
Still Searching: A Meta-Synthesis of a Good Death from the Bereaved Family Member Perspective

Abstract
:1. Introduction
2. Materials and Method
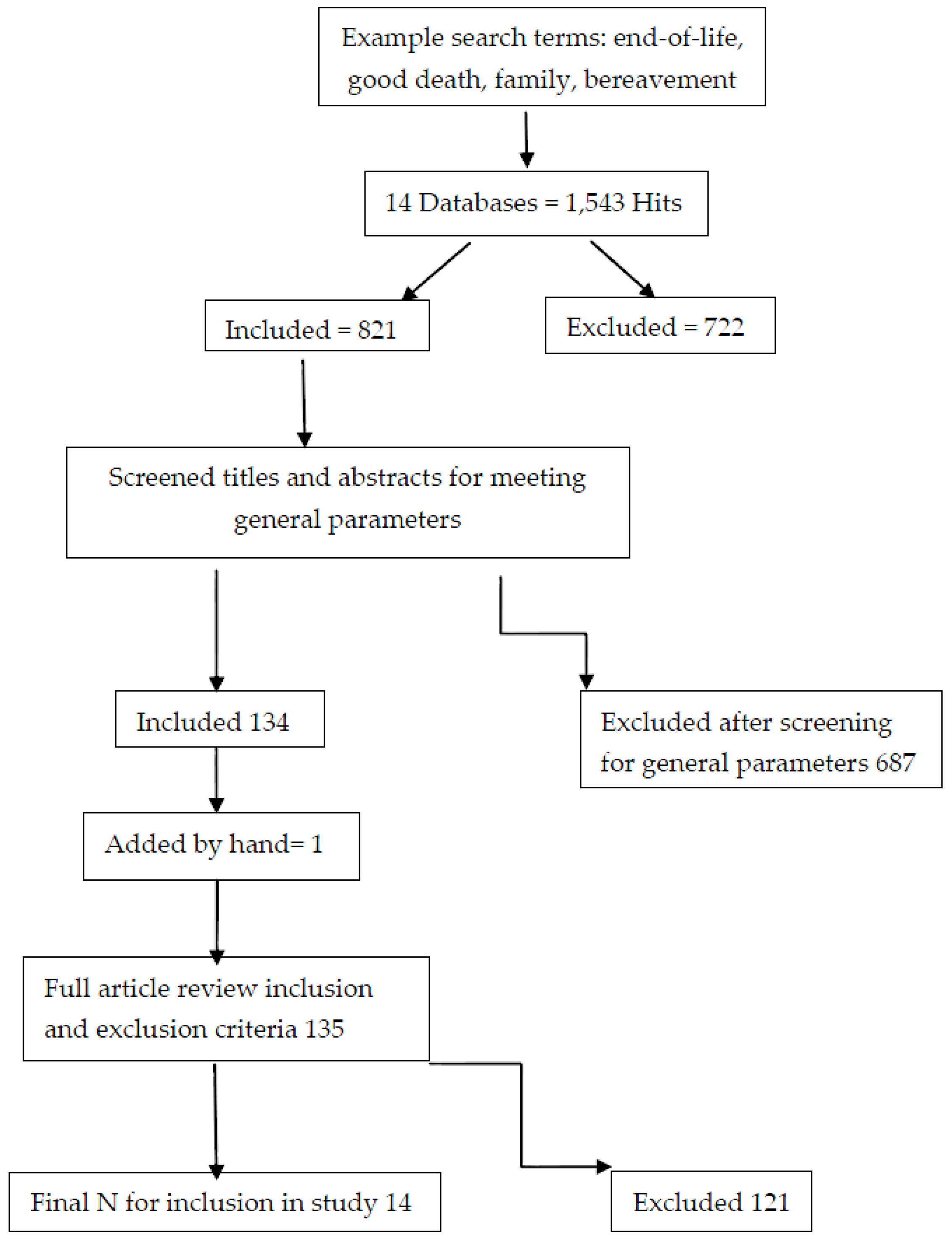
2.1. Step 1: Literature Search Process
2.1.1. Inclusion vs. Exclusion
2.1.2. Search Results
2.2. Step 2: Quality Appraisal
2.3. Step 3: Classification Findings
2.4. Step 4: Data Abstraction and Synthesis
2.5. Validity
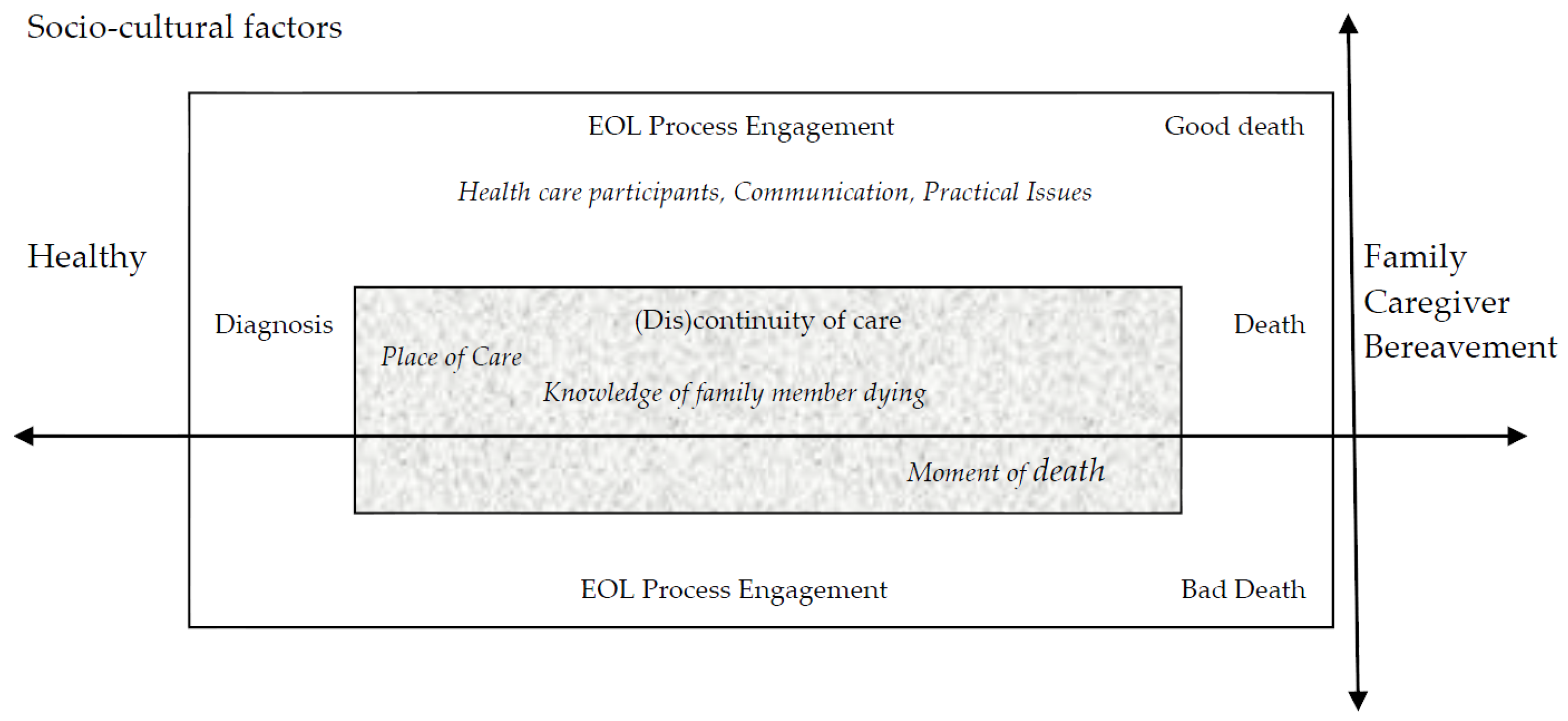
3. Results
3.1. Socio-Cultural Factors
3.2. EOL Process Engagement
3.2.1. Healthcare Participants
3.2.2. Communication
3.2.3. Practical Issues
3.3. (Dis)continuity of Care
3.3.1. Place of Care
3.3.2. Knowledge of Family Member Dying
3.3.3. Moment of Death
3.4. Good vs. Bad Death Experiences
3.5. Presence
4. Discussion
5. Conclusions
Conflicts of Interest
Appendix A

{kind=link}
{kind=link}
| Source/Country | Aim/Purpose | Methods/Data Collection | Sample N | Bereavement Period | Classification and QA Score |
|---|---|---|---|---|---|
| Holdsworth, (2015) [45] United Kingdom | “The aim of this article is to describe the end-of-life experience from the point of view of bereaved family carers with particular reference to the role that care providers play in shaping this experience” [45] (p. 835). | Interviews | 45 | 6–10 months | Thematic/21 |
| Wilson, MacLeod, & Houttekier, (2016) [48] Canada | “As it does not appear that research has focused on a linkage between death quality and the intensity of bereavement grief, we conducted a mixed-methods research study to determine if this relationship exists and for evidence-based insights into any connections between bereavement grief and death quality” [48] (p. 261). | Interviews | 41 | 5 months–8 years | Thematic/18 |
| Nelson, Schrader, & Eidsness, (2009) [54] United States | “The aim of this study was to explore end-of-life (EOL) experiences of South Dakotans who had experienced the death of a loved one in the last 5 years” [54] (p. 905). | Interviews | 35 | Within 5 years | Topical/14 |
| Lee, Woo, & Goh, (2013) [19] Singapore | “The aim of this study was to examine the concept of a good death from the perspectives of both the dying person and the family caregiver, as perceived by bereaved family caregivers of advanced cancer patients” [19] (p. 37). | 5 focus groups, 1 interview | 18 | 6–18 months | Thematic/16 |
| Kongsuwan, Chaipetch, & Matchim, (2012) [55] Thailand | “The purpose of the study was to describe the concept of a peaceful death in ICUs from Thai Buddhist family members’ perspectives” [55] (p.152). | Interviews | 9 | 2–12 months | Conceptual/20 |
