
Designing for Engagement in Primary Health Education Through Digital Game-Based Learning: Cross-National Behavioral Evidence from the iLearn4Health Platform

 ,
,  , ,
, , 
Abstract
1. Introduction
2. Literature Review
2.1. Theoretical Frameworks Distinguishing Gamification and DGBL in Education and Health Promotion
2.2. Design Principles for Effective Gamification vs. DGBL in Primary School Health Education
2.3. Implementation Technologies for Primary School Health Education: Gamification Tools vs. Complete DGBL Platforms
3. Materials and Methods
3.1. Platform Design Features and Architecture
3.2. Design Evaluator Selection and Study Framework
3.3. Design Assessment Data Collection
- Steps Completed: The platform’s modular structure consisted of 55 instructional steps. The majority of teachers completed 53 or more steps, indicating high task completion rates across the cohort.
- Total Time Spent: Time-on-platform varied substantially—from a few minutes to multiple days—reflecting diverse usage patterns and levels of engagement. A small subset of users accounted for disproportionately high usage, with time spent exceeding 85 h in extreme cases.
- Progress Ratios: A normalized metric (steps completed/total steps) was used to compare engagement across users. This revealed a bimodal distribution: a large cluster of users completed most of the platform, while another cluster disengaged early.
- Engagement Patterns by Demographics: Correlation analysis revealed strong positive relationships between age and both time spent (r = 0.60) and steps completed (r = 0.80). The strongest correlation was observed between steps completed and time spent (r = 0.95), emphasizing the importance of sustained interaction for educational progression.
3.4. Technical Implementation and Design Validation
3.5. Design Testing and Validation Process
3.6. Online Training Program Development
4. Results
4.1. Design Evaluation Framework and Evaluator Demographics
- Identify developmental differences in navigation patterns and interaction behaviors that inform age-appropriate design principles
- Isolate cognitive processing variations in how health information is interpreted across developmental stages
- Quantify differences in engagement duration and pattern metrics between children and adults to refine age-targeted game mechanics
- Validate that game elements were appropriately calibrated for primary school cognitive capabilities rather than inadvertently designed for more advanced cognitive stages
- Top-left: A navigation puzzle encouraging decision-making as the character progresses toward an “Exit” by selecting the correct paths.
- Top-right: A multiple-choice question asking players to identify the healthiest meal option, reinforcing knowledge through engaging dialogue.
- Bottom-left: A character-run gameplay scene where players collect healthy food items while avoiding unhealthy ones.
- Bottom-right: A feedback screen highlighting the difference between vegetable oils and solid fats, reinforcing correct dietary decisions.
4.2. Digital Educational Games’ Implementation
- Top-left: A welcome message introduces players to the game world, encouraging them to embark on health-themed adventures.
- Top-right: Main menu screen offering the options to start a new game or continue a previous session, with language selection for inclusivity.
- Bottom-left: Game module selection screen showcasing a variety of educational topics such as healthy eating, physical activity, Internet safety, and more, each tailored to specific age groups.
- Bottom-right: Character selection interface where players can choose from diverse avatars, promoting personalization and engagement before starting the game.
4.3. Participant Demographics and Engagement Patterns
4.4. Design Engagement Pattern Analysis
4.5. Age-Based Design Assessment Patterns
4.6. Cross-National Design Implementation Assessment
4.7. Correlation Analysis and Design Engagement Relationships
4.8. Predictive Modeling of Design Engagement
4.9. Design User Typology Analysis
4.10. Design Validation Through Teacher Evaluation
4.11. Summary of Key Findings
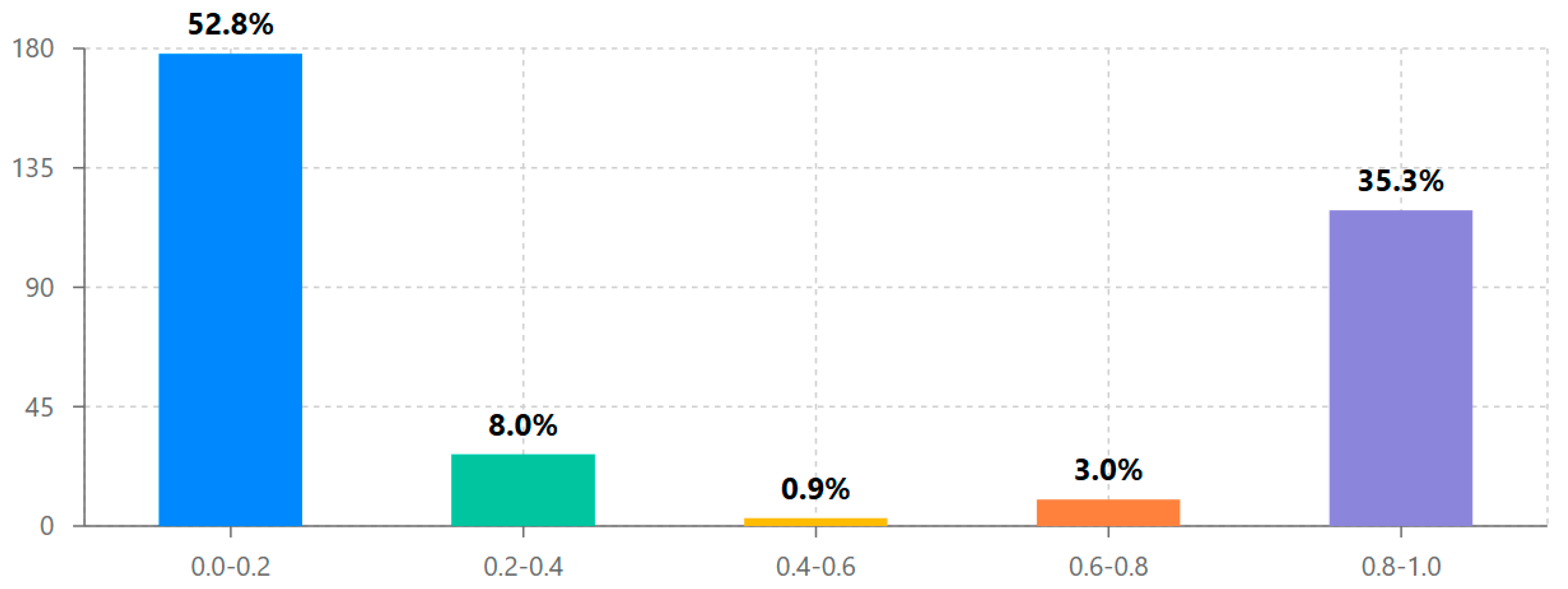
- Design assessment followed a distinctive bimodal distribution, with 52.8% conducting limited exploration and 35.3% performing comprehensive evaluation, supporting the hypothesis that once evaluators progress beyond initial interface exploration, they typically continue to systematic design assessment.
