1. Introduction
Managerial practices in the healthcare sector are facing considerable challenges to improve the performance of medical staff in the ever-growing hospital market conditions. In the opinion of Reference [
1], nurses, among all healthcare practitioners, are the front-line care of patients in providing timely, quality health services in hospitals. Nurses also make up the largest human resource in healthcare organizations, and nursing performance remains a long-standing determinate of the quality of patient care. Therefore, the assessment of factors influencing the performance of nurses became essential for scholars and hospital management executives. This study, however, is particularly interested in Vietnamese hospital nurses.
Previous studies explored a variety of factors affecting job performance such as working environment, interpersonal relationships, job satisfaction, commitment, leadership styles, etc. [
2,
3,
4]. This study focused on interpersonal relationships in the workplace and how these interactions affected the working manner and performance of employees. The extant scholarship indicates that employees who are well informed through relationships at work report higher levels of job satisfaction and commitment [
5,
6]. The higher the workplace interaction quality, the better informed employees are and, in turn, the less uncertain they are about tasks and goals and the better the perceived performance [
7].
Of particular interest, the ways in which workplace relationships may influence the received information and resources were discussed through two primary sources of relationships with supervisors and colleagues. Prior studies showed evidence on the positive connections between these two relationship categories and the performance appraisal ratings of employees [
8,
9,
10]. In light of this, employees can rely on their immediate leaders for an exchange of technical skills and resources, and the high-quality relationship with supervisors is associated with a higher level of trust, respect, obligation, support, and encouragement [
11]. Otherwise, coworker relationships provide employees the source of emotional and instrumental support as they have an understanding of the internal working environment [
12]. However, the literature on coworker relationships appears inconsistent regarding the healthcare sector, in which peer cohesion was less available between staff nurses who usually work on different rotating shifts [
13,
14]. Most of the related research focused on European countries and the United States.
Healthy workplace relationships receive a lot of interest since they are associated with the benefits of employees [
15] and achieving the goals of the organization [
16]. In addition, several previous studies also concentrated on examining the role of staff nurses’ participation in decision-making processes to improve the organizational process [
17] and create a strong impact of health institution management models on clinical practice [
18], as well as seeking clinical practice benchmarking to improve the quality of care [
19], and identifying alternative models of effective funding systems in the national health service [
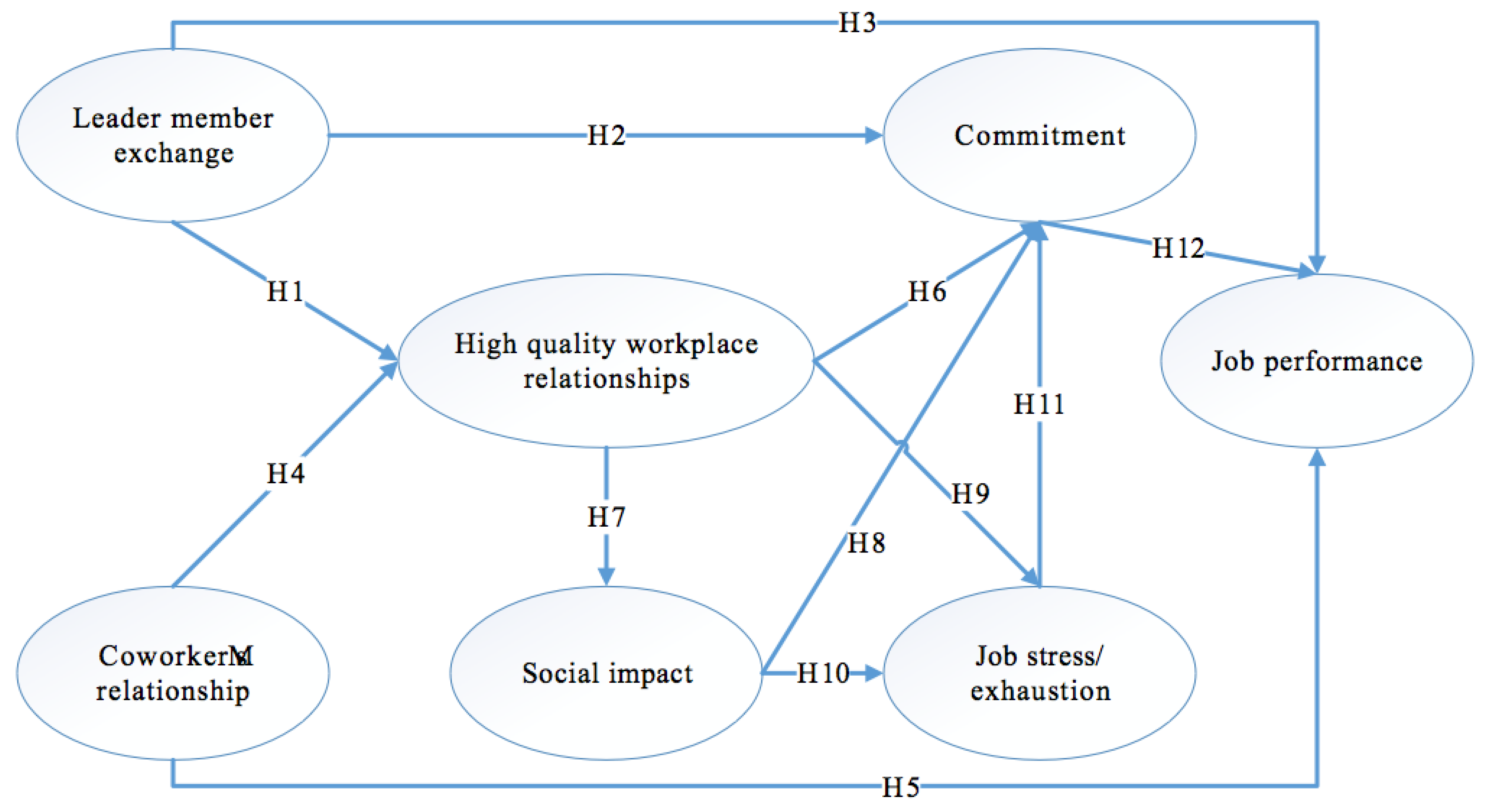
20]. To further investigate this stream of research, Caillier [
21] investigated the impact of high-quality workplace relationships on the overall performance of the organization through employee behaviors such as commitment, social impact, and job stress/exhaustion. However, the significance of healthy interpersonal relationships at work in Vietnam is of critical concern; however, it remains unexplored in research.