| Abib El Halal, Piva, Lago, El Halal, Cabral, Nilson, & Garcia, 2013 [47] Brazil | “The aim of this study was to explore parents’ perspectives of the quality of the care offered to them and their terminally ill child in the child’s last days of life in two Brazilian PICUs” [47] (p. 496). | Semi-structured interview | 15 | 6–12 months | Thematic/16 |
| Donnelly & Battley, (2010) [49] Ireland | “To describe the contemporary experience of relatives in a tertiary referral hospital of the moment of death, traditionally a very significant event” [49] (p. 96). | Interviews | 24 | Unclear | Topical/18 |
| Robert, Zhukovsky, Mauricio, Gilmore, Morrison, & Palos; (2012) [51] United States | “To understand the needs and experiences of bereaved parents whose child had received care at one National Cancer Institute-designated comprehensive cancer center. The investigators were particularly interested in the parents’ perceptions of the care received by their child, their expectations of palliative care, and recommendations on how best to improve palliative care for children with cancer and their parents” [51] (p. 318). | Focus groups | 14 | Lost a loved one a minimum of one year before study | Thematic/20 |
| Evans, Cutson, Steinhauser, & Tulsky (2006) [52] United States | “To describe caregivers’ reasons for transfer from home hospice to inpatient facilities, preferences for site of care and death, and their experiences during these transfers” [52] (p. 100). | Interviews | 18 | Contacted about study at least four weeks after patient death | Thematic/17 |
| Jack, O'Brien, Scrutton, Baldry, & Groves, (2015) [53] United Kingdom | “To explore bereaved family carers’ perceptions and experiences of a hospice at home service” [53] (p. 131). | Interviews | 20 | At least 3 months | Conceptual/20 |
| Williams, Bailey, Noh, Woodby, Wittich & Burgio (2015) [56] United States | “The purpose of this qualitative study was to explore the personal and interpersonal context of next-of-kin’s discussions with clinicians regarding discharge planning to home hospice or inpatient palliative care service for hospitalized veterans” [56] (p. 51). | Participant obser-vation, focus groups, and interviews | 78 | 3–6 months | Interpretive/17 |
| Wilches-Gutiérrez, Arenas-Monreal, Paulo-Maya, Peláez-Ballestas, & Idrovo, (2012) [46] Mexico | “To ascertain the elements comprising the health/illness /death process in the context of a holiday in this municipality (Yautepec, Morelos, Mexico)” [46] (p. 775). | Interviews | 7 | Loss within the last four years | Conceptual/18 |
