Creative Arts Interventions for Stress Management and Prevention—A Systematic Review

 , and
, and
Abstract
1. Introduction
1.1. Stress as a Preparation to Act
1.2. Creative Arts Therapies and Arts Interventions for Stress Management and Prevention
1.3. Researching CATs and Arts Interventions in the Context of Stress Prevention and Stress Management
2. Methods
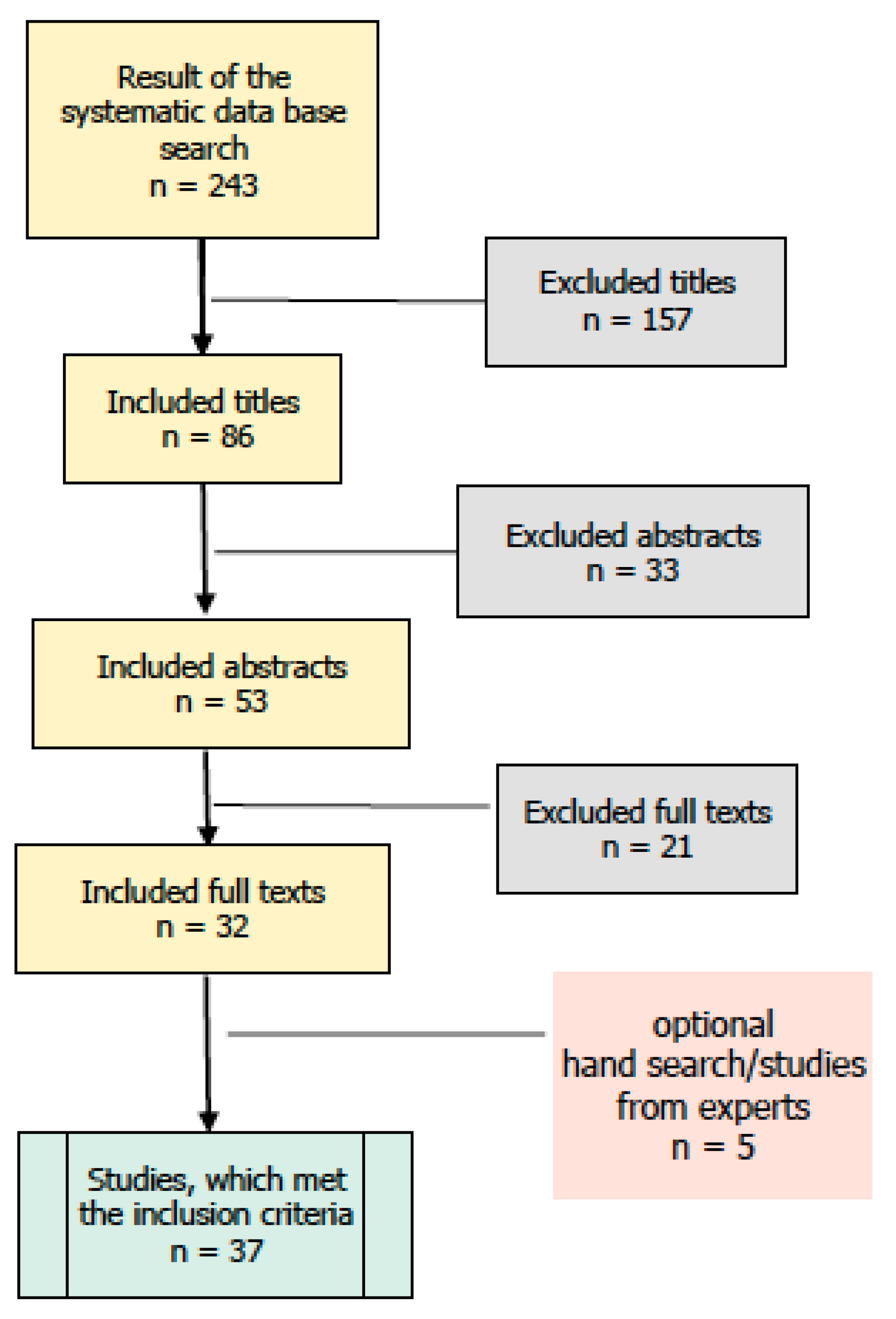
Process of the Systematic Study Search
3. Results
4. Discussion
Acknowledgments
Author Contributions
Conflicts of Interest
References
- Korczak, D.; Kister, C.; Huber, B. Differentialdiagnostik des Burnout-Syndroms; Schriftenreihe Health Technology Assessment (HTA) in der Bundesrepublik Deutschland: Köln, Germany, 2010; Available online: https://portal.dimdi.de/de/hta/hta_berichte/hta278_bericht_de.pdf (accessed on 1 December 2016).
- Franke, A.; Franzkowiak, P. Stress und Stressbewältigung. In Leitbegriffe der Gesundheitsförderung: Glossar; Bundeszentrale für gesundheitliche Aufklärung, Ed.; Verlag für Gesundheitsförderung: Köln, Germany, 2011. [Google Scholar]
- GKV-Spitzenverband (Ed.) Leitfaden Prävention 2014; Handlungsfelder und Kriterien des GKV-Spitzenverbandes zur Umsetzung der §§ 20 und 20a SGB V vom 21. Juni 2000 in der Fassung vom 10, Dezember 2014; GKV-Spitzenverband: Berlin, Germany, 2014. [Google Scholar]
- Russ, T.C.; Stamatakis, E.; Hamer, M.; Starr, J.M.; Kivimaki, M.; Batty, G.D. Association between psychological distress and mortality: Individual participant pooled analysis of 10 prospective cohort studies. BMJ 2012, 345, e4933. [Google Scholar] [CrossRef] [PubMed]
- Techniker-Krankenkasse. Entspann Dich, Deutschland—TK-Stressstudie 2016. Available online: https://www.tk.de/ centaurus /servlet /contentblob/921466/Datei/177594/TK-Stressstudie%202016%20Pdf%20 barrierefrei.pdf (accessed on 1 December 2016).
