Abstract
This paper presents a methodology for designing a humanitarian supply chain (HSC) for immunization in Mexico. The study analyzes the abilities of HSCs provided in the literature and those that are relevant for the HSC vaccination in Mexico. In addition, the stakeholders involved in HSC for immunization were studied. A sentiment analysis of more than 900 newspaper articles was conducted to determine society’s perception of the government’s strategy for vaccine distribution. Considering these aspects and a review of the state-of-the-art in the design of supply chains, a methodology for HSC is proposed. Some of the findings are that resilience and agility, the most important abilities in HSCs in Mexico, can be achieved through government support and strong collaboration between different stakeholders, which was found to be the weakest point of the strategy. The problems observed in the vaccination strategy in Mexico were as follows: (1) a single physical space per municipality was defined for the application of the vaccine, (2) there is a shortage of vaccines, and (3) as far as we know, no methodology has been applied to carry out immunization. This approach considers the design of HSCs in terms of capabilities and stakeholders, which, to the best of our knowledge, is a novel aspect of the literature. This methodology can be used for various scenarios of HSCs in Mexico.
1. Introduction
Humanitarian supply chains (HSCs) should be diverse, global, dynamic, and temporary (Van Wassenhove 2006). By being dynamic, supply chains can cope with unexpected situations, such as damage in transportation, late deliveries, or variations in demand. Additionally, the main stakeholders in HSCs generate and require various information resources, which need to be obtained in a shifting environment. Thus, the challenge for this type of supply chain is identifying the degree of need that victims experience at specific moments (Sheu 2010).
In addition to the problem of information asynchrony, this dynamism results in a low degree of predictability, which further highlights the need to provide solutions to issues relegated to HSC management. This study analyzes the case of immunization supply chains, which adds a layer of difficulty to the study because they respond to currently evolving problems rather than post-disaster scenarios. Therefore, the degree of the impact of an HSC cannot be predicted as time progresses.
For these reasons, investigating the dynamism of HSCs requires focus. The objective is to generate solutions to the issues that accompany a highly dynamic environment. To this end, the study conducts an analysis of the capabilities of HSCs. Previous studies demonstrated that an analysis of such capabilities can lead to better solutions (Altay et al. 2018; Prakash et al. 2020; Tablakar 2017).
Specifically, the study highlights the capabilities of supply chains and the role of the involved stakeholders to propose an optimal design for the distribution of COVID-19 vaccines in Mexico. The main reason the study is being undertaken is because the country currently holds the third position among countries with the highest mortality rates resulting from COVID-19 (Forbes 2021). Moreover, the study hopes that the proposed methodology could be used in other scenarios related to HSCs, not only in Mexico but in other countries in Latin America.
The rest of the paper is structured as follows. Section 2 presents the methodology used to answer the research questions and Section 3 discusses the evolution of COVID-19 in Mexico. Section 4 presents the state-of-the-art of supply chain capabilities and those relevant for HSC vaccination in Mexico. Section 5 presents the actors involved in the distribution of vaccines, considering the World Health Organization’s (WHO) opinion, as well as the context in Mexico. Additionally, Section 5 presents society’s opinion on the vaccination strategy in Mexico through a sentiment analysis of the main newspapers in Mexico, because both society and the media are main actors in the HSC. Furthermore, with the review of the state-of-the-art on the methodologies for the supply chain design, Section 5 presents a methodology for designing a vaccination HSC and developing the first phases for Mexico. Finally, Section 6 presents the conclusions and scope for future work.
2. Methodology
The holistic methodological approach based on the general system theory, particularly the methodology of soft systems (Checkland 1999), provides the status of a given problem situation and contrasts this with the ideal state through systematic thinking.
Our hypothesis is that no HSC design methodology was used for COVID-19 vaccination in Mexico. However, this is difficult to prove. The society has perceived serious errors in the management of vaccine distribution, but the government says that it has followed the best strategy.
To design the HSC for the distribution of vaccines in Mexico, these research questions were posed:
- RQ1.
- What is the social perception of the vaccine distribution strategy in Mexico?
- RQ2.
- What are the problems of the vaccination strategy in Mexico?
- RQ3.
- What are the capabilities that the supply chain should have for the distribution of vaccines?
- RQ4.
- Who are the actors involved in the supply chain of vaccine distribution in Mexico?
- RQ5.
- Is there a methodology for the design of the supply chain for the distribution of vaccines in Mexico?
To answer these questions, the following actions were performed:
- Documentary analysis of the evolution of COVID-19 in Mexico, analyzing statistics and government positions regarding health regulations to contrast the effects of the epidemic. The documents were found in newscasts, newspapers, and official documents of the Mexican government.
- Sentiment analysis based on articles featured in the prominent newspapers in circulation to understand social perception of the vaccination strategy of Mexico.
- Review of the literature to investigate the requisite abilities of the supply chain for vaccine distribution in Mexico.
- Analysis of the stakeholders involved in the supply chain for the distribution of vaccines in Mexico and their participation, according to international standards.
- A methodology for the design of a humanitarian supply chain in Mexico.
3. Evolution of COVID-19 in Mexico
The series of events that positioned Mexico as the second leading country in terms of mortality resulting from COVID-19 can be explained through the following events.
On 31 December 2019, the World Health Organization (WHO) office in China was informed of an atypical case of pneumonia detected in Wuhan. On the same day, the WHO epidemic platform, namely, the Epidemic Intelligence from Open Sources, received a report from PicMed detailing a cluster of cases of unknown causes. Two days after this, the WHO informed the Global Alert and Response Network about these cases. The WHO published the first alert of the disease on Twitter on 4 January 2020. After rapid action, the cause of the surge of pneumonia was identified as a type of coronavirus. On January 10, the WHO published its orientation documentation on the disease. The first case of the disease outside China was detected in Thailand on January 13, and the first epidemic alert was published on January 16, immediately after the detection of the first case in Japan. Eight days after the disease was categorized as an epidemic, France announced the existence of its first three cases. On the same day, the director of the Health Panamerican Organization issued advice to locate and isolate infected patients.
After grasping the potential scope of the infection, the WHO published advice regarding the use of face masks on 29 January 2020. On February 25, Africa and Latin America reported their first cases. The first case in Mexico was recorded on February 28. On March 3, the WHO urged industries and governments to increase the production of personal protection equipment by 40% due to the rapid spread of the disease. As cases continued to increase exponentially, COVID-19 was officially classified as a pandemic on March 11. In response, Mexican universities transitioned to virtual teaching beginning on March 13 due to the risk of transmission. However, Mexican authorities allowed the music festival known as Vive Latino to be held on March 14. Two days later, massive events in Mexico City were suspended. Mexico saw its first official death due to COVID-19 on March 18. The Mexican government launched an awareness campaign known as “Sana Distancia (translated as Healthy Distance)” on March 23 to encourage the population to engage in safety measures to reduce infections. Nevertheless, one day after the launch of this campaign, Mexico entered phase two of the pandemic, with 367 confirmed cases. By April 17, it exceeded 1000 deaths and entered phase three on April 21.
On June 1, the government established a stop-light strategy to define the regional situation for the operation of non-essential businesses. Meanwhile, in the global scenario, COVAX1 (Berkley 2021; Baker-Sheikh et al. 2021) committed to catering to more than 150 countries to provide innovative and equitable access to COVID-19 diagnostics, treatments, and vaccines, with 75 countries expressing interest in financing the production of vaccines through their public budgets.
On 31 July 2020, Mexico was ranked as having the third highest number of deaths due to COVID-19. The WHO called on manufacturers of COVID-19 vaccines to apply for pre-approval and inclusion in the emergency use roll on October 1. Moreover, the WHO and UNICEF made a public call to action to prevent measles and poliomyelitis epidemics due to the interruption of immunization campaigns caused by COVID-19. The WHO published provisional advice to help governments develop and renew national action plans on immunization campaigns on November 16. One month later (December 11), the Mexican dependency named Comisión Federal para la Protección contra Riesgos Sanitarios (COFEPRIS, translated as Federal Commission for the Protection against Sanitary Risk) stated their approval for the emergency use of vaccines manufactured by Pfizer and BioNTech. The increasing movement and interactions of civilians that accompany the approaching holidays accelerated the daily number of infections. For this reason, Mexico City and Estado de Mexico re-instated the red-stop-light phase on December 18. The first batch of Pfizer vaccines arrived in the country on December 23, and vaccination efforts for medical personnel were initiated the following day.
