Income and Self-Rated Mental Health: Diminished Returns for High Income Black Americans



Abstract
:1. Introduction
2. Methods
2.1. Design and Setting
2.2. Sampling Eligibility
2.3. Sampling Procedure
2.4. Data Collection
2.5. Interviewer Training
2.6. Ethical Considerations
2.7. Measures
2.7.1. Independent Variable
2.7.2. Dependent Variable
2.7.3. Covariates
2.7.4. Moderator
2.8. Statistical Analysis
3. Results
3.1. Descriptive Statistics
3.2. Bivariate Correlations
3.3. Logistic Regressions in the Overall Sample
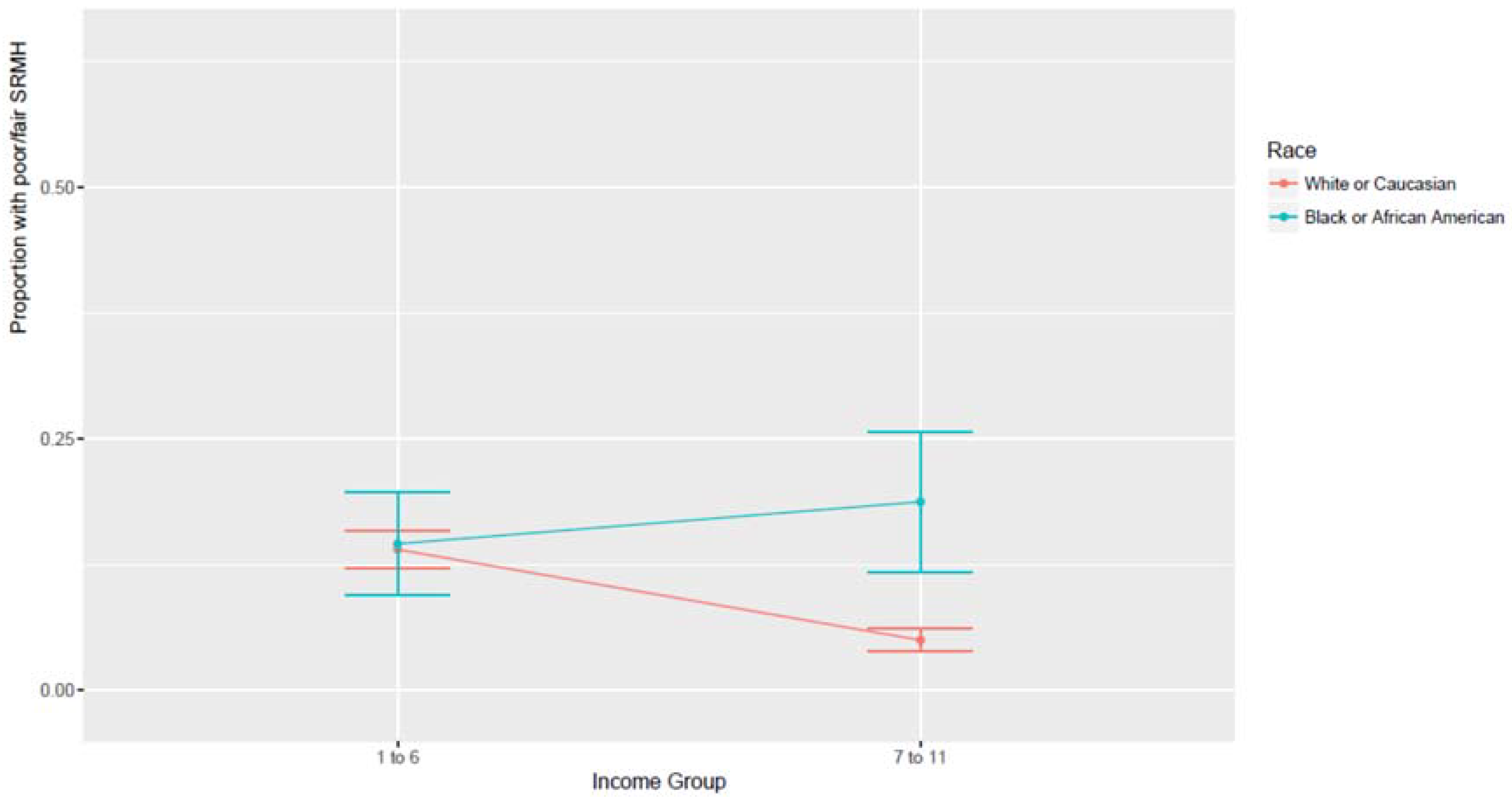
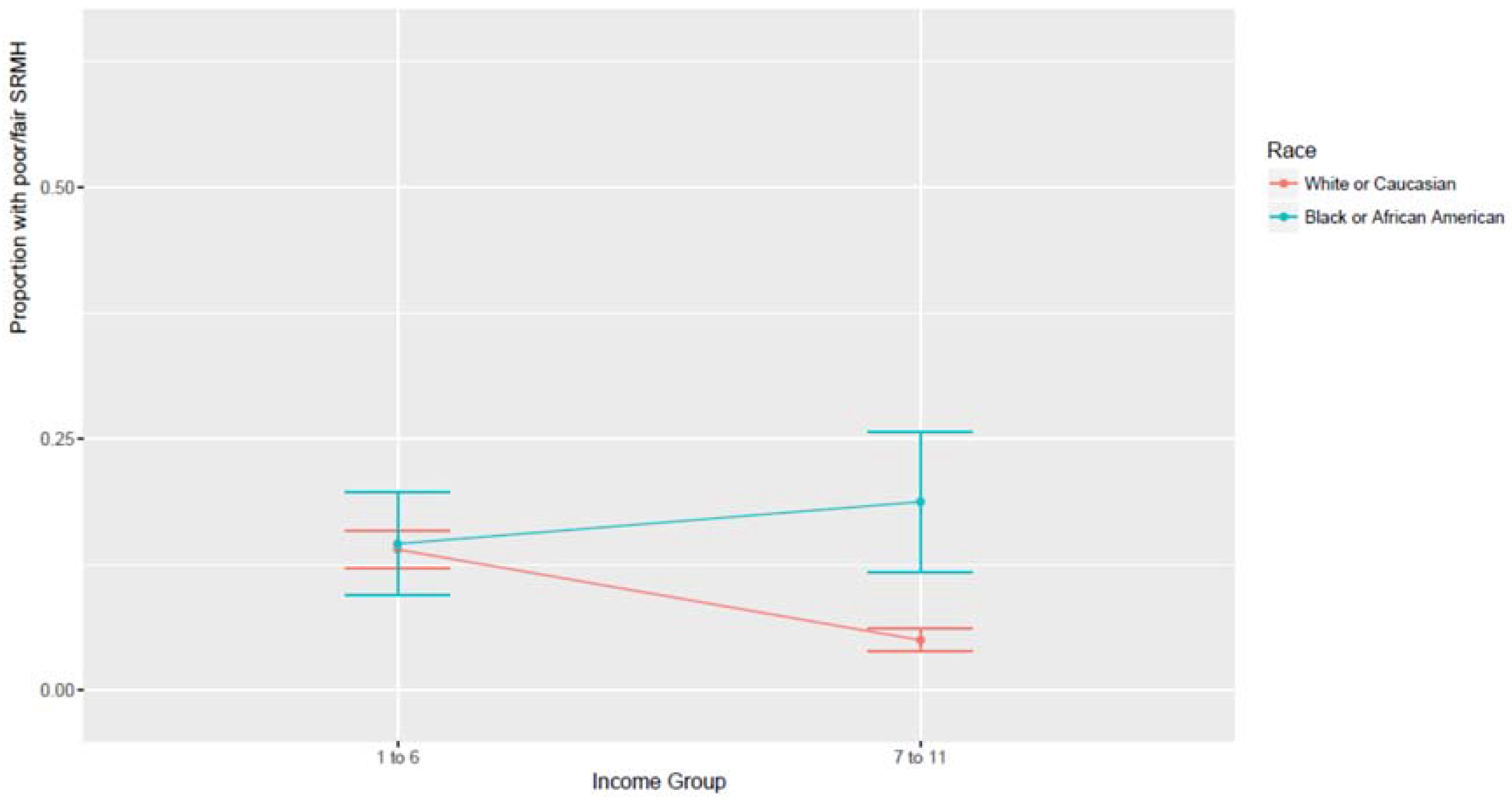
3.4. Logistic Regressions by Race/Ethnicity
4. Discussion
Limitations
5. Conclusions
Author Contributions
Acknowledgments
Conflicts of Interest
Appendix A. State of the State Survey (SOSS) Consent
Appendix B. State of the State Survey (SOSS) Regions
- Upper Peninsula: Alger, Baraga, Chippewa, Delta, Dickinson, Gogebic, Houghton, Iron, Keweenaw, Luce, Ontonagon, Mackinac, Marquette, Menominee, Schoolcraft
- Northern Lower Peninsula: Alcona, Alpena, Antrim, Benzie, Charlevoix, Cheboygan, Crawford, Emmet, Grand Traverse, Iosco, Kalkaska, Leelanau, Missaukee, Montmorency, Ogemaw, Oscoda, Otsego, Presque Isle, Roscommon, Wexford
- West Central: Allegan, Barry, Ionia, Kent, Lake, Manistee, Mason, Mecosta, Montcalm, Muskegon, Newaygo, Oceana, Osceola, Ottawa
- East Central: Arenac, Bay, Clare, Clinton, Gladwin, Gratiot, Huron, Isabella, Midland, Saginaw, Sanilac, Shiawassee, Tuscola
- Southwest: Berrien, Branch, Calhoun, Cass, Eaton, Hillsdale, Ingham, Jackson, Kalamazoo, St. Joseph, Van Buren
- Southeast: Genesee, Lapeer, Lenawee, Livingston, Macomb, Monroe, Oakland, St. Clair, Washtenaw, Wayne [excluding Detroit]
- Detroit
References
- Marmot, M.G.; Shipley, M.J. Do socioeconomic differences in mortality persist after retirement? 25 year follow up of civil servants from the first Whitehall study. Br. Med. J. 1996, 313, 1170–1180. [Google Scholar] [CrossRef]
- Van Groenou, M.I.B.; Deeg, D.J.; Penninx, B.W. Income differentials in functional disability in old age: Relative risks of onset, recovery, decline, attrition and mortality. Aging Clin. Exp. Res. 2003, 15, 174–183. [Google Scholar] [CrossRef]
- Berkman, C.S.; Gurland, B.J. The relationship among income, other socioeconomic indicators, and functional level in older persons. J. Aging Health 1998, 10, 81–98. [Google Scholar] [CrossRef] [PubMed]
- Baker, D.P.; Leon, J.; Smith Greenaway, E.G.; Collins, J.; Movit, M. The education effect on population health: A reassessment. Popul. Dev. Rev. 2011, 37, 307–332. [Google Scholar] [CrossRef] [PubMed]