- Currie, C.; Roberts, C.; Morgan, A.; Smith, R.; Settertobulte, W.; Samdal, O.; Rasmussen, V.B. Young People’s Health in Context. Health Behaviour in Schoolaged Children (HBSC) Study: International Report from the 2001/2002 Survey; Word Health Organization: Copenhagen, Denmark, 2004. [Google Scholar]
- Selye, H. The Stress of Life; McGraw-Hill: New York, NY, USA, 1956. [Google Scholar]
- Folkman, S.; Lazarus, R.S.; Gruen, R.J.; DeLongis, A. Appraisal, coping, health status, and psychological symptoms. J. Personal. Soc. Psychol. 1986, 50, 571–579. [Google Scholar] [CrossRef]
- Folkman, S. Stress: Appraisal and coping. In Encyclopedia of Behavioral Medicine; Springer: New York, NY, USA, 2013; pp. 1913–1915. [Google Scholar]
- Thoits, P.A. Stress and health: Major findings and policy implications. J. Health Soc. Behav. 2010, 51, 41–53. [Google Scholar] [CrossRef] [PubMed]
- Folkman, S.; Moskowitz, J.T. Coping: Pitfalls and promise. Annu. Rev. Psychol. 2004, 55, 745–774. [Google Scholar] [CrossRef] [PubMed]
- Lazarus, R.S.; Folkman, S. Stress, Appraisal and Coping; Springer: New York, NY, USA, 1984. [Google Scholar]
- Bodenmann, G.; Gmelch, S. Stressbewältigung. In Lehrbuch der Verhaltenstherapie; Margraf, J., Schneider, S., Eds.; Springer: New York, NY, USA, 2009. [Google Scholar]
- Payne, P.; Crane-Godreau, M.A. The preparatory set: A novel approach to understanding stress, trauma, and the bodymind therapies. Front. Hum. Neurosci. 2015, 9. [Google Scholar] [CrossRef] [PubMed]
- Koch, S.C.; Fuchs, T. Embodied Arts Therapies. Arts Psychother. 2011, 38, 276–280. [Google Scholar] [CrossRef]
- Prinz, J. Emotion, Psychosemantics, and Embodied Appraisals. R. Inst. Philos. Suppl. 2003, 52, 69–86. [Google Scholar] [CrossRef]
- Antonovsky, A. Salutogenese. Zur Entmystifizierung der Gesundheit. Forum für Verhaltenstherapie und Psychosoziale Praxis; Franke, A., Ed.; Dgvt: Tübingen, Germany, 1997; Volume 36. [Google Scholar]
- Koch, S.; Martin, L. Verkörperte Ästhetik: Ein identitätsstiftender Wirkfaktor der Künstlerischen Therapien. In Spezifisches und Unspezifisches in den Künstlerischen Therapien; Tüpker, R., Gruber, H., Eds.; HPB University Press: Berlin, Germany, 2017; Volume 6, pp. 81–106. [Google Scholar]
- Koch, S.C. Arts and Health. Active factors and a theory framework of embodied aesthetics. Arts Psychother. 2017, 54, 88–98. [Google Scholar] [CrossRef]
- Oepen, R.; Gruber, H. Ein kunsttherapeutischer Projekttag zur Gesundheitsförderung bei Klienten aus Burnout-Selbsthilfegruppen—Eine explorative Studie. Psychother. Psychosom. Med. Psychol. 2014, 64, 268–274. [Google Scholar] [CrossRef] [PubMed]
- Bräuninger, I. Dance movement therapy group intervention in stress treatment: A randomized controlled trial (RCT). Arts Psychother. 2012, 39, 443–450. [Google Scholar] [CrossRef]
- Karkou, V.; Sanderson, P. Arts Therapies: A Research-Based Map of the Field; Elsevier Health Sciences: Oxford, UK, 2006. [Google Scholar]
- ECArTE—European Consortium for Arts Therapies Edcuation. Available online: http://www.ecarte.info/ (accessed on 4 December 2017).
- Malchiodi, C.A. Expressive Therapies; The Guildford Press: New York, NY, USA, 2005. [Google Scholar]
- Mc Niff, S. Art-Based Research. In Handbook of the Arts in Qualitative Research: Perspectives, Methodologies, Examples and Issues; Knowles, J.G., Cole, A.L., Eds.; Sage Publications Inc.: Thousand Oaks, CA, USA, 2008; pp. 29–40. [Google Scholar]
- Deutsche Musiktherapeutische Gesellschaft. Kasseler Thesen zur Musiktherapie. 2010. Available online: http://www.musiktherapie.de/fileadmin/user_upload/medien/pdf/Kasseler_Thesen_zur_Musiktherapie.pdf (accessed on 5 December 2017).
- Kunzmann, B.; Aldridge, D.; Gruber, H.; Wichelhaus, B. Künstlerische Therapien: Zusammenstellungen von Studien zu Künstlerischen Therapien in der Onkologie und Geriatrie: Hintergrund-Umsetzung-Perspektiven-Aufforderung. Musik Tanz Kunsttherapie 2015, 16, 77–86. [Google Scholar] [CrossRef]
- Bergmann, T.; Sappok, T.; Diefenbacher, A.; Dames, S.; Heinrich, M.; Ziegler, M.; Dziobek, I. Music-based Autism Diagnostics (MUSAD)—A newly developed diagnostic measure for adults with intellectual developmental disabilities suspected of autism. Res. Dev. Disabil. 2015, 43, 123–135. [Google Scholar] [CrossRef] [PubMed]
- Von Spreti, F. Kunsttherapie bei Psychischen Störungen, 1st ed.; Elsevier Urban & Fischer: München, Germany, 2005. [Google Scholar]
- Archer, S.; Buxton, S.; Sheffield, D. The effect of creative psychological interventions on psychological outcomes for adult cancer patients: A systematic review of randomised controlled trials. Psycho-Oncology 2015, 24, 1–10. [Google Scholar] [CrossRef] [PubMed]
- EADMT. Available online: http://www.eadmt.com/ (accessed on 1 November 2017).
- Hanna, J.L. Dancing for Health: Conquering and Preventing Stress; Rowman Altamira: Lanham, MD, USA, 2006. [Google Scholar]
- Martin, L.; Koch, S.C.; Hirjak, D.; Fuchs, T. Overcoming Disembodiment: The Effect of Movement Therapy on Negative Symptoms in Schizophrenia—A Multicenter Randomized Controlled Trial. Front. Psychol. 2016, 7, 483. [Google Scholar] [CrossRef] [PubMed]
- Koch, S.C.; Mergheim, K.; Raeke, J.; Riegner, E.; Machado, C.B.; Nolden, J.; Diermayr, G.; Moreau, D.; Hillecke, T. The Embodied Self in Parkinson’s Disease: Feasibility of a Single Tango Intervention for Assessing Changes in Psychological Health Outcomes and Aesthetic Experience. Front. Neurosci. 2016, 10, 287. [Google Scholar] [CrossRef] [PubMed]
- Klees, S. A Hero’s Journey in a German psychiatric hospital: A case study on the use of role method in individual drama therapy. Drama Ther. Rev. 2016, 2, 99–110. [Google Scholar] [CrossRef]
- Landy, R. Role theory and the role method of drama therapy. Curr. Approaches Drama Ther. 2009, 2, 65–88. [Google Scholar]
- Acolin, J. The Mind–Body Connection in Dance/Movement Therapy: Theory and Empirical Support. Am. J. Dance Ther. 2016, 38, 311–333. [Google Scholar] [CrossRef]
- Gruber, H.; Rose, J.P.; Mannheim, E.; Weis, J. Künstlerische Therapien in der Onkologie—Wissenschaftlicher Kenntnisstand und Ergebnisse einer Studie. Musikther. Umsch. 2011, 32, 206–218. [Google Scholar] [CrossRef]
- Al-Nawas, B.; Baulig, C.; Krummenauer, F. Von der Übersichtsarbeit zur Meta-Analyse—Möglichkeiten und Risiken. From Review to Meta Analysis—Challenges and chances. Z. Zahnärztl. Impl. 2010, 26, 400–404. [Google Scholar]
- Agency for Healthcare Research and Quality (AHRQ). Grading the Strength of a Body of Evidence When Assessing Health Care Interventions for the Effective Health Care Program of the Agency for Healthcare Research and Quality: An Update. In Methods Guide for Comparative Effectiveness Reviews; AHRQ Publication: Rockville, MD, USA, 2013; Volume 13, p. 14. [Google Scholar]