| Bruinsma, Brown, van der Heide, Deliens, Anquinet, Payne, Seymour, & Rietjens, (2014) [20] Belgium, United Kingdom, Netherlands | “The purpose of the study was to explore relatives’ descriptions and experiences of continuous sedation in end-of-life care for cancer patients and to identify and explain differences between respondents from the Netherlands, Belgium, and the UK” [20] (p. 3243). | Interviews | 38 | 3–18 months | Thematic/18 |
| Workman & Mann, (2007) [50] Canada | “To identify areas for improvement in delivering high quality end-of-life care on the medical teaching unit” [50] (p. 433). | Interviews | 6 | 6 months | Thematic/15 |
References
- Twycross, R. Patient care: Past, Present, and Future. Omega J. Death Dying 2007, 56, 7–19. [Google Scholar] [CrossRef]
- Masson, J.D. Non-Professional Perceptions of ‘Good Death’: A Study of the Views of Hospice Care Patients and Relatives of Deceased Hospice Care Patients. Mortality 2002, 7, 191–209. [Google Scholar] [CrossRef]
- Van Gennip, I.E.; Pasman, H.R.W.; Kaspers, P.J.; Oosterveld-Vlug, M.G.; Willems, D.L.; Deeg, D.J.H.; Onwuteaka-Philipsen, B.D. Death with Dignity from the Perspective of the Surviving Family: A Survey Study Among Family Caregivers of Deceased Older Adults. Palliat. Med. 2013, 27, 616–624. [Google Scholar] [CrossRef] [PubMed]
- Good, M.J.D.; Gadmer, N.M.; Ruopp, P.; Lakoma, M.; Sullivan, A.M.; Redinbaugh, E.; Arnold, R.M.; Block, S.D. Narrative Nuances on Good and Bad Deaths: Internists’ Tales from High-Technology Work Places. Soc. Sci. Med. 2004, 58, 939–953. [Google Scholar] [CrossRef]
- Lee, H.J.; Jo, K.H.; Chee, K.H.; Lee, Y.J. The Perception of Good Death among Human Services Students in South Korea: A Q-methodological Approach. Death Stud. 2008, 32, 870–890. [Google Scholar] [CrossRef] [PubMed]
- Miyashita, M.; Morita, T.; Sato, K.; Hirai, K.; Shima, Y.; Uchitomi, Y. Good Death Inventory: A Measure for Evaluating Good Death from the Bereaved Family Member’s Perspective. J. Pain Symptom Manag. 2008, 35, 486–498. [Google Scholar] [CrossRef] [PubMed]
- Patrick, D.L.; Engelberg, R.A.; Curtis, J.R. Evaluating the Quality of Dying and Death. J. Pain Symptom Manag. 2001, 22, 717–726. [Google Scholar] [CrossRef]
- Griggs, C. Community Nurses’ Perceptions of a Good death: A Qualitative Exploratory Study. Int. J. Palliat. Nurs. 2010, 16, 140–149. [Google Scholar] [CrossRef] [PubMed]
- Cipolletta, S.; Oprandi, N. What is a Good Death? Health Care Professionals’ Narrations on End-of-Life Care. Death Stud. 2014, 38, 20–27. [Google Scholar] [CrossRef] [PubMed]