- Significant cross-national differences were observed in design engagement approaches, with Romania showing 53% higher average exploration ratios than Cyprus (0.460 vs. 0.301, p < 0.01), indicating important contextual factors in design assessment methodology across different educational systems.
- Initial engagement emerged as the strongest predictor of comprehensive design evaluation (β = 0.479, p < 0.001), suggesting that the early interface experience plays a crucial role in determining systematic assessment outcomes.
- Evaluator age had a statistically significant but small effect on design engagement (β = 0.108, p = 0.049), with the 26–35 age group showing the highest average assessment completion rates.
- Cluster analysis identified three distinct evaluator typologies (comprehensive assessors, initial explorers, and selective evaluators), providing a nuanced understanding of design assessment approaches beyond the simple bimodal distribution.
- A strong positive correlation between steps completed and time spent (r = 0.95, p < 0.001) confirmed that sustained engagement is essential for comprehensive design evaluation in Digital Game-Based Learning environments.
5. Discussion
5.1. Design Principles and Interface Effectiveness in DGBL vs. Gamification
5.2. Design Assessment and Interface Validation for Primary School Health Education
5.3. Design Implementation Considerations for Primary School Health Education Interfaces
5.4. Design Privacy and Ethical Considerations in Primary School Health Education Interfaces
5.5. Future Directions in DGBL Interface Design for Health Education
5.6. Design Limitations and Critical Assessment
5.7. Future Research Directions
6. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Abou Hashish, E. A., Al Najjar, H., Alharbi, M., Alotaibi, M., & Alqahtany, M. M. (2024). Faculty and students perspectives towards game-based learning in health sciences higher education. Heliyon, 10(12), e32898. [Google Scholar] [CrossRef] [PubMed]
- Aguiar-Castillo, L., & Clavijo-Rodriguez, A. (2021). Gamification and deep learning approaches in higher education. Journal of Hospitality, Leisure, Sport & Tourism Education, 28, 100290. [Google Scholar] [CrossRef]
- Alam, A. (2023, March 17–18). Leveraging the power of ‘modeling and computer simulation’ for education: An exploration of its potential for improved learning outcomes and enhanced student engagement. 2023 International Conference on Device Intelligence, Computing and Communication Technologies (DICCT) (pp. 445–450), Dehradun, India. [Google Scholar] [CrossRef]
- Alamri, I. K. A. (2024). Gameful learning: Investigating the impact of game elements, interactivity, and learning style on students’ success. Multidisciplinary Science Journal, 6(1), 2025108. [Google Scholar] [CrossRef]
- AlDaajeh, S., Saleous, H., Alrabaee, S., Barka, E., Breitinger, F., & Choo, K. K. R. (2022). The role of national cybersecurity strategies on the improvement of cybersecurity education. Computers & Security, 119, 102754. [Google Scholar] [CrossRef]
- All, A., Castellar, E. N. P., & Van Looy, J. (2021). Digital game-based learning effectiveness assessment: Reflections on study design. Computers & Education, 167, 104160. [Google Scholar] [CrossRef]
- Al-Rayes, S., Al Yaqoub, F. A., Alfayez, A., Alsalman, D., Alanezi, F., Alyousef, S., Alessa, A., Almutairi, B., Alharbi, R., Alosaimi, M., Aloufi, N., Alamri, E., Alharbi, S., Almutairi, T., Alshammari, T., Alotaibi, F., & Alanzi, T. M. (2022). Gaming elements, applications, and challenges of gamification in healthcare. Informatics in Medicine Unlocked, 31, 100974. [Google Scholar] [CrossRef]
- Andrea Navarro-Espinosa, J., Vaquero-Abellán, M., Perea-Moreno, A. J., Pedrós-Pérez, G., del Pilar Martínez-Jiménez, M., & Aparicio-Martínez, P. (2022). Gamification as a promoting tool of motivation for creating sustainable higher education institutions. International Journal of Environmental Research and Public Health, 19(5), 2599. [Google Scholar] [CrossRef] [PubMed]
- Andrews, J. C., Walker, K. L., Netemeyer, R. G., & Kees, J. (2023). Helping youth navigate privacy protection: Developing and testing the children’s online privacy scale. Journal of Public Policy & Marketing, 42(3), 345–362. [Google Scholar] [CrossRef]
- Antonopoulou, H., Halkiopoulos, C., Gkintoni, E., & Katsibelis, A. (2022). Application of gamification tools for identification of neurocognitive and social function in distance learning education. International Journal of Learning, Teaching and Educational Research, 21(5), 367–400. [Google Scholar] [CrossRef]
- Aresi, G., Chiavegatti, B., & Marta, E. (2024). Participants’ experience with gamification elements of a school-based health promotion intervention in Italy: A mixed-methods study. Journal of Prevention, 45(5), 820. [Google Scholar] [CrossRef]
- Arora, C., & Razavian, M. (2021). Ethics of gamification in health and fitness tracking. International Journal of Environmental Research and Public Health, 18(21), 11052. [Google Scholar] [CrossRef] [PubMed]
- Arruzza, E., & Chau, M. (2021). A scoping review of randomized controlled trials to assess the value of gamification in the higher education of health science students. Journal of Medical Imaging and Radiation Sciences, 52(1), 58–68. [Google Scholar] [CrossRef] [PubMed]
- Balalle, H. (2024). Exploring student engagement in technology-based education in relation to gamification, online/distance learning, and other factors: A systematic literature review. Social Sciences & Humanities Open, 9, 100870. [Google Scholar] [CrossRef]
- Basyoni, L., Tabassum, A., Shaban, K., Elmahjub, E., Halabi, O., & Qadir, J. (2024). Navigating privacy challenges in the metaverse: A comprehensive examination of current technologies and platforms. IEEE Internet of Things Magazine, 7(2), 48–55. [Google Scholar] [CrossRef]
