
Through the Kinesthetic Lens: Observation of Social Attunement in Autism Spectrum Disorders


Abstract
:1. Introduction:
2. Dance Movement Therapy in ASD
2.1. DMT: General Theoretical Background and Methods
2.2. DMT with Participants with ASD
3. Movement Observation and DMT/ASD
3.1. Movement Observation and DMT
3.2. Movement Observation and ASD
4. Methodology
4.1. Procedures
4.2. Participants
4.3. Data-Collection
4.4. Data-Analysis
4.5. Quality Issues
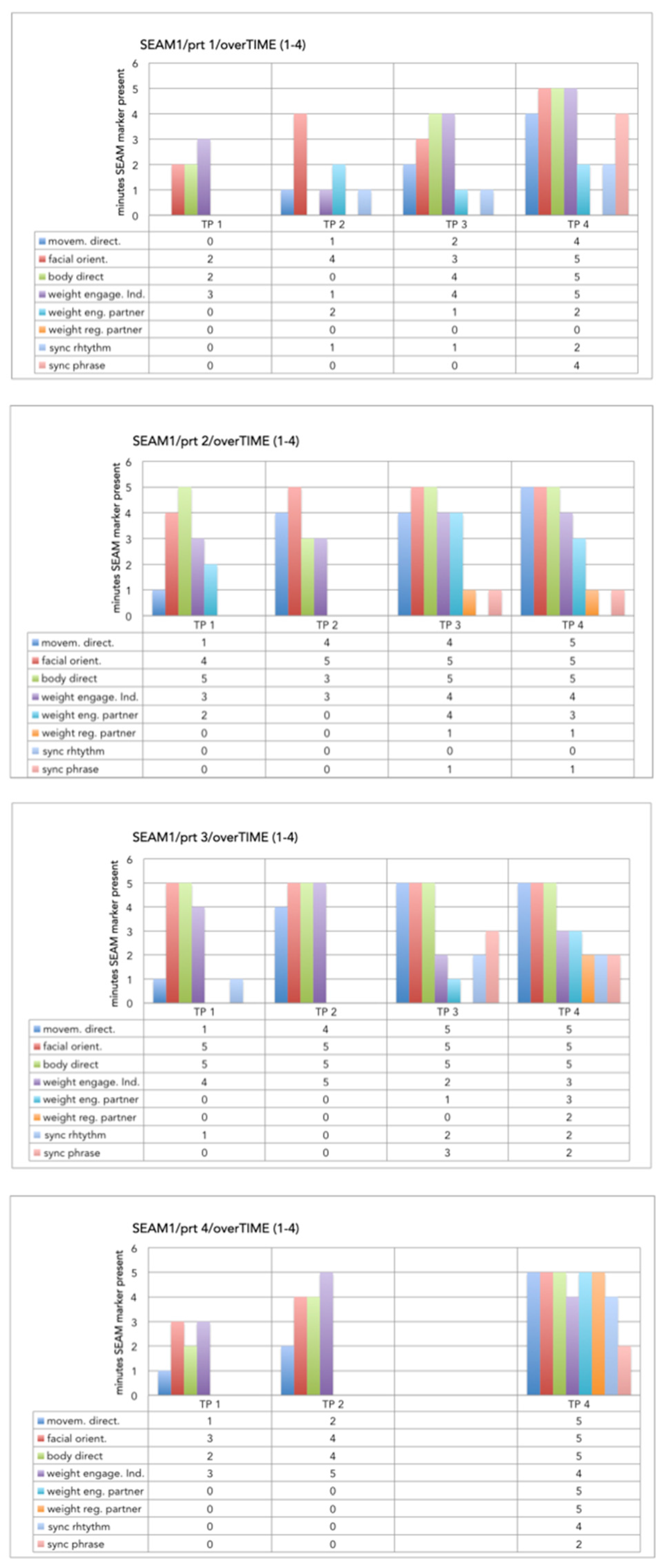
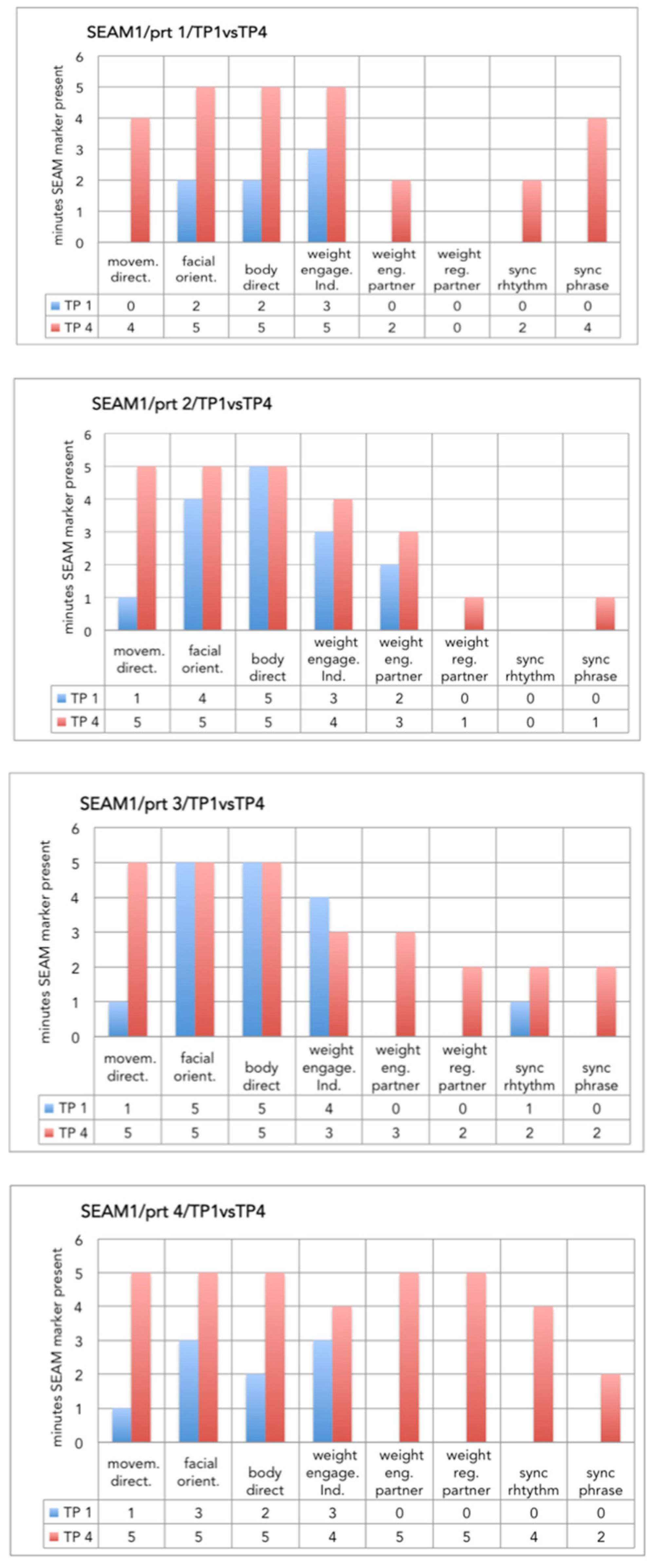
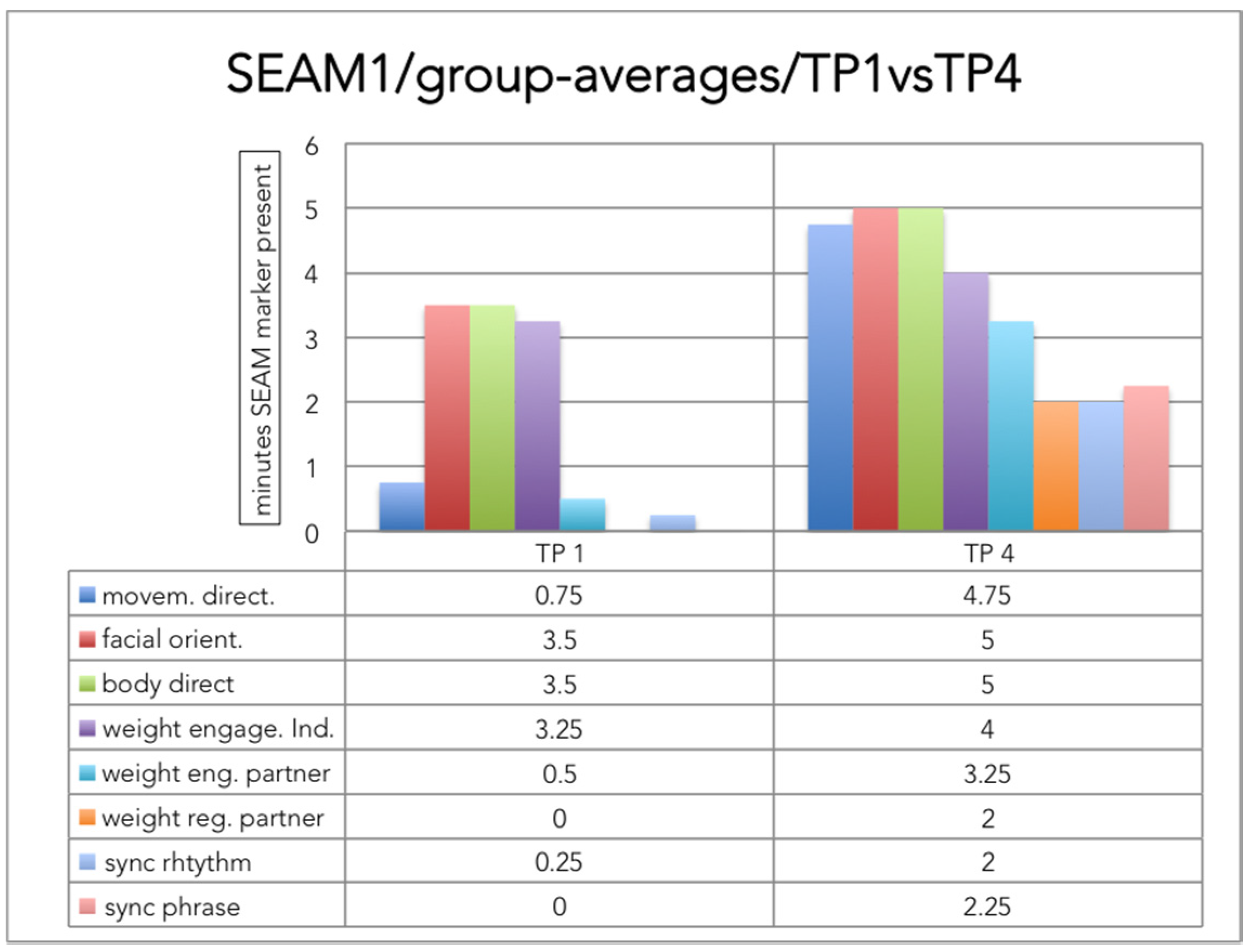
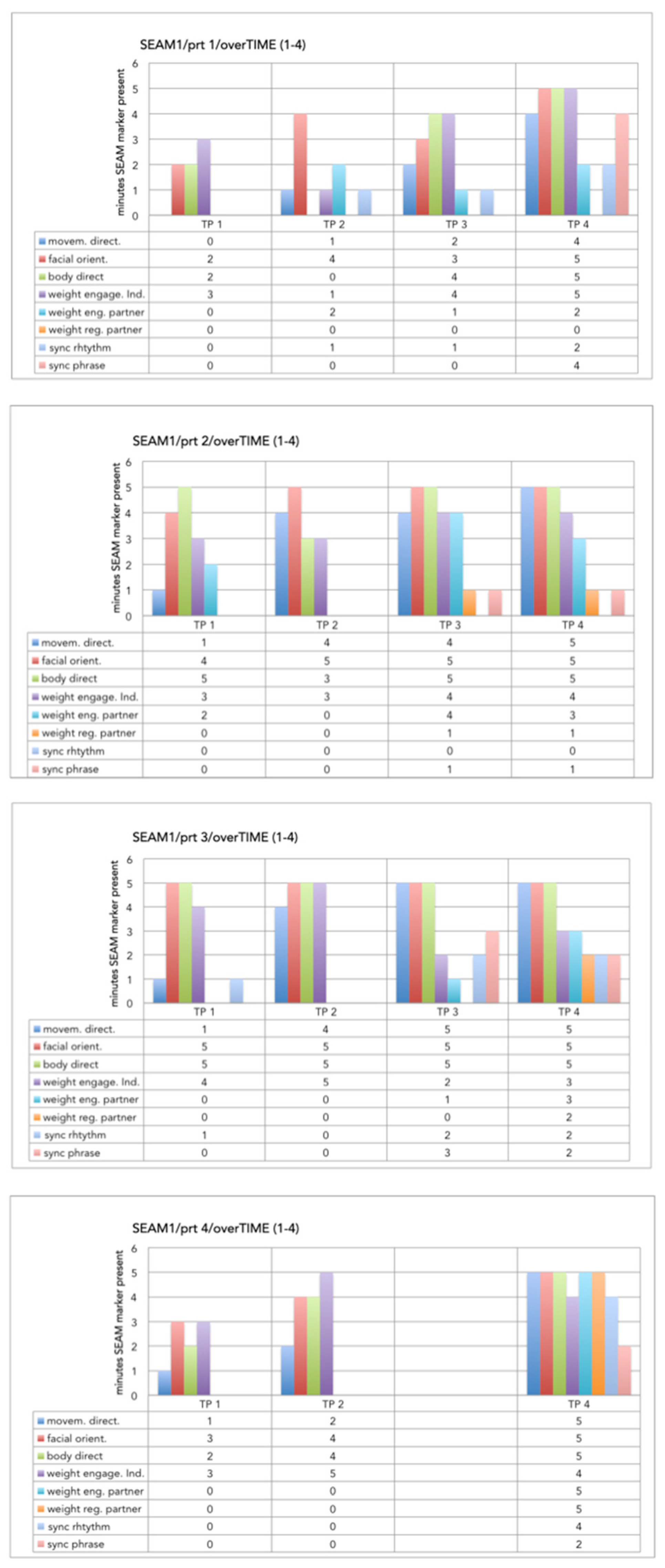
5. Results
5.1. GTA Procedure
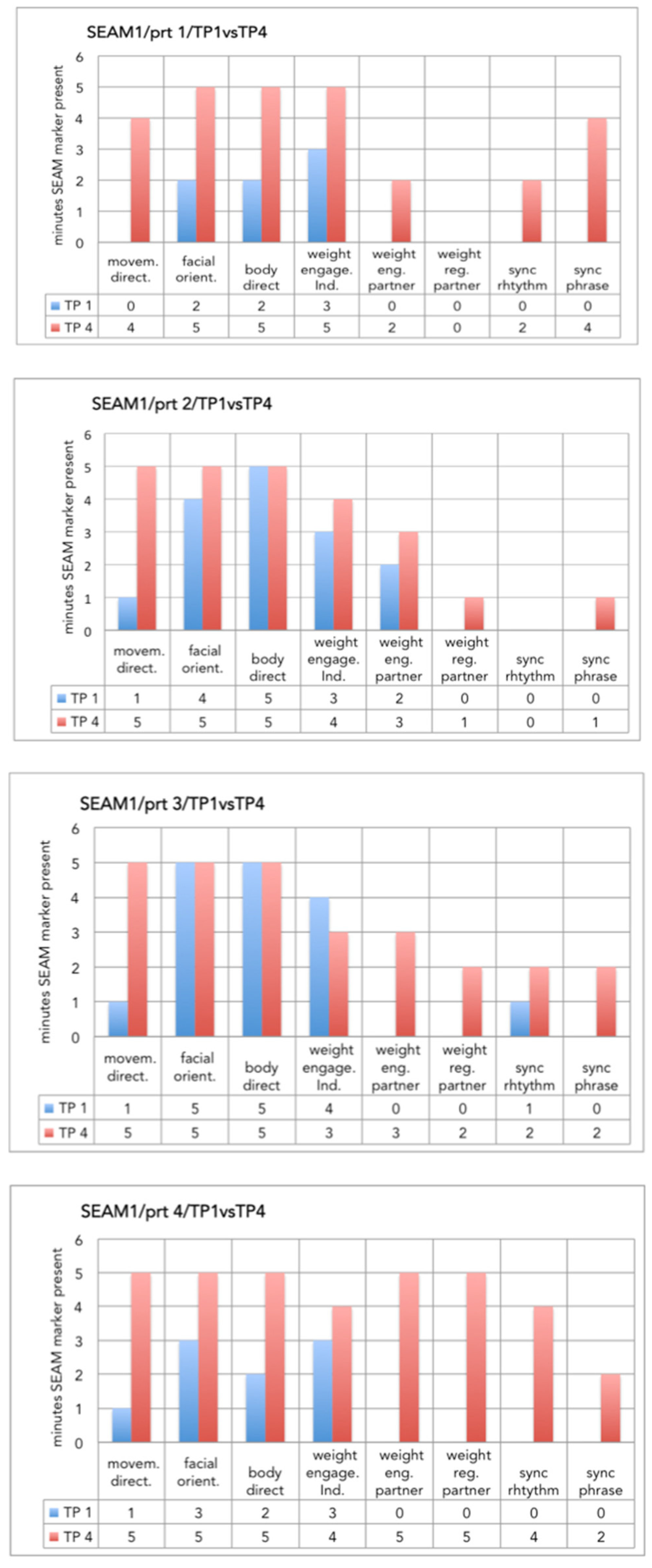
5.2. Selective Observation
6. Discussion
Limitations
7. Conclusions
Author Contributions
Conflicts of Interest
Appendix A
References
- Kanner, L. Autistic Disturbances of Affective Contact. Nerv. Child 1943, 2, 217–250. [Google Scholar]
- Baron-Cohen, S. Autism: Research into causes and intervention. Pediatr. Rehabil. 2004, 7, 73–78. [Google Scholar] [CrossRef] [PubMed]
- APA (American Psychiatric Association). Diagnostic and Statistical Manual of Mental Disorders, 4th text rev. ed.; American Psychiatric Association: Washington, DC, USA, 2000. [Google Scholar]
- APA (American Psychiatric Association). Diagnostic and Statistical Manual of Mental Disorders, 5th ed.; American Psychiatric Association: Washington, DC, USA, 2013. [Google Scholar]
- WHO. The ICD-10 Classification of Mental and Behavioral Disorders; WHO: Geneva, Switzerland, 1992. [Google Scholar]
- Baron-Cohen, S.; Leslie, A.M.; Frith, U. Does the autistic child have a “theory of mind”? Cognition 1985, 21, 37–46. [Google Scholar] [CrossRef]