- Mayring, P. Qualitative Inhaltsanalyse. In Handbuch Qualitative Forschung in der Psychologie; Mey, G., Mruck, K., Eds.; VS Verlag für Sozialwissenschaften: Wiesbaden, Germany, 2010; pp. 601–613. [Google Scholar]
- Abbott, K.; Shanahan, M.J.; Neufeld, R.W.J. Artistic tasks outperform nonartistic tasks for stress reduction. Art Ther. 2013, 30, 71–78. [Google Scholar] [CrossRef]
- Curl, K. Assessing Stress Reduction as a Function of Artistic Creation and Cognitive Focus. Art Ther. 2008, 25, 164–169. [Google Scholar] [CrossRef]
- Huss, E.; Sarid, O. Visually transforming artwork and guided imagery as a way to reduce work related stress: A quantitative pilot study. Arts Psychother. 2014, 41, 409–412. [Google Scholar] [CrossRef]
- Kaimal, G.; Ray, K.; Muniz, J. Reduction of Cortisol Levels and Participants’ Responses Following Art Making. Art Ther. 2016, 33, 74–80. [Google Scholar] [CrossRef] [PubMed]
- Kimport, E.R.; Robbins, S.J. Efficacy of Creative Clay Work for Reducing Negative Mood: A Randomized Controlled Trial. Art Ther. 2012, 29, 74–79. [Google Scholar] [CrossRef]
- Mercer, A.; Warson, E.; Zhao, J. Visual journaling: An intervention to influence stress, anxiety and affect levels in medical students. Arts Psychother. 2010, 37, 143–148. [Google Scholar] [CrossRef]
- Pizarro, J. The Efficacy of Art and Writing Therapy: Increasing Positive Mental Health Outcomes and Participant Retention after Exposure to Traumatic Experience. Art Ther. 2004, 21, 5–12. [Google Scholar] [CrossRef]
- Sandmire, D.A.; Gorham, S.R.; Rankin, N.E.; Grimm, D.R. The Influence of Art Making on Anxiety: A Pilot Study. Art Ther. 2012, 29, 68–73. [Google Scholar] [CrossRef]
- Schrade, C.; Tronsky, L.; Kaiser, D.H. Physiological effects of mandala making in adults with intellectual disability. Arts Psychother. 2011, 38, 109–113. [Google Scholar] [CrossRef]
- Smolarski, K.; Leone, K.; Robbins, S.J. Reducing Negative Mood through Drawing: Comparing Venting, Positive Expression, and Tracing. Art Ther. 2015, 32, 197–201. [Google Scholar] [CrossRef]
- Walsh, S.M.; Martin, S.C.; Schmidt, L.A. Testing the Efficacy of a Creative-Arts Intervention with Family Caregivers of Patients with Cancer. J. Nurs. Scholarsh. 2004, 36, 214–219. [Google Scholar] [CrossRef] [PubMed]
- Beck, B.D.; Hansen, A.M.; Gold, C. Coping with Work-Related Stress through Guided Imagery and Music (GIM): Randomized Controlled Trial. J. Music Ther. 2015, 52, 323–352. [Google Scholar] [CrossRef] [PubMed]
- Brodsky, W.; Sloboda, J.A. Clinical trial of a music generated vibrotactile therapeutic environment for musicians: Main effects and outcome differences between therapy subgroups. J. Music Ther. 1997, 34, 2–32. [Google Scholar] [CrossRef]
- Brooks, D.M.; Bradt, J.; Eyre, L.; Hunt, A.; Dileo, C. Creative approaches for reducing burnout in medical personnel. Arts Psychother. 2010, 37, 255–263. [Google Scholar] [CrossRef]
- Byrnes, S.R. The effect of audio, video, and paired audio-video stimuli on the experience of stress. J. Music Ther. 1996, 33, 248–260. [Google Scholar] [CrossRef]
- Chang, M.-Y.; Chen, C.-H.; Huang, K.-F. Effects of music therapy on psychological health of women during pregnancy. J. Clin. Nurs. 2008, 17, 2580–2587. [Google Scholar] [CrossRef] [PubMed]
- DuRousseau, D.R.; Mindlin, G.; Insler, J.; Levin, I.I. Operational Study to Evaluate music-based neurotraining at improving sleep quality, mood and daytime function in a first responder population. J. Neurother. 2011, 15, 389–398. [Google Scholar] [CrossRef][Green Version]
- Goff, L.C.; Pratt, R.R.; Madrigal, J.L. Music listening and A-lgA levels in patients undergoing a dental procedure. Int. J. Arts Med. 1998, 5, 22–26. [Google Scholar]
- Hatta, T.; Nakamura, M. Can antistress music tapes reduce mental stress? Stress Med. 1991, 7, 181–184. [Google Scholar] [CrossRef]
- Ilie, G.; Rehana, R. Effects of Individual Music Playing and music listening on acute-stress recovery. Can. J. Music Ther. 2013, 19, 23–46. [Google Scholar]
- Jacobsen, S.L.; McKinney, C.H.; Holck, U. Effects of a dyadic music therapy intervention on parent-child interaction, parent stress, and parent-child relationship in families with emotionally neglected children: A randomized controlled trial. J. Music Ther. 2014, 51, 310–332. [Google Scholar] [CrossRef] [PubMed]
- Kim, S.-A. Predictors of Acculturative Stress among International Music Therapy Students in the United States. Music Ther. Perspect. 2011, 29, 126–132. [Google Scholar] [CrossRef]
- Lesiuk, T. The effect of preferred music listening on stress levels of air traffic controllers. Arts Psychother. 2008, 35, 1–10. [Google Scholar] [CrossRef]
- Maschi, T.; Bradley, C. Recreational Drumming: A creative arts intervention strategy for social work teaching and practice. J. Baccalaureate Soc. Work 2010, 15, 53–66. [Google Scholar]
- Mohammadi, A.Z.; Shahabi, T.; Panah, F.M. An evaluation of the effect of group music therapy on stress, anxiety, and depression levels in nursing home residents. Can. J. Music Ther. 2011, 17, 55–68. [Google Scholar]
- Murphy, E.M.; Nichols, J.; Somkuti, S.G.; Sobel, M.; Braverman, A.; Barmat, L.I. Randomized Trial of Harp Therapy During In Vitro Fertilization–Embryo Transfer. J. Evid. Based Complement. Altern. Med. 2013, 19, 93–98. [Google Scholar] [CrossRef] [PubMed]
- Rider, M.S.; Floyd, J.W.; Kirkpatrick, J. The Effect of Music, Imagery, and Relaxation on Adrenal Corticosteroids and the Re-entrainment of Circadian Rhythms. J. Music Ther. 1985, 22, 46–58. [Google Scholar] [CrossRef] [PubMed]
- Sharma, M.; Jagdev, T. Use of Music therapy for enhancing self-esteem among Academically Stressed Adolescents. Pak. J. Psychol. Res. 2012, 27, 53–64. [Google Scholar]
- Smith, J.C.; Joyce, C.A. Mozart versus New Age Music: Relaxation States, Stress, and ABC Relaxation Theory. J. Music Ther. 2004, 41, 215–224. [Google Scholar] [CrossRef] [PubMed]
- Smith, M. The Effects of a Single Music Relaxation Session on State Anxiety Levels of Adulats in a Workplace Environment. Aust. J. Music Ther. 2008, 19, 45–66. [Google Scholar]
- Toyoshima, K.; Fukui, H.; Kuda, K. Piano playing reduces stress more than other creative art activities. Int. J. Music Educ. 2011, 29, 257–263. [Google Scholar] [CrossRef]
- Pinniger, R.; Brown, R.F.; Thorsteinsson, E.B.; McKinley, P. Argentine tango dance compared to mindfulness meditation and a waiting-list control: A randomised trial for treating depression. Complement. Ther. Med. 2012, 20, 377–384. [Google Scholar] [CrossRef] [PubMed]