- Morris, J.K.; Cook, D.G.; Shaper, A.G. Loss of employment and mortality. Br. Med. J. 1994, 308, 1135–1139. [Google Scholar] [CrossRef]
- Burgard, S.A.; Elliott, M.R.; Zivin, K.; House, J.S. Working conditions and depressive symptoms: A prospective study of US adults. J. Occup. Environ. Med. 2013, 55, 1007–1014. [Google Scholar] [CrossRef] [PubMed]
- Brodish, P.H.; Massing, M.; Tyroler, H.A. Income inequality and all cause mortality in the 100 counties of North Carolina. South Med. J. 2000, 93, 386–391. [Google Scholar] [CrossRef] [PubMed]
- Herd, P.; Goesling, B.; House, J.S. Socioeconomic position and health: The differential effects of education versus income on the onset versus progression of health problems. J. Health Soc. Behav. 2007, 48, 223–238. [Google Scholar] [CrossRef] [PubMed]
- Lowry, R.; Kann, L.; Collins, J.L.; Kolbe, L.J. The effect of socioeconomic status on chronic disease risk behaviors among US adolescents. J. Am. Med. Assoc. 1996, 276, 792–797. [Google Scholar] [CrossRef]
- Callan, M.J.; Kim, H.; Matthews, W.J. Predicting self-rated mental and physical health: The contributions of subjective socioeconomic status and personal relative deprivation. Front. Psychol. 2015, 6, 1415. [Google Scholar] [CrossRef] [PubMed]
- Meyer, O.L.; Castro-Schilo, L.; Aguilar-Gaxiola, S. Determinants of mental health and self-rated health: A model of socioeconomic status, neighborhood safety, and physical activity. Am. J. Public Health 2014, 104, 1734–1741. [Google Scholar] [CrossRef] [PubMed]
- Assari, S.; Lankarani, M.M. Demographic and Socioeconomic Determinants of Physical and Mental Self-rated Health across 10 Ethnic Groups in the United States. Int. J. Epidemiol. Res. 2017, 4, 185–193. [Google Scholar]
- Lorant, V.; Deliège, D.; Eaton, W.; Robert, A.; Philippot, P.; Ansseau, M. Socioeconomic inequalities in depression: A meta-analysis. Am. J. Epidemiol. 2003, 157, 98–112. [Google Scholar] [CrossRef] [PubMed]
- Assari, S. Ethnic and Gender Differences in Additive Effects of Socio-economics, Psychiatric Disorders, and Subjective Religiosity on Suicidal Ideation among Blacks. Int. J. Prev. Med. 2015, 6, 53. [Google Scholar] [CrossRef] [PubMed]
- Rehkopf, D.H.; Buka, S.L. The association between suicide and the socio-economic characteristics of geographical areas: A systematic review. Psychol. Med. 2006, 36, 145–157. [Google Scholar] [CrossRef] [PubMed]
- Purselle, D.C.; Heninger, M.; Hanzlick, R.; Garlow, S.J. Differential association of socioeconomic status in ethnic and age-defined suicides. Psychiatry Res. 2009, 167, 258–265. [Google Scholar] [CrossRef] [PubMed]
- Goodman, E.; Huang, B. Socioeconomic status, depressive symptoms, and adolescent substance use. Arch. Pediatr. Adolesc. Med. 2002, 156, 448–453. [Google Scholar] [CrossRef] [PubMed]
