
Resurgence of Severe Challenging Behavior and Schedule Thinning with the Terminal Schedule Probe Method
 , and
, and
Abstract
1. Introduction
2. Methods
2.1. Participants, Setting, and Analytic Design
2.2. Response Definitions
2.3. Data Collection and Interobserver Agreement
2.4. General Procedures
2.4.1. Interpretation of Functional Analysis Data
2.4.2. Treatment
2.5. Terminal Schedule Probe Thinning
2.6. Dense-to-Lean Thinning
2.7. Resurgence Analysis
3. Results
3.1. Functional Analysis Outcomes
3.2. Treatment Evaluation
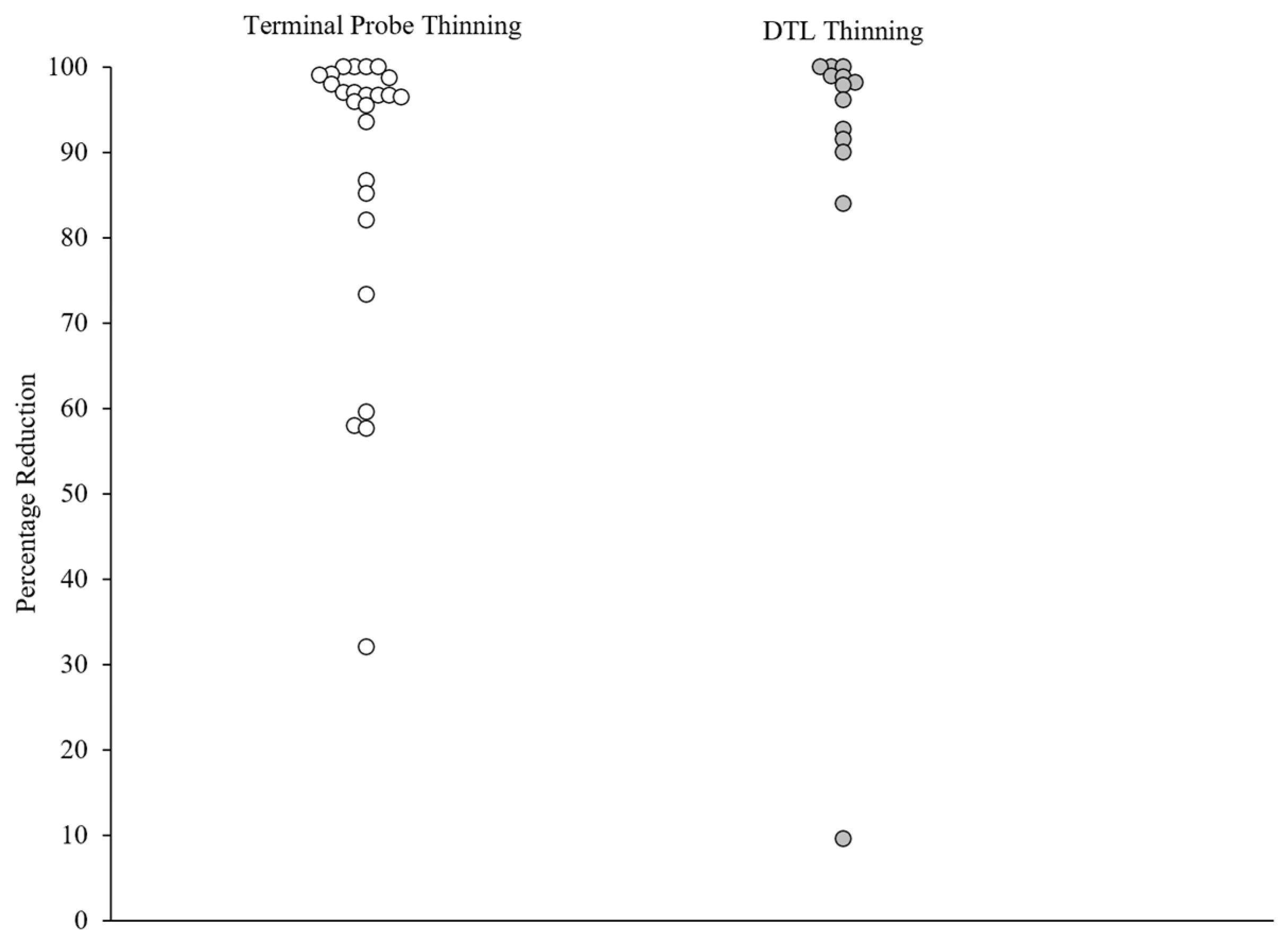