- Pinninger, R.; Thorsteinsson, E.B.; Brown, R.F.; McKinley, P. Intensive Tango Dance Program for People with Self-Referred Affective Symptoms. Music Med. 2013, 5, 15–22. [Google Scholar] [CrossRef]
- Quiroga Murcia, C.; Bongard, S.; Kreutz, G. Emotional and neurohumoral responses to dancing tango argentino: The effects of music and partner. Music Med. 2009, 1, 14–21. [Google Scholar] [CrossRef]
- West, J.; Otte, C.; Geher, K.; Johnson, J.; Mohr, D.C. Effects of Hatha yoga and African dance on perceived stress, affect, and salivary cortisol. Ann. Behav. Med. 2004, 28, 114–118. [Google Scholar] [CrossRef] [PubMed]
- Wiedenhofer, S.; Koch, S.C. Active factors in dance/movement therapy: Specifying health effects of non-goal-orientation in movement. Arts Psychother. 2016, 52, 10–23. [Google Scholar] [CrossRef]
- Körlin, D.; Nybäck, H.; Goldberg, F.S. Creative arts groups in psychiatric care. Development and evaluation of a therapeutic alternative. Nord. J. Psychiatry 2009, 54, 333–340. [Google Scholar] [CrossRef]
- Koch, S.C.; Kolter, A.; Kurz, T. Indikationen und Kontraindikation in der Tanz- und Bewegungstherapie. Eine induktive Bestandsaufnahme. Musik Tanz Kunsttherapie 2013, 23, 87–105. [Google Scholar] [CrossRef]
- Stegemann, T.; Schmidt, H.-U. A pilot investigation on indication and contraindication of music therapy in child and adolescent psychiatry. Musikther. Umsch. 2010, 31, 87–101. [Google Scholar] [CrossRef]


{kind=link}
| Study (Author/Year) | Level of Evidence | Object of Investigation | N/Sample | Design | Intervention | Methods | Exemplary Results | |
|---|---|---|---|---|---|---|---|---|
| Data Collection | Analysis | |||||||
| ART THERAPY | ||||||||
| Abbott et al. (2013) [42] | Ib | Effect of an artistic action vs. art reception on the stress level | 52 Students, 34f/18m, M = 22.7 years | 2 × 2 factorial, randomized, controlled | Active & passive artistic condition: painting/drawing vs. viewing art; active/passive non-artistic condition: puzzle vs. viewing the puzzle pictures; 1 single interven-tion | Stress: Mental Arithmetic Task; Stress Induction Task, Stress Adjective Checklist; Creative Personality Scale; Subjective Stress Scale | Multifactorial Analysis of Covariance (MANCOVA) | Stress reduction sig. higher in the group allocated to active artistic condition. F(2, 44) = 3.45, p < 0.05 |
| Curl (2008) [43] | Ib | Short-term stress reduction by focusing on a positive, stress-free experience versus a negative, stressful experience during artistic activity | 40 Psychology Students, 30f/10m, M = 19.65 years | 2 × 2 factorial, randomized, controlled | 4 experimental groups: drawing with positive and negative focus; creating collages with positive and negative focus; 1 single intervention | Stress, anxiety: State Trait Anxiety Inventory; collection of heartrate pre-post Level of focusing on positive and negative experiences: Manipulation Check | t-test for independent samples; ANOVA | Focusing on positive experiences while artistic activity leads to stress reduction, regardless of the type of artistic technique. F(1) = 13.76, p < 0.01 |
| Huss & Sarid (2014) [44] | Ib | Effect of changing compositional elements (shape, size, color, texture) of a self-designed image of a memory vs. a simple memory (guided imagery) on the experience of stress. | 35 Healthcare professionals (doctors, nurses, social workers) | Intervention-evaluation-study, randomized, controlled | Group I (Art Therapy): Constructing a stressful work experience on paper, transforming the experience into a stress-free event; Group II (Guided Imagery): introducing and recalling a stressful work experience, 2 days workshop | Definition of artistic elements: Compositional Elements Scale Discomfort, Stress: Subjective Units of Discomfort Scale (SUDS) | Descriptive: frequency analysis of compositional elements, paired significance tests, mean and standard deviation calculation of individual values | Reduction of stress level in Group I and Group II. The compositional elements of shape, size and color are of particular importance. X2 = 8.61(df = 1), p = 0.03; X2 = 7.56(df = 1), p = 0.04; t-test = 3.27(df = 1), p = 0.03, t-test = 2.03(df = 1), p = 0.04, respectively |
| Kaimal, Ray & Muniz (2016) [45] | IIb | The impact of visual art making on the cortisol level | 39 Students, staff & faculty from a large university, 33f/6m, M = 38.88 | Single arm, pre-post-design, quasi-experimental | 1 single session: 45 min of art making using collage materials, modeling clay, and/or markers, 15 min for consent and data collection before and after the session | Cortisol Level: Saliva Sample (pre/post; ELISA kit method) Prior Art making experience: limited, some, extensive experience self-reported perceived impact of art making: Written responses from participants (qualitative data) converted into numeric data, entered into quantitative database | t-test for paired samples, one-way ANOVA, t-test for independent samples, Correlation Analysis: | Sig. reductions in cortisol following the intervention: cortisol levels pre- and posttest differed significantly t(38) = 4.54, p < 0.01 No sig. differences based on prior experiences on cortisol levels, F(2, 36) = 0.64, p = 0.53 No sig. differences based on gender on changes in cortisol, t(37) = 0.456, p = 0.65 Self-reported themes were not strongly correlated with changes in cortisol levels |
| Kimport & Robbins (2012) [46] | Ib | Effect of a guided intervention with clay on the mood | 102 Students of an American University, 74f/28m, M = 22.3 years | 2 × 2 × 3 factorial, randomized, controlled | Creation of negative mood by showing a short film; 4 different 5-min interventions: Group A: clay + instruction; Group B: clay without instruction; Group C: stress ball + Instruction; Group D: stress ball without instruction; 1 single session | Mood State, Anxiety: Profile of Mood States (POMS), State-Trait Anxiety Inventory (STAI) | Multifactorial Analysis of Variance (ANOVA) | Editing tone (with and without instruction) reduces negative mood (mood and anxiety) more than working with stress balls; guided interventions (clay and balls) reduce negative mood more than interventions without guidance; POMS: F(1, 98) = 7.6, p < 0.05; STAI-S: F(1, 98) = 4.4, p < 0.05. |
| Mercer et al. (2010) [47] | III | Stress reduction through visualization (Visual Journaling) | 10 5 medical Students, 5 Lecturers | Single-arm, pre-post-design with follow-up | Visualization of a stress-inducing vs. a stress-free emotion, drawing of these emotions, self-explanatory questions for a better understanding of the stress situation; 1 single intervention | Mood State, Anxiety: quantitative: State-Trait Anxiety Inventory (STAI-Y), the Positive and Negative Affect Schedule (PANAS) qualitative: Questions on stress situation | paired t-tests | Non-significant reduction of anxiety and improvement of mood. |