- Assari, S. Combined racial and gender differences in the long-term predictive role of education on depressive symptoms and chronic medical conditions. J. Racial Ethn. Health Dispar. 2016, 4, 385–396. [Google Scholar] [CrossRef] [PubMed]
- Assari, S.; Lankarani, M.M. Race and urbanity alter the protective effect of education but not income on mortality. Front. Public Health 2016, 4, 100. [Google Scholar] [CrossRef] [PubMed]
- Assari, S.; Lankarani, M.M. Education and alcohol consumption among older Americans. Black-White Differences. Front. Public Health 2016, 4, 67. [Google Scholar] [CrossRef] [PubMed]
- Assari, S. Health Disparities Due to Diminished Return among Black Americans: Public Policy Solutions. Soc. Issues Policy Rev. 2018, 12, 112–145. [Google Scholar] [CrossRef]
- Assari, S. Unequal gain of equal resources across racial groups. Int. J. Health Policy Manag. 2017, 6, 1–6. [Google Scholar] [CrossRef] [PubMed]
- Assari, S. Life expectancy gain due to employment status depends on race, gender, education, and their intersections. J. Racial Ethn. Health Dispar. 2018, 5, 375–386. [Google Scholar] [CrossRef] [PubMed]
- Assari, S.; Caldwell, C.H. Social Determinants of Perceived Discrimination among Black Youth: Intersection of Ethnicity and Gender. Children 2018, 5, 24. [Google Scholar] [CrossRef] [PubMed]
- Assari, S.; Thomas, A.; Caldwell, C.H.; Mincy, R.B. Blacks’ Diminished Health Return of Family Structure and Socioeconomic Status; 15 Years of Follow-up of a National Urban Sample of Youth. J. Urban Health 2017, 95, 21–35. [Google Scholar] [CrossRef] [PubMed]
- Assari, S. Social Determinants of Depression: The Intersections of Race, Gender, and Socioeconomic Status. Brain Sci. 2017, 7, 156. [Google Scholar] [CrossRef] [PubMed]
- Farmer, M.M.; Ferraro, K.F. Are racial disparities in health conditional on socioeconomic status? Soc. Sci. Med. 2005, 60, 191–204. [Google Scholar] [CrossRef] [PubMed]
- Assari, S. The Benefits of Higher Income in Protecting against Chronic Medical Conditions Are Smaller for African Americans than Whites. Healthcare 2018, 6, 2. [Google Scholar] [CrossRef] [PubMed]
- Holzer, C.; Shea, B.; Swanson, J.; Leaf, P.; Myers, J.; George, L.; Weissman, M.; Bednarski, P. The increased risk for specific psychiatric disorders among persons of low socioeconomic status: Evidence from the Epidemiologic Catchment Area Surveys. Am. J. Soc. Psychiatry 1986, 4, 259–271. [Google Scholar]
- Weissman, M.; Bruce, M.; Leaf, P.; Florio, L.; Holzer, C. Affective Disorders. In Psychiatric Disorders in America; Robins, K., Reiger, D., Eds.; The Free Press: New York, NY, USA, 1991; pp. 53–80. [Google Scholar]
