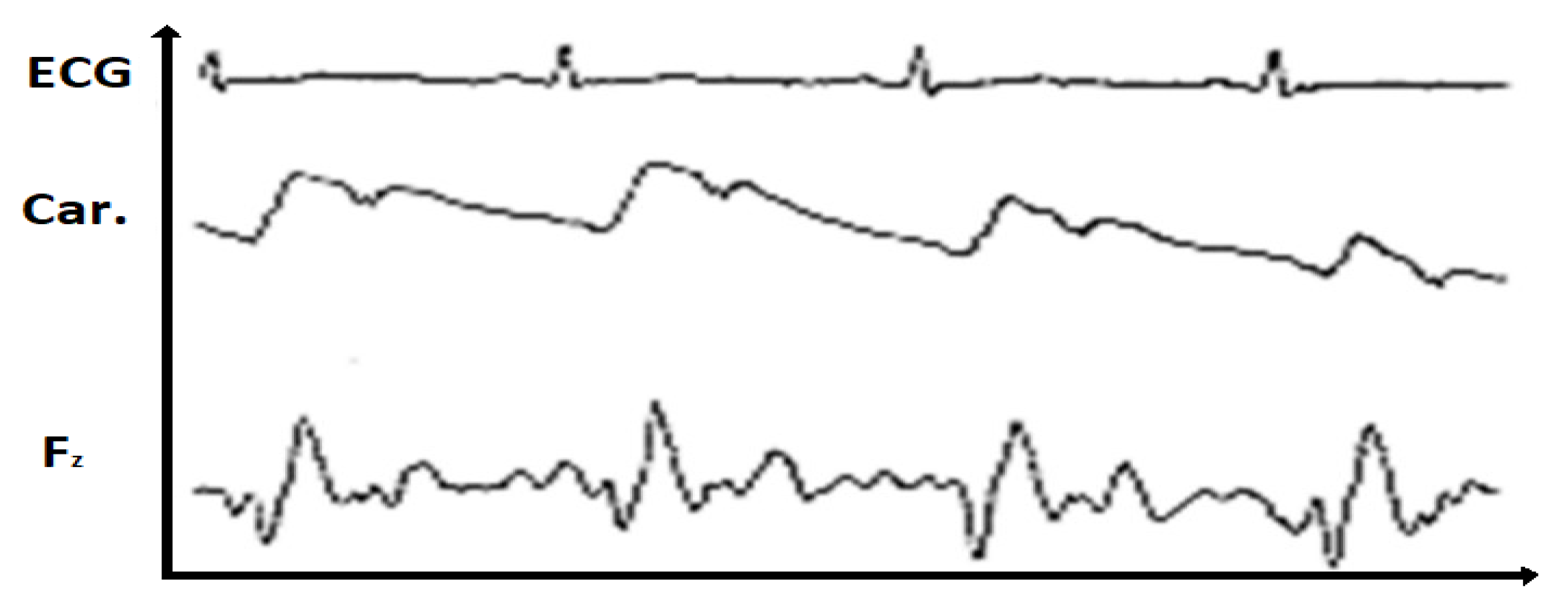
- Stürm, R.; Nigg, B.; Koller, E.A. The impact of cardiac activity on triaxially recorded endogenous microvibrations of the body. Eur. J. Appl. Physiol. Occup. Physiol. 1980, 44, 83–96. [Google Scholar] [CrossRef] [PubMed]
- Keppel, G. Design and Analysis: A Researcher’s Handbook, 3rd ed.; Prentice-Hall, Inc.: New York City, NY, USA, 1991. [Google Scholar]
- Ellis, P.D. The Essential Guide to Effect Sizes: Statistical Power, Meta-Analysis, and the Interpretation of Research Results; Cambridge University Press: Cambridge, NY, USA, 2010. [Google Scholar]
- Baker, R.J.; Patel, D. Lower back pain in the athlete: Common conditions and treatment. Prim. Care 2005, 32, 201–229. [Google Scholar] [CrossRef] [PubMed]
- Fries, E.; Hesse, J.; Hellhammer, J.; Hellhammer, D.H. A new view on hypocortisolism. Psychoneuroendocrinology 2005, 30, 1010–1016. [Google Scholar] [CrossRef]
- Bono, C.M. Low-back pain in athletes. Bone Jt. Surg. Am. 2004, 86, 382–396. [Google Scholar] [CrossRef] [PubMed]
- Barr, K.P.; Griggs, M.; Cadby, T. Lumbar stabilization: Core concepts and current literature, Part 1. Am. J. Phys. Med. Rehabil. 2005, 84, 473–480. [Google Scholar] [CrossRef]
- George, S.Z.; Childs, J.D.; Teyhen, D.S.; Wu, S.S.; Wright, A.C.; Dugan, J.L.; Robinson, M.E. Rationale, design, and protocol for the prevention of low back pain in the military. BMC Musculoskelet Disord 2007, 14, 92. [Google Scholar]
- Atkinson, G.; Nevill, A.M. Statistical methods for assessing measurement error (reliability) in variables relevant to sports medicine. Sports Med. 1998, 26, 217–238. [Google Scholar] [CrossRef]










{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Total Group | Male (52%) | Female (48%) | |
|---|---|---|---|
| Age (J.) | 39.9 ± 17.5 | 40.4 ± 16.6 | 40.54 ± 17.66 |
| Weight (kg) | 75.8 ± 15.6 | 83.9 ± 13.7 | 66.13 ± 11.93 |
| Size (cm) | 171.5 ± 25.8 | 180.9 ± 7.7 | 160.30 ± 34.21 |
| Shoe size (EU) | 42.8 ± 2.7 | 42.5 ± 5.5 | 38.9 ± 1.5 |
| Condition | Area Mean | Area sd | Area var |
|---|---|---|---|