| Pizarro (2004) [48] | Ib | Comparison of art and writing therapy concerning their effects on psychological and health conditions | 45 Students, 27f/18m, M = 19 years | randomized, controlled, pre-post-design with follow-up | 2 experimental groups: Induction of a stressful situation based on a text; painting this situation (art-stress) vs. writing about this situation (write-stress); control group: painting a still life after a neutral text, 2 sessions on 2 days | Health, Stress, Physical Symptoms, Mood: General Health Questionaire (GHQ-28), The Global Measure of Perceived Stress (GMPS), Physical Symptoms Inventory (PSI), Profile of Mood States (POMS) (short version) qualitative: Questioning on satisfaction; Questionnaire for the Assessment of stress reduction in art and writing intervention (follow-up) | Analysis of Covariance (ANCOVA) | Sig. reduction of social dysfunction in the writing-stress group: F(2, 37) = 3.17, p = 0.05; No health improvements in the art groups: F(2, 37) = 0.10, ns; But more joy and commitment of study participation in the art groups. |
| Sandmire et al. (2012) [49] | Ib | Reduction of anxiety through artistic activity | 57 Students, 45f/12m, M = 18.8 years | randomized, controlled | experimental group: Choice of one of five artistic activities (mandala, free painting, collage, clay, drawing), 1 single session, duration: 30 min.; control group: no intervention | Anxiety: State Trait Anxiety Inventory (STAI) | t-tests for paired samples; multifactorial Analysis of Variance (ANOVA) | Sig. reduction of anxiety (state and trait) before final exams. p < 0.001, F(1) = 12.72 |
| Schrade et al. (2011) [50] | Ib | Relaxation and reduction of stress levels through painting mandalas. | 15 Adults with mental disabilities 9f/10m | Repeated measure, randomized, controlled | 3 conditions: painting mandalas, free painting, neutral control condition (puzzle, board games, etc.), 1 single session | Stress: blood pressure, pulse (Sphygmomanometers) | three separate ANOVAs for repeated measures | Sig. reduction of blood pressure (systolic and diastolic) in the mandala group over time: F(2, 28) = 6.05, p < 0.05; no sig. change of stress levels comparing the three groups. |
| Smolarski et al. (2015) [51] | Ib | Effect of instructions on emotional expression on the mood-enhancing qualities of drawing | 45 Students, 28f/17m | randomized, controlled, doubleblind, pre-post design | 1. Inducing a negative mood 2. Randomized allocation to three groups: Group A: drawing happiness (acting out a positive mood) Group B: drawing current stress (acting out a negative mood) Group C: tracing and coloring a simple drawing (control group, distraction strategy), 1 single session | Mood State: Profile of Mood States (POMS) | two-factorial ANOVA with repeated measures (3 groups; time: baseline, pre-post-treatment) | Sig. mood improvement through the expression of a positive emotion while drawing in comparison to the expression of a negative emotion (venting) or the drawing of simple lines (control group), F(2, 42) = 4.0, p < 0.05. |
| Walsh et al. (2004) [52] | IIb | Effect of an artistic intervention on anxiety and stress among family members of cancer patients | 40 family members of cancer patients, 30f/10m, M = 51.43 years | pre-post-design, quasi-experimental | Creative-artistic intervention, e.g., painting mandalas, painting; Implementation in the hospital room of the patient, 1 single intervention | Mood State: Mini-POMS Anxiety: Beck Anxiety Inventory (BAI) Negative and positive emotions: Derogatis Affects Balance Scale (DABS) | t-tests for paired samples | Sig. reduction of stress, anxiety: t(40) = −3.42, p = 0.001; increase of positive emotions, t(46) = 11.87, p < 0.001. |
| MUSIC THERAPY | ||||||||
| Beck, Hansen & Gold (2015) [53] | Ib | Effect of MT on biopsychosocial parameter | 20 Danish workers with stress-related incapacity to work, 16f/4m, M = 45.5 years | randomized, controlled | Music Therapeutic Intervention: Guided Imagery and Music (GIM) 2-hour-sessions, 6 sessions in 9 weeks | Cortisol, testosterone, melatonin: analysis of saliva in the laboratory Stress: Perceived Stress Scale (PSS); Profile of Moods States (POMS-37); Visual analogue scale for immediate stress sensation before and after the sessions; Karolinska Sleep Diary (KSQ); Unpublished 16-item scale for physical stress symptoms Willingness to work: single item Well-being: WHO-5 Well-Being Index Anxiety: Generalized Anxiety Disorder 7 (GAD-7) Depression: Major Depression Inventory | t-test for independent samples | Sig. improvement in well-being and sig. reduction in sleep disturbance and physical distress. Early intervention leads to faster re-entry of work & positive sig. effects on stress, mood, sleep disorder, depression, anxiety and physical symptoms of distress. (see Table 2, p. 339, in original study) |
| Brodsky & Sloboda (1997) [54] | Ib | Comparison of effect of Music Therapy and traditional verbal Psychotherapy | 55 Musician of a symphony orchestra, M = 36 years | randomized, controlled, pre/post design with follow-up | Three groups: (a) Somatron: traditional verbal psychotherapy, abbreviated progressive relaxation training (APRT), recorded music complemented by music-generated vibrations (b) Music: verbal psychotherapeutic counseling, APRT relaxation exercises supplemented with recorded music (c) Counseling: verbal psychotherapeutic counseling 1 h per week, 8 weeks | Baseline (Anxiety, Stress, Mood State, Burnout): General Health Questionnaire (GHQ-28), Spielberger State Trait Anxiety Inventory (STAI), Derogatis Stress Profile (DSP), Profile of Mood States (POMS), Maslach Burnout Inventory of Music Performer’s Stress (AMPS), and the Music Performance Stress Survey (MPSS) Pre-Post (Mood State, Relaxation): POMS, relaxation exercises | Multifactorial ANOVA with repeated measures | Music-supported forms of therapy as efficient as traditional counseling. 14 of the 52 sets of variables were statistically and clinically significant at measuring time 2 and 3. Differences between groups were not sig. F(2.46) = 4.16; p = 0.22. |