- Reiger, D.; Farmer, M.; Rae, D.; Myers, J.; Kramer, M.; Robins, L.; George, L.; Karno, M.; Locke, B. One-month prevalence of mental disorders in the United States and sociodemographic characteristics: The Epidemiologic Catchment Area study. Acta Psychiatr. Scand. 1993, 88, 35–47. [Google Scholar] [CrossRef]
- Alegria, M.; Bijl, R.; Lin, E.; Walters, E.; Kessler, R. Income differences in persons seeking outpatient treatment for mental disorders: A comparison of the United States with Ontario and the Netherlands. Arch. Gen. Psychiatry 2000, 57, 383–391. [Google Scholar] [CrossRef] [PubMed]
- Blazer, D.; George, K.; Landerman, R.; Pennybacker, M.; Melville, M.; Woodbury, M.; Manton, K.; Jordan, K.; Locke, B. Psychiatric disorders: A rural/urban comparison. Arch. Gen. Psychiatry 1985, 42, 651–656. [Google Scholar] [CrossRef] [PubMed]
- Leaf, P.; Weissman, M.; Myers, J.; Holzer, C.; Tischler, G. Psychosocial risks and correlates of major depression in one United States urban community. In Mental Disorders in the Community: Progress and Challenge; Barrett, D., Rose, R., Eds.; The Guilford Press: New York, NY, USA, 1986; pp. 47–66. [Google Scholar]
- Bruce, M.; Takeuchi, D.; Leaf, P. Poverty and psychiatric status: Longitudinal evidence from the New Haven Epidemiologic Catchment Area Study. Arch. Gen. Psychiatry 1991, 48, 470–474. [Google Scholar] [CrossRef] [PubMed]
- Kessler, R.; Zhao, S.; Blazer, D.; Swartz, M. Prevalence, correlates, and course of minor depression and major depression in the national comorbidity survey. J. Affect. Disord. 1997, 45, 19–30. [Google Scholar] [CrossRef]
- Kessler, R.; Berglund, P.; Demler, O.; Jin, R.; Koretz, D.; Merikangas, K.; Rush, J.; Walters, E.; Wang, P. The epidemiology of major depressive disorder: Results from the National Comorbidity Survey Replication (NCS-R). J. Am. Med. Assoc. 2003, 289, 3095–3105. [Google Scholar] [CrossRef] [PubMed]
- Assari, S.; Caldwell, C.H. High Risk of Depression in High-Income African American Boys. J. Racial Ethn. Health Dispar. 2017, 1–12. [Google Scholar] [CrossRef] [PubMed]
- Gavin, A.R.; Walton, E.; Chae, D.H.; Alegria, M.; Jackson, J.S.; Takeuchi, D. The associations between socio-economic status and major depressive disorder among Blacks, Latinos, Asians and non-Hispanic Whites: Findings from the Collaborative Psychiatric Epidemiology Studies. Psychol. Med. 2010, 40, 51–61. [Google Scholar] [CrossRef] [PubMed]
- State of the State Survey (SOSS). Institute for Public Policy and Social Research. Michigan State University. Available online: http://ippsr.msu.edu/survey-research/state-state-survey-soss/about-soss (accessed on 1 April 2018).
