
Depression May Not Be Related to Impaired Interoceptive Sensibility: The Role of Alexithymia

 ,
, 

Abstract
1. Background
2. Method
2.1. Participants
2.2. Measurements
2.2.1. Interoception
2.2.2. Alexithymia
2.2.3. Depressive Symptoms
2.3. Procedure
2.4. Statistical Analysis
3. Results
3.1. Associations Between Interoception and Depressive Symptoms in the DEP Group
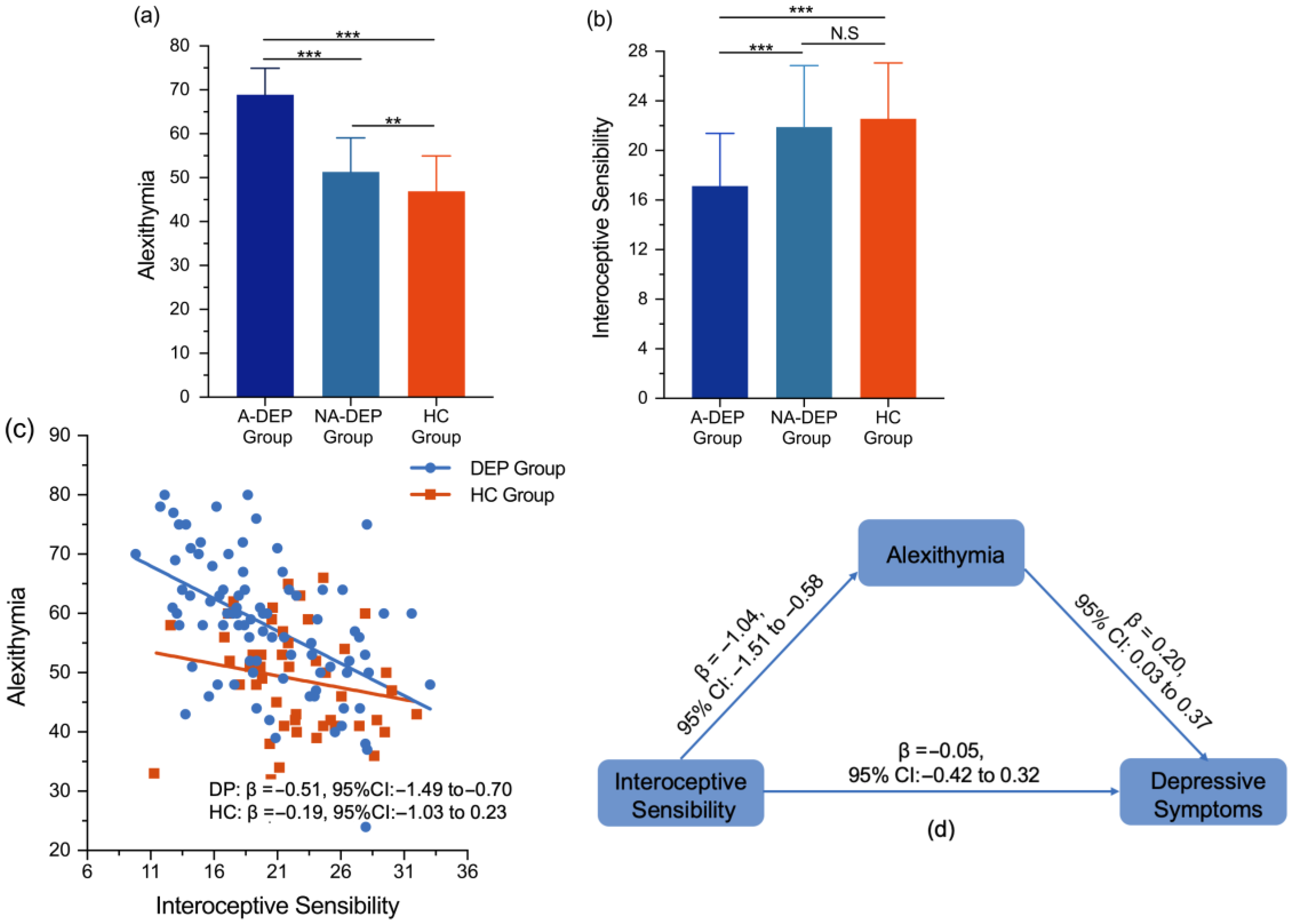
3.2. Comparison of Interoception Among A-DEP, NA-DEP, and HC Groups
3.3. Associations Between Interoception and Alexithymia in the DEP and HC Groups
3.4. Mediation Effects of Alexithymia Between Interoception and Depressive Symptoms in the DEP Group
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Avery, J. A., Drevets, W. C., Moseman, S. E., Bodurka, J., Barcalow, J. C., & Simmons, W. K. (2014). Major depressive disorder is associated with abnormal interoceptive activity and functional connectivity in the Insula. Biological Psychiatry, 76(3), 258–266. [Google Scholar] [CrossRef] [PubMed]
- Bagby, R. M., Parker, J. D. A., & Taylor, G. J. (2020). Twenty-five years with the 20-item Toronto Alexithymia Scale. Journal of Psychosomatic Research, 131, 109940. [Google Scholar] [CrossRef] [PubMed]
- Bagby, R. M., Taylor, G., Parker, J., & Dickens, S. (2006). The development of the Toronto structured interview for alexithymia: Item selection, factor structure, reliability and concurrent validity. Psychotherapy and Psychosomatics, 75, 25–39. [Google Scholar] [CrossRef] [PubMed]
- Barrett, L. F., Quigley, K. S., & Hamilton, P. (2016). An active inference theory of allostasis and interoception in depression. Philosophical Transactions of the Royal Society B-Biological Sciences, 371(1708), 20160011. [Google Scholar] [CrossRef]
- Bär, K. J., Terhaar, J., Viola, F. C., & Debener, S. (2012). Heartbeat evoked potentials mirror altered body perception in depressed patients. International Journal of Psychophysiology, 85(3), 351–352. [Google Scholar] [CrossRef]
- Benjamini, Y., & Hochberg, Y. (1995). Controlling the false discovery rate—A practical and powerful approach to multiple testing. Journal of the Royal Statistical Society Series B-Statistical Methodology, 57(1), 289–300. [Google Scholar] [CrossRef]
- Benjamini, Y., & Yekutieli, D. (2001). The control of the false discovery rate in multiple testing under dependency. Annals of Statistics, 29(4), 1165–1188. [Google Scholar] [CrossRef]
- Betka, S., Pfeifer, G., Garfinkel, S., Prins, H., Bond, R., Sequeira, H., Duka, T., & Critchley, H. (2018). How do self-assessment of alexithymia and sensitivity to bodily sensations relate to alcohol consumption? Alcoholism-Clinical and Experimental Research, 42(1), 81–88. [Google Scholar] [CrossRef]