| Brooks, Bradt, Eyre, Hunt & Dileo (2010) [55] | Ib | Effect of MT on self-assessment of burnout, sense of coherence and job satisfaction | 65 Medical nursing staff, 43f/9m M = 42.16 years | Randomized, controlled | Guided Imagery with music and relaxation exercises, 3-6 weeks, 60 min sessions | Burnout: Maslach Burnout Inventory Sense of Coherence: Sense of Coherence Scale Job Satisfaction: Job Satisfaction Survey Individual perception of interventions: Self-report on interventions (qualitative survey) | Independent t-test Grounded theory | Quantitative results: No sig. differences between experimental group (MT) and control group (waiting). Qualitative results: Music therapeutic Intervention helped subjects to relax and to recharge energy. |
| Byrnes (1996) [56] | Ib | Effect of audio, video and audio-video stimuli on the stress experience | 54 33 Adults (participants of a university summer course) 21 students of music and/or education | Randomized, controlled, pre-post-design | Three groups: (a) Audio-Video: Music-Video excerpt from “Tropical Sweets” (with classical music) (b) Audio: “Aquarium” by Camille Saint-Saens (c) Video: Underwater movie about tropical marine life, 1 single session | Questionnaire on socio-demographic data, music preferences and activities for relaxation, current level of stress Stress Experience Continuous Response Digital Interface (CRDI) | Paired t-tests | Stress reduction especially for participants with a high level of stress at the beginning: t = 3.695, df = 53, p = 0.001; Sig. reduction in audio-video condition, audio or video condition alone did not sig. affect stress. |
| Chang, Chen & Huang (2008) [57] | Ib | Effect of MT on the stress level, anxiety and the degree of depression | 236 pregnant, Taiwanese women M = 30.48 years | randomized, controlled | EG: passive music therapy intervention: listening to music 2 weeks, 30 min. per day CG: general prenatal treatment without MT | Stress: Perceived Stress Scale (PSS) Anxiety: State Scale of the State-Trait Anxiety Inventory (S-STAI) Depression: Edinburgh Postnatal Depression Scale (EPDS) | Paired t-test Analysis of Covariance (ANCOVA) | Stress reduction, anxiety reduction and reduction of the degree of depression sig. higher in the EG with music therapy intervention than in the CG (see Table 4, p. 2585, in the original study). |
| Du Rousseau et al. (2011) [58] | IIa | Improvement of sleep quality, mood state, everyday functions | 41 Law enforcement officers, firefighters, 13f/28m | pre-post-design, controlled | Brain Music (BM) Music-based Neurofeedback Therapy | Insomnia, sleep quality, depression, life satisfaction, everyday functions: Pittsburgh Insomnia Rating Scale, Subjective Sleep Questionnaire, Beck Depression Inventory, Life Satisfaction Scale, Daytime Functioning Scale, 4 weeks intervention | Analysis of Variance (ANOVA), paired t-tests | Sig. improvement of sleeping quality, insomnia, mood and everyday functioning (see Table 1, p. 392, in the original study). |
| Goff et al. (1998) [59] | Ib | Comparison of the effects of music and nitrous oxide on the pain-, anxiety- and stress-levels of subjects during a dental treatment | 80 dental patients | randomized, controlled, 2 × 2 factorial | (a) treatment under nitrous oxide and Level 1 = no music/level 2 = with music (b) treatment accompanied by self-selected music (Level 1 = without nitrous oxide, level 2 = with nitrous oxide) | Pain, Anxiety, Stress: Saliva samples before and after treatment for determination of S-IgA concentration (secretory immunoglobulins A) | multifactorial Analysis of Variance (ANOVA) | No sig. differences between the two treatment methods; in women sig. stress reduction with music accompaniment (see Tables 1 and 2, p. 24, in the original study). |
| Hatta & Nakamura (1991) [60] | Ib | Effect of Anti-stress Music-CDs on stress level | 52 Students, 28f/24m | Randomized, controlled, Pre-Post-Design | EG: Classical Music vs. Nature Sounds vs. Pop music; CG: no intervention, single session | Stress, Arousal: Stress/Arousal adjective checklist (SACL) | 2-factorial Analysis of Variance (ANOVA) | Sig. reduction of stress and arousal through listening to music, regardless of the type of music, F(9, 144) = 4.25, p < 0.01. |
| Ilie & Rehana (2013) [61] | Ib | Effect of playing music on the iPhone on the acute stress level | 54 Students, 27f/27m | Randomized, controlled, 2 × 3 factorial, pre-post-design | Group 1: induction of a stress situation Group 2: no stress induction Each: (a) Pressing the music app “Smule Ocarina” for 10 min, i.e., Playing the melody “Twinkle, Twinkle, Little Star” (b) listening to the melody; (c) Sitting quietly 1 single session | Mood State, Arousal: Profile of Mood States (POMS) Level of Cortisol: Salimetrics Oral Swab (SOS) | Mixed-model ANOVA | Sig. reduction of cortisol level in the stress-induced group by listening to or playing the app compared to the control group, F(1, 65) = 21.54, p < 0.001. |
| Jacobsen, McKinney & Holck (2014) [62] | Ib | Effect of MT on the parent-child interaction and parent-child relationship as well as the stress experience of the parents | 18 Parent-child dyads from Denmark with neglected children | Randomized, controlled | EG: music therapeutic Intervention CG: standard treatment without MT 10 weekly sessions, 45 to 50 min. | Parent Competencies: Assessment of Parenting Competencies (APC) Stress experience of parents: Parenting Stress Index (PSI) Parent-Child-Relationship: Parent-Child Relationship Inventory (PCRI) | Multifactorial Analysis of Variance (ANOVA) | Improvement of parent competencies and parent-child interaction, as well as stress reduction in the experimental group with MT intervention higher than in the control group (see pp. 321–326 in original study). |
| Kim (2008) [63] | Ib | Effect of two music therapy approaches on Music Performance Anxiety (MPA) | 30 Music Students (Piano) | Randomized, controlled, pre-post-design | 2 Groups (a) improved-music-assisted-desensitization-group (b) music-assisted progressive muscle relaxation (PMR) and imagery-group 6 weekly sessions | Anxiety, Stress, tension, relaxation: Visual Analogue Scale (VAS), State-Trait Anxiety Inventory (STAI), Music Performance Anxiety Questionnaire (MPAQ); Measurement of the finger temperature | Tests of significance, Analysis of Variance (ANOVA) | Sig. reduction of MPA in the music-assisted desensitization group at 6 out of 7 measurement points; Anxiety reduction in the music-assisted PMR group to a lesser extent than in the former group, but sig. for stress and tension level. Level of tension: F = 7.55, p = 0.016, df = 1, 14; state anxiety of the STAI, F = 5.57, p = 0.033, df = I, 14; finger temperature measure, F = 7.87, p = 0.014, df = 1, 14 |