COFEPRIS authorized the emergency use of the Oxford-AstraZeneca vaccine on 4 January 2021. The government reported that 594,725 vaccines were administered as of January 22, which amounted to 27, 346 shots on a daily basis. Despite these favorable results, Mexico reached a total of 20,057 infections on January 23, and the country surpassed 150,000 deaths due to COVID-19 on January 25. COFEPRIS announced their approval for the Sputnik V vaccine on February 2. Three hundred and seventy-six days after the WHO urged the global population to wear face masks to slow the spread of the disease, the Mexican president announced his rejection of wearing face masks on February 8.
On 24 August 2021, according to Statista (2021a), Mexico ranked fourth among countries with the highest number of cases in Latin America, with more than 3 million confirmed cases (Figure 1).
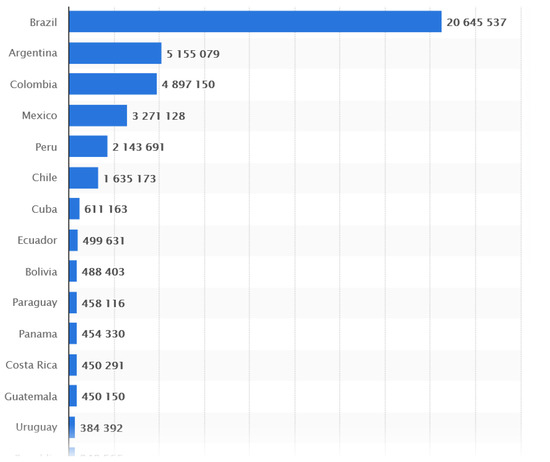
Figure 1.
Coronavirus (COVID-19) Global Cases by Johns Hopkins CSSE (Statista 2021a).
The next section describes the supply and transfer capacities used in vaccine distribution.
4. Supply Chain Capabilities
Supply chains are characterized by their internal and external abilities to integrate, construct, or reconfigure the chain. In the specific case of HSCs, such abilities are intended to function in highly dynamic environments. Polater (2020) conducted a framework review of the literature and observed the following HSC abilities.
Agility: This capability refers to the HSCs’ ability to respond in a rapid manner and to remain cost-effective. It is used during periods of high levels of uncertainty and demand (Altay et al. 2018). To achieve agility, other capabilities are required, such as clearly understanding the problem (sensing), determining the necessary resources (seizing), and reviewing strategies for effective operation (reconfiguring and transforming). L’Hermitte et al. (2016) defines agility as the balance needed to determine capabilities in the long-term and to adapt to unexpected changes. For this capability to be feasible, achieving collaboration between different stakeholders and maintaining the organizational culture are necessary prerequisites.
Resilience: This aspect denotes the capacity to recover, return to the original state, or reconfigure according to the necessities of the environment. Resilience is related to the speed to return to a normal state after reaching a state of disaster. Furthermore, it is the ability to react to unexpected situations (Ali et al. 2017; Carvalho 2012; Ponomarov and Holcomb 2009; Purvis et al. 2016). Mishra et al. (2020) proposed that different organizations should collaborate to achieve this purpose and to save human lives.
Other related capabilities include sensing, seizing, and reconfiguring (Polater 2020). The achievement of sensing requires the use of reliable and real-time data. However, this aspect can prove difficult in developing countries (Mishra et al. 2020). Another capability is knowledge in accessing dynamic abilities (Defee and Fugate 2010). This characteristic refers to obtaining knowledge about the abilities of HSC stakeholders to further utilize these capabilities. Lastly, the sustaining capability (Mishra et al. 2020) refers to the generation of long-term strategies that benefit all stakeholders in a supply chain.
The successful operation of HSCs requires different capabilities. Nevertheless, according to Altay et al. (2018), two are worth highlighting: agility and resilience. Therefore, the study recognizes the need to analyze and evaluate both capabilities and their influence on the pre-disaster phase. However, researchers suggest that agility is more significant in the post-disaster phase. For agility and resilience, collaboration among the actors of HSCs plays an important role. A literature review perceived agility and resilience as the most important capabilities, because the others are closely related to these two. The subsequent section discusses these two capacities against the background of HSCs in Mexico.
Capabilities for Vaccine Distribution in Mexico
This study aims to describe several aspects that are directly related to the capabilities of supply chains. As previously specified, previous studies on the distribution of vaccines mainly conducted analyses before or during disasters. The current analysis, however, reveals that the most significant abilities of HSCs are agility and resilience (Altay et al. 2018). Notably, a resilient supply chain does not always guarantee the highest cost-efficiency, or, in other words, is not always the most agile.
Agility: As previously mentioned, agility is the ability to provide a quick and cost-effective response to dynamic environments. In the case of vaccine distribution, the achievement of agility is related to an optimization model that enables decision-makers to determine the number of distribution sites across the country. Furthermore, the model aims to determine distribution costs based on the access routes of each state in which the vaccine will be applied and establish a strategy for the last-mile distribution that ensures vaccines are available at the appropriate time and place. The term right time refers to the delivery of vaccines under optimal conditions for use. As well as decisions on distribution according to route, the mode of transportation should be considered, which should be able to cross different zones and lands, affecting distribution costs. Thus, the study suggests determination of the appropriate optimization model as a future goal in this field. In the meantime, the goal is to design appropriate methods for supply chains given the concurrent conditions and investigate the role of stakeholders in vaccine distribution in Mexico.
Resilience: As previously noted, resilience refers to the ability of supply chains to resist or adapt to uncertainties in the environment. In the case of vaccine distribution, this study pertains to the number of required vaccine doses. At present, the existing vaccines in the market require either one or two doses or shots of the vaccine and specific thermoregulation conditions for storage. The vaccines developed by Pfizer and BioNTech require storage at a temperature of −70 °C. Another example is the AstraZeneca/Oxford vaccine, which can survive within temperatures ranging from 2 °C to 8 °C. For this reason, pharma companies propose the development of dry ice containers to prolong the lifespan of vaccines outside industrial freezers.
Table 1 presents a comparison of the vaccines that have been accepted for use in Mexico and their logistic requirements.

Table 1.
Comparison of vaccines accepted for use in Mexico.
As can be seen in Table 1, the availability of the vaccine types is not the same. A purchase was scheduled with the pharmaceutical companies of 180,400,000 vaccines for the year 2021, of which 42.9% correspond to AstraZeneca, 19% to CanSino, and 18% to Pfizer. However, by June 2021 only 47,716,810 vaccines had arrived and, because of their availability, 40% correspond to Pfizer and 25.76% to AstraZeneca (Figure 2).
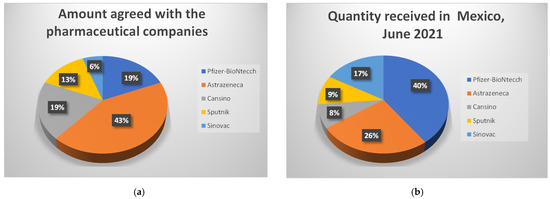
Figure 2.
Vaccine availability in México in 2021, (a) Amount agreed with the pharmaceutical companies and (b) Quantity received in Mexico, June 2021 (Leyva 2021; Expansión Política 2021).
In Mexico, the Pfizer vaccines were administered only to healthcare personnel, while AstraZeneca and Sinovac vaccines were administered to adults over 60 years of age. The CanSino vaccine applications started in April 2021 for education service providers. Sputnik V was provided to those in the age group of 50–59 years and AstraZeneca and Sinovac for the groups of 40–49 years and older than 18 years, but this varied by state and even by region.