- Cheng, S.-Y.; Hu, W.-Y.; Liu, W.-J.; Yao, C.-A.; Chen, C.-Y.; Chiu, T.-Y. Good Death Study of Elderly Patients with Terminal Cancer in Taiwan. Palliat. Med. 2008, 22, 626–632. [Google Scholar] [CrossRef] [PubMed]
- Granda-Cameron, C.; Houldin, A. Concept Analysis of Good Death in Terminally ill Patients. Am. J. Hosp. Palliat. Med. 2012, 29, 632–639. [Google Scholar] [CrossRef] [PubMed]
- Steinhauser, K.E.; Clipp, E.C.; McNeilly, M.; Christakis, N.A.; McIntyre, L.M.; Tulsky, J.A. In Search of a Good Death: Observations of Patients, Families, and Providers. Ann. Intern. Med. 2000, 132, 825–832. [Google Scholar] [CrossRef] [PubMed]
- Meier, E.A.; Gallegos, J.V.; Montross-Thomas, L.P.; Depp, C.A.; Irwin, S.A.; Jeste, D.V. Defining a Good Death (Successful Dying): Literature Review and a Call for Research and Public Dialogue. Am. J. Geriatr. Psychiatry 2016, 24, 261–271. [Google Scholar] [CrossRef] [PubMed]
- Munn, J.C.; Dobbs, D.; Meier, A.; Williams, C.S.; Biola, H.; Zimmerman, S. The End-of-Life Experience in Long-Term Care: Five Themes Identified from Focus Groups with Residents, Family Members, and Staff. Gerontologist 2008, 48, 485–494. [Google Scholar] [CrossRef] [PubMed]
- Pattison, N.; Carr, S.M.; Turnock, C.; Dolan, S. ‘Viewing in Slow Motion’: Patients’, Families’, Nurses’ and Doctors’ Perspectives on End-of-Life Care in Critical Care. J. Clin. Nurs. 2013, 22, 1442–1454. [Google Scholar] [CrossRef] [PubMed]
- Leichtentritt, R.D.; Rettig, K.D. The Good Death: Reaching an Inductive Understanding. Omega 2000, 41, 221–248. [Google Scholar] [CrossRef] [PubMed]
- Rainsford, S.; MacLeod, R.D.; Glasgow, N.J.; Wilson, D.M.; Phillips, C.B.; Wiles, R.B. Rural Residents’ Perspectives on the Rural “Good Death”: A Scoping Review. Health Soc. Care Community 2016. [Google Scholar] [CrossRef] [PubMed]
- Hsu, M.; Kahn, D.L.; Hsu, M. A Single Leaf Orchid: Meaning of a Husband’s Death for Taiwanese Widows. Ethos 2002, 30, 306–326. [Google Scholar] [CrossRef]
- Lee, G.L.; Woo, I.M.H.; Goh, C. Understanding the Concept of a Good Death among Bereaved Family Caregivers of Cancer Patients in Singapore. Palliat. Support. Care 2013, 11, 37–46. [Google Scholar] [CrossRef] [PubMed]
- Bruinsma, S.M.; Brown, J.; van der Heide, A.; Deliens, L.; Anquinet, L.; Payne, S. Making Sense of Continuous Sedation in End-of-Life Care for Cancer Patients: An Interview Study with Bereaved Relatives in Three European Countries. Support. Care Cancer 2014, 22, 3243–3252. [Google Scholar] [CrossRef] [PubMed]