Since current research possesses little evidence about the expected impact of relationships at work on employee working manner, this paper aims to clarify the way in which healthy workplace interactions affect the working behaviors of staff nurses (commitment, stress level, the awareness level of social impact) and performance ratings by examining two subcategories of relationships individually. This study followed the same path as Li and Hung [
22], who examined two subtypes of relationships separately and also grouped these types of relationships into one variable proposed by Hansen [
23], allowing the consideration of separate effects and a whole effect.
3. Methodology
To test the research model and proposed hypotheses, this paper adopted a quantitative method where data were gathered by means of large-sample survey. The measures, sample and data collection, and data analysis technique are presented below.
3.1. Measures
Referring to an extensive literature review, the study constructed a 33-item measurement scale to examine the latent variables observed. Firstly, the rate of the relationship with managers was assessed through the five-item scale from Graen and Uhl-Bien’s [
31], which measures LME. Secondly, a three-item scale was adopted from Kram and Isabella [
95] and typology relationships (three peer relationships distinguished by developmental and psychosocial function) [
96,
97] to assess coworker relationships. Each item was used to describe each type of coworker relationship by Sias [
11]. Thirdly, high-quality workplace relationships were examined by the three-item scale from Hansen [
23]. Fourthly, the social impact was assessed by the six-item scale following Bullock et al., [
68] which included the definition of the social impact developed by Grant [
67] (p. 51) (the actions of employees that make differences to others), and the same items built by Grant and Campbell [
98]. Fifthly, instead of testing separately the two indicators of job stress/exhaustion by Steiber and Pichler [
99], the study combined two indicators to make a five-item scale to measure job stress/exhaustion. This was in accordance with the theory of the Maslach Burnout Inventory developed by Maslach and Jackson [
100]. Sixthly, a seven-item scale was applied by Bullock et al., [
68] and Allen and Meyer [
6] to examine the commitment. Finally, job performance was investigated through the four-item scale stated by Colquitt et al. [
101]. A five-point Likert scale (1 = strongly disagree, 5 = strongly agree) was used to evaluate the level of respondents’ agreement.
3.2. Sample and Data Collection
In the sampling process, one of the most important questions is how many observations or respondents to use for the research sample. Deciding on the appropriate sample size is “an important and complex issue” which “depends on the statistical estimating precision needed by the researcher and the number of variables” [
102]. Although larger sample sizes always provide better projection of the whole population, it is supported that a range from 200 to 400 is considered to be critical for multiple regression and path analysis [
103]. Green [
104] and Tabachmick and Fidell [
105] suggest a rule of thumb for determining the sample size. Accordingly, sample size = 50 + (8 × number of measurement items). Because there were overall 33 items used for the measurement of the model’s constructs, a total of 314 observations was considered to be effective sample size.