Resiliency can be achieved through governmental support, adequate capacity planning, the establishment of a strong collaboration between different stakeholders, and the provision of agility (Singh et al. 2018; Balcik et al. 2017). Previous studies have observed that the weakest point of HSCs in Mexico is the collaboration between stakeholders, which can be understood to be due to the media, lack of communication between stakeholders, and surplus or deficit of resources. The next section addresses these important aspects of the immunization supply chain.
5. Stakeholders in the Supply Chain: The Case of Vaccine Distribution
Day (2014) established the three elements considered necessary for the construction of an HSC, namely, topology, length of HSC route, clusters and redundancies, entities or stakeholders that represent the government, non-governmental organizations, the military, paid logistic companies, and donors, among others, and the environment, which may be presented as cases where natural disasters occur. The subsequent analysis focuses on the stakeholders involved in vaccine distribution.
According to the World Health Organization (2017), the management of stakeholders across processes should be highly prioritized. Understanding their identities and involving them can promote public trust in vaccination efforts. Nevertheless, previous researchers proposes that relationships with stakeholders should be established prior to a crisis. As discussed in the previous section, establishing such relationships can aid in the achievement of resilience and agility in the supply chain.
The World Health Organization (WHO) identifies the major stakeholders as those at the governmental level, such as sanitary authorities, national crisis response and emergency teams, healthcare ministries, and public healthcare institutes for the country in question, among others. The main provider in the immunization effort is the government, which is responsible for providing the necessary support to ensure financial sustainability, enforce public policy, and develop a regional strategy alongside other stakeholders in the country. In addition, the government should provide the public with timely information on concerns regarding vaccine security and efficacy and ensure that the programs employ the proper personnel by providing the capacity and incentives needed to manage the program.
Apart from boosting awareness of the efforts of immunization programs, the government should be open to discussion with citizens and pharmaceutical companies to ensure accessibility to the vaccine (World Health Organization 2012). In the same manner, the participation of regional experts, such as members of the National Immunization Technical Advisory Group (NITAG2), prominent medical doctors, and key immunization opinion leaders, should be considered. International organizations should be responsible for helping countries define the guiding principles and normativity of immunization services to establish synergy with other healthcare services.
Regarding the medical sector, the WHO also recommends considering doctors, nurses, pharmaceutical companies, healthcare personnel, and community leaders as stakeholders that may have high levels of participation in the government’s immunization efforts. Healthcare personnel are responsible for providing services, educating colleagues, and identifying areas of opportunity within the processes of fostering improvement and utilizing emerging technologies to facilitate the creation of information systems. At the same time, pharma companies and manufacturers of immunization equipment should continue the development and production of high-quality vaccines that meet the needs and experiences of various countries. They should also establish relationships that promote growth in production capacity.
Another group of stakeholders comprises academic and research centers, who bear the responsibility of promoting innovation and vaccine development, contributing to logistic challenges, and incorporating multidisciplinary research that target end-users. Moreover, the academe should aim to improve their dialog with fellow researchers. In addition, researchers in this field should disclose the data and methodologies employed to promote scientific evidence, which can guide healthcare policies.
Conversely, public figures in general play an important role. For instance, despite the common association of the term influencer with social media, the WHO categorizes members of congress, bloggers, civilian organizations, local opinion leaders, and the business and tourism sectors as influencers. Another stakeholder that is closely related to the previous group includes mass-printed and web media and journalists.
The last two groups of immunization stakeholders are composed of the public and society in general, including individuals who have recently been vaccinated or those who are expecting to receive a dose. This group of stakeholders, which possesses less visibility, includes individuals who are indirectly affected by the pandemic or events related to the epidemic, such as the experience gained indirectly through a diseased or inoculated relative, immunocompromised individuals, and school personnel. According to the WHO, persons who received a vaccine dose bear the responsibility of understanding the associated risks and benefits, and participating and contributing to the vial delivery processes, as well as providing information about the perspective and needs of their communities, and demanding safe and efficient immunization programs from their governments.
5.1. Stakeholders of Vaccine Distribution in Mexico
The subsequent section describes the situation of the stakeholders of vaccine distribution in Mexico. The Federal Sanitary System and its equivalent or homologue entities across regions or states are formed by the Federal Commission for Protection Against Sanitary Risks or COFEPRIS3. This system was integrated with the objective of organizing and harmonizing control actions and sanitary promotion across Mexico to enable a coordinated execution at the federal and regional levels by the Ministry of Health through COFEPRIS. In terms of the functions of the Federal Sanitary System, one of the main problems faced by Mexico is the lack of regulation and penalization regarding the several sanitary measures that were implemented, such as the use of facemasks or the prohibition of civilians gather in mass events.
The Ministry of Health in Mexico is a branch of the Executive Power, which is mainly in charge of disease prevention and health promotion for the population (Gobierno de México 2019b). The Ministry of Health established a healthcare strategy that promotes community actions that are linked and integrated with the first level of attention. The first level of attention comprises (1) promotion campaigns for community healthcare, (2) specialized brigades, and (3) clinical attention equipment units, which are coordinated among one another. However, they have not provided the expected results because Mexico is one of the highest-ranked countries in terms of mortality. A document (Secretaría de Salud 2020) that exposes this strategy mentions that actions should be organized and coordinated from the Healthcare Unit at the first level, or by those that operate in corresponding territories. In other words, these units are operating at the local level and communicate to the federal level after this. However, even the task of providing timely follow-up to patients presents a problem in this case. The massive numbers of local brigades are those tasked with providing information on which actions are being taken to the first-level unit. However, this process lacks a real-time information system. As such, this system lacks effectivity at the metropolis level, where an increase in COVID-related cases and deaths is observed. The rate of disease transmission has led to a loss of control according to this strategy. Moreover, this document does not mention the participation of stakeholders in immunization strategies, but only highlights the patient follow-up.
Despite constant communication with the Executive Power, the message remains confusing. The use of face masks as a preventive measure against COVID-19 is being promoted worldwide (World Health Organization 2020; Centro Mario Molina 2020; Centers for Disease Control and Prevention 2021); nevertheless, health authorities in Mexico at the federal level have not updated the guidelines on their use. Moreover, they have continued to disregard the effectiveness of wearing face masks (Daen and Aguirre 2021; Infobae 2020), such that the issue of wearing face masks is becoming an issue in electoral politics4 (Navarro 2020; Xímenez Fyvie 2021). Apparently, the function of informing and promoting dialog is conducted through the daily report known as “La Mañanera” (translated as: The Morning). Nevertheless, such dialogs remain ambiguous and confusing in terms of guidelines on sanctions for failure to comply with preventive measures and there is a lack of regard of the importance of following these protocols.
The Institute for Public Health is an academic institution that is committed to offering results based on research on relevant problems and public healthcare to prevent and control diseases (Gobierno de México 2019c). Ideally, the institute should work alongside researchers from private and public universities in Mexico to find a cure and deliver immunization options. Some universities have lent their infrastructure and supported logistics within their facilities for application of the vaccine. However, these have been few. Eventually, these institutions ceased their participation in external logistics (Expansión Política 2020; Huerta 2021).
Communication media, specifically digital newspapers, have been the main sources shaping citizens’ opinions on the vaccine distribution strategy. An analysis of the four digital news organizations with the largest online presence in Mexico was performed. The study employed Amazon’s tool, Alexa, to determine web ranking. Table 2 presents the result of the search for the month of May 2021. Although there are more than 2000 digital newspapers in Mexico, only the top 100 newspapers according to the Alexa (2021) were considered.
Table 2.
Journals with the largest online presence (Own elaboration based on Alexa rankings (Alexa 2021)).
Given that news reporting should be impartial, objective, and neutral, the study analyzed the opinion or editorial section of each news website, because the news section could not fulfill this objective, that is, to analyze the feelings of journalists reporting on the government’s vaccination strategies. The corresponding websites of the news organizations were screened for articles that contain the keywords “vaccination”, “strategy”, “Mexico”, and “COVID” between January 2020 and March 2021. Table 3 provides the number of articles retrieved after data screening.