- Bornemann, B., & Singer, T. (2017). Taking time to feel our body: Steady increases in heartbeat perception accuracy and decreases in alexithymia over 9 months of contemplative mental training. Psychophysiology, 54(3), 469–482. [Google Scholar] [CrossRef]
- Brewer, R., Cook, R., & Bird, G. (2016). Alexithymia: A general deficit of interoception. Royal Society Open Science, 3(10), 150664. [Google Scholar] [CrossRef]
- Butera, C. D., Harrison, L., Kilroy, E., Jayashankar, A., Shipkova, M., Pruyser, A., & Aziz-Zadeh, L. (2023). Relationships between alexithymia, interoception, and emotional empathy in autism spectrum disorder. Autism, 27(3), 690–703. [Google Scholar] [CrossRef]
- Celikel, F. C., Kose, S., Erkorkmaz, U., Sayar, K., Cumurcu, B. E., & Cloninger, C. R. (2010). Alexithymia and temperament and character model of personality in patients with major depressive disorder. Comprehensive Psychiatry, 51(1), 64–70. [Google Scholar] [CrossRef] [PubMed]
- Chai, Y., Sheline, Y. I., Oathes, D. J., Balderston, N. L., Rao, H., & Yu, M. (2023). Functional connectomics in depression: Insights into therapies. Trends in Cognitive Sciences, 27(9), 814–832. [Google Scholar] [CrossRef] [PubMed]
- Chen, L. Z., Dai, A. Y., Yao, Y., Si, R., Hu, Z., Ge, L., Du, X., Li, A., & Wei, G. X. (2021). Effects of 8-week tai chi chuan practice on mindfulness level. Mindfulness, 12(6), 1534–1541. [Google Scholar] [CrossRef]
- Critchley, H. D. (2005). Neural mechanisms of autonomic, affective, and cognitive integration. Journal of Comparative Neurology, 493(1), 154–166. [Google Scholar] [CrossRef]
- Datko, M., Lutz, J., Gawande, R., Comeau, A., To, M. N., Desel, T., Gan, J., Desbordes, G., Napadow, V., & Schuman-Olivier, Z. (2022). Increased insula response to interoceptive attention following mindfulness training is associated with increased body trusting among patients with depression. Psychiatry Research-Neuroimaging, 327, 111559. [Google Scholar] [CrossRef]
- Davey, C. G. (2025). The body intervenes: How active inference explains depression’s clinical presentation. Neuroscience & Biobehavioral Reviews, 175, 106229. [Google Scholar] [CrossRef]
- Desdentado, L., Miragall, M., Llorens, R., & Baños, R. (2022). Disentangling the role of interoceptive sensibility in alexithymia, emotion dysregulation, and depression in healthy individuals. Current Psychology, 42, 20570–20582. [Google Scholar] [CrossRef]
- Desmedt, O., Van den Houte, M., Walentynowicz, M., Dekeyser, S., Luminet, O., & Corneille, O. (2022). How does heartbeat counting task performance relate to theoretically-relevant mental health outcomes? A meta-analysis. Collabra-Psychology, 8(1), 33271. [Google Scholar] [CrossRef]