- Birch, K., Cochrane, D. T., & Ward, C. (2021). Data as asset? The measurement, governance, and valuation of digital personal data by Big Tech. Big Data & Society, 8(1), 2053951721101730. [Google Scholar] [CrossRef]
- Breien, F. S., & Wasson, B. (2021). Narrative categorization in digital game-based learning: Engagement, motivation & learning. British Journal of Educational Technology, 52(1), 91–111. [Google Scholar] [CrossRef]
- Burn, A. M., Ford, T. J., Stochl, J., Jones, P. B., Perez, J., & Anderson, J. K. (2022). Developing a web-based app to assess mental health difficulties in secondary school pupils: Qualitative user-centered design study. JMIR Formative Research, 6(2), e30565. [Google Scholar] [CrossRef] [PubMed]
- Buzzai, C., Sorrenti, L., Costa, S., Toffle, M. E., & Filippello, P. (2021). The relationship between school-basic psychological need satisfaction and frustration, academic engagement and academic achievement. School Psychology International, 42(4), 497–519. [Google Scholar] [CrossRef]
- Camacho-Sánchez, R., Manzano-León, A., Rodríguez-Ferrer, J. M., Serna, J., & Lavega-Burgués, P. (2023). Game-based learning and gamification in physical education: A systematic review. Education Sciences, 13(2), 183. [Google Scholar] [CrossRef]
- Camacho-Sánchez, R., Rillo-Albert, A., & Lavega-Burgués, P. (2022). Gamified digital game-based learning as a pedagogical strategy: Student academic performance and motivation. Applied Sciences, 12(21), 11214. [Google Scholar] [CrossRef]
- Caprara, L., & Caprara, C. (2022). Effects of virtual learning environments: A scoping review of literature. Education and Information Technologies, 27(1), 785–825. [Google Scholar] [CrossRef] [PubMed]
- Castellano-Tejedor, C., & Cencerrado, A. (2024). Gamification for mental health and health psychology: Insights at the first quarter mark of the 21st century. International Journal of Environmental Research and Public Health, 21(8), 990. [Google Scholar] [CrossRef] [PubMed]
- Chatterjee, A., Prinz, A., Gerdes, M., Martinez, S., Pahari, N., & Meena, Y. K. (2022). ProHealth eCoach: User-centered design and development of an eCoach app to promote healthy lifestyle with personalized activity recommendations. BMC Health Services Research, 22(1), 1–20. [Google Scholar] [CrossRef] [PubMed]
- Chen, F. H. (2021). Sustainable education through e-learning: The case study of iLearn2.0. Sustainability, 13(18), 10186. [Google Scholar] [CrossRef]
- Chen, Y., & Zhao, S. (2022). Chinese EFL learners’ acceptance of gamified vocabulary learning apps: An integration of self-determination theory and technology acceptance model. Sustainability, 14(18), 11288. [Google Scholar] [CrossRef]
- Cheng, C., & Ebrahimi, O. V. (2023a). A meta-analytic review of gamified interventions in mental health enhancement. Computers in Human Behavior, 138, 107621. [Google Scholar] [CrossRef]
- Cheng, C., & Ebrahimi, O. V. (2023b). Gamification: A novel approach to mental health promotion. Current Psychiatry Reports, 25(11), 645–656. [Google Scholar] [CrossRef]
- Christopoulos, A., & Sprangers, P. (2021). Integration of educational technology during the COVID-19 pandemic: An analysis of teacher and student receptions. Cogent Education, 8(1), 1964690. [Google Scholar] [CrossRef]
- Cichy, P., Salge, T. O., & Kohli, R. (2021). Privacy concerns and data sharing in the internet of things: Mixed methods evidence from connected cars. MIS Quarterly, 45(4), 1863–1892. [Google Scholar] [CrossRef]
- Cong-Lem, N., Soyoof, A., & Tsering, D. (2025). A systematic review of the limitations and associated opportunities of ChatGPT. International Journal of Human-Computer Interaction, 41(2), 234–256. [Google Scholar] [CrossRef]
- Crepax, T., Muntés-Mulero, V., Martinez, J., & Ruiz, A. (2022). Information technologies exposing children to privacy risks: Domains and children-specific technical controls. Computer Standards & Interfaces, 82, 103624. [Google Scholar] [CrossRef]
- Dah, J., Hussin, N., Zaini, M. K., Isaac Helda, L., Senanu Ametefe, D., & Adozuka Aliu, A. (2024). Gamification is not working: Why? Games and Culture, 19(4), 456–478. [Google Scholar] [CrossRef]
- Dahalan, F., Alias, N., & Shaharom, M. S. N. (2024). Gamification and game based learning for vocational education and training: A systematic literature review. Education and Information Technologies, 29, 3685–3720. [Google Scholar] [CrossRef]
- de Carvalho, C. V., & Coelho, A. (2022). Game-based learning, gamification in education and serious games. Computers, 11(3), 36. [Google Scholar] [CrossRef]
- del Cura-González, I., Ariza-Cardiel, G., Polentinos-Castro, E., López-Rodríguez, J. A., Sanz-Cuesta, T., Barrio-Cortes, J., García-Sagredo, P., Hernández-Santiago, V., Rodríguez-Barrientos, R., Zabaleta-del-Olmo, E., García-Agua-Soler, N., González-González, A. I., García-de-Blas-González, F., de-Dios-del-Valle, R., Escortell-Mayor, E., & Martín-Fernández, J. (2022). Effectiveness of a game-based educational strategy e-EDUCAGUIA for implementing antimicrobial clinical practice guidelines in family medicine residents in Spain: A randomized clinical trial by cluster. BMC Medical Education, 22(1), 843. [Google Scholar] [CrossRef] [PubMed]
- De Salas, K., Ashbarry, L., Seabourne, M., Lewis, I., Wells, L., Dermoudy, J., Williams, R., Scott, J., & Kay, J. (2022). Improving environmental outcomes with games: An exploration of behavioral and technological design and evaluation approaches. Simulation & Gaming, 53(5), 470–512. [Google Scholar] [CrossRef]
- Di Minin, E., Fink, C., Hausmann, A., Kremer, J., & Kulkarni, R. (2021). How to address data privacy concerns when using social media data in conservation science. Conservation Biology, 35(2), 437–446. [Google Scholar] [CrossRef]
- Drljević, N., Botički, I., & Wong, L. H. (2022). Investigating the different facets of student engagement during augmented reality use in primary school. British Journal of Educational Technology, 53(4), 1032–1049. [Google Scholar] [CrossRef]