| Lesiuk (2008) [64] | Ib | Effect of listening to self-selected music at the workplace on stress levels | 33 air traffic controllers, 2f/31m, M = 34 years | Randomized, controlled; Pre-Post-Design | EG: 15 min. Listening to favorite music, in the break of 4 working shifts in 2 weeks; CG: sitting in silence instead of listening to music | Extraversion, Introversion: Eysenck Personality Inventory; Anxiety: State-Trait-Anxiety Inventory (STAI); Measurement of heart rate, blood pressure, state anxiety and subjectively perceived aviation activity | Multifactorial Analysis of Variance (ANOVA) | No sig. differences between physiological and psychological components in the comparison of both groups; Sig. anxiety reduction (state anxiety) in EG and CG over time, F = 19.22, d.f. = 2, p = 0.000, and reduced perception of air traffic in both groups. |
| Maschi & Bradley (2010) [65] | III | Effect of relaxation drums on well-being, empowerment and social connectedness | 31 Social Work Students, 29f/2m | Pre-Post-Design | One single session of 2 h relaxation drumming in the group | Stress, Energy, Empowerment, Bonding: Session Impact Scale | paired t-tests | Sig. stress reduction, increased energy, empowerment and a sense of community (see Table 3, p. 61, in the original study). |
| Mohammadi, Shahabi & Panah (2011) [66] | Ib | Effect of MT on stress, anxiety and the degree of depression | 19 residents of a home for elderly, 9f/10m, M = 69.4 years | Randomized, controlled | Experimental Group: MT group intervention (music listening, singing, percussion), 10 weeks of 90 min. daily sessions Control group: standard day-to-day acitivities | Stress, Anxiety & Depression: Depression Anxiety Stress Scale (DASS) | Mann-Whitney U-Test | Stress reduction, anxiety reduction and reduction of the degree of depression sig. higher in the experimental group with MT than in the control group (standard day-to-day activities) (see Table 1, p. 63, in the original study). |
| Murphy et al. (2014) [67] | Ib | Effect of harp therapy on the stress level and clinical outcome values | 181 Women in an in vitro reproduction surgery | Prospective, randomized, controlled, pre-post design | EG: harp therapy for in vitro fertilization CG: standard therapy | Anxiety: State-Trait Anxiety Inventory; Pulse, respiratory rate, blood pressure | t-test for paired samples, Wilcoxon rang sum test | Sig. higher reduction of anxiety (state anxiety) over time in the EG than in the CG; Conception rate higher in EG than in CG; positive effect on the acute stress level; no sig. Improvement of heart rate and respiratory rate (see Tables 6–9, pp. 96–97, in the original study). |
| Rider et al. (1985) [68] | III | Effect of music/progressive muscle relaxation (PMR)/guided imagery (GI) on stress hormones | 12 Nurses | Quasi-experimental, pre-post design | 20-min program of classical music (audio cassettes) incl. PMR and GI (visualization of imaginative images); 5 times a week over 3 months | Adrenal Corticosteroid (Stress hormones): Urine samples, temperature measurements; Taylor-Johnson Temperament Analysis, State-Trait Anxiety Inventory, Torrance Test of Creativity, Circadian Type Questionnaire | t-tests | Reduction of circadian amplitude and corticosteroid temperature rhythms during music listening; The average corticosteroid level did not improve sig. over time. |
| Sharma & Jagdev (2012) [69] | Ib | Effect of MT on the self-esteem of adolescents | 60 adolescents with high school stress levels & low self-esteem, M = 16.85 years | pre-post design, controlled | EG: 30 min listening to classical Indian music (raga, flute) per day, 15 days; CG: discussion of study irrelevant topics | School Stress (Anxiety, Frustration, Pressure Conflict): Scale of Academic Stress (SAS-3) Self Esteem: Self Esteem Inventory (SEI) | t-tests | Sig. increase in self-esteem in the EG compared to the CG. (see Table 2, p. 59, in the original study) |
| Smith & Joyce (2004) [70] | IIa | Effect of MT on the state of relaxation and stress | 63 students, 45f/18m, M = 20.88 years | Quasi-experimental, controlled | EG1: receptive MT-Intervention (Mozart). EG2: receptive MT-Intervention (New Age Music) CG: reading offer without MT Relaxation Sessions of 28 min, 3 days in a row, once a day | State of Relaxation and Stress: Smith Relaxation States Inventory (SRSI) | Pearson chi2-test | Stress reduction and increase of the relaxation state higher in EG1 (Mozart) compared to EG2 (New Age Music) or to the control group (reading of leisure magazines). (see p. 220) |
| Smith (2008) [71] | Ib | Effect of MT on Anxiety | 80 Employees of a call center 40f/40m, M = 37.5 years | Randomized, controlled | Experimental group: Progressive muscle relaxation with music Control group: verbal discussion, 1 single session | Anxiety: State Trait Anxiety Inventory | t-test with repeated measures | Anxiety reduction sig. higher in the EG with musical relaxation intervention than in the CG (verbal discussion): decrease in tense rating: t(39) = 12; p < 0.01; increase in pleasant and relaxed rating: t(39) = −20.27; p < 0.01; t(39) = −16.2; p < 0.01. |
| Toyoshima, Fukui & Kuda (2011) [72] | Ib | Effect of creative activities on cortisol levels and anxiety | 57 Students, 30f/27m, M = 21.5 years | Randomized, controlled | Three experimental groups (1 piano playing, 2 clay modulations, 3 calligraphy) and a control group (lingering in silence) 1 single session | Anxiety: State Trait Anxiety Inventory Detection of cortisol in saliva | Multifactorial Analysis of Variance (ANOVA) | Anxiety reduction and cortisol degradation higher in the EG (creative interventions) than in the CG (lingering in silence). Playing the piano shows the biggest effects. F(1,113) = 5.57, p = 0.0202 |
| DANCE/MOVEMENT THERAPY | ||||||||
| Bräuninger (2012) [21] | Ib | Improvement of stress management and stress reduction, as well as the influence of DMT group intervention on quality of life (QoL) | N = 162 Clients suffering from stress (self-assessed), 147f/15m M = 44 years | Randomized, controlled, pre-post-design with follow-up after 6 months | EG: DMT, group intervention, 10 weeks CG: waiting control group | Stress management and stress reduction: Stress processing questionnaire/SVF 120 General Stress Level and Psychopathology (Brief Symptom Inventory/BSI) Quality of Life (QoL): The World Health Organization Quality of Life Questionnaire 100 (WHOQOL-100) and Munich Life Dimension List (MLDL) | Stress Data: Multifactorial Analysis of Variance (ANOVA) Quality of Life: Analysis of Variance with repeated measures (repeated measures ANOVA) | Negative stress management strategies decreased sig. in short and long term comparisons, positive strategies of distraction increased, as well as relaxation; sig. short-term improvements in the BSI, especially with regard to anxiety scores; QoL dimensions were sig. better in the EG than in the CG (see Tables 4 and 5, pp. 447–448, in the original study). |