- Dunn, B. D., Dalgleish, T., Ogilvie, A. D., & Lawrence, A. D. (2007). Heartbeat perception in depression. Behaviour Research and Therapy, 45(8), 1921–1930. [Google Scholar] [CrossRef]
- Eggart, M., Lange, A., Binser, M. J., Queri, S., & Müller-Oerlinghausen, B. (2019). Major depressive disorder is associated with impaired interoceptive accuracy: A systematic review. Brain Sciences, 9(6), 131. [Google Scholar] [CrossRef] [PubMed]
- Faul, F., Erdfelder, E., Lang, A. G., & Buchner, A. (2007). G*Power 3: A flexible statistical power analysis program for the social, behavioral, and biomedical sciences. Behavior Research Methods, 39(2), 175–191. [Google Scholar] [CrossRef] [PubMed]
- Fissler, M., Winnebeck, E., Schroeter, T., Gummersbach, M., Huntenburg, J. M., Gaertner, M., & Barnhofer, T. (2016). An investigation of the effects of brief mindfulness training on self-reported interoceptive awareness, the ability to decenter, and their role in the reduction of depressive symptoms. Mindfulness, 7(5), 1170–1181. [Google Scholar] [CrossRef]
- Franz, M., Popp, K., Schaefer, R., Sitte, W., Schneider, C., Hardt, J., Decker, O., & Braehler, E. (2008). Alexithymia in the German general population. Social Psychiatry and Psychiatric Epidemiology, 43(1), 54–62. [Google Scholar] [CrossRef]
- Furman, D. J., Waugh, C. E., Bhattacharjee, K., Thompson, R. J., & Gotlib, I. H. (2013). Interoceptive awareness, positive affect, and decision making in Major Depressive Disorder. Journal of Affective Disorders, 151(2), 780–785. [Google Scholar] [CrossRef]
- Garfinkel, S. N., & Critchley, H. D. (2013). Interoception, emotion and brain: New insights link internal physiology to social behaviour. Commentary on: “Anterior insular cortex mediates bodily sensibility and social anxiety” by Terasawa et al. (2012). Social Cognitive and Affective Neuroscience, 8(3), 231–234. [Google Scholar] [CrossRef]
- Garfinkel, S. N., Seth, A. K., Barrett, A. B., Suzuki, K., & Critchley, H. D. (2015). Knowing your own heart: Distinguishing interoceptive accuracy from interoceptive awareness. Biological Psychology, 104, 65–74. [Google Scholar] [CrossRef]
- Guenther, V., Rufer, M., Kersting, A., & Suslow, T. (2016). Predicting symptoms in major depression after inpatient treatment: The role of alexithymia. Nordic Journal of Psychiatry, 70(5), 392–398. [Google Scholar] [CrossRef]
- Hamilton, M. (1960). A rating scale for depression. Journal of Neurology, Neurosurgery & Psychiatry, 23(1), 56–62. [Google Scholar] [CrossRef]
- Herbert, B. M., Herbert, C., & Pollatos, O. (2011). On the relationship between interoceptive awareness and alexithymia: Is interoceptive awareness related to emotional awareness? Journal of Personality, 79(5), 1149–1175. [Google Scholar] [CrossRef]