- Rogers, S.J.; Hepburn, S.L.; Stackhouse, T.; Wehner, E. Imitation performance in toddlers with autism and those with other developmental disorders. J. Child Psychol. Psychiatry 2003, 44, 763–781. [Google Scholar] [CrossRef] [PubMed]
- De Jaegher, H.; Di Paolo, E. Participatory sense-making: An enactive approach to social cognition. Phenomenol. Cogn. Sci. 2007, 6, 485–507. [Google Scholar] [CrossRef]
- De Jaegher, H. Embodiment and sense-making in autism. Front. Integr. Neurosci. 2013, 7, 15. [Google Scholar] [CrossRef] [PubMed]
- Brownell, C.A. Early Developments in Joint Action. Rev. Philos. Psychol. 2011, 2, 193–211. [Google Scholar] [CrossRef] [PubMed]
- Robledo, J.; Donnellan, A.M.; Strandt-Conroy, K. An exploration of sensory and movement differences from the perspective of individuals with autism. Front. Integr. Neurosci. 2012, 16, 6–107. [Google Scholar] [CrossRef] [PubMed]
- Donnellan, A.M.; Hill, D.A.; Leary, M.R. Rethinking autism: Implications of sensory and movement differences for understanding and support. Front. Integr. Neurosci. 2013, 6, 124. [Google Scholar] [CrossRef] [PubMed]
- Trevarthen, C.; Delafield-Butt, J.T. Autism as a developmental disorder in intentional movement and affective engagement. Front. Integr. Neurosci. 2013, 7, 49. [Google Scholar] [CrossRef] [PubMed]
- Trevarthen, C.; Aitken, K.J. Infant intersubjectivity: Research, theory, and clinical applications. J. Child Psychol. Psychiatry 2001, 42, 3–48. [Google Scholar] [CrossRef] [PubMed]
- Reddy, V. On being the object of attention: Implications for self-other consciousness. Trends Cogn. Sci. 2003, 7, 397–402. [Google Scholar] [CrossRef]
- Beebe, B.; Lachmann, F. The relational turn in psychoanalysis: A dyadic systems view from infant research. Contemp. Psychoanal. 2003, 39, 379–409. [Google Scholar] [CrossRef]