- Hirai, K.; Miyashita, M.; Morita, T.; Sanjo, M.; Uchitomi, Y. Good Death in Japanese Cancer care: A Qualitative Study. J. Pain Symptom Manag. 2006, 31, 140–147. [Google Scholar] [CrossRef] [PubMed]
- Grant, E.; Murray, S.A.; Grant, A.; Brown, J. A Good Death in Rural Kenya? Listening to Meru Patients and their Families Talk about Care Needs at the End of Life. J. Palliat. Care 2003, 19, 159–167. [Google Scholar] [PubMed]
- Carr, D. A “Good Death” for Whom? Quality of Spouse’s Death and Psychological Distress among Older Widowed Persons. J. Health Soc. Behav. 2003, 44, 215–232. [Google Scholar] [CrossRef] [PubMed]
- Maeda, I.; Miyashita, M.; Yamagishi, A.; Kinoshita, H.; Shirahige, Y.; Izumi, N.; Yamaguchi, T.; Igarashi, M.; Kato, M.; Morita, T. Changes in Relatives’ Perspectives on Quality of Death, quality of Care, Pain Relief, and Caregiving Burden Before and After a Region-Based Palliative Care Intervention. J. Pain Symptom Manag. 2016, 52, 637–645. [Google Scholar] [CrossRef] [PubMed]
- Rainsford, S.; MacLeod, R.D.; Glasgow, N.J.; Wilson, D.M.; Phillips, C.B.; Wiles, R.B. Rural End-of-Life Care from the Experiences and Perspectives of Patients and Family Caregivers: A Systematic Literature Review. Palliat. Med. 2017. [Google Scholar] [CrossRef] [PubMed]
- Quill, T.E. Initiating End-of-Life Discussions with Seriously Ill Patients: Addressing the Elephant in the Room. J. Am. Med. Assoc. (JAMA) 2000, 284, 2502–2507. [Google Scholar] [CrossRef]
- Pecchioni, L.L.; Overton, C.B.; Thompson, T. Families communicating about health. In The Sage Handbook of Family Communication; Turner, L.H., West, R., Eds.; Sage: Los Angeles, CA, USA, 2015; pp. 306–319. [Google Scholar]
- Stajduhar, K.I.; Funk, L.; Outcalt, L. Family Caregiver Learning-How Family Caregivers Learn to Provide Care at the End of Life: A Qualitative Secondary Analysis of Four Datasets. Palliat. Med. 2013, 27, 657–664. [Google Scholar] [CrossRef] [PubMed]
- Linderholm, M.; Friedrichsen, M. A Desire to Be Seen: Family Caregivers’ Experiences of their Caring Role in Palliative Home Care. Cancer Nurs. 2010, 33, 28–36. [Google Scholar] [CrossRef] [PubMed]
- Gladding, S.T. Family Therapy: History, Theory, and Practice, 5th ed.; Pearson Education, Inc.: Upper Saddle River, NY, USA, 2011. [Google Scholar]
- Miyajima, K.; Fujisawa, D.; Yoshimura, K.; Ito, M.; Nakajima, S.; Shirahase, J.; Mimura, M.; Miyashita, M. Association Between Quality of End-of-Life Care and Possible Complicated Grief Among Bereaved Family Members. J. Palliat. Med. 2014, 17, 1025–1031. [Google Scholar] [CrossRef] [PubMed]