- Esmaeilzadeh, P. (2021). The influence of gamification and information technology identity on postadoption behaviors of health and fitness app users: Empirical study in the United States. JMIR Serious Games, 9(4), e28282. [Google Scholar] [CrossRef]
- Farhan, K. A., Asadullah, A. B. M., Kommineni, H. P., Gade, P. K., & Venkata, S. S. M. G. N. (2023). Machine learning-driven gamification: Boosting user engagement in business. Global Disclosure of Economics and Business, 12(1), 41–52. [Google Scholar] [CrossRef]
- Feldhacker, D. R., Wesner, C., Yockey, J., Larson, J., & Norris, D. (2025). Strategies for Health: A game-based, interprofessional approach to teaching social determinants of health: A randomized controlled pilot study. Journal of Interprofessional Care, 39(1), 85–94. [Google Scholar] [CrossRef] [PubMed]
- Furtado, L. S., de Souza, R. F., Lima, J. L. D. R., & Oliveira, S. R. B. (2021). Teaching method for software measurement process based on gamification or serious games: A systematic review of the literature. International Journal of Computer Games Technology, 2021, 8873997. [Google Scholar] [CrossRef]
- Gajardo Sánchez, A. D., Murillo-Zamorano, L. R., López-Sánchez, J., & Bueno-Muñoz, C. (2023). Gamification in health care management: Systematic review of the literature and research agenda. SAGE Open, 13(4), 21582440231218834. [Google Scholar] [CrossRef]
- Gao, F. (2024). Advancing gamification research and practice with three underexplored ideas in self-determination theory. TechTrends, 68(3), 412–423. [Google Scholar] [CrossRef]
- Ghahramani, A., de Courten, M., & Prokofieva, M. (2022). The potential of social media in health promotion beyond creating awareness: An integrative review. BMC Public Health, 22(1), 2399. [Google Scholar] [CrossRef]
- Ghosh, T., S., S., & Dwivedi, Y. K. (2022). Brands in a game or a game for brands? Comparing the persuasive effectiveness of in-game advertising and advergames. Psychology & Marketing, 39(11), 2028–2045. [Google Scholar] [CrossRef]
- Gkintoni, E., Antonopoulou, H., Sortwell, A., & Halkiopoulos, C. (2025a). Challenging cognitive load theory: The role of educational neuroscience and artificial intelligence in redefining learning efficacy. Brain Sciences, 15(2), 203. [Google Scholar] [CrossRef]
- Gkintoni, E., Dimakos, I., & Nikolaou, G. (2025b). Cognitive insights from emotional intelligence: A systematic review of EI models in educational achievement. Emerging Science Journal, 8, 262–297. [Google Scholar] [CrossRef]
- Gkintoni, E., Vantaraki, F., Skoulidi, C., Anastassopoulos, P., & Vantarakis, A. (2024a). Gamified health promotion in schools: The integration of neuropsychological aspects and CBT—A systematic review. Medicina, 60(12), 2085. [Google Scholar] [CrossRef]
- Gkintoni, E., Vantaraki, F., Skoulidi, C., Anastassopoulos, P., & Vantarakis, A. (2024b). Promoting physical and mental health among children and adolescents via gamification—A conceptual systematic review. Behavioral Sciences, 14(2), 102. [Google Scholar] [CrossRef]
- Govender, T., & Arnedo-Moreno, J. (2021). An analysis of game design elements used in digital game-based language learning. Sustainability, 13(12), 6679. [Google Scholar] [CrossRef]
- Guan, X., Sun, C., Hwang, G. J., Xue, K., & Wang, Z. (2024). Applying game-based learning in primary education: A systematic review of journal publications from 2010 to 2020. Interactive Learning Environments, 32(4), 1456–1478. [Google Scholar] [CrossRef]
- Gupta, P., & Goyal, P. (2022). Is game-based pedagogy just a fad? A self-determination theory approach to gamification in higher education. International Journal of Educational Management, 36(4), 456–472. [Google Scholar] [CrossRef]
- Halkiopoulos, C., & Gkintoni, E. (2024). Leveraging AI in E-learning: Personalized learning and adaptive assessment through cognitive neuropsychology—A systematic analysis. Electronics, 13(18), 3762. [Google Scholar] [CrossRef]
- Hassan, A., Pinkwart, N., & Shafi, M. (2021). Serious games to improve social and emotional intelligence in children with autism. Entertainment Computing, 38, 100417. [Google Scholar] [CrossRef]
- Hassan Alhazmi, A., & Asanka Gamagedara Arachchilage, N. (2023). Evaluation of game design framework using a gamified browser-based application. Computers & Security, 128, 103141. [Google Scholar]
- Hayes, J. L., Brinson, N. H., Bott, G. J., & Moeller, C. M. (2021). The influence of consumer-brand relationships on the personalized advertising privacy calculus in social media. Journal of Interactive Marketing, 55(1), 16–30. [Google Scholar] [CrossRef]
- Henry, J., Hernalesteen, A., & Collard, A. S. (2021). Teaching artificial intelligence to K-12 through a role-playing game questioning the intelligence concept. KI-Künstliche Intelligenz, 35(2), 171–179. [Google Scholar] [CrossRef]
- Höyng, M. (2022). Encouraging gameful experience in digital game-based learning: A double-mediation model of perceived instructional support, group engagement, and flow. Computers & Education, 180, 104408. [Google Scholar] [CrossRef]
- Hsiao, W. Y., Chen, C. H., Chen, P. C., & Hou, W. H. (2024). Investigating the effects of different game-based learning on the health care knowledge and emotions for middle-aged and older adults. Interactive Learning Environments, 32(10), 4182–4197. [Google Scholar] [CrossRef]
- Ibrahim, E. N. M., Jamali, N., & Suhaimi, A. I. H. (2021). Exploring gamification design elements for mental health support. International Journal of Advanced Technology and Engineering Exploration, 8(74), 114. [Google Scholar] [CrossRef]
- Jingili, N., Oyelere, S. S., Nyström, M. B., & Anyshchenko, L. (2023). A systematic review on the efficacy of virtual reality and gamification interventions for managing anxiety and depression. Frontiers in Digital Health, 5, 1239435. [Google Scholar] [CrossRef]
- Keyes, K. M., & Platt, J. M. (2024). Annual Research Review: Sex, gender, and internalizing conditions among adolescents in the 21st century—Trends, causes, consequences. Journal of Child Psychology and Psychiatry, 65(4), 384–408. [Google Scholar] [CrossRef] [PubMed]