- Stern, D.N. The Interpersonal World of the Infant: A View from Psychoanalysis and Developmental Psychology; Basic Books: New York, NY, USA, 1985. [Google Scholar]
- Dosamantes-Beaudry, I. Divergent cultural self construals: Implications for the practice of dance movement therapy. Arts Psychother. 1999, 26, 225–231. [Google Scholar] [CrossRef]
- Gallagher, S. Direct perception in the intersubjective context. Conscious. Cogn. 2008, 17, 535–543. [Google Scholar] [CrossRef] [PubMed]
- Samaritter, R. The use of metaphors in dance movement therapy. Body Mov. Dance Psychother. 2009, 4, 33–43. [Google Scholar] [CrossRef]
- Avindipents & ARTE. Jazzlegende Wayne Shorter; Arte: Kehl, Germany, 25 August 2013. [Google Scholar]
- Payne, H. Shut in, shut out: Dance movement therapy with children and adolescents. In Dance Movement Therapy: Theory and Practice; Payne, H., Ed.; Routledge: London, UK, 1992; pp. 39–81. [Google Scholar]
- Devereaux, C. Moving into relationships. Dance movement therapy with children with autism. In Play-Based Interventions for Children and Adolescents with Autism Spectrum Disorders; Gallo-Lopez, L., Rubin, L., Eds.; Routledge: New York, NY, USA, 2012; pp. 333–351. [Google Scholar]
- Scharoun, S.M.; Reinders, N.J.; Bryden, P.J.; Fletcher, P.C. Dance movement therapy as an Intervention for Children with Autism Spectrum Disorders. Am. J. Dance Ther. 2014, 36, 209–228. [Google Scholar] [CrossRef]
- Martin, M. Moving on the spectrum: Dance movement therapy as a potential early intervention tool for children with Autism Spectrum Disorders. Arts Psychother. 2014, 41, 545–553. [Google Scholar] [CrossRef]
- Samaritter, R.; Payne, H. Kinaesthetic intersubjectivity: A dance informed contribution to self- other relatedness and shared experience in non-verbal psychotherapy with an example from autism. Arts Psychother. 2013, 40, 143–150. [Google Scholar] [CrossRef]