Table 3.
Number of journals analyzed.
After data screening on the websites, the study conducted a sentiment analysis (Methodology for Designing Humanitarian Supply Chains Distribution of COVID-19 Vaccines in Mexico 2021). The articles were translated into the English language to take advantage of the existing dictionaries that utilize artificial intelligence to classify the emotions contained within a string of text, such as anticipation, aversion, fear, joy, sadness, surprise, and trust. The results show a similar percentage across the newspapers (Figure 3).
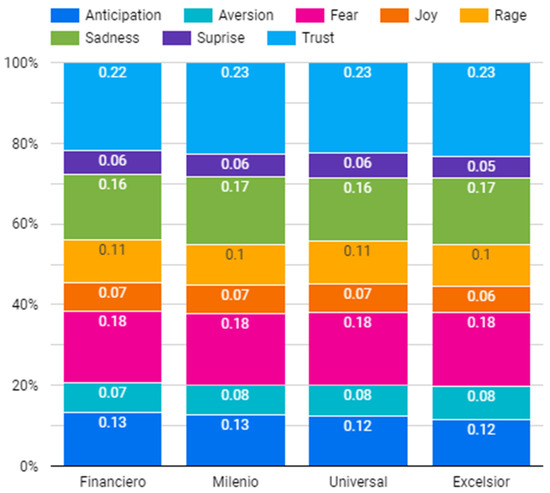
Figure 3.
Proportions of various emotions (anticipation, aversion, fear, joy, sadness, surprise, and trust).
The analysis revealed that the distribution of emotions is relatively similar across news websites. Notably, the ideological trends behind every newspaper represent the left, central, and right political inclinations. The overall trend of the articles was either negative or positive, as shown in Figure 4. Another distinct observation is that when the government’s strategy fails, the media plays an important role in informing citizens about the pandemic situation and the strategies being undertaken to avoid it.
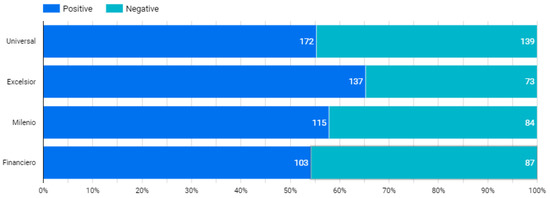
Figure 4.
Positive and negative trends of emotions detected from newspaper articles.
The study classified the predominating opinions within articles into negative and positive and plotted a graph for each news site to assess the overall distribution of opinions. As presented in Figure 4, more than 50% of the articles conveyed a positive tone. The news site with the greatest number of articles with positive opinions is Excelsior, a leftist newspaper. Nevertheless, when analyzing the predominating emotions and categorizing them into negative (sadness, aversion, rage, and fear), positive (joy and trust), and neutral (surprise and anticipation) emotions, the study found that negative emotions across all newspapers surpass the frequencies of positive and neutral emotions, as depicted by the bar graphs in Figure 5.
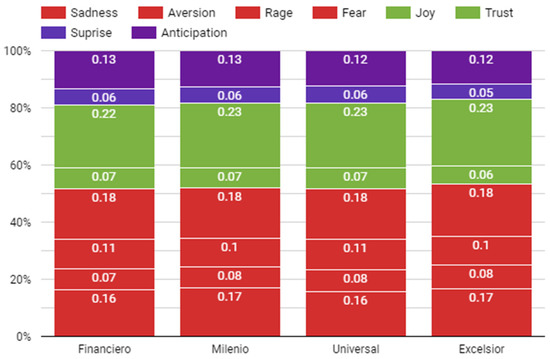
Figure 5.
Categorization of predominant emotions.
Lastly, using this categorization, the study analyzed trends according to the publication dates of the articles (Figure 6). Negative emotions continued to dominate the timeline of published articles. However, the frequency of negative emotions seemed to decline by the end of March, which coincides with the start of the application of vaccines to the population over than 60 years. Thus, the study proposes that media opinions should be investigated throughout the remainder of the vaccination strategy as a future effort.
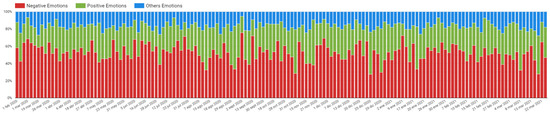
Figure 6.
Classification of emotions according to timeline.
The next section discusses several aspects of the vaccination strategy in detail.
5.2. Vaccination Strategy in Mexico
The vaccination strategy of the Mexican government is divided into five phases, as described in Table 4.
Table 4.
Vaccination phases in Mexico as proposed by the government. Source: Gobierno de México (2021a, 2021b).
The first stage was conducted with 439,725 doses of the Pfizer-BioNTech vaccine, which were distributed across states in the country. The second stage was initiated on 12 February 2020 with the application of the AstraZeneca Vaccine in 333 municipalities across the 32 states. The parameters for eligibility for inoculation were based only on the recipients’ age. As such, no studies were conducted on the effects of the vaccines on individuals with chronic diseases or regarding the density of the infection at the regional level. The Mexican population was asked to fill out an online form as a means of registration to receive the vaccine. Nevertheless, the platform had technical difficulties and excludes people lacking technological skills and access to the Internet. Mexico is currently in the second stage. The government decided to vaccinate education workers to prioritize the return to face-to-face education, (Varela 2021); however, as of August 2021, no one has gone back to school, and many workers in their 30s and 40s have yet to receive their second dose.
On 25 August 2021, 82,678,717 doses of the COVID-19 vaccine had been applied in Mexico, according to the data presented by the Ministry of Health. With these doses, 56,925,095 have been vaccinated, of which 32,278,249 (56.70%) have completed the vaccination scheme and 24,646,846 have received one dose (Ramos and Contreras 2021). However, these data vary depending on the source. According to Statista (2021b) in Figure 7, only 44.01% have been vaccinated with a single dose and only 24% have received the recommended dose.
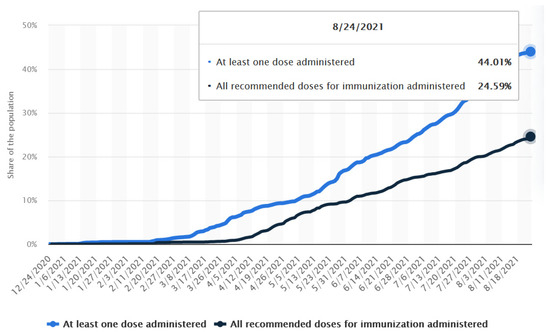
Figure 7.
Share of the population that are partially or fully vaccinated against COVID-19 in Mexico as of 24 August 2021, Statista (2021b).
At present, the vaccination of individuals aged from 16 to 39 years is ongoing, but has not yet started in all the states of the Mexican Republic. There is a third wave with the delta variant that is causing infections among the youngest citizens, who have not yet been vaccinated.
Several problems observed with the vaccination strategy are as follows: (1) public health personnel have been prioritized over the private sector, (2) a single physical space was defined per municipality or locality for the application of the vaccine; this centralization of the application generated abuse and anarchy, and (3) a group called the “servants of the nation5” was commissioned to integrate the vaccination brigades (Sánchez 2021). However, the vaccination rate remained low, as a result of the scarcity of the vaccine (Badillo 2021).
6. Design of the Supply Chain
Although previous studies were conducted on the design of manufacturing supply chains, studies that investigated the design for HSCs were few and mainly written in the last year (Malmir and Zobel 2021; Sokat and Altay 2021). Furthermore, to the best of our knowledge, no article that discusses the design of the cold chain for vaccine distribution using the proposed methodology for designing HSCs has been published. In the case of Mexico, optimization models are necessary, among other strategies. The most relevant is to ensure the effectiveness of the vaccine distribution supply chain. Our proposal involves considering the capacities of the supply chain and involving stakeholders in different phases.