- Pierce, G.L. Methodological Report: Michigan State University State of the State Survey 74 (Spring 2017 Round); Institute for Public Policy and Social Research, Michigan State University: East Lansing, MI, USA, 2017. [Google Scholar]
- McDowell, I. Measuring Health: A Guide to Rating Scales and Questionnaires, 3rd ed.; Oxford University Press: New York, NY, USA, 2006. [Google Scholar]
- Assari, S.; Dejman, M.; Neighbors, H.W. Ethnic Differences in Separate and Additive Effects of Anxiety and Depression on Self-rated Mental Health Among Blacks. J. Racial Ethn. Health Dispar. 2016, 3, 423–430. [Google Scholar] [CrossRef] [PubMed]
- Phelan, J.C.; Link, B.G.; Diez-Roux, A.; Kawachi, I.; Levin, B. “Fundamental causes” of social inequalities in mortality: A test of the theory. J. Health Soc. Behav. 2004, 45, 265–285. [Google Scholar] [CrossRef] [PubMed]
- Link, B.G.; Northridge, M.E.; Phelan, J.C.; Ganz, M.L. Social epidemiology and the fundamental cause concept: On the structuring of effective cancer screens by socioeconomic status. Milbank Q. 1998, 76, 375–402. [Google Scholar] [CrossRef] [PubMed]
- Marmot, M.; Allen, J.J. Social determinants of health equity. Am. J. Public Health 2014, 104, S517–S519. [Google Scholar] [CrossRef] [PubMed]
- Braveman, P.; Gottlieb, L. The social determinants of health: It’s time to consider the causes of the causes. Public Health Rep. 2014, 129, 19–31. [Google Scholar] [CrossRef] [PubMed]
- Ross, C.; Mirowsky, J. Education, Social Status, and Health (Social Institutions and Social Change); Aldine Transaction: Piscataway, NJ, USA, 2003. [Google Scholar]
- Hayward, M.D.; Hummer, R.A.; Sasson, I. Trends and group differences in the association between educational attainment and U.S. adult mortality: Implications for understanding education’s causal influence. Soc. Sci. Med. 2015, 127, 8–18. [Google Scholar] [CrossRef] [PubMed]
- Backlund, E.; Sorlie, P.D.; Johnson, N.J. A comparison of the relationships of education and income with mortality: The national longitudinal mortality study. Soc. Sci. Med. 1999, 49, 1373–1384. [Google Scholar] [CrossRef]
- Everett, B.G.; Rehkopf, D.H.; Rogers, R.G. The nonlinear relationship between education and mortality: An examination of cohort, race/ethnic, and gender differences. Popul. Res. Policy Rev. 2013, 32, 893–917. [Google Scholar] [CrossRef] [PubMed]
- Cutler, D.M.; Lleras-Muney, A. Education and Health: Evaluating Theories and Evidence. National Bureau of Economic Research. Available online: Http://www.nber.org/papers/w12352/ (accessed on 9 September 2017).
- Holmes, C.J.; Zajacova, A. Education as “the great equalizer”: Health benefits for black and white adults. Soc. Sci. Q. 2014, 95, 1064–1085. [Google Scholar] [CrossRef]
- Williams, D.R.; Mohammed, S.A.; Leavell, J.; Collins, C. Race, Socioeconomic Status and Health: Complexities, Ongoing Challenges and Research Opportunities. Ann. N. Y. Acad. Sci. 2010, 1186, 69–101. [Google Scholar] [CrossRef] [PubMed]
- Duckett, P.; Artiga, S. Health Coverage for the Black Population Today and Under the Affordable Care Act; Henry, J., Ed.; Kaiser Family Foundation: San Francisco, CA, USA, 2013. [Google Scholar]
- Assari, S.; Caldwell, C.H.; Mincy, R. Family Socioeconomic Status at Birth and Youth Impulsivity at Age 15; Blacks’ Diminished Return. Children 2018, 5, 58. [Google Scholar] [CrossRef] [PubMed]
- Assari, S.; Mistry, R. Educational Attainment and Smoking Status in a National Sample of American Adults; Evidence for the Blacks’ Diminished Return. Int. J. Environ. Res. Public Health 2018, 15, 763. [Google Scholar] [CrossRef] [PubMed]
- Assari, S.; Lankarani, M.M. Blacks’ diminished return of education on fruit and Vegetable intake. J. 2018, in press. [Google Scholar]
- Assari, S.; Caldwell, C.H.; Mincy, R.B. Maternal Educational Attainment at Birth Promotes Future Self-Rated Health of White but Not Black Youth: A 15-Year Cohort of a National Sample. J. Clin. Med. 2018, 7, 93. [Google Scholar] [CrossRef] [PubMed]
- Assari, S. Socioeconomic Status and Self-Rated Oral Health; Diminished Return among Hispanic Whites. Dent. J. 2018, 6, 11. [Google Scholar] [CrossRef] [PubMed]