- Jackson, J.; Derderian, L.; White, P.; Ayotte, J.; Fiorini, J.; Hall, R.O.; Shay, J.T. Family Perspectives on End-of-Life Care: A Metasynthesis. J. Hosp. Palliat. Nurs. 2012, 14, 303–311. [Google Scholar] [CrossRef]
- Bosticco, C.; Thompson, T. The Role of Communication and Storytelling in the Family Grieving System. J. Fam. Commun. 2005, 5, 255–278. [Google Scholar] [CrossRef]
- Campbell, R.; Pound, P.; Pope, C.; Britten, N.; Pill, R.; Morgan, M.; Donovan, J. Evaluating Meta-Ethnography: A Synthesis of Qualitative Research on Lay Experiences of Diabetes and Diabetes Care. Soc. Sci. Med. 2003, 56, 671–684. [Google Scholar] [CrossRef]
- Hammell, K. Quality of Life after Spinal Cord Injury: A Meta-Synthesis of Qualitative Findings. Spinal Cord 2007, 45, 124–139. [Google Scholar] [CrossRef] [PubMed]
- Evans, C.J.; Harding, R.; Higginson, I.J. ‘Best practice’ in Developing and Evaluating Palliative and End-of-Life Care Services: A Meta-Synthesis of Research Methods for the MORECare Project. Palliat. Med. 2013, 27, 885–898. [Google Scholar] [CrossRef] [PubMed]
- May, C.R.; Masters, J.; Welch, L.; Hunt, K.; Pope, C.; Myall, M.; Griffiths, P.; Roderick, P.; Glanville, J.; Richardson, A. EXPERTS 1-Experiences of Long-Term Life-Limiting Conditions Among Patients and Carers: Protocol for a Qualitative Meta-Synthesis and Conceptual Modelling Study. BMJ Open 2015, 5, e007372. [Google Scholar] [CrossRef] [PubMed]
- Sandelowski, M.; Barroso, J. Handbook for Synthesizing Qualitative Research; Sandelowski, M., Barroso, J., Eds.; Springer Publishing Company: New York, NY, USA, 2007; Available online: http://ebookcentral.proquest.com/lib/buffalo/detail.action?docID=423305 (accessed on 23 January 2017).
- Mohammed, M.; Moles, R.; Chen, T. Meta-Synthesis of Qualitative Research: The Challenges and Opportunities. Int. J. Clin. Pharm. 2016, 38, 695–704. [Google Scholar] [PubMed]
- Duggleby, W.; Hicks, D.; Nekolaichuk, C.; Holtslander, L.; Williams, A.; Chambers, T.; Eby, J. Hope, Older Adults, and Chronic Illness: A Meta-Synthesis of Qualitative Research. J. Adv. Nurs. 2012, 68, 1211–1223. [Google Scholar] [CrossRef] [PubMed]
- Hammell, K.W. Informing Client-Centred Practice through Qualitative Inquiry: Evaluating the Quality of Qualitative Research. Br. J. Occup. Ther. 2002, 65, 175–184. [Google Scholar] [CrossRef]
- Critical Appraisal Skills Programme (CASP). 10 Questions to Help You Make Sense of Qualitative Research. 2013. Available online: http://media.wix.com/ugd/dded87_29c5b002d99342f788c6ac670e49f274.pdf (accessed on 24 January 2017).