- Khaleghi, A., Aghaei, Z., & Mahdavi, M. A. (2021). A gamification framework for cognitive assessment and cognitive training: Qualitative study. JMIR Serious Games, 9(1), e21900. [Google Scholar] [CrossRef]
- Kim, J., & Castelli, D. M. (2021). Effects of gamification on behavioral change in education: A meta-analysis. International Journal of Environmental Research and Public Health, 18(7), 3550. [Google Scholar] [CrossRef] [PubMed]
- Kniestedt, I., Lefter, I., Lukosch, S., & Brazier, F. M. (2022). Re-framing engagement for applied games: A conceptual framework. Entertainment Computing, 40, 100475. [Google Scholar] [CrossRef]
- Komljenovic, J. (2022). The future of value in digitalised higher education: Why data privacy should not be our biggest concern. Higher Education, 83(1), 119–135. [Google Scholar] [CrossRef]
- Krath, J., Schürmann, L., & Von Korflesch, H. F. O. (2021). Revealing the theoretical basis of gamification: A systematic review and analysis of theory in research on gamification, serious games, and game-based learning. Computers in Human Behavior, 125, 106963. [Google Scholar] [CrossRef]
- Kulkov, I., Kulkova, J., Rohrbeck, R., Menvielle, L., Kaartemo, V., & Makkonen, H. (2024). Artificial intelligence-driven sustainable development: Examining organizational, technical, and processing approaches to achieving global goals. Sustainable Development, 32(2), 456–473. [Google Scholar] [CrossRef]
- Landers, R. N., & Sanchez, D. R. (2022). Game-based, gamified, and gamefully designed assessments for employee selection: Definitions, distinctions, design, and validation. International Journal of Selection and Assessment, 30(1), 1–13. [Google Scholar] [CrossRef]
- Lappeman, J., Marlie, S., Johnson, T., & Poggenpoel, S. (2022). Trust and digital privacy: Willingness to disclose personal information to banking chatbot services. Journal of Financial Services Marketing, 28(2), 337–352. [Google Scholar] [CrossRef]
- Lee, C., & Ahmed, G. (2021). Improving IoT privacy, data protection, and security concerns. International Journal of Technology, Innovation and Management (IJTIM), 1(1), 18–33. [Google Scholar] [CrossRef]
- Leitão, R., Maguire, M., Turner, S., Arenas, F., & Guimarães, L. (2022a). Ocean literacy gamified: A systematic evaluation of the effect of game elements on students’ learning experience. Environmental Education Research, 28(3), 412–432. [Google Scholar] [CrossRef]
- Leitão, R., Maguire, M., Turner, S., & Guimarães, L. (2022b). A systematic evaluation of game elements effects on students’ motivation. Education and Information Technologies, 27(2), 2341–2365. [Google Scholar] [CrossRef]
- Leonardou, A., Rigou, M., Panagiotarou, A., & Garofalakis, J. (2022). Effect of OSLM features and gamification motivators on motivation in DGBL: Pupils’ viewpoint. Smart Learning Environments, 9(1), 14. [Google Scholar] [CrossRef]
- Li, Q., Yin, X., Yin, W., Dong, X., & Li, Q. (2023). Evaluation of gamification techniques in learning abilities for higher school students using FAHP and EDAS methods. Soft Computing, 27(14), 9321–9338. [Google Scholar] [CrossRef]
- Luo, Z. (2022). Gamification for educational purposes: What are the factors contributing to varied effectiveness? Education and Information Technologies, 27(1), 1035–1057. [Google Scholar] [CrossRef]
- Lynch, P., Singal, N., & Francis, G. A. (2024). Educational technology for learners with disabilities in primary school settings in low-and middle-income countries: A systematic literature review. Educational Review, 76(2), 234–256. [Google Scholar] [CrossRef]
- Lynch, Z., & Sankey, M. (2016). Reboot your course—From beta to better. Distance Education, 37(2), 156–170. [Google Scholar]
- Macey, J., Adam, M., Hamari, J., & Benlian, A. (2025). Examining the commonalities and differences between gamblification and gamification: A theoretical perspective. International Journal of Human-Computer Interaction, 41(3), 234–256. [Google Scholar] [CrossRef]
- Masi, L., Abadie, P., Herba, C., Emond, M., Gingras, M. P., & Amor, L. B. (2021). Video games in ADHD and non-ADHD children: Modalities of use and association with ADHD symptoms. Frontiers in Pediatrics, 9, 632272. [Google Scholar] [CrossRef]
- Mazeas, A., Duclos, M., Pereira, B., & Chalabaev, A. (2022). Evaluating the effectiveness of gamification on physical activity: Systematic review and meta-analysis of randomized controlled trials. Journal of Medical Internet Research, 24(1), e26779. [Google Scholar] [CrossRef]
- Michael, K. (2024). Mitigating risk and ensuring human flourishing using design standards: IEEE 2089–2021 an age appropriate digital services framework for children. IEEE Transactions on Technology and Society, 5(3), 145–158. [Google Scholar] [CrossRef]
- Mohanty, S., & Christopher, B. P. (2023). A bibliometric analysis of the use of the gamification octalysis framework in training: Evidence from web of science. Humanities and Social Sciences Communications, 10(1), 836. [Google Scholar] [CrossRef]
- Muniandy, N., Kamsin, A., & Sabri, M. I. (2023, November 18). Enhancing children’s health awareness through narrative game-based learning using digital technology: A framework and methodology. 2023 9th International HCI and UX Conference in Indonesia (CHIuXiD) (pp. 123–128), Bali, Indonesia. [Google Scholar] [CrossRef]
- Nadeem, M., Oroszlanyova, M., & Farag, W. (2023). Effect of digital game-based learning on student engagement and motivation. Computers, 12(9), 177. [Google Scholar] [CrossRef]
- Nivedhitha, K. S., Giri, G., & Pasricha, P. (2025). Gamification as a panacea to workplace cyberloafing: An application of self-determination and social bonding theories. Internet Research, 35(1), 123–145. [Google Scholar] [CrossRef]
- Nordby, A., Vibeto, H., Mobbs, S., & Sverdrup, H. U. (2024). System thinking in gamification. SN Computer Science, 5(1), 299. [Google Scholar] [CrossRef]