- Assari, S. Diminished Economic Return of Socioeconomic Status at Birth among Black than White Youth. Soc. Sci. 2018, 7, 74. [Google Scholar] [CrossRef]
- Parker, S.; Kleiner, R.J. The culture of poverty: An adjustive dimension. Am. Anthropol. 1970, 72, 516–527. [Google Scholar] [CrossRef]
- Neighbors, H.W.; Jackson, J.S.; Broman, C.; Thompson, E. Racism and the mental health of African Americans: The role of self and system blame. Ethn. Dis. 1996, 6, 167–175. [Google Scholar] [PubMed]
- Bronder, E.C.; Speight, S.L.; Witherspoon, K.M.; Thomas, A.J. John Henryism, depression, and perceived social support in Black women. J. Black Psychol. 2014, 40, 115–137. [Google Scholar] [CrossRef]
- Ryff, C.D.; Keyes, C.L.M. The structure of psychological well-being revisited. J. Pers. Soc. Psychol. 1995, 69, 719–727. [Google Scholar] [CrossRef] [PubMed]
- Keyes, C.L. The Black–White paradox in health: Flourishing in the face of social inequality and discrimination. J. Pers. 2009, 77, 1677–1706. [Google Scholar] [CrossRef] [PubMed]
- Steele, R.E. Relationship of race, sex, social class, and social mobility to depression in normal adults. J. Soc. Psychol. 1978, 104, 37–47. [Google Scholar] [CrossRef] [PubMed]
- Chen, E.; Martin, A.D.; Matthews, K.A. Understanding health disparities: The role of race and socioeconomic status in children’s health. Am. J. Public Health 2006, 96, 702–708. [Google Scholar] [CrossRef] [PubMed]
- Hudson, D.L.; Bullard, K.M.; Neighbors, H.W.; Geronimus, A.T.; Yang, J.; Jackson, J.S. Are benefits conferred with greater socioeconomic position undermined by racial discrimination among African American men? J. Men’s Health 2012, 9, 127–136. [Google Scholar] [CrossRef] [PubMed]
- Lampe, F.C.; Walker, M.; Lennon, L.T.; Whincup, P.H.; Ebrahim, S. Validity of a self-reported history of doctor-diagnosed angina. J. Clin. Epidemiol. 1999, 52, 73–81. [Google Scholar] [CrossRef]
- Assari, S.; Lankarani, M.M.; Burgard, S. Black-white difference in long-term predictive power of self-rated health on all-cause mortality in United States. Ann. Epidemiol. 2016, 26, 106–114. [Google Scholar] [CrossRef] [PubMed]
- Assari, S.; Burgard, S.; Zivin, K. Long-term reciprocal associations between depressive symptoms and number of chronic medical conditions: Longitudinal support for black-white health paradox. J. Racial Ethn. Health Dispar. 2015, 2, 589–597. [Google Scholar] [CrossRef] [PubMed]
- Assari, S.; Moazen-Zadeh, E.; Lankarani, M.M.; Micol-Foster, V. Race, depressive symptoms, and all-cause mortality in the United States. Front. Public Health 2016, 4, 40. [Google Scholar] [CrossRef] [PubMed]
- Assari, S.; Lankarani, M.M. Depressive symptoms are associated with more hopelessness among white than black older adults. Front. Public Health 2016, 4, 82. [Google Scholar] [CrossRef] [PubMed]
- Assari, S.; Burgard, S. Black-White differences in the effect of baseline depressive symptoms on deaths due to renal diseases: 25 year follow up of a nationally representative community sample. J. Ren. Inj. Prev. 2015, 4, 127–134. [Google Scholar] [CrossRef] [PubMed]
- Assari, S. Hostility, anger, and cardiovascular mortality among Blacks and Whites. Res. Cardiovasc. Med. 2017, 6. [Google Scholar] [CrossRef]
- Assari, S. Race, sense of control over life, and short-term risk of mortality among older adults in the United States. Arch. Med. Sci. 2017, 13, 1233. [Google Scholar] [CrossRef] [PubMed]
- Assari, S. Perceived neighborhood safety better predicts 25-year mortality risk among Whites than Blacks. J. Racial Ethn. Health Dispar. 2017, 4, 937–948. [Google Scholar] [CrossRef] [PubMed]
- Smith, C.W. Younger Blacks Are Less Likely to Suggest That Discrimination Explains Racial Disparities, Tending to Ascribe Them to Blacks’ Lack of Will to “Pull up Their Bootstraps”; LSE American Politics and Policy: London, UK, 2014. [Google Scholar]
- Lee, W.; Roemer, J.E. Racism and redistribution in the United States: A solution to the problem of American exceptionalism. J. Public Econ. 2006, 90, 1027–1052. [Google Scholar] [CrossRef]