Elgazzar et al. (2019) conducted a review of the literature by examining more than 269 articles and identified the necessary design elements of a supply chain. Elgazzar et al. (2019), after the review, infers that the steps required for designing a commercial supply chains are scope, function, tools, and performance measures. Based on these steps, the study proposes a methodology for designing HSCs, adding the implementation plan, considering resilience and agility abilities that should be considered in the HSC and accounting for the involved stakeholders.
- Scope: This phase evaluates or characterizes performance. HSCs should obtain a clear concept of the context of the situation and outline the objectives for designing the supply chain.
- Function: In this phase, causal relationships between performance variables should be investigated. For HSCs, this phase involves assessing the interactions between actors and establishing how these interactions should be conducted to achieve agility and resilience as HSCs.
- Tools: The type of tools that will be used to measure the effectiveness of the HSCs before implementation should be determined. Elgazzar et al. (2019) proposes various tools, such as simulation, fuzzy logic, mathematical programming, and regression. As in business-oriented SCs, a tool should be used to model HSCs. Several studies have discussed optimization in this field, especially regarding the transportation and distribution of medicines (Sabouhi et al. 2020; Cardona-Valdés et al. 2011; Papageorgiou et al. 2001); modeling with mathematical programming (Salman Habib et al. 2016), stochastic programming and robust optimization, and considering uncertainty in disaster (Hazem and Nayeem 2021). These tools guarantee the agility of the HSCs, which ensures the delivery of products (vaccines) in a timely manner.
- Performance measures: Performance measures are relevant to evaluate if the HSCs are effective. In this phase, tools such as simulation or mathematical programming should be considered to minimize the costs or time required to deliver the vaccines to their final destinations, as well as social coverage, understood as the number of people benefited over time. Moreover, measures should consider the fact that the supply chain can be reconfigured in the case of unpredictable events (i.e., resilience).
- Implementation plan: This phase is outside of the scope of the review conducted by Elgazzar et al. (2019). However, in the case of the distribution of vaccines and given the urgency and unpredictability of this type of chain, the manner in which stakeholders interact should be specified due to the complexity of the organizational characteristics of humanitarian operations. For instance, bureaucracy can slow down operations (Tomasini and Van Wassenhove 2009). Therefore, integration and communication between stakeholders and processes are vital components for the appropriate and efficient function of the supply chain. This aspect can only be achieved with communication between processes and stakeholders (Mitchel and Kovach 2016).
Figure 8 provides a graphic illustration of the proposed methodology for designing HSCs and the involvement of HSC capabilities. The study proposes that these capabilities should be considered throughout the different stages to enable the effective formulation, implementation, and reconfiguration of the design.

Figure 8.
Methodology for humanitarian supply chains (Own elaboration, adapted from Elgazzar et al. 2019).
6.1. Design of the Supply Chain: Vaccine Strategy in Mexico
This section discusses the first two phases of the proposed methodology for designing the supply chain for the distribution of vaccines in Mexico. The choice of optimization tool and the definition of the performance metrics will be analyzed in detail in a future study. The literature provides optimization models that can be used in the distribution of the humanitarian supply chain; however, in Mexico, it is important that, in addition to these models, supply capacities are considered as well as the stakeholders involved, since the current strategy has not done this and is perceived negatively by society; furthermore, it has not reached the necessary coverage.
6.1.1. Scope
The objective of the supply chain is to distribute vaccines to the greatest number of people possible in the shortest possible time, considering the lifespan of the vaccine and the temperature conditions required to prevent its spoilage.
6.1.2. Function
The context was analyzed in Section 2 with the timeline of the COVID situation in Mexico. In addition, an analysis of stakeholders and their role in the distribution of vaccines was conducted in Section 4. The findings suggest that the government should establish the strategy with the help of public healthcare institutes and the federal healthcare system, not alone, and society’s perception of the strategy founded in the sentiment analysis is more negative than positive. Public healthcare institutes have limited themselves to the application of available vaccines wherever possible with political intent, but have not been considered in decision-making. However, this scenario has had an impact on agility and led citizens, the private sector, and the media to perceive the absence of a vaccination strategy and a delay in the application of vaccines. Moreover, a shift in priorities was perceived regarding which citizens should be immunized. As such, citizens lack appropriate information and encouragement to observe prevention measures, such as the use of facemasks, or lack awareness on the existing types of vaccines and their side effects. The population is wary of being vaccinated and dissatisfied about the external logistics of immunization facilities. Universities, which may propose solutions regarding the external distribution logistics, have not been considered. As such, the participation of several universities has been limited to the use of their infrastructure for healthcare personnel. In addition, the population has been divided, because only healthcare professionals from the public sector have been vaccinated, excluding doctors and nurses from private clinics. In summary, the private sector has been excluded and restrained from participating in vaccine acquisition or logistic support. Figure 9 depicts the most suitable function of the supply chain for the distribution of vaccines in Mexico.
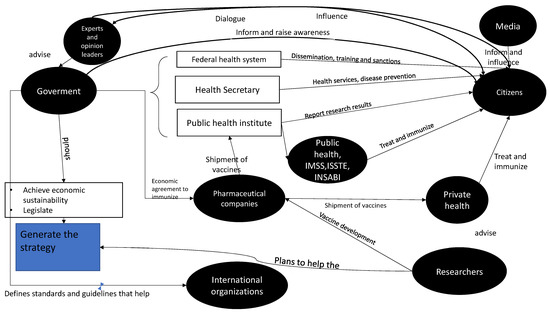
Figure 9.
Stakeholders of vaccine distribution through the humanitarian supply chain in Mexico. Adapted from the World Health Organization (World Health Organization 2012).
Among the suggested functions of this chain, establishing a council with the participation of public and private institutions, researchers, and the government is important to enable collaboration in a vaccination strategy given the current pandemic, or any kind of future sanitary emergency. The collaboration should also consider the immunized population and the methods and entities required for the acquisition and application of vaccines. Lastly, support should be given to the formulation and manufacture of vaccines in Mexico. Since it is not a producer of vaccines, Mexico has had to negotiate the purchase of vaccines from producing countries. Although COVAX is a WHO initiative that promotes the equitable distribution of vaccines, these have not arrived in the planned time and quantities, which has also hampered vaccination. As a positive aspect, it should be noted that the groups chosen for vaccination have been treated equally, regardless of their economic and social condition. However, we highlight the need for Mexico to aim to be a producer of vaccines. This would make vaccination more agile and even cheaper in our country. At this point, universities and private entities should be invited to aid in logistics.
6.1.3. Tools
Different techniques can be used to address HSC, where demand can be maximized and costs minimized. There are even multi-objective problems at present. Deterministic and non-deterministic integer programming, such as fuzzy logic and simulation, can be used. Some review papers were analyzed to search for the model and algorithms that can be used to solve the problem. Manopiniwes and Irohara (2014) provide a review of the optimization models used in the HSC. These authors found that the problems related to the distribution of humanitarian aid can be classified into facility location, distribution model, and inventory. We found that most of the articles focus on a post-disaster perspective and very few are from the stochastic perspective.
Salman Habib et al. (2016) study mathematical contributions by classifying the HSC problem into facility location, relief distribution, and mass evacuation, contrary to the previous study, where they observed that the investigations focused more on the pre-disaster and during the disaster period than the post-disaster period. Very few articles integrated all the phases due to their complexity, as they can be deterministic and consider restrictions not attached to reality (unrealistic assumptions). Behl and Dutta (2019) reviewed articles from 2011 to 2017, classifying them into different topics: theory-focused research, case studies, mathematical models, and HSC properties and resources needed, concluding that it is necessary to add the role of stakeholders, with the inclusion of qualitative methods, that is, mixed approaches.