- Novak, E., McDaniel, K., Daday, J., & Soyturk, I. (2022). Frustration in technology-rich learning environments: A scale for assessing student frustration with e-textbooks. British Journal of Educational Technology, 53(2), 456–473. [Google Scholar] [CrossRef]
- Oke, A. E., Aliu, J., Tunji-Olayeni, P., & Abayomi, T. (2024). Application of gamification for sustainable construction: An evaluation of the challenges. Construction Innovation, 24(3), 567–584. [Google Scholar] [CrossRef]
- Oliveira, H., Figueiredo, G., Pereira, B., Magalhães, M., Rosário, P., & Magalhães, P. (2024). Understanding children’s perceptions of game elements in an online gamified intervention: Contributions by the self-determination theory. International Journal of Human-Computer Interaction, 40(12), 3456–3471. [Google Scholar] [CrossRef]
- Oliveira, W., Hamari, J., Joaquim, S., Toda, A. M., Palomino, P. T., Vassileva, J., & Isotani, S. (2022). The effects of personalized gamification on students’ flow experience, motivation, and enjoyment. Smart Learning Environments, 9(1), 16. [Google Scholar] [CrossRef]
- Ongoro, C. A., & Fanjiang, Y. Y. (2023). Digital game-based technology for English language learning in preschools and primary schools: A systematic analysis. IEEE Transactions on Learning Technologies, 16(3), 345–362. [Google Scholar] [CrossRef]
- Papakostas, C. (2024). Faith in frames: Constructing a digital game-based learning framework for religious education. Teaching Theology & Religion, 27(2), 123–142. [Google Scholar] [CrossRef]
- Peláez, C. A., & Solano, A. (2023). A practice for the design of interactive multimedia experiences based on gamification: A case study in elementary education. Sustainability, 15(3), 2385. [Google Scholar] [CrossRef]
- Pellas, N., Mystakidis, S., & Christopoulos, A. (2021). A systematic literature review on the user experience design for game-based interventions via 3D virtual worlds in K-12 education. Multimodal Technologies and Interaction, 5(6), 28. [Google Scholar] [CrossRef]
- Pitic, D., & Irimiaș, T. (2023). Enhancing students’ engagement through a business simulation game: A qualitative study within a higher education management course. The International Journal of Management Education, 21(2), 100839. [Google Scholar] [CrossRef]
- Qiu, Y. (2024). The role of playfulness in gamification for health behavior motivation. Computers in Human Behavior, 148, 107892. [Google Scholar]
- Quach, S., Thaichon, P., Martin, K. D., Weaven, S., & Palmatier, R. W. (2022). Digital technologies: Tensions in privacy and data. Journal of the Academy of Marketing Science, 50(6), 1299–1323. [Google Scholar] [CrossRef]
- Riar, M., Morschheuser, B., Zarnekow, R., & Hamari, J. (2022). Gamification of cooperation: A framework, literature review and future research agenda. International Journal of Information Management, 65, 102549. [Google Scholar] [CrossRef]
- Ruggiu, D., Blok, V., Coenen, C., Kalloniatis, C., Kitsiou, A., Mavroeidi, A. G., Porcari, A., Rerimassie, V., Stahl, B. C., & Sitzia, A. (2022). Responsible innovation at work: Gamification, public engagement, and privacy by design. Journal of Responsible Innovation, 9(3), 315–343. [Google Scholar] [CrossRef]
- Rycroft-Smith, L. (2022). Knowledge brokering to bridge the research-practice gap in education: Where are we now? Review of Education, 10(2), e3341. [Google Scholar] [CrossRef]
- Samala, A. D., Rawas, S., Wang, T., Reed, J. M., Kim, J., Howard, N. J., & Ertz, M. (2025). Unveiling the landscape of generative artificial intelligence in education: A comprehensive taxonomy of applications, challenges, and future prospects. Education and Information Technologies, 30(2), 1234–1267. [Google Scholar] [CrossRef]
- Sáiz-Manzanares, M. C., Martin, C. F., Alonso-Martínez, L., & Almeida, L. S. (2021). Usefulness of digital game-based learning in nursing and occupational therapy degrees: A comparative study at the University of Burgos. International Journal of Environmental Research and Public Health, 18(22), 11757. [Google Scholar] [CrossRef]
- Sezgin, S., & Yüzer, T. V. (2022). Analyzing adaptive gamification design principles for online courses. Behaviour & Information Technology, 41(3), 567–583. [Google Scholar] [CrossRef]
- Shaheen, A., Ali, S., & Fotaris, P. (2023). Assessing the efficacy of reflective game design: A design-based study in digital game-based learning. Education Sciences, 13(12), 1204. [Google Scholar] [CrossRef]
- Shahzad, M. F., Xu, S., Rehman, O., & Javed, I. (2023). Impact of gamification on green consumption behavior integrating technological awareness, motivation, enjoyment, and virtual CSR. Scientific Reports, 13(1), 20835. [Google Scholar] [CrossRef] [PubMed]
- Shrestha, A. K., Barthwal, A., Campbell, M., Shouli, A., Syed, S., Joshi, S., & Vassileva, J. (2024). Navigating AI to unpack youth privacy concerns: An in-depth exploration and systematic review. arXiv, arXiv:2412.16369. [Google Scholar]
- Simonofski, A., Zuiderwijk, A., Clarinval, A., & Hammedi, W. (2022). Tailoring open government data portals for lay citizens: A gamification theory approach. International Journal of Information Management, 65, 102511. [Google Scholar] [CrossRef]
- Sinha, N. (2021). Introducing gamification for advancing current mental healthcare and treatment practices. In IoT in healthcare and ambient assisted living (pp. 234–251). Springer. [Google Scholar] [CrossRef]
- Speelman, E. N., Escano, E., Marcos, D., & Becu, N. (2023). Serious games and citizen science; from parallel pathways to greater synergies. Current Opinion in Environmental Sustainability, 62, 101320. [Google Scholar] [CrossRef]
- Taneja-Johansson, S., & Singal, N. (2025). Pathways to inclusive and equitable quality education for people with disabilities: Cross-context conversations and mutual learning. International Journal of Inclusive Education, 29(4), 567–584. [Google Scholar] [CrossRef]