Since the purpose of the study was clarified, we contacted the Department of Health in both Ho Chi Minh City and Binh Duong province, Vietnam to get references for the list of hospitals. Then, we attempted to contact hospital managers to ask for help conducting the questionnaire survey. This enabled the delivery of the majority of the questionnaires to be done in person and to utilize the managers’ personal contact with many nurses. Consequently, researchers received the approval of hospital authorities from four hospitals in Ho Chi Minh City and two hospitals in Binh Duong province, Vietnam to conduct the questionnaire survey.
In order to assure ethical requirements, a cover letter was introduced in the first page of the questionnaire survey where the purpose of this study was clearly identified. It also involved the authors’ names, addresses, and university of the authors with the perspective of increasing the confidence of the staff nurse employees and for them to be familiar with whom they were answering as mentioned by Reference [
106]. Researchers ensured that respondents’ information was kept confidential, used only for academic purposes. Firstly, the questionnaire was translated into Vietnamese and it was checked and corrected by an English lecturer. However, the first Vietnamese version was not easily understandable. Secondly, researchers conducted a pilot test of face-to-face interviews with 30 staff nurses in March 2018. The results of the pilot test enabled researchers to verify and modify the final questionnaire for easy understanding and improving the response rate under the Vietnamese context.
With kind support from hospital managers, researchers distributed 80 questionnaires in each hospital. The managers assisted researchers in asking staff nurses to fill in the questionnaire. Researchers stopped by each hospital every weekend to receive the completed questionnaires. It took about three months to finish the data collection from April to June 2018. Out of the 480 questionnaires delivered to staff nurses in six hospitals, 382 responses were returned. However, 77 questionnaires were eliminated from the analysis because of missing data in the responses, effectively completing a response rate of 63.12% (303 responses) of usable responses for this study. A copy of the final questionnaire used in this paper is presented in
Appendix A.
3.3. Data Analysis Technique
Firstly, exploratory factor analysis (EFA) was implemented to all scales together for a preliminarily assessment of dimensionality, convergence, and discriminant validity. Secondly, confirmatory factor analysis (CFA) was carried out to test the full measurement model which included seven constructs and their respective items.
5. Discussion
Among the two sources of workplace relationships, LME was indicated to be positively and significantly related to workplace relationship quality, employee commitment, and performance appraisal. These hypotheses support that high levels of LME, which feature mutual trust, emotional support, respect, and reciprocal influence create many positive outcomes including higher standard of patient care [
77,
113], greater job commitment, and stronger performance ratings [
114]. These results are consistent with a majority of previous studies. Regarding nursing management, the findings agreed with Brunetto and Wharton [
115] regarding positive connections between LME levels and the degree of nurses’ commitment and were in line with Han and Jekel [
116] about the negative influence of high LME levels on nurse turnover rate in the United States. Additionally, in accordance with social exchange theory, the results support a recent study of Sepdiningtyas et al. [
117] where LME was positively related to individual performance in the nursing profession.
The results, however, pointed out the insignificant contribution of coworker relationships among Vietnamese hospital nurses in improving workplace relationship quality and job performance. This was explained by the fact that nursing has its own special characteristics when compared to other professions. The exchange of information and support is not highly valued among staff nurses since they usually follow their own work shifts or are in charge of different tasks and care areas. This line of reasoning is highly consistent with Blake [
50], who argued that high levels of workplace environment were generated by effective communication and collaboration, and decision-making promotion among nurses. These reasons also support the insignificance of peer relationships and job performance. The study opposed Wong et al. [
118] that weighted peer interactions, as the stronger driver on work engagement than supervisory relationships, were explained by the more frequent peer communications. The finding also contradicted previous studies in nursing by AbuAl-Rub [
119] and Amarneh et al. [
120] who reported a positive relationship between coworker social support and job performance among hospital nurses in the United States and Jordan, respectively.
The results indicate that high-quality workplace relationship was negatively and significantly related to job stress, which is highly consistent with previous studies [
16,
77,
78,
79,
80]. This is implied by the fact that, within positive workplace relationships, nurses are powered by instrumental resources and emotional support from supervisors and peers, which results in a lower level of reported stress. Moreover, the findings revealed that high-quality workplace relationships were considered as a significant driver of social impact. This is because a positive workplace relationship quality creates an understanding for the nurses of what they are doing and their awareness of the difference they are making in society. The results agree with Caillier [
21] in the positive influence of high-quality workplace relationships on social impact among nurses. Additionally, there was a significant coefficient describing the positive interaction of social impact and job stress. A potential clarification could be that nurses who realize the impact they have on others put more effort and time toward preserving this aim. As a result, they reported a lower level of job stress or exhaustion. In the end, the study concluded on the mediating effect of social impact on the correlation between high-quality workplace relationship and job stress among staff nurses, which was highly consistent with Caillier [
21]. Such workplace relationship quality stems from a transformational leadership style, which is described through the ideals of influence, inspiring motivation, individualized consideration, and intellectual stimulation [
22,
82,
121]. Hence, transformational leaders provide staff with meaningful tasks and goals [
83,
84], which in turn enhances the social impact among nurses and contributes to relieving job stress [
83].