Hazem and Nayeem (2021) reviewed articles from 2000 to 2020, and focused on mathematical models in HCS, classifying the chain into three main problems: facility location problem, relief distribution and mass evacuation, in deterministic and non-deterministic problems. They also found that the response phase (disaster) is the most addressed phase, and the post-disaster phase continues to receive the least attention. Other studies, such as that by Hu et al. (2019), focus on a particular problem, such as the optimization of the delivery of emergency material, concentrating on the optimization model and the applied algorithms, presenting both mathematical and heuristic methods. We need to rely on the vaccine distribution optimization model and the exact and heuristic algorithms needed to solve it. In the current study, we research methods to forecast the demand for vaccines, to focus on the model. We believe that our model will be able to use mathematical programming for transportation, warehousing, and vaccine distribution to ensure the agility of HSCs and stochastic programming to consider the risks and different scenarios for achieving agility and resilience; this was added to the article in lines.
6.1.4. Performance Measures
This phase aims to minimize the costs and time required to transport vaccines to their destination and achieve the highest coverage of the vaccinated population. Moreover, the supply chain can be reconfigured in the future in the case of unpredicted events to promote resilience. For that reason, different scenarios should be considered.
6.1.5. Implementation Plan
In this phase, the interaction of each actor should be specified and outlined after the optimization of HSCs, given the complexity of organizational characteristics in humanitarian operations, especially in Mexico.
7. Conclusions and Future Research
This paper presents a methodology for designing the humanitarian supply chains (HSCs) for immunization in Mexico. A context and documentary analysis was conducted of the vaccination strategy. As far as we know, no methodology has been applied to carry out immunization. The study cited a literature review on the capabilities that manufacturing supply chains require, and which of these capabilities should be considered for a supply chain dedicated to the distribution of vaccines, that is, agility and resilience. Thus, the present study conducted an analysis of the stakeholders and their role in the distribution of vaccines in relation to the capabilities. Considering these capabilities and stakeholders to propose a methodology for designing HSC is an innovative aspect of the study. To the best of our knowledge, no study has discussed the design of the vaccine supply chain considering the capabilities and stakeholders involved.
In the case of Mexico, given that the vaccination strategy has not worked as expected, before deliberating on optimization models, it is necessary to consider the stakeholders and context. The study aims to generate a methodology for designing HSCs to provide solutions in a highly dynamic environment that is full of complexity, where the strategy has been perceived as ineffective. This methodology can be applied not only to vaccine distribution, but also to other disasters that involve HSC.
According to the sentiment analysis of opinions from different news websites, the results indicate that the predominant emotions were negative. The study observed that the frequency of negative emotions declined when the application of the vaccines began (RQ1). Moreover, Mexico is perceived to lack a strategy, and vaccine distribution is perceived to be politicized. Some of the most important problems have been the centralization of the vaccine application, low vaccination rate, and control from the Executive Power (RQ2).
The most important aspect or methodology highlighted by the study is the conjunction of the capabilities and roles of stakeholders. The capabilities that should be considered in the design of the vaccine distribution supply chain are agility and resilience (RQ3). Different stakeholders participate in the vaccine distribution, as described in Section 5.1, but the most important aspect is the collaboration between all of them (RQ4) Thus, the study suggests the establishment of a council to encourage the participation of public and private institutions, researchers, and the government. Through this collaboration, the council can decide on the vaccination strategy or any other strategies for sanitary emergencies. Agility and resilience can be achieved through collaboration between stakeholders and government support.
Some of the main problems observed in the vaccine strategy are as follows: single physical space per municipality for the vaccine application, shortage of vaccines, lack of regulation and penalization regarding several sanitary measures, and lack of an applied methodology for immunization. Regarding those aspects, this study proposed a methodology for designing HSCs considering capabilities such as agility and resilience, combined with an analysis of the role of stakeholders in the supply chain. To the best of our knowledge, studies that propose a methodology for designing HSCs are lacking. The main contribution to the literature focuses on optimization models for the distribution of food or medicine in the HSC. Additionally, the study provided an overview of the current situation of the pandemic in Mexico to solidify the context of the supply chain (RQ5). As a limitation, this study covered only the first two phases of the methodology, namely, scope and function. Therefore, future studies should focus on the optimization of supply points and mode of transportation, enhanced by mathematical and stochastic programming, so that the implementation plan can be brought to fruition.
Author Contributions
Conceptualization, E.S.H.G. and N.H.-G.; Data curation, K.S.C.; Formal analysis, E.S.H.G. and N.H.-G.; Funding acquisition, N.H.-G.; Investigation, E.S.H.G., N.H.-G. and K.S.C.; Methodology, E.S.H.G.; Writing—original draft, E.S.H.G. and K.S.C.; Writing—review & editing, E.S.H.G. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Institutional Review Board Statement
Not applicable.
Informed Consent Statement
Not Applicable.
Data Availability Statement
The sentiment analysis results are available in https://doi.org/10.6084/m9.figshare.16548078.
Conflicts of Interest
The authors declare no conflict of interest.
Notes
| 1 | COVAX is one of three pillars of the Access to COVID-19 Tools (ACT) Accelerator, which was launched in April by the World Health Organization (WHO), the European Commission, and France in response to the pandemic. Bringing together governments, global health organizations, manufacturers, scientists, private sector, civil society, and philanthropists, with the aim of providing innovative and equitable access to COVID-19 diagnostics, treatments, and vaccines (Berkley 2021), COVAX is a multilateral initiative to enable the development of COVID 19 vaccines and ensure that they are equitably distributed in low- and middle-income countries. According to Eccleston-Turner and Upton (2021), despite the fact that, through this initiative, the development of vaccines has been accelerated, these benefits do not flow to low- and middle-income countries because of the vaccine nationalism of manufacturing countries. Baker-Sheikh et al. (2021) agrees that it is nationalism that has led to vaccines not being distributed to countries that are not producers and do not have the necessary resources. Between populations and communities, it is necessary to attend to those who are at greater risk of being infected, regardless of their country or economic condition. |
| 2 | NITAGs provide scientific recommendations to their respective ministries of health to enable them to make evidence-based immunization-related policy and program decisions (World Health Organization 2010). |
| 3 | The Federal Commission for the Protection against Sanitary Risks is the English translation of COFEPRIS. Its mission is to protect the population against health risks caused by the use and consumption of goods and services, health supplies, and exposure to factors such as environmental and labor issues, as well as the occurrence of health emergencies and provision of health services through the regulation, control, and prevention of health risks (Gobierno de México 2019a). |
| 4 | Alfredo Paredes, the CEO of Capitol Consulting & Communication and an expert in strategic communication, mentions that the president, at the beginning of the pandemic, made statements such as “COVID-19 did not infect the poor, we are prepared, and we will get out of the situation quickly”, in an effort to communicate that the country would recover quickly and that the country had no cause for worry. The message from the president is that the 4T (4th transformation) remains solid and firm, and the use of face masks would be a symbol of economic recession and of job loss. These statements cited these reasons, apart from giving points to his adversaries, which he does not want to assume. |
| 5 | The servants of the nation (Siervos de la Nación in Spanish) is a group that promotes the reelection of the current president and his party. |
References
- Alexa. 2021. Top Sites in Mexico. Available online: https://www.alexa.com/topsites/countries/MX (accessed on 14 June 2021).
- Ali, Imran, Sev Nagalingam, and Bruce Gurd. 2017. Building Resilience in SMEs of Perishable Product Supply Chains: Enablers, Barriers and Risks. Production Planning and Control 28: 1236–50. [Google Scholar] [CrossRef]
- Altay, Nezih, Angappa Gunazekaran, Rameshwar Dubey, and Stephen J. Childe. 2018. Agility and Resilience as antecedents of Supply. Production Planning & Control: The Management of Operation 29: 1–17. [Google Scholar] [CrossRef]
- Animal Político. 2021. Vacunas COVID: Las Autorizadas, sus dosis y a quiénes se destinarán en Mexico. Animal Político. February 20. Available online: https://www.animalpolitico.com/2021/02/vacunas-covid-las-autorizadas-sus-dosis-y-a-quienes-se-destinaran-en-mexico/ (accessed on 23 April 2021).