- Torresan, S., & Hinterhuber, A. (2023). Continuous learning at work: The power of gamification. Management Decision, 61(8), 2234–2253. [Google Scholar] [CrossRef]
- Trang, S., & Weiger, W. H. (2021). The perils of gamification: Does engaging with gamified services increase users’ willingness to disclose personal information? Computers in Human Behavior, 116, 106644. [Google Scholar] [CrossRef]
- Tyack, A., & Mekler, E. D. (2024). Self-determination theory and HCI games research: Unfulfilled promises and unquestioned paradigms. ACM Transactions on Computer-Human Interaction, 31(2), 40. [Google Scholar] [CrossRef]
- Tzachrista, M., Gkintoni, E., & Halkiopoulos, C. (2023). Neurocognitive profile of creativity in improving academic performance—A scoping review. Education Sciences, 13(11), 1127. [Google Scholar] [CrossRef]
- Udoudom, U., George, K., & Igiri, A. (2023). Impact of digital learning platforms on behaviour change communication in public health education. Pancasila International Journal of Applied Social Science, 2(1), 512. [Google Scholar] [CrossRef]
- Van Toorn, C., Kirshner, S. N., & Gabb, J. (2022). Gamification of query-driven knowledge sharing systems. Behaviour & Information Technology, 41(5), 959–980. [Google Scholar] [CrossRef]
- Vázquez-Calatayud, M., García-García, R., Regaira-Martínez, E., & Gómez-Urquiza, J. (2024). Real-world and game-based learning to enhance decision-making. Nurse Education Today, 138, 106276. [Google Scholar] [CrossRef]
- Ventouris, A., Panourgia, C., & Hodge, S. (2021). Teachers’ perceptions of the impact of technology on children and young people’s emotions and behaviours. International Journal of Educational Research Open, 2, 100081. [Google Scholar] [CrossRef]
- Vijay, M., & Jayan, J. P. (2023, August 10–11). Evolution of research on adaptive gamification: A bibliometric study. 2023 International Conference on Circuit Power and Computing Technologies (ICCPCT) (pp. 1–6), Kollam, India. [Google Scholar] [CrossRef]
- Vorlíček, M., Prycl, D., Heidler, J., Herrador-Colmenero, M., Nábělková, J., Mitáš, J., Rubín, L., Krejčí, M., Jakubec, L., & Frömel, K. (2024). Gameful education: A study of gamifiter application’s role in promoting physical activity and active lifestyle. Smart Learning Environments, 11(1), 1–14. [Google Scholar] [CrossRef]
- Wang, G., Zhao, J., Van Kleek, M., & Shadbolt, N. (2022, April 29–May 5). Informing age-appropriate AI: Examining principles and practices of AI for children. 2022 CHI Conference on Human Factors in Computing Systems (pp. 1–15), New Orleans, LA, USA. [Google Scholar] [CrossRef]
- Wang, K., Liu, P., Zhang, J., Zhong, J., Luo, X., Huang, J., & Zheng, Y. (2023). Effects of digital game-based learning on students’ cyber wellness literacy, learning motivations, and engagement. Sustainability, 15(7), 5716. [Google Scholar] [CrossRef]
- Warsinsky, S., Schmidt-Kraepelin, M., Rank, S., Thiebes, S., & Sunyaev, A. (2021). Conceptual ambiguity surrounding gamification and serious games in healthcare: Literature review and development of game-based intervention reporting guidelines (GAMING). Journal of Medical Internet Research, 23(9), e30390. [Google Scholar] [CrossRef]
- Weatherly, K. I. C. H., Wright, B. A., & Lee, E. Y. (2024). Digital game-based learning in music education: A systematic review between 2011 and 2023. Research Studies in Music Education, 46(2), 234–256. [Google Scholar] [CrossRef]
- Wiljén, A., Chaplin, J. E., Crine, V., Jobe, W., Johnson, E., Karlsson, K., Forsander, G., & Nilsson, S. (2022). The development of an mHealth tool for children with long-term illness to enable person-centered communication: User-centered design approach. JMIR Pediatrics and Parenting, 5(1), e30364. [Google Scholar] [CrossRef] [PubMed]
- Xiao, R., Wu, Z., & Hamari, J. (2022). Internet-of-gamification: A review of literature on IoT-enabled gamification for user engagement. International Journal of Human-Computer Interaction, 38(12), 1113–1137. [Google Scholar] [CrossRef]
- Xiong, Z., Liu, Q., & Huang, X. (2022). The influence of digital educational games on preschool children’s creative thinking. Computers & Education, 189, 104578. [Google Scholar] [CrossRef]
- Xu, J., Lio, A., Dhaliwal, H., Andrei, S., Balakrishnan, S., Nagani, U., & Samadder, S. (2021). Psychological interventions of virtual gamification within academic intrinsic motivation: A systematic review. Journal of Affective Disorders, 293, 444–465. [Google Scholar] [CrossRef] [PubMed]
- Xu, M., Luo, Y., Zhang, Y., Xia, R., Qian, H., & Zou, X. (2023). Game-based learning in medical education. Frontiers in Public Health, 11, 1113682. [Google Scholar] [CrossRef] [PubMed]
- Yang, C., Ye, H. J., & Feng, Y. (2021). Using gamification elements for competitive crowdsourcing: Exploring the underlying mechanism. Behaviour & Information Technology, 40(9), 837–854. [Google Scholar] [CrossRef]
- Zahedi, L., Batten, J., Ross, M., Potvin, G., Damas, S., Clarke, P., & Davis, D. (2021). Gamification in education: A mixed-methods study of gender on computer science students’ academic performance and identity development. Journal of Computing in Higher Education, 33(2), 441–474. [Google Scholar] [CrossRef]
- Zhang, Q., & Yu, Z. (2022). Meta-analysis on investigating and comparing the effects on learning achievement and motivation for gamification and game-based learning. Education Research International, 2022, 1519880. [Google Scholar] [CrossRef]
- Zhang, R., Cheng, G., & Zou, D. (2025). Effects of digital game elements on engagement and vocabulary development. University of Hawaii Press. [Google Scholar]
- Zhao, D., Inaba, M., & Monroy-Hernández, A. (2022). Understanding teenage perceptions and configurations of privacy on Instagram. Proceedings of the ACM on Human-Computer Interaction, 6(CSCW2), 550. [Google Scholar] [CrossRef]
- Zhao, D., Playfoot, J., De Nicola, C., Guarino, G., Bratu, M., Di Salvadore, F., & Muntean, G. M. (2021). An innovative multi-layer gamification framework for improved STEM learning experience. IEEE Access, 9, 164892–164909. [Google Scholar] [CrossRef]