- Laban, R. The Mastery of Movement, 4th ed.; Revised and enlarged by Ullmann, L.; MacDonald and Evans: London, UK, 1980. [Google Scholar]
- Kestenberg-Amighi, J.; Loman, S.; Lewis, P.; Sossin, K.M. The Meaning of Movement: Developmental and Clinical Perspectives of the Kestenberg Movement Profile; Gordon & Breach: Amsterdam, The Netherlands, 1999. [Google Scholar]
- Eberhard-Kaechele, M. Von der Ko-Regulation zur Selbstregulation: Spiegelungsphänomene in der Tanz- und Ausdruckstherapie (From co-regulation to self-regulation. Mirroring in Dance and Expressive Therapy). In Körper–Gefühl—Denken. Körperpsychotherapie und Selbstregulation (Body-Emotion-Thinking. Bodypsychotherapy and Self-Regulation); Thielen, M., Ed.; Psychosozial Verlag: Giessen, Germany, 2009; pp. 251–264. [Google Scholar]
- Erfer, T. Treating children with autism in a public school system. In Dance and Other Expressive Art Therapies; Levy, F., Ed.; Routledge: New York, NY, USA, 1995; pp. 191–213. [Google Scholar]
- Hartshorn, K.; Olds, L.; Filed, T.; Delage, J.; Dullen, C.; Escalona, A. Creative movement therapy benefits children with autism. Early Child Dev. Care 2001, 166, 1–5. [Google Scholar] [CrossRef]
- Koch, S.C.; Mehl, L.; Sobanski, E.; Sieber, M.; Fuchs, T. Fixing the mirrors: A feasibility study of the effects of dance movement therapy on young adults with autism spectrum disorder. Autism 2014, 19, 338–350. [Google Scholar] [CrossRef] [PubMed]
- Rouhiainen, L. Living Transformative Lives; Acta Scenica 13; Theatre Academy: Helsinki, Finland, 2003. [Google Scholar]
- Tufnell, M.; Crickmay, C. Body Space Image; Dance Books: London, UK, 1990. [Google Scholar]
- Bartenieff, I.; Lewis, D. Body Movement. Coping with the Environment; Routledge: London, UK, 2002. [Google Scholar]