- Sandelowski, M.; Barroso, J. Classifying the Findings in Qualitative Studies. Qual. Health Res. 2003, 13, 905–923. [Google Scholar] [CrossRef] [PubMed]
- Charmaz, K. Constructing Grounded Theory: A Practical Guide through Qualitative Analysis, 2nd ed.; Sage: Los Angeles, CA, USA, 2014. [Google Scholar]
- Holdsworth, L.M. Bereaved Carers’ Accounts of the End of Life and the Role of Care Providers in a ‘Good Death’: A Qualitative Study. Palliat. Med. 2015, 29, 834–841. [Google Scholar] [CrossRef] [PubMed]
- Wilches-Gutiérrez, J.L.; Arenas-Monreal, L.; Paulo-Maya, A.; Peláez-Ballestas, I.; Idrovo, A.J. A ‘Beautiful Death’: Mortality, Death, and Holidays in a Mexican Municipality. Soc. Sci. Med. 2012, 74, 775–782. [Google Scholar] [CrossRef] [PubMed]
- Abib El Halal, G.M.C.; Piva, J.P.; Lago, P.M.; El Halal, M.G.; Cabral, F.C.; Nilson, C.; Garcia, P.C. Parents’ Perspectives on the Deaths of their Children in Two Brazilian Pediatric Intensive Care Units. Int. J. Palliat. Nurs. 2013, 19, 495–502. [Google Scholar] [CrossRef] [PubMed]
- Wilson, D.M.; MacLeod, R.; Houttekier, D. Examining Linkages between Bereavement Grief Intensity and Perceived Death Quality: Qualitative findings. OMEGA J. Death Dying 2016, 74, 260–274. [Google Scholar] [CrossRef]
- Donnelly, S.; Battley, J. Relatives’ Experience of the Moment of Death in a Tertiary Referral Hospital. Mortality 2010, 15, 81–100. [Google Scholar] [CrossRef]
- Workman, S.; Mann, O.E. ‘No Control Whatsoever’: End-of-Life Care on a Medical Teaching Unit from the Perspective of Family Members. QJM Q. J. Med. 2007, 100, 433–440. [Google Scholar] [CrossRef] [PubMed]
- Robert, R.; Zhukovsky, D.S.; Mauricio, R.; Gilmore, K.; Morrison, S.; Palos, G.R. Bereaved Parents’ Perspectives on Pediatric Palliative Care. J. Soc. Work End-of-Life Palliat. Care 2012, 8, 316–338. [Google Scholar] [CrossRef] [PubMed]
- Evans, W.G.; Cutson, T.M.; Steinhauser, K.E.; Tulsky, J.A. Is there No Place like Home? Caregivers Recall Reasons for and Experience upon Transfer from Home Hospice to Inpatient Facilities. J. Palliat. Med. 2006, 9, 100–110. [Google Scholar] [CrossRef] [PubMed]
- Jack, B.A.; O’Brien, M.R.; Scrutton, J.; Baldry, C.R.; Groves, K.E. Supporting Family Carers Providing End-of-Life Home Care: A Qualitative Study on the Impact of a Hospice at Home Service. J. Clin. Nurs. 2015, 24, 131–140. [Google Scholar] [CrossRef] [PubMed]
- Nelson, M.L.; Schrader, S.L.; Eidsness, L.M. “South Dakota’s dying to Know”: Personal Experiences with End-of-Life Care. J. Palliat. Med. 2009, 12, 905–913. [Google Scholar] [CrossRef] [PubMed]
- Kongsuwan, W.; Chaipetch, O.; Matchim, Y. Thai Buddhist Families’ Perspective of a Peaceful Death in ICUs. Nurs. Crit. Care 2012, 17, 151–159. [Google Scholar] [CrossRef] [PubMed]
- Williams, B.R.; Bailey, F.A.; Noh, H.; Woodby, L.L.; Wittich, A.R.; Burgio, K.L. “I was Ready to Take Him Home”: Next-of-Kin’s Accounts of Loved One’s Death During Hospice and Palliative Care Discussions in Veterans Affairs Medical Centers. J. Soc. Work End-of-Life Palliat. Care 2015, 11, 50–73. [Google Scholar] [CrossRef] [PubMed]