- Herbert, B. M., Pollatos, O., & Schandry, R. (2007). Interoceptive sensitivity and emotion processing: An EEG study. International Journal of Psychophysiology, 65(3), 214–227. [Google Scholar] [CrossRef] [PubMed]
- Jinyao, Y., Shuqiao, Y., & Xiongzhao, Z. (2003). The Chinese version of the TAS-20: Reliability and validity. Chinese Mental Health Journal, 17(11), 763–767. [Google Scholar]
- Khalsa, S. S., Adolphs, R., Cameron, O. G., Critchley, H. D., Davenport, P. W., Feinstein, J. S., Feusner, J. D., Garfinkel, S. N., Lane, R. D., Mehling, W. E., & Meuret, A. E. (2018). Interoception and mental health: A roadmap. Biological Psychiatry-Cognitive Neuroscience and Neuroimaging, 3(6), 501–513. [Google Scholar] [CrossRef]
- Kim, J. H., Lee, S. J., Rim, H. D., Kim, H. W., Bae, G. Y., & Chang, S. M. (2008). The Relationship between alexithymia and general symptoms of patients with depressive disorders. Psychiatry Investigation, 5(3), 179–185. [Google Scholar] [CrossRef]
- Leweke, F., Leichsenring, F., Kruse, J., & Hermes, S. (2012). Is alexithymia associated with specific mental disorders? Psychopathology, 45(1), 22–28. [Google Scholar] [CrossRef]
- Li, S. W., Zhang, B., Guo, Y. F., & Zhang, J. P. (2015). 6 The association between alexithymia as assessed by the 20-item Toronto Alexithymia Scale and depression: A meta-analysis. Psychiatry Research, 227(1), 1–9. [Google Scholar] [CrossRef]
- Lin, F.-L., Hsu, C.-C., Mehling, W., & Yeh, M.-L. (2017). Translation and psychometric testing of the chinese version of the multidimensional assessment of interoceptive awareness. Journal of Nursing Research, 25(1), 76–84. Available online: https://journals.lww.com/jnr-twna/fulltext/2017/02000/translation_and_psychometric_testing_of_the.13.aspx (accessed on 10 February 2017). [CrossRef]
- Luminet, O., & Nielson, K. A. (2025). Alexithymia: Toward an experimental, processual affective science with effective interventions. Annual Review of Psychology, 76(1), 741–769. [Google Scholar] [CrossRef]
- Mehling, W. E., Chesney, M. A., Metzler, T. J., Goldstein, L. A., Maguen, S., Geronimo, C., Agcaoili, G., Barnes, D. E., Hlavin, J. A., & Neylan, T. C. (2018). A 12-week integrative exercise program improves self-reported mindfulness and interoceptive awareness in war veterans with posttraumatic stress symptoms. Journal of Clinical Psychology, 74(4), 554–565. [Google Scholar] [CrossRef] [PubMed]
- Mehling, W. E., Price, C., Daubenmier, J. J., Acree, M., Bartmess, E., & Stewart, A. (2012). The Multidimensional Assessment of Interoceptive Awareness (MAIA). PLoS ONE, 7(11), e48230. [Google Scholar] [CrossRef] [PubMed]