| Knee.flexion | 0.67 | 0.24 | 0.06 |
| Knee.without.flexion | 0.16 | 0.13 | 0.01 |
| Test Quantity (F) | p Value | Etasq | Power | |
|---|---|---|---|---|
| condition | 34.825 | 0 | 0.635 | 1 |
| Gender | Degree of Pain | Area.Mean (Nm2) | Area.sd | Area.var |
|---|---|---|---|---|
| Male | Korff 1 | 3.98 | 1.92 | 3.69 |
| Male | Korff > 4 | 3.48 | 1.66 | 2.78 |
| Female | Korff 1 | 4.08 | 2.12 | 4.51 |
| Female | Korff > 4 | 3.41 | 1.62 | 2.63 |
| Test Quantity (F) | p Value | Etasq | Partial.Etasq | Partial.Omegasq | Power | |
|---|---|---|---|---|---|---|
| Gender | 0.664 | 0.416 | 0.001 | 0.001 | −0.001 | 0.129 |
| Degre of Pain | 9.733 | 0.002 | 0.018 | 0.018 | 0.016 | 0.877 |
| Gender: Degree of Pain | 0.193 | 0.660 | 0.000 | 0.000 | −0.001 | 0.072 |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Koltermann, J.J.; Beck, H.; Beck, M. Investigation of the Correlation between Factors Influencing the Spectrum of Center of Pressure Measurements Using Dynamic Controlled Models of the Upright Stand and Subject Measurements. Appl. Sci. 2020, 10, 3741. https://doi.org/10.3390/app10113741
Koltermann JJ, Beck H, Beck M. Investigation of the Correlation between Factors Influencing the Spectrum of Center of Pressure Measurements Using Dynamic Controlled Models of the Upright Stand and Subject Measurements. Applied Sciences. 2020; 10(11):3741. https://doi.org/10.3390/app10113741
Chicago/Turabian StyleKoltermann, Jan Jens, Heidrun Beck, and Michael Beck. 2020. "Investigation of the Correlation between Factors Influencing the Spectrum of Center of Pressure Measurements Using Dynamic Controlled Models of the Upright Stand and Subject Measurements" Applied Sciences 10, no. 11: 3741. https://doi.org/10.3390/app10113741
APA StyleKoltermann, J. J., Beck, H., & Beck, M. (2020). Investigation of the Correlation between Factors Influencing the Spectrum of Center of Pressure Measurements Using Dynamic Controlled Models of the Upright Stand and Subject Measurements. Applied Sciences, 10(11), 3741. https://doi.org/10.3390/app10113741