- Teitelbaum, P.; Teitelbaum, O.; Nye, J.; Fryman, J.; Maurer, R.G. Movement analysis in infancy may be useful for early diagnosis of autism. Proc. Natl. Acad. Sci. USA 1998, 95, 23. [Google Scholar] [CrossRef]
- Rinehart, N.J.; Bellgrove, M.A.; Tonge, B.J.; Brereton, A.V.; Howells-Rankin, D.; Bradshaw, J. An Examination of Movement Kinematics in Young People with High-functioning Autism and Asperger’s Disorder: Further Evidence for a Motor Planning Deficit. J. Autism Dev. Disord. 2006, 36, 757–767. [Google Scholar] [CrossRef] [PubMed]
- Fournier, K.A.; Hass, C.J.; Naik, S.K.; Lodha, N.; Cauraugh, J.H. Motor coordination in autism spectrum disorders: A synthesis and meta-analysis. J. Autism Dev. Disord. 2010, 40, 1227–1240. [Google Scholar] [CrossRef] [PubMed]
- Bhat, A.N.; Landa, R.J.; Galloway, J.C. Current perspectives on motor functioning in infants, children, and adults with autism spectrum disorders. Phys. Ther. 2011, 91, 1116–1129. [Google Scholar] [CrossRef] [PubMed]
- Ayres, A.J. Sensory Integration and Praxis Tests; Western Psychological Services: Los Angeles, CA, USA, 1989. [Google Scholar]
- Hammink, M.N. Psychomotorische Diagnostiek Binnen het Kinder- en Jeugdpsychiatrisch Zorgveld (Psychomotor Diagnostics in the Child- and Youth Psychiatry Care); Shaker Publishing: Maastricht, The Netherlands, 2003. [Google Scholar]
- Emck, C.; Hammink, M.N.; Bosscher, R.J. Psychomotorische Diagnostiek en Indicatiestelling voor Kinderen van 6 tot 12 Jaar (Psychomotor Diagnostics and Indications for Chidlren Age 6 to 12); Web: Utrecht, The Netherlands, 2007. [Google Scholar]
- Adler, J. The Study of an Autistic Child. In Proceedings of the 3rd Annual Conference of the American Dance Therapy Association, Madison, WI, USA, 25–27 October 1968; American Dance Therapy Association: Baltimore, MD, USA, 1968. [Google Scholar]