- Mul, C. L., Stagg, S. D., Herbelin, B., & Aspell, J. E. (2018). The feeling of me feeling for you: Interoception, alexithymia and empathy in Autism. Journal of Autism and Developmental Disorders, 48(9), 2953–2967. [Google Scholar] [CrossRef]
- Murphy, J., Brewer, R., Hobson, H., Catmur, C., & Bird, G. (2018). Is alexithymia characterised by impaired interoception? Further evidence, the importance of control variables, and the problems with the Heartbeat Counting Task. Biological Psychology, 136, 189–197. [Google Scholar] [CrossRef] [PubMed]
- Norman, H., Marzano, L., Coulson, M., & Oskis, A. (2019). Effects of mindfulness-based interventions on alexithymia: A systematic review. Evidence-Based Mental Health, 22(1), 36–43. [Google Scholar] [CrossRef] [PubMed]
- Porcelli, P., Tulipani, C., Di Micco, C., Spedicato, M. R., & Maiello, E. (2011). Temporal stability of alexithymia in cancer patients following a psychological intervention. Journal of Clinical Psychology, 67(12), 1177–1187. [Google Scholar] [CrossRef]
- Scarpazza, C., Zangrossi, A., Huang, Y.-C., Sartori, G., & Massaro, S. (2022). Disentangling interoceptive abilities in alexithymia. Psychological Research-Psychologische Forschung, 86(3), 844–857. [Google Scholar] [CrossRef]
- Schachter, S., & Singer, J. (1962). Cognitive, social, and physiological determinants of emotional state. Psychological Review, 69(5), 379. [Google Scholar] [CrossRef]
- Schandry, R. (1981). Heart beat perception and emotional experience. Psychophysiology, 18(4), 483–488. [Google Scholar] [CrossRef]
- Serafini, G., De Berardis, D., Valchera, A., Canepa, G., Geoffroy, P. A., Pompili, M., & Amore, M. (2020). Alexithymia as a possible specifier of adverse outcomes: Clinical correlates in euthymic unipolar individuals. Journal of Affective Disorders, 263, 428–436. [Google Scholar] [CrossRef]
- Shen, H. R., Du, X. H., Fan, Y. Y., Dai, J. A., & Wei, G. X. (2023). Interoceptive sensibility mediates anxiety changes induced by mindfulness-based Tai Chi Chuan Movement Intervention. Mindfulness, 14(7), 1662–1673. [Google Scholar] [CrossRef]
- Sifneos, P. E. (1973). Prevalence of alexithymic characteristics in psychosomatic patients. Psychotherapy and Psychosomatics, 22(2–6), 255–262. [Google Scholar] [CrossRef]
- Taycan, O., Ozdemir, A., & Erdogan Taycan, S. (2017). Alexithymia and somatization in depressed patients: The role of the type of somatic symptom attribution. Noropsikiyatri Arsivi-Archives of Neuropsychiatry, 54(2), 99–104. [Google Scholar] [CrossRef]
- Taylor, G. J., Bagby, R. M., & Parker, J. D. A. (1997). Disorders of affect regulation: Alexithymia in medical and psychiatric illness. Cambridge University Press. [Google Scholar] [CrossRef]