- Badillo, Diego. 2021. Los costos de la lenta campaña de vacunación contra la COVID-19 en Mexico. El Economista. March 21. Available online: https://www.eleconomista.com.mx/politica/Los-costos-de-la-lenta-campana-de-vacunacion-contra-la-COVID-19-en-Mexico-20210321-0001.html. (accessed on 3 May 2021).
- Baker-Sheikh, Abu, Suman Pal, Nismat Javed, and Rahul Shekar. 2021. COVID-19 Vaccination in Developing Nations: Challenges and Opportunities for Innovation. Infectious Disease Reports 13: 429–36. [Google Scholar] [CrossRef]
- Balcik, Burcu, Benita M. Beamon, Caroline C. Krejci, Kyle M. Muramatsu, and Magaly Ramirez. 2017. Coordination in humanitarian relief chains: Practices, challenges and opportunities. International Journal of Production Economics 126: 22–34. [Google Scholar] [CrossRef]
- Behl, Abhishek, and Pankaj Dutta. 2019. Humanitarian supply chain management: A thematic literature review and future directions of research. Annals of Operations Research 283: 1001–44. [Google Scholar] [CrossRef]
- Berkley, Seth. 2021. What is Covax? Gavi Vaccine Alliance. February 18. Available online: www.gavi.org/vaccineswork/covax-explained (accessed on 20 June 2021).
- Cardona-Valdés, Yajaira, Ada Álvarez, and Deniz Ozdemir. 2011. A bi-objective supply chain design problem with uncertainty. Transportation Research Part C: Emerging Technologies 19: 821–32. [Google Scholar] [CrossRef]
- Carvalho, Helena, Susana Azevedo, and Virgilio Cruz-Machado. 2012. Agile and Resilient Approaches to Supply Chain Management: Influence on Performance and Competitiveness. Logistics Research 4: 49–62. [Google Scholar] [CrossRef]
- Centers for Disease Control and Prevention. 2021. Pfizer-BioNTech COVID-19 Vaccine Overview and Safety. April 16. Available online: https://www.cdc.gov/coronavirus/2019-ncov/vaccines/different-vaccines/Pfizer-BioNTech.html (accessed on 23 April 2021).
- Centro Mario Molina. 2020. Cubrebocas y Transmisión de COVID-19. June 10. Available online: https://centromariomolina.org/identificando-la-transmision-por-aire-como-la-principal-fuente-de-contagio-para-covid-19/ (accessed on 23 April 2021).
- Checkland, Peter. 1999. Systems Thinking, Systems Practice. New York: John Wiley and Sons. [Google Scholar]
- Daen, Arturo, and Samedi Aguirre. 2021. Uso de cubrebocas evoluciona en el mundo, mientras en México aún se cuestiona su eficacia. Animal Político. February 20. Available online: https://www.animalpolitico.com/elsabueso/cubrebocas-efectividad-contagios-uso-mundo-mexico/ (accessed on 23 June 2021).
- Day, Jamison M. 2014. Fostering Emergent Resilience: The Complex Adaptive Supply Network of Disaster Relief. International Journal of Production Research 52: 1970–88. [Google Scholar] [CrossRef]
- Defee, C. Clifford, and Brian S. Fugate. 2010. Changing perspective of capabilities in the dynamic supply chain era. International Journal of Logistics Management 21: 180–206. [Google Scholar] [CrossRef]
- Eccleston-Turner, Mark, and Harry Upton. 2021. International Collaboration to Ensure Equitable Access to Vaccines for COVID-19: The ACT-Accelerator and the COVAX Facility. The Milkbank Quarterly 99: 426–49. [Google Scholar] [CrossRef]
- Elgazzar, Sara, Nicoleta Tipi, and Glynis Jones. 2019. Key characteristics for designing. International Journal of Productivity and Performance Management 69: 296–318. [Google Scholar] [CrossRef] [Green Version]
- Expansión Política. 2020. Universidades ofrecen su equipo y personal para aplicar la vacuna COVID-19. Expansión Política. December 7. Available online: https://politica.expansion.mx/mexico/2020/12/07/universidades-ofrecen-su-equipo-y-personal-para-aplicar-la-vacuna-covid-19 (accessed on 3 May 2021).
- Expansión Política. 2021. Tras elecciones, se cumplen dos semanas con baja en aplicación de vacunas COVID. Expansión Política. June 21. Available online: https://politica.expansion.mx/mexico/2021/06/21/tras-elecciones-se-cumplen-dos-semanas-con-baja-en-aplicacion-de-vacunas-covid (accessed on 28 September 2021).
- Forbes. 2021. México es el tercer país con más muertes por COVID-19 en el mundo. Forbes México. April 20. Available online: https://www.forbes.com.mx/mexico-es-el-tercer-pais-con-mas-muertes-por-covid-19-en-el-mundo/ (accessed on 4 May 2021).
- Gobierno de México. 2019a. Comisión Federal contra Riesgos Sanitarios: ¿Qué hacemos? Available online: https://www.gob.mx/cofepris/que-hacemos (accessed on 18 February 2021).
- Gobierno de México. 2019b. Secretaría de Salud: ¿Qué hacemos? Available online: https://www.gob.mx/salud/que-hacemos (accessed on 18 February 2021).
- Gobierno de México. 2019c. Bienvenida INSP. Available online: https://www.insp.mx/el-instituto.html (accessed on 18 February 2021).
- Gobierno de México. 2021a. Guía Técnica para para la aplicación de la vacuna. February 20. Available online: https://coronavirus.gob.mx/wp-content/uploads/2021/03/GTApp_SputnikV_050321.pdf (accessed on 23 April 2021).
- Gobierno de México. 2021b. Guía Tecnica para la Aplicación de la Vacuna Recombinante del Vector de Adenovirus Tipo 5 contra el Virus SARS-Cov 2 de Cansino Biologics. March 16. Available online: https://coronavirus.gob.mx/wp-content/uploads/2021/03/GTApp_Cansino_16Mar2021.pdf (accessed on 23 April 2021).
- Hazem, Ibrahim M., and Moddassir K. Nayeem. 2021. A Systematic Literature Review on Mathematical Models of Humanitarian Logistics. Symmetry 13: 11. [Google Scholar] [CrossRef]
- Hu, Hui, Jing He, Xiongfei He, Wanli Yang, Jing Nie, and Bin Ran. 2019. Emergency material scheduling optimization model and algorithms: A review. Journal of Traffic Transportation Engineering 6: 441–54. [Google Scholar] [CrossRef]
- Huerta, Por Juan Carlos. 2021. ¡Atención, comunidad de la UdeG! Podrán participar en la estrategia de vacunación COVID. El Financiero. January 21. Available online: https://www.elfinanciero.com.mx/estados/atencion-comunidad-de-la-udeg-podran-participar-en-la-estrategia-de-vacunacion-covid (accessed on 3 May 2021).
- Infobae. 2020. El uso del cubrebocas: La polémica que ha seguido a López-Gatell durante toda la pandemia Infobae. November 20. Available online: https://www.infobae.com/america/mexico/2020/11/19/el-uso-del-cubrebocas-la-polemica-que-ha-seguido-a-lopez-gatell-durante-toda-la-pandemia/ (accessed on 23 April 2021).
- Leyva, Juan. 2021. Vacunas COVID 19 que se están aplicando en México. Debate. March 15. Available online: https://www.debate.com.mx/salud/Vacunas-COVID-19-que-se-estan-aplicando-en-Mexico-20210315-0110.htm (accessed on 28 September 2021).