- Loman, S. The case of Warren: A KMP approach to autism. In Dance and Other Expressive Art Therapies; Levy, F., Ed.; Routledge: New York, NY, USA, 1995; pp. 213–225. [Google Scholar]
- Partelli, L. Aesthetic Listening: Contributions of dance movement therapy to the psychic understanding of motor Stereotypes and Distortions in Autism and psychosis in childhood and adolescence. Arts Psychother. 1995, 22, 241–247. [Google Scholar]
- Tortora, S. Ways of seeing: An early childhood integrated therapeutic approach for parents and babies. Clin. Soc. Work J. 2010, 38, 37–50. [Google Scholar] [CrossRef]
- Sossin, M.; Loman, S. Clinical applications of the KMP. In The Body Mind Connection in Human Movement Analysis; Loman, S., Ed.; Antioch New England Graduate School: Keene, NH, USA, 1992. [Google Scholar]
- Loman, S.; Merman, H. The KMP: A tool for dance movement therapy. Am. J. Dance Ther. 1996, 18, 29–52. [Google Scholar] [CrossRef]
- Kalish, B.I. Body Movement Scale for Autistic and Other Atypical Children: An Exploratory Study Using a Normal Group and an Atypical Group; Bryn Mawr College: Bryn Mawr, PA, USA, 1976. [Google Scholar]
- Wenar, C.; Ruttenberg, B.A.; Kalish-Weiss, B.; Wolf, E.G. The development of normal and autistic children: A comparative study. J. Autism Dev. Disord. 1986, 16, 317–333. [Google Scholar] [CrossRef] [PubMed]
- Dulicai, D. Movement assessment of families: A system model. In Movement Analysis of Interaction/Bewegungsanalyse von Interaktionen; Bender, S., Ed.; Logos: Berlin, Germany, 2010; pp. 49–61. [Google Scholar]