- Chae, D.H.; Nuru-Jeter, A.M.; Adler, N.E.; Brody, G.H.; Lin, J.; Blackburn, E.H.; Epel, E.S. Discrimination, racial bias, and telomere length in African-American men. Am. J. Prev. Med. 2014, 46, 103–111. [Google Scholar] [CrossRef] [PubMed]
- Drury, S.S.; Esteves, K.; Hatch, V.; Woodbury, M.; Borne, S.; Adamski, A.; Theall, K.P. Setting the trajectory: Racial disparities in newborn telomere length. J. Pediatr. 2015, 166, 1181–1186. [Google Scholar] [CrossRef] [PubMed]
- Oliveira, B.S.; Zunzunegui, M.V.; Quinlan, J.; Fahmi, H.; Tu, M.T.; Guerra, R.O. Systematic review of the association between chronic social stress and telomere length: A life course perspective. Ageing Res. Rev. 2016, 26, 37–52. [Google Scholar] [CrossRef] [PubMed]
- Karpin, I. Regulatory Responses to the Gendering of Transgenerational Harm. Aust. Fem. Stud. 2016, 31, 139–153. [Google Scholar] [CrossRef]
- Anderson, K. The Epigenome. In The Physiology of Sexist and Racist Oppression; Oxford University Press: Oxford, UK, 2015; Volume 99. [Google Scholar]
- Zahran, S.; Snodgrass, J.G.; Maranon, D.G.; Upadhyay, C.; Granger, D.A.; Bailey, S.M. Stress and telomere shortening among central Indian conservation refugees. Proc. Natl. Acad. Sci. USA 2015, 112, E928–E936. [Google Scholar] [CrossRef] [PubMed]
- Geronimus, A.T.; Hicken, M.; Keene, D.; Bound, J. “Weathering” and age patterns of allostatic load scores among blacks and whites in the United States. Am. J. Public Health 2006, 96, 826–833. [Google Scholar] [CrossRef] [PubMed]
- Goosby, B.J.; Heidbrink, C. Transgenerational Consequences of Racial Discrimination for African American Health. Soc. Compass 2013, 7, 630–643. [Google Scholar] [CrossRef]
- Kuzawa, C.W.; Sweet, E. Epigenetics and the embodiment of race: Developmental origins of US racial disparities in cardiovascular health. Am. J. Hum. Biol. 2009, 21, 2–15. [Google Scholar] [CrossRef] [PubMed]
- Sellers, S.L.; Neighbors, H.W.; Zhang, R.; Jackson, J.S. The impact of goal-striving stress on physical health of white Americans, African Americans, and Caribbean blacks. Ethn. Dis. 2012, 22, 21–28. [Google Scholar] [PubMed]
- Sellers, S.L.; Neighbors, H.W.; Bonham, V.L. Goal-striving stress and the mental health of college-educated Black American men: The protective effects of system-blame. Am. J. Orthopsychiatry 2011, 81, 507–518. [Google Scholar] [CrossRef] [PubMed]
- Sellers, S.L.; Neighbors, H.W. Effects of goal-striving stress on the mental health of black Americans. J. Health Soc. Behav. 2008, 49, 92–103. [Google Scholar] [CrossRef] [PubMed]
- Sellers, S.L.; Neighbors, H.W. Goal-striving stress, social economic status, and the mental health of black Americans. Ann. N. Y. Acad. Sci. 1999, 896, 469–473. [Google Scholar] [CrossRef] [PubMed]
- James, S.A.; Hartnett, S.A.; Kalsbeek, W.D. John Henryism and blood pressure differences among black men. J. Behav. Med. 1983, 6, 259–278. [Google Scholar] [CrossRef]
- James, S.A. John Henryism and the health of African-Americans. Cult. Med. Psychiatry 1994, 18, 163–182. [Google Scholar] [CrossRef] [PubMed]
- Neighbors, H.W.; Sellers, S.L.; Zhang, R.; Jackson, J.S. Goal-striving stress and racial differences in mental health. Race Soc. Probl. 2011, 3, 51–62. [Google Scholar] [CrossRef]
- Dowd, J.J.; Bengtson, V.L. Aging in minority populations an examination of the double jeopardy hypothesis. J. Gerontol. 1978, 33, 427–436. [Google Scholar] [CrossRef] [PubMed]
- Bowleg, L.; Huang, J.; Brooks, K.; Black, A.; Burkholder, G. Triple jeopardy and beyond: Multiple minority stress and resilience among Black lesbians. J. Lesbian Stud. 2003, 7, 87–108. [Google Scholar] [CrossRef] [PubMed]
- King, D.K. Multiple jeopardy, multiple consciousness: The context of a Black feminist ideology. J. Women Cult. Soc. 1988, 14, 42–72. [Google Scholar] [CrossRef]
- Cole, E.R.; Omari, S.R. Race, class and the dilemmas of upward mobility for African Americans. J. Soc. Issues 2003, 59, 785–802. [Google Scholar] [CrossRef]
- Short, S.E.; Mollborn, S. Social Determinants and Health Behaviors: Conceptual Frames and Empirical Advances. Curr. Opin. Psychol. 2015, 5, 78–84. [Google Scholar] [CrossRef] [PubMed]