- Trevisan, D. A., Altschuler, M. R., Bagdasarov, A., Carlos, C., Duan, S., Hamo, E., Kala, S., McNair, M. L., Parker, T., Stahl, D., & Winkelman, T. (2019). A meta-analysis on the relationship between interoceptive awareness and alexithymia: Distinguishing interoceptive accuracy and sensibility. Journal of Abnormal Psychology, 128(8), 765–776. [Google Scholar] [CrossRef] [PubMed]
- Valins, S. (1966). Cognitive effects of false heart-rate feedback. Journal of Personality and Social Psychology, 4(4), 400–408. [Google Scholar] [CrossRef] [PubMed]
- Van Bael, K., Scarfo, J., Suleyman, E., Katherveloo, J., Grimble, N., & Ball, M. (2024). A systematic review and meta-analysis of the relationship between subjective interoception and alexithymia: Implications for construct definitions and measurement. PLoS ONE, 19(11), e0310411. [Google Scholar] [CrossRef] [PubMed]
- Vivas-Rivas, L., Serpa-Barrientos, A., Oblitas-Guerrero, S., Carranza Cubas, S., & Saintila, J. (2024). Does interoceptive awareness influence depression through anxiety in peruvian adults? A mediation analysis. Psychiatry International, 5, 927–938. [Google Scholar] [CrossRef]
- Westwood, H., Mandy, W., & Brewer, R. (2025). The relationship between interoception, alexithymia, autistic traits and eating pathology in autistic adults. Journal of Autism and Developmental Disorders. online ahead of print. [Google Scholar] [CrossRef]
- Zamariola, G., Frost, N., Van Oost, A., Corneille, O., & Luminet, O. (2019). Relationship between interoception and emotion regulation: New evidence from mixed methods. Journal of Affective Disorders, 246, 480–485. [Google Scholar] [CrossRef]
- Zheng, Y. P., Zhao, J. P., Phillips, M., Liu, J. B., Cai, M. F., Sun, S. Q., & Huang, M. F. (1988). Validity and reliability of the Chinese hamilton depression rating scale. The British Journal of Psychiatry, 152, 660–664. [Google Scholar] [CrossRef]
- Zhou, H., Liu, J., Wu, Y., Huang, Z., Wang, W., Ma, Y., Zhu, H., Zhou, Z., Wang, J., & Jiang, C. (2024). Unveiling the interoception impairment in various major depressive disorder stages. CNS Neuroscience & Therapeutics, 30(8), e14923. [Google Scholar] [CrossRef]

{kind=link}
| Interoceptive Sensibility | Interoceptive Accuracy | Interoceptive Awareness | Alexithymia | Depressive Symptoms | |
|---|---|---|---|---|---|
| Interoceptive Sensibility | |||||
| Interoceptive Accuracy | 0.04 | ||||
| Interoceptive Awareness | 0.13 | 0.52 ** | |||
| Alexithymia | −0.51 ** | −0.10 | −0.31 ** | ||
| Depressive Symptoms | −0.18 | −0.19 | −0.18 | 0.33 ** |
| A-DEP Group (n = 34) | NA-DEP Group (n = 54) | HC Group (n = 50) | F/χ2 | p | Effect Size | |
|---|---|---|---|---|---|---|
| Age (Years, Mean ± SD) | 25.68 ± 6.36 | 27.15 ± 8.84 | 26.40 ± 4.71 | 1.68 | 0.372 | 0.04 |
| Sex (M/F) | 7/27 | 14/40 | 12/38 | 0.33 | 0.849 | 0.04 |