- Zohari, M., Karim, N., Malgard, S., Aalaa, M., Asadzandi, S., & Borhani, S. (2023). Comparison of gamification, game-based learning, and serious games in medical education: A scientometrics analysis. Journal of Advances in Medical Education & Professionalism, 11(3), 145–157. [Google Scholar]
- Zolfaghari, Z., Karimian, Z., Zarifsanaiey, N., & Farahmandi, A. Y. (2025). A scoping review of gamified applications in English language teaching: A comparative discussion with medical education. BMC Medical Education, 25(1), 22. [Google Scholar] [CrossRef] [PubMed]








{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Variable | M | SD | Min | Max | Mdn | Skewness | Kurtosis |
|---|---|---|---|---|---|---|---|
| Age (years) | 38.64 | 14.04 | 18 | 66 | 41 | −0.27 | −0.83 |
| Steps completed | 22.31 | 23.79 | 0 | 53 | 8 | 0.31 | −1.85 |
| Progress ratio | 0.41 | 0.43 | 0 | 0.96 | 0.15 | 0.47 | −1.74 |
| Country | N | % | 95% CI |
|---|---|---|---|
| Romania | 209 | 62.0 | [56.8, 67.2] |
| Cyprus | 52 | 15.4 | [11.5, 19.3] |
| Greece | 38 | 11.3 | [7.9, 14.7] |
| Spain | 35 | 10.4 | [7.1, 13.7] |
| Poland | 3 | 0.9 | [0, 1.9] |
| Progress Ratio | n | % | Cumulative % |
|---|---|---|---|
| 0.0–0.2 (Limited exploration) | 178 | 52.8 | 52.8 |
| 0.2–0.4 (Basic assessment) | 27 | 8.0 | 60.8 |
| 0.4–0.6 (Moderate assessment) | 3 | 0.9 | 61.7 |
| 0.6–0.8 (Extended assessment) | 10 | 3.0 | 64.7 |
| 0.8–1.0 (Comprehensive assessment) | 119 | 35.3 | 100.0 |
| Age Group | n | Steps Completed | Progress Ratio | Cohen’s d | |||
|---|---|---|---|---|---|---|---|
| M | SD | 95% CI | M | SD | |||
| 18–25 | 55 | 21.45 | 22.87 | [15.20, 27.70] | 0.39 | 0.42 | - |
| 26–35 | 42 | 24.83 | 23.15 | [17.61, 32.05] | 0.45 | 0.42 | 0.14 |
| 36–50 | 183 | 22.55 | 24.16 | [19.02, 26.08] | 0.41 | 0.44 | 0.05 |
| 51–65 | 52 | 20.10 | 24.33 | [13.32, 26.88] | 0.37 | 0.44 | −0.05 |
| Country | n | Progress Ratio | Significant Differences | ||
|---|---|---|---|---|---|
| M | SD | 95% CI | |||
| Romania | 209 | 0.460 | 0.44 | [0.399, 0.521] | A |
| Poland | 3 | 0.370 | 0.41 | [0.000, 0.791] | a,b |
| Spain | 35 | 0.337 | 0.42 | [0.203, 0.471] | a,b |
| Greece | 38 | 0.315 | 0.40 | [0.190, 0.440] | b |
| Cyprus | 52 | 0.301 | 0.38 | [0.196, 0.406] | b |
| Source | SS | df | MS | F | p | η2 |
|---|---|---|---|---|---|---|
| Between groups | 1.26 | 4 | 0.315 | 4.37 | 0.002 | 0.050 |
| Within groups | 23.94 | 332 | 0.072 | |||
| Total | 25.20 | 336 |
| Variables | R | 95% CI | p |
|---|---|---|---|
| Steps completed—Time spent | 0.95 | [0.93, 0.97] | <0.001 |
| Age—Steps completed (full sample) | 0.01 | [−0.10, 0.12] | 0.859 |
| Age—Steps completed (adult subgroup) | 0.80 | [0.73, 0.85] | <0.001 |
| Age—Time spent (adult subgroup) | 0.60 | [0.50, 0.69] | <0.001 |
| Design exploration ratio—Time spent | 0.94 | [0.91, 0.96] | <0.001 |
| Predictor | B | SE B | β | t | p | 95% CI |
|---|---|---|---|---|---|---|
| Constant | 0.210 | 0.074 | 2.84 | 0.005 | [0.065, 0.355] | |
| Age | 0.003 | 0.002 | 0.108 | 1.97 | 0.049 | [0.000, 0.006] |
| Initial engagement * | 0.346 | 0.038 | 0.479 | 9.11 | <0.001 | [0.271, 0.421] |
| Country: Romania † | 0.159 | 0.048 | 0.183 | 3.31 | 0.001 | [0.065, 0.253] |
| Country: Spain † | 0.036 | 0.065 | 0.026 | 0.55 | 0.580 | [−0.092, 0.164] |
| Country: Greece † | 0.014 | 0.063 | 0.010 | 0.22 | 0.825 | [−0.110, 0.138] |
| Country: Poland † | 0.069 | 0.165 | 0.019 | 0.42 | 0.676 | [−0.256, 0.394] |
| Cluster | n | Age | Steps Completed | Progress Ratio | Time Spent (min) | Key Characteristics | ||||
|---|---|---|---|---|---|---|---|---|---|---|
| M | SD | M | SD | M | SD | M | SD | |||
| Comprehensive design assessors | 119 | 39.8 | 12.6 | 52.2 | 1.6 | 0.95 | 0.03 | 987.4 | 463.2 | Complete most/all modules |
| Initial design explorers | 178 | 38.1 | 14.9 | 4.5 | 3.8 | 0.08 | 0.07 | 65.3 | 52.8 | Disengage after initial exploration |
| Selective design evaluators | 40 | 37.9 | 13.5 | 29.3 | 7.1 | 0.53 | 0.13 | 384.6 | 159.7 | Complete specific topics of interest |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Gkintoni, E.; Magriplis, E.; Vantaraki, F.; Skoulidi, C.-M.; Anastassopoulos, P.; Cornea, A.; Inchaurraga, B.; Santurtun, J.; Mancha, A.d.l.C.; Giorgakis, G.; et al. Designing for Engagement in Primary Health Education Through Digital Game-Based Learning: Cross-National Behavioral Evidence from the iLearn4Health Platform. Behav. Sci. 2025, 15, 847. https://doi.org/10.3390/bs15070847
Gkintoni E, Magriplis E, Vantaraki F, Skoulidi C-M, Anastassopoulos P, Cornea A, Inchaurraga B, Santurtun J, Mancha AdlC, Giorgakis G, et al. Designing for Engagement in Primary Health Education Through Digital Game-Based Learning: Cross-National Behavioral Evidence from the iLearn4Health Platform. Behavioral Sciences. 2025; 15(7):847. https://doi.org/10.3390/bs15070847
Chicago/Turabian StyleGkintoni, Evgenia, Emmanuella Magriplis, Fedra Vantaraki, Charitini-Maria Skoulidi, Panagiotis Anastassopoulos, Alexandra Cornea, Begoña Inchaurraga, Jaione Santurtun, Ainhoa de la Cruz Mancha, George Giorgakis, and et al. 2025. "Designing for Engagement in Primary Health Education Through Digital Game-Based Learning: Cross-National Behavioral Evidence from the iLearn4Health Platform" Behavioral Sciences 15, no. 7: 847. https://doi.org/10.3390/bs15070847
APA StyleGkintoni, E., Magriplis, E., Vantaraki, F., Skoulidi, C.-M., Anastassopoulos, P., Cornea, A., Inchaurraga, B., Santurtun, J., Mancha, A. d. l. C., Giorgakis, G., Kouppas, K., Timotheou, S., Moreno Juan, M. J., Muñagorri, M., Harasiuk, M., Lopez, A. G., Skoulidi, E., & Vantarakis, A. (2025). Designing for Engagement in Primary Health Education Through Digital Game-Based Learning: Cross-National Behavioral Evidence from the iLearn4Health Platform. Behavioral Sciences, 15(7), 847. https://doi.org/10.3390/bs15070847