- Emanuel, L.L.; Emanuel, E.J. The Promise of a Good Death. J. Lancet 1998, 351, SII21–SII29. [Google Scholar] [CrossRef]
- Payne, S.; Burton, C.; Addington-Hall, J.; Jones, A. End-of-Life Issues in Acute Stroke Care: A Qualitative Study of the Experiences and Preferences of Patients and Families. Palliat. Med. 2010, 24, 146–153. [Google Scholar] [CrossRef] [PubMed]
- Naef, R.; Ward, R.; Mahrer-Imhof, R.; Grande, G. Characteristics of the Bereavement Experience of Older Persons after Spousal Loss: An Integrative Review. Int. J. Nurs. Stud. 2013, 50, 1108–1121. [Google Scholar] [CrossRef] [PubMed]
- Hinds, P.S.; Schum, L.; Baker, J.N.; Wolfe, J. Key factors affecting dying children and their families. J. Palliat. Med. 2005, 8, S-70–S-78. [Google Scholar] [CrossRef] [PubMed]
- Finlay, I.G. Quality of Life to the End. Commun. Med. 2005, 2, 91–95. [Google Scholar] [CrossRef] [PubMed]
- Institute of Medicine; Committee on Approaching Death: Addressing Key End of Life Issues. Dying in America: Improving Quality and Honoring Individual Preferences near the End of Life; National Academies Press: Washington, DC, USA, 2015; Available online: https://www.nap.edu/read/18748/chapter/1 (accessed on 16 April 2017).
- Casarett, D.J.; Quill, T.E. “I’m Not Ready for Hospice”: Strategies for Timely and Effective Hospice Discussions. Ann. Intern. Med. 2007, 146, 443–449. [Google Scholar] [CrossRef] [PubMed]
- Baile, W.F.; Buckman, R.; Lenzi, R.; Glober, G.; Beale, E.A.; Kudelka, A.P. SPIKES—A Six-Step Protocol for Delivering Bad News: Application to the Patient with Cancer. Oncologist 2000, 5, 302–311. [Google Scholar] [CrossRef] [PubMed]
- Villigran, M.; Goldsmith, J.; Wittenberg-Lyles, E.; Baldwin, P. Creating COMFORT: A Communication-Based Model for Breaking Bad News. Commun. Educ. 2010, 59, 220–234. [Google Scholar] [CrossRef]
- Clayton, J.M.; Hancock, K.M.; Butow, P.N.; Tattersall, M.H.N.; Currow, D.C. Clinical Practice Guidelines for Communicating Prognosis and End-of-Life Issues with Adults in the Advanced Stages of A Life-Limiting Illness, and Their Caregivers. Med. J. Aust. 2007, 186, 77–108. [Google Scholar]
- Lieberman, J.A.; Stuart, M.R. The BATHE method: Incorporating counseling and psychotherapy into the everyday management of patients. Prim. Care Companion J. Clin. Psychiatry 1999, 1, 35–38. [Google Scholar] [CrossRef] [PubMed]


© 2017 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Tenzek, K.E.; Depner, R. Still Searching: A Meta-Synthesis of a Good Death from the Bereaved Family Member Perspective. Behav. Sci. 2017, 7, 25. https://doi.org/10.3390/bs7020025
Tenzek KE, Depner R. Still Searching: A Meta-Synthesis of a Good Death from the Bereaved Family Member Perspective. Behavioral Sciences. 2017; 7(2):25. https://doi.org/10.3390/bs7020025
Chicago/Turabian StyleTenzek, Kelly E., and Rachel Depner. 2017. "Still Searching: A Meta-Synthesis of a Good Death from the Bereaved Family Member Perspective" Behavioral Sciences 7, no. 2: 25. https://doi.org/10.3390/bs7020025
APA StyleTenzek, K. E., & Depner, R. (2017). Still Searching: A Meta-Synthesis of a Good Death from the Bereaved Family Member Perspective. Behavioral Sciences, 7(2), 25. https://doi.org/10.3390/bs7020025