| Illness duration (Years) | 3.23 ± 2.64 | 3.07 ± 2.90 | 0.17 | 0.685 | 0.02 | |
| Alexithymia | 68.88 ± 6.02 | 51.30 ± 7.70 | 46.88 ± 8.07 | 91.13 | <0.001 | 0.59 |
| Interoceptive Sensibility | 17.14 ± 4.25 | 21.90 ± 4.96 | 22.56 ± 4.50 | 15.18 | <0.001 | 0.19 |
| Interoceptive Accuracy | 0.46 ± 0.31 | 0.58 ± 0.20 | 3.70 | 0.058 | 0.16 | |
| Interoceptive Awareness | 0.25 ± 0.25 | 0.35 ± 0.24 | 2.68 | 0.106 | 0.11 | |
| Depressive Symptoms | 13.73 ± 7.70 | 10.42 ± 6.42 | 4.89 | 0.031 | 0.18 |
| Independent Variable | Indirect Effect | Direct Effect | Total Effect | |||
|---|---|---|---|---|---|---|
| β | 95%CI | β | 95%CI | β | 95%CI | |
| Interoceptive sensibility | −0.21 | [−0.39, −0.02] | −0.05 | [−0.42, 0.32] | −0.26 | [−0.59, −0.08] |
| Noticing | 0.59 | [−0.04, 1.38] | 0.61 | [−1.19, 2.40] | 1.20 | [−0.62, 3.00] |
| Not-distracting | −0.33 | [−0.93, 0.37] | 1.08 | [−0.70, 2.83] | 0.75 | [−1.07, 2.58] |
| Not-worrying | −0.66 | [−1.43, −0.04] | −1.44 | [−3.31, 0.43] | −2.10 | [−3.92, −0.29] |
| Attention regulation | −0.78 | [−1.74, −0.11] | −0.65 | [−2.40, 1.09] | −1.43 | [−3.09, −0.23] |
| Emotional awareness | −0.43 | [−1.14, 0.10] | 0.60 | [−0.97, 2.18] | 0.17 | [−1.45, 1.81] |
| Self-regulation | −0.87 | [−1.69, 0.03] | −0.52 | [−2.17, 1.13] | −1.39 | [−2.86, 0.08] |
| Body listening | −0.73 | [−1.59, −0.05] | −0.14 | [−1.70, 1.43] | −0.87 | [−2.38, −0.66] |
| Trust | −0.84 | [−2.02, 0.05] | −0.73 | [−2.35, 0.90] | −1.57 | [−2.93, −0.19] |
| Interoceptive accuracy | 0.01 | [−0.57, 0.78] | −2.30 | [−0.41, 0.05] | −2.20 | [−4.15, −0.43] |
| Interoceptive awareness | −0.91 | [−3.95, 0.39] | −1.57 | [−3.39, 0.25] | −2.48 | [−3.81, −0.19] |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Shen, H.; Li, J.; Zeng, R.; He, Y.; Dai, J.; Li, Z.; Li, Y.; Wei, G. Depression May Not Be Related to Impaired Interoceptive Sensibility: The Role of Alexithymia. Behav. Sci. 2025, 15, 995. https://doi.org/10.3390/bs15080995
Shen H, Li J, Zeng R, He Y, Dai J, Li Z, Li Y, Wei G. Depression May Not Be Related to Impaired Interoceptive Sensibility: The Role of Alexithymia. Behavioral Sciences. 2025; 15(8):995. https://doi.org/10.3390/bs15080995
Chicago/Turabian StyleShen, Haoran, Juanhua Li, Renjie Zeng, Yaping He, Jingang Dai, Zezhi Li, Youfa Li, and Gaoxia Wei. 2025. "Depression May Not Be Related to Impaired Interoceptive Sensibility: The Role of Alexithymia" Behavioral Sciences 15, no. 8: 995. https://doi.org/10.3390/bs15080995
APA StyleShen, H., Li, J., Zeng, R., He, Y., Dai, J., Li, Z., Li, Y., & Wei, G. (2025). Depression May Not Be Related to Impaired Interoceptive Sensibility: The Role of Alexithymia. Behavioral Sciences, 15(8), 995. https://doi.org/10.3390/bs15080995