- Knoblauch, H.; Schnettler, B.; Raab, J. Video-Analysis. Methodological Aspects of Interpretive Audiovisual Analysis in Social Research. In Video Analysis. Methodology and Methods. Qualitative Audiovisual Data Analysis in Sociology; Knoblauch, H., Schnettler, B., Raab, J., Soeffner, H.-G., Eds.; Peter Lang: Frankfurt am Main, Germany, 2009; pp. 9–29. [Google Scholar]
- De Vaus, D. Retrospective study. In The SAGE Dictionary of Social Research Methods; Jupp, V., Ed.; Sage: London, UK, 2006; pp. 269–270. [Google Scholar]
- Glaser, B.; Strauss, A. The Discovery of Grounded Theory. Strategies for Qualitative Research; Aldine Publishing Company: Chicago, IL, USA, 1967. [Google Scholar]
- Ellis, C.; Adams, T.E.; Bochner, A.P. Autoethnography: An overview. Forum Qual. Soc. Res. 2011, 12, 1. [Google Scholar]
- Wittenburg, P.; Brugman, H.; Russel, A.; Klassmann, A.; Sloetjes, H. ELAN: A Professional Framework for Multimodality Research. In Proceedings of the LREC 2006 5th International Conference on Language Resources and Evaluation, Genova, Italy, 22–28 May 2006.
- Lausberg, H.; Sloetjes, H. NGCS/ELAN—Coding movement behavior in psychotherapy. Psychother. Psychosom. Med. Psychol. 2009, 59, 0259. [Google Scholar] [CrossRef]
- Schoonewille, E. Imitation as an Intervention Integrated in a Dance-Movement Therapy (DMT) Training for Children with an Autism Spectrum Disorder (ASD). Master’s Thesis, Developmental Psychology, University of Maastricht, Maastricht, The Netherlands, 2011. [Google Scholar]
- Bakeman, R.; Quera, V. Sequential Analysis and Observational Methods for the Behavioral Sciences; Cambridge University Press: Cambridge, UK, 2011. [Google Scholar]
- Altman, D.G. Practical Statistics for Medical Research; Chapman & Hall: London, UK, 1991. [Google Scholar]
- Cohen, D.J.; Crabtree, B.J. Qualitative Research Guidelines Project. 2006. Available online: http://www.qualres.org (accessed on 6 July 2015).