- Bécares, L.; Nazroo, J.; Jackson, J. Ethnic density and depressive symptoms among African Americans: Threshold and differential effects across social and demographic subgroups. Am. J. Public Health 2014, 104, 2334–2341. [Google Scholar] [CrossRef] [PubMed]
- Cutrona, C.E.; Wallace, G.; Wesner, K.A. Neighborhood Characteristics and Depression: An Examination of Stress Processes. Curr. Dir. Psychol. Sci. 2006, 15, 188–192. [Google Scholar] [CrossRef] [PubMed]

{kind=link}
| Characteristics | All | Whites | Blacks | |||
|---|---|---|---|---|---|---|
| % | 95% CI | % | 95% CI | % | 95% CI | |
| Race | ||||||
| Whites | 84.76 | 80.94–87.93 | ||||
| Blacks | 15.24 | 12.07–19.06 | ||||
| Gender | ||||||
| Women | 52.80 | 48.72–56.84 | 51.98 | 47.75–56.18 | 57.34 | 44.42–69.33 |
| Men | 47.20 | 43.16–51.28 | 48.02 | 43.82–52.25 | 42.66 | 30.67–55.58 |
| Education (≥12 years) *a | ||||||
| Less than college | 55.46 | 51.36–59.49 | 52.47 | 48.22–56.69 | 72.08 | 59.22–82.10 |
| Completed college | 44.54 | 40.51–48.64 | 47.53 | 43.31–51.78 | 27.92 | 17.90–40.78 |
| Employment *a | ||||||
| Not in labor force | 36.59 | 32.89–40.45 | 38.62 | 34.68–42.72 | 25.28 | 16.71–36.31 |
| In labor force | 63.41 | 59.55–67.11 | 61.38 | 57.28–65.32 | 74.72 | 63.69–83.29 |
| SRMH *a | ||||||
| Good–excellent | 88.22 | 85.06–90.78 | 90.03 | 87.21–92.29 | 78.11 | 64.35–87.58 |
| Poor/Fair | 11.78 | 9.22–14.94 | 9.97 | 7.71–12.79 | 21.89 | 12.42–35.65 |
| Mean | 95% CI | Mean | 95% CI | Mean | 95% CI | |
| Age (years) * | 48.24 | 46.63–49.86 | 50.25 | 48.57–51.94 | 43.48 | 38.17–48.79 |
| Household income (USD10,000) *b | 6.60 | 6.33–6.86 | 6.70 | 6.43–6.97 | 5.54 | 4.62–6.47 |
| Characteristics | 1 | 2 | 3 | 4 | 5 | 6 | 7 |
|---|---|---|---|---|---|---|---|
| 1 Race/ethnicity (Black) | 1.00 | ||||||
| 2 Gender (men) | −0.07 | 1.00 | |||||
| 3 Age | −0.16 * | −0.05 | 1.00 | ||||
| 4 Employment (in labor force) | 0.06 | 0.09 * | −0.46 * | 1.00 | |||
| 5 Education (completed college) | −0.09 * | 0.01 | −0.01 | 0.11 * | 1.00 | ||
| 6 Household Iincome | −0.09 * | 0.16 * | −0.14 * | 0.29 * | 0.37 * | 1.00 | |
| 7 Poor SRMH | 0.05 | −0.07 | −0.10 * | −0.04 | −0.11 * | −0.15 * | 1.00 |
| Characteristics | Model 1 Main Effects | Model 2 Model 1 + Interactions | ||
|---|---|---|---|---|
| B | 95% CI | B | 95% CI | |
| Race/ethnicity (Black) | 1.93 | 0.87–4.30 | 0.48 | 0.09–2.53 |
| Gender (men) | 0.80 | 0.43–1.48 | 0.76 | 0.41–1.41 |
| Age | 0.96 * | 0.95–0.98 | 0.96 * | 0.95–0.98 |
| Employment (in labor force) | 0.58 | 0.28–1.22 | 0.59 | 0.29–1.20 |
| Education (Completed college) | 0.57 | 0.28–1.14 | 0.59 | 0.30–1.18 |
| Household income | 0.88 ** | 0.78–0.99 | 0.82 * | 0.73–0.92 |
| Household income * race/ethnicity | -- | 1.29 * | 1.01-1.66 | |
| Characteristics | Model 3 Whites | Model 4 Blacks | ||
|---|---|---|---|---|
| B | 95% CI | B | 95% CI | |
| Gender (men) | 0.55 # | 0.28–1.09 | 1.14 | 0.14–9.01 |
| Age | 0.98 * | 0.96–1.00 | 0.89 ** | 0.83–0.95 |
| Employment (in labor force) | 0.72 | 0.35–1.48 | 0.27 | 0.02–3.87 |
| Education (completed college) | 0.89 | 0.44–1.81 | 0.08 # | 0.01–1.34 |
| Household income | 0.81 ** | 0.72–0.90 | 1.10 | 0.74–1.62 |
© 2018 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Assari, S.; Lapeyrouse, L.M.; Neighbors, H.W. Income and Self-Rated Mental Health: Diminished Returns for High Income Black Americans. Behav. Sci. 2018, 8, 50. https://doi.org/10.3390/bs8050050
Assari S, Lapeyrouse LM, Neighbors HW. Income and Self-Rated Mental Health: Diminished Returns for High Income Black Americans. Behavioral Sciences. 2018; 8(5):50. https://doi.org/10.3390/bs8050050
Chicago/Turabian StyleAssari, Shervin, Lisa M. Lapeyrouse, and Harold W. Neighbors. 2018. "Income and Self-Rated Mental Health: Diminished Returns for High Income Black Americans" Behavioral Sciences 8, no. 5: 50. https://doi.org/10.3390/bs8050050
APA StyleAssari, S., Lapeyrouse, L. M., & Neighbors, H. W. (2018). Income and Self-Rated Mental Health: Diminished Returns for High Income Black Americans. Behavioral Sciences, 8(5), 50. https://doi.org/10.3390/bs8050050