- L’Hermitte, Cécile, Peter Tatham, Marcus Bowles, and Ben Brooks. 2016. Developing organisational capabilities to support agility in humanitarian logistics: An exploratory study. Journal of Humanitarian Logistics and Supply Chain Management 6: 72–99. [Google Scholar] [CrossRef]
- Malmir, Behnam, and Christopher W. Zobel. 2021. An applied approach to multi-criteria humanitarian supply chain planning for pandemic response. Journal of Humanitarian Logistics and Supply Chain Management 11: 320–46. [Google Scholar] [CrossRef]
- Manopiniwes, Wapee, and Takashi Irohara. 2014. A Review of Relief Supply Chain Optimization. Industrial Engineering & Management Systems 13: 1–14. [Google Scholar] [CrossRef]
- MarcaClaro. 2021. Vacuna COVID-19 Mexico hoy 23 de abril: ¿Cuántas dosis se han aplicado y cuántos casos de coronavirus van al momento? April 23. Available online: https://www.marca.com/claro-mx/trending/coronavirus/2021/04/23/6082366f268e3e7b098b460a.html (accessed on 24 April 2021).
- Methodology for Designing Humanitarian Supply Chains Distribution of COVID-19 Vaccines in Mexico. 2021. Available online: https://doi.org/10.6084/m9.figshare.16548078 (accessed on 6 November 2021).
- Mishra, Jyoti, Kudzai Chiwenga, Nishikant Mishra, and Sonal Choudhary. 2020. Extending dynamic capabilities towards lean thinking in humanitarian supply chains. Production Planning and Control 4: 1–22. [Google Scholar] [CrossRef]
- Mitchel, Erin M., and Jamison V. Kovach. 2016. Improving supply chain information sharing using Design for Six Sigma. European Research on Management and Business Economics 22: 147–54. [Google Scholar] [CrossRef] [Green Version]
- Navarro, María Fernanda. 2020. El uso (político) del cubrebocas en México. Forbes México. July 24. Available online: https://www.forbes.com.mx/el-uso-politico-del-cubrebocas-en-mexico/ (accessed on 23 April 2021).
- Papageorgiou, Lazaros, Guillermo Rotstein, and Nilay Shah. 2001. Strategic supply chain optimization for the pharmaceutical industries. Industrial & Engineering Chemistry Research 40: 275–86. [Google Scholar] [CrossRef]
- Polater, Abdussamet. 2020. Dynamic capabilities in humanitarian supply chain management: A systematic literature review. Journal of Humanitarian Logistics and Supply Chain Management 11: 46–80. [Google Scholar] [CrossRef]
- Ponomarov, Serhiy Y., and Mary C. Holcomb. 2009. Understanding the Concept of Supply Chain Resilience. The International Journal of Logistics Management 20: 124–43. [Google Scholar] [CrossRef]
- Prakash, Chandra, Maria Besiou, Parikshit Chara, and Sumeet Gupta. 2020. Organization theory in humanitarian operations: A review and suggested research agenda. Journal of Humanitarian Logistics and Supply Chain Management 10: 261–84. [Google Scholar] [CrossRef]
- Purvis, L., S. Spall, M. Naim, and Virginia Spiegler. 2016. Developing a Resilient Supply Chain Strategy during ‘Boom’ and ‘Bust’. Production Planning and Control 27: 579–90. [Google Scholar] [CrossRef]
- Ramos, Y., and E. Contreras. 2021. La vacunación contra COVID-19 en Mexico está en la quinta etapa, que incluye a personas de 16 a 39 años. ¿Cómo avanza la inmunización en el país? Serindipia. August 27. Available online: https://serendipia.digital/covid-19/cuantas-vacunas-contra-covid-ha-aplicado-mexico/ (accessed on 28 August 2021).
- Sabouhi, Mohammad Saeed-Jabalameli Fatemeh, Armin Jabbarzadeh, and Behnam Fahimnia. 2020. A multi-cut L-shaped method for resilient and responsive supply chain network design. International Journal of Production Research 58: 7353–81. [Google Scholar] [CrossRef]
- Salman Habib, Muhammad, Young Hae Lee, and Muhammad Saad Memon. 2016. Mathematical Models in Humanitarian Supply Chain Management: A Systematic Literature Review. Mathematical Problems in Engineering 2016: 3212095. [Google Scholar] [CrossRef] [Green Version]
- Sánchez, Cano Alejo. 2021. Fracaso en la aplicación de la vacuna. El Financiero. January 19. Available online: https://www.elfinanciero.com.mx/opinion/alejo-sanchez-cano/fracaso-en-la-aplicacion-de-la-vacuna/ (accessed on 3 May 2021).
- Secretaria de Salud. 2020. Estrategia de Prevención de la Salud, Prevención, Atención y Mitigación de la Covid 19 en el Marco de la Atención Primaria de Salud. July 24. Available online: https://coronavirus.gob.mx/wp-content/uploads/2020/10/APS_COVID_v17_08_2020.pdf (accessed on 18 February 2021).
- Sheu, Jiu-Biing. 2010. Dynamic relief-demand management for emergency logistics operations under Large-Scale Disasters. Transportation Research Part E: Logistics and Transportation Review 46: 1–17. [Google Scholar] [CrossRef]
- Singh, Rajesh Kumar, Ayush Gupta, and Angappa Gunasekaran. 2018. Analyzing the interaction of factors for resilient humanitarian supply chain. International Journal of Production Research 56: 6809–27. [Google Scholar] [CrossRef]
- Sokat, Kezban Yagci, and Nezih Altay. 2021. Serving vulnerable populations under the threat of epidemics and pandemics. Journal of Humanitarian Logistics and Supply Chain Management 11: 176–97. [Google Scholar] [CrossRef]
- Statista. 2021a. Coronavirus COVID-19 Global Cases by Johns Hopkins CSSE. August 27. Available online: https://0-www-statista-com.biblioteca-ils.tec.mx/statistics/1101643/latin-america-caribbean-coronavirus-cases/ (accessed on 27 August 2021).
- Statista. 2021b. Share of the Population Partially or Fully Vaccinated against COVID-19 in Mexico. August 27. Available online: https://0-www-statista-com.biblioteca-ils.tec.mx/statistics/1104529/population-vaccinated-against-covid-19-mexico/ (accessed on 27 August 2021).
- Tablakar, Tunca. 2017. Scalability and Resilience in Humanitarian Supply Chains, 1st ed. Helsinki: Hanken School of Economics, Available online: https://helda.helsinki.fi/dhanken/bitstream/handle/123456789/172374/319%20-%20Tabaklar.pdf?sequence=1 (accessed on 6 November 2021).
- Tomasini, Rolando, and Luk Van Wassenhove. 2009. Humanitarian Logistics. London: Palgrave. [Google Scholar]
- Van Wassenhove, Luk. 2006. Humanitarian aid logistics: Supply chain management in high gear. Journal of the Operational Research Society 57: 475–89. [Google Scholar] [CrossRef]
- Varela, Micaela. 2021. Los maestros de Chiapas, Nayarit, Veracruz, Tamaulipas y Coahuila recibirán la vacuna china de CanSino. El País. April 16. Available online: https://elpais.com/mexico/2021-04-16/los-maestros-de-chiapas-nayarit-veracruz-tamaulipas-y-coahuila-recibiran-la-vacuna-china-de-cansino.html (accessed on 23 April 2021).
- World Health Organization. 2010. National Immunization Technical Advisory Groups (NITAGs). Available online: https://www.who.int/immunization/sage/national_advisory_committees/en/ (accessed on 18 February 2021).
- World Health Organization. 2012. Global Vaccine Action Plan Annex 2: Stakeholder. Available online: https://www.who.int/immunization/global_vaccine_action_plan/GVAP_Annex2.pdf (accessed on 18 February 2021).
- World Health Organization. 2017. Stakeholder Management. Available online: https://www.euro.who.int/en/health-topics/disease-prevention/vaccines-and-immunization/publications/2017/stakeholder-management-2017 (accessed on 18 February 2021).
- World Health Organization. 2020. Mask Use in the Context of COVID-19 Interim Guidance. December 1. Available online: https://apps.who.int/iris/bitstream/handle/10665/337199/WHO-2019-nCov-IPC_Masks-2020.5-eng.pdf?sequence=1&isAllowed=y (accessed on 23 April 2021).
- Xímenez Fyvie, Laurie Ann. 2021. Un daño irreparable: La criminal gestión de la pandemia en Mexico. Mexico: Planeta. [Google Scholar]
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).