Extracted from the results, it was observed that high-quality workplace relationships were positively and significantly related to nurse commitment. These findings support the previous findings ([
122], [
58] and [
21]), they contended that interactions with leaders and peers in a positive workplace relationship enhanced employee psychological attachment to the organization. Furthermore, social impact was found as an insignificant influential factor on nurses’ attachment to the organization. The fact is that the nursing profession is likely to be undervalued by the public since they believe that nurses simply follow doctors’ instructions. However, nurses tend to believe in their professional goals to do good for society, contribute effortlessly in caring, and have a personal feeling of pride for their profession [
72,
73]. Consistent with this view, nurses remain working in the nursing sector and preserve the loyalty to their profession [
72]. Since social impact is not a significant driver of nurse commitment, the result otherwise rejects [
21] regarding the mediating effect of social impact on the relationship between high-quality workplace relationship and nurse commitment.
Finally, the study demonstrated that organizational commitment emerged as an insignificant driver of the staff nurses’ performance in Vietnamese hospitals. This finding contradicts most of the previous research along this line. However, the study supported studies of Angle and Lawson [
92], and Mathieu and Zajac’s [
93], where the influence of commitment on perceived organizational performance was perceived negative, insignificant, or even weak. The variation can be explained by the way in which commitment and performance were conceptualized in each study. Gong et al. [
123] examined different categories of organizational commitment and found out that, although affective commitment was explored to enhance job performance, continuance commitment was not. Meanwhile, Schrock et al. [
124] reported the negative association between continuance commitment on job performance. Additionally, Biçer et al.,’s study [
94] did not conclude a statistically significant interaction between affective commitment and perceived organizational performance. This is likely attributable to the fact that variable design shortcoming and other ambiguities suggest potential associations between kinds of commitment and job performance among Vietnamese hospital nurses. Several suggestions were proposed to enhance the understanding on this relationship, including investigating potential moderators [
93], and examining different dimensions of performance [
92] and commitment (affective, continuance, and normative).
6. Conclusions
This paper aimed to examine the drivers of job performance among nurses in Vietnamese hospitals, paying attention to the significance of the quality of workplace interpersonal interactions. Since a positive workplace relationship is of crucial importance for the proper functioning and goal achievement of an organization, this study established an integrated model that aimed to explain the expected association of a high-quality workplace relationship, its subcategories, and working attitudes of Vietnamese hospital nurses. The findings showed that only the leader–member exchange relationship was a direct and significant predictor of high-quality workplace relationships and nurse performance, but not coworker relationships. Additionally, it also revealed that a healthy workplace relationship created a significant contribution to enhancing nurse commitment, relieving job stress/exhaustion, and increasing the perception of nurses about the social impact of the nursing profession. Unfortunately, the study did not demonstrate the significant relationship between commitment and job performance, and further research would need to be conducted to investigate the connections between the two concepts in the Vietnamese context. The divergence between the majority of previous studies on the commitment–performance relationship and that in the Vietnamese hospital context was also explained.
This study contributes to the extant research in two ways. Firstly, the paper firstly clarifies the process via which healthy workplace interactions affect the working behaviors of staff nurses (commitment, stress level, the awareness level of social impact) and performance ratings by examining two subcategories of relationships individually. Secondly, the study confirmed the significance of the association between workplace relationships, employee work attitudes, and job performance by considering different characteristics of the Vietnamese healthcare industry.
The findings of this study will provide valuable evidence and implications for healthcare management with regards to the importance of enhancing interpersonal interactions and performance ratings. Adequate attention should be paid to prioritizing solid interactions among staff nurses when they are demonstrated to have no contribution to the quality of workplace relationships and job performance among Vietnamese hospital nurses. Since such actions may improve the workplace relationship quality and job performance, this will in turn increase commitment, reduce stress levels, and improve nurses’ awareness of social impact.
In spite of the limitations, further studies may advance this line of research by widening the measurement variables of job commitment and performance to gain a deeper understanding about the connection between these two concepts among nurses in Vietnam. In addition, considering the generalizability of the findings, future research should examine other potential job performance drivers and any positive outcomes of coworker relationships in nurse performance and nurses’ working attitudes among various hospital sizes and characteristics. Another obvious limitation is that a larger-scale study across several countries should be conducted to eliminate the possible effects of the disparity between countries on the quality of healthcare services.


{kind=link}