| Pinninger, Brown & McKinley (2012) [73] | Ib | Comparison of tango and mindfulness meditation regarding stress reduction, reduction of anxiety and depression symptoms and improvement of well-being | Sample N = 79 (self-assessed) depressedPersons, 19.5f/80.5, M = 38.68 years | 3 × 2 factorial design, randomized-controlled, pre-post test | Three interventions: Tango: 6 weeks, 1 ½ h per week Mindfulness meditation: 6 weeks, 1 ½ h per week Waiting control group | Anxiety, Depression: Depression, Anxiety and Stress Scale (DASS-21-Scale); Rosenberg Self Esteem Scale; Satisfaction with Life Scale, and Mindful Attention Awareness Scale. | Analysis of Covariance (ANCOVA) and Multiple regression analysis | Significantly reduced depression symptoms in both (F(2, 59) = 6.00, p = 0.004), the tango group and the mindfulness group compared to the control group; reduced stress only in the tango group (F(2, 59) = 3.88, p = 0.026); participation in the tango dance was a significant predictor of improved mindfulness. |
| Pinninger, Brown & McKinley (2013) [74] | Ib | Effect of an intensive program of Tango dance on self-reported stress, anxiety or symptoms of depression | N = 41 (experimental group: 20, waiting control group: 21) | Randomized, controlled (RCT) Pre, Post-Test, follow-up after one month | EG: Tango dance program (4 × 1 ½ h in 2 weeks), waiting control group | Self-assessment scales of stress, anxiety and depression symptoms: Depression Anxiety and Stress Scale (DASS-21); Insomnia Severity Index; Satisfaction with Life Scale; General Self-efficacy Scale; Mindful Attention Awareness Scale; Qualitative feedback | Analyzes of Covariance (ANCOVAs) | Self-assessed stress-, anxiety- and depression-symptoms in the experimental group sig. improved compared to the control group; effects were retained at follow-up time (1 month); life satisfaction and self-efficacy sig. improved; mindfulness did not change sig.: stress, F(1,38) = 12.59, p = 0.001; anxiety, F(1,38) = 8.31, p = 0.006; depression, F(1,38) = 25.60, p = 0.001; insomnia, F(1,38) = 8. 30, p = 0.006 |
| Quiroga Murcia, Bongard & Kreutz (2009) [75] | IIa | Effects of tango dance on psychophysiological emotion or stress measurements | 22 healthy individuals with min. 1 year tango experience, 11f/11m M = 43.09 years | 2 × 2 factorial, controlled | 4 Conditions: 1. Regular tango dance with partner and music 2. Tango dance with partner without music 3. Dance without partner but with music 4. Movement without a partner and without music 20 min sessions | Stress: Positive and Negative Affect Schedule (PANAS) Saliva samples for the study of cortisol and testosterone | Multivariate Analysis of Variance (MANOVA) with repeated measures | Sig. reduction of negative affect, sig. improvement of positive affect (F(1, 21) = 5.06, p < 0.05), and sig. reduction of cortisol concentration in saliva through tango dance with music and partner (F(1, 19)= 5.45, p < 0.05). The effect was dependent on the music, but not on the partner. |
| West et al. (2004) [76] | IIa | Comparison of African Dance and Hatha Yoga regarding their influence on well-being | 69 Students 47f/22m M = 19 years | 3 × 3 factorial, controlled | 3 Conditions: 1. Hatha Yoga 2. African Dance 3. Biology Lecture 90 min courses, single session | Stress: Perceived Stress Scale (PSS), Positive and Negative Affect Schedule (PANAS), saliva samples for the measurement of cortisol | Multivariate Analysis of Variance (MANOVA) with repeated measures | Sig. reduction of perceived stress and negative affect as well as improvement of the positive affect in Hatha Yoga and in African dance: F(2, 66) =11.77, p < 0.0001; Sig. reduction in cortisol concentration in saliva in the yoga condition (F(2, 59) = 17.28, p < 0.0001); Increase of cortisol in saliva in the dance condition and no change of cortisol in the control condition. |
| Wiedenhofer & Koch (2016) [77] | IIa | Comparison of non-goal-directed movement and goal-directed movement in terms of their influence on stress and well-being | N = 57 Students, 44f/12m M = 23.21 | Two-factorial, controlled, pre-post design | EG: non-goal-directed movement improvisation to music, one-time participation 40–50 min. CG: goal-directed movement improvisation to the same music. Colorful post it-notes were used as target points in the room, one-time participation | Perceived Stress: PSQ30 questionnaire Well-being: HSI (Heidelberg State Inventory) Self-efficacy: General Perceived Self-Efficacy Scale (GSE scale) Body-self-efficacy: Self-Efficacy-Scale (BSE) | MANOVA with repeated measures t-tests for paired samples | Perceived stress in EG sig. more reduced than in CG F(56,1) = 4.71, p = 0.034 ; Body-Self-efficacy increased sig. in EG F(56,1) = 7.00, p = 0.011, no difference in well-being:. |
| Time of Publication | Evidence Level | ||||||
|---|---|---|---|---|---|---|---|
| Arts Modality | 1980–1999 | 2000–2016 | Total | Ib | IIa | IIb | III |
| Art therapy/art interventions | 0 (0/0) | 11 (0/11) | 11 (0/11) | 8 (0/8) | 0 (0/0) | 2 (0/2) | 1 (0/1) |
| Music therapy/music interventions | 5 (1/4) | 15 (10/5) | 20 (11/9) | 16 (9/7) | 2 (2/0) | 0 (0/0) | 2 (0/2) |
| Dance/movement therapy/dance interventions | 0 (0/0) | 6 (1/5) | 6 (1/5) | 3 (1/2) | 3 (0/3) | 0 (0/0) | 0 (0/0) |
| Drama therapy/drama interventions | 0 (0/0) | 0 (0/0) | 0 (0/0) | 0 (0/0) | 0 (0/0) | 0 (0/0) | 0 (0/0) |
| Total | 5 | 32 | 37 | 27 | 5 | 2 | 3 |
© 2018 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Martin, L.; Oepen, R.; Bauer, K.; Nottensteiner, A.; Mergheim, K.; Gruber, H.; Koch, S.C. Creative Arts Interventions for Stress Management and Prevention—A Systematic Review. Behav. Sci. 2018, 8, 28. https://doi.org/10.3390/bs8020028
Martin L, Oepen R, Bauer K, Nottensteiner A, Mergheim K, Gruber H, Koch SC. Creative Arts Interventions for Stress Management and Prevention—A Systematic Review. Behavioral Sciences. 2018; 8(2):28. https://doi.org/10.3390/bs8020028
Chicago/Turabian StyleMartin, Lily, Renate Oepen, Katharina Bauer, Alina Nottensteiner, Katja Mergheim, Harald Gruber, and Sabine C. Koch. 2018. "Creative Arts Interventions for Stress Management and Prevention—A Systematic Review" Behavioral Sciences 8, no. 2: 28. https://doi.org/10.3390/bs8020028
APA StyleMartin, L., Oepen, R., Bauer, K., Nottensteiner, A., Mergheim, K., Gruber, H., & Koch, S. C. (2018). Creative Arts Interventions for Stress Management and Prevention—A Systematic Review. Behavioral Sciences, 8(2), 28. https://doi.org/10.3390/bs8020028