- Ingersoll, B.; Lewis, E.; Kroman, E. Teaching the imitation and spontaneous use of descriptive gestures in young children with autism using a naturalistic behavioral intervention. J. Autism Dev. Disord. 2007, 37, 1446–1456. [Google Scholar] [CrossRef] [PubMed]
- Field, T.; Sanders, C.; Nadel, J. Children with autism display more social behaviors after repeated imitation sessions. Autism 2001, 5, 317–323. [Google Scholar] [CrossRef] [PubMed]
- Escalona, A.; Field, T.; Nadel, J.; Lundy, B. Brief report: Imitation effects on children with autism. J. Autism Dev. Disord. 2002, 32, 141–144. [Google Scholar] [CrossRef] [PubMed]
- Robins, B.; Dautenhahn, K.; Dickerson, P. From isolation to communication: A case study evaluation of robot assisted play for children with autism with a minimally expressive humanoid robot. In Proceedings of the Second International Conferences on Advances in Computer-Human Interactions, Cancun, Mexico, 1–7 February 2009.
- Guionnet, S.; Nadel, J.; Bertasi, E.; Sperduti, M.; Delaveau, P.; Fossati, P. Reciprocal Imitation: Toward a Neural Basis of Social Interaction. Cereb. Cortex 2012, 22, 971–978. [Google Scholar] [CrossRef] [PubMed]
- Nadel, J.; Aouka, N.; Coulon, N.; Gras-Vincendon, A.; Canet, P.; Fagard, J.; Bursztejn, C. Yes they can! An approach to observational learning in low-functioning children with autism. Autism 2011, 15, 421–435. [Google Scholar] [CrossRef] [PubMed]
- Sapsford, R. Validity of measurement. In The SAGE Dictionary of Social Research Methods; Jupp, V., Ed.; Sage: London, UK, 2006; pp. 314–315. [Google Scholar]
- Cruz, R.F.; Feder, B. Feders’ the Art and Science of Evaluation in the Arts Therapies, 2nd ed.; Charles C. Thomas: Springfield, IL, USA, 2013. [Google Scholar]
- Amos, P. Rhythm and timing in autism: Learning to dance. Front. Integr. Neurosci. 2013, 7, 27. [Google Scholar] [CrossRef] [PubMed]
- Trevarthen, C. The concept and foundations of infant intersubjectivity. In Intersubjective Communication and Emotion in Early Ontogeny; Bråten, S., Ed.; Cambridge University Press: Cambridge, UK, 1998; pp. 15–47. [Google Scholar]
- Gross, M.M.; Crane, E.A.; Fredrickson, B.L. Methodology for assessing bodily expression of emotion. J. Nonverbal Behavior. 2010, 34, 223–248. [Google Scholar] [CrossRef]
- Hilliard, R.B. Single-case methodology in psychotherapy process and outcome research. J. Consult. Clin. Psychol. 1993, 61, 373–380. [Google Scholar] [CrossRef] [PubMed]
- Shotter, J. Situated dialogic action research: Disclosing “Beginnings” for innovative change in organizations. Organ. Res. Methods 2010, 13, 268–285. [Google Scholar] [CrossRef]
- Aspers, P. Empirical Phenomenology: A Qualitative Research Approach (The Cologne Seminars). Indo-Pac. J. Phenomenol. 2009, 9, 1–12. [Google Scholar] [CrossRef]

{kind=link}
{kind=link}
{kind=link}
| Overarching structures | Social Engagement and Attunement Movement (SEAM) behavior as observed: |
|---|---|
| Observed interpersonal movement behavior in terms of space |
|
| Observed interpersonal movement behavior in terms of weight |
|
| Observed interpersonal movement behavior in terms of time |
|
© 2017 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license ( http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Samaritter, R.; Payne, H. Through the Kinesthetic Lens: Observation of Social Attunement in Autism Spectrum Disorders. Behav. Sci. 2017, 7, 14. https://doi.org/10.3390/bs7010014
Samaritter R, Payne H. Through the Kinesthetic Lens: Observation of Social Attunement in Autism Spectrum Disorders. Behavioral Sciences. 2017; 7(1):14. https://doi.org/10.3390/bs7010014
Chicago/Turabian StyleSamaritter, Rosemarie, and Helen Payne. 2017. "Through the Kinesthetic Lens: Observation of Social Attunement in Autism Spectrum Disorders" Behavioral Sciences 7, no. 1: 14. https://doi.org/10.3390/bs7010014
APA StyleSamaritter, R., & Payne, H. (2017). Through the Kinesthetic Lens: Observation of Social Attunement in Autism Spectrum Disorders. Behavioral Sciences, 7(1), 14. https://doi.org/10.3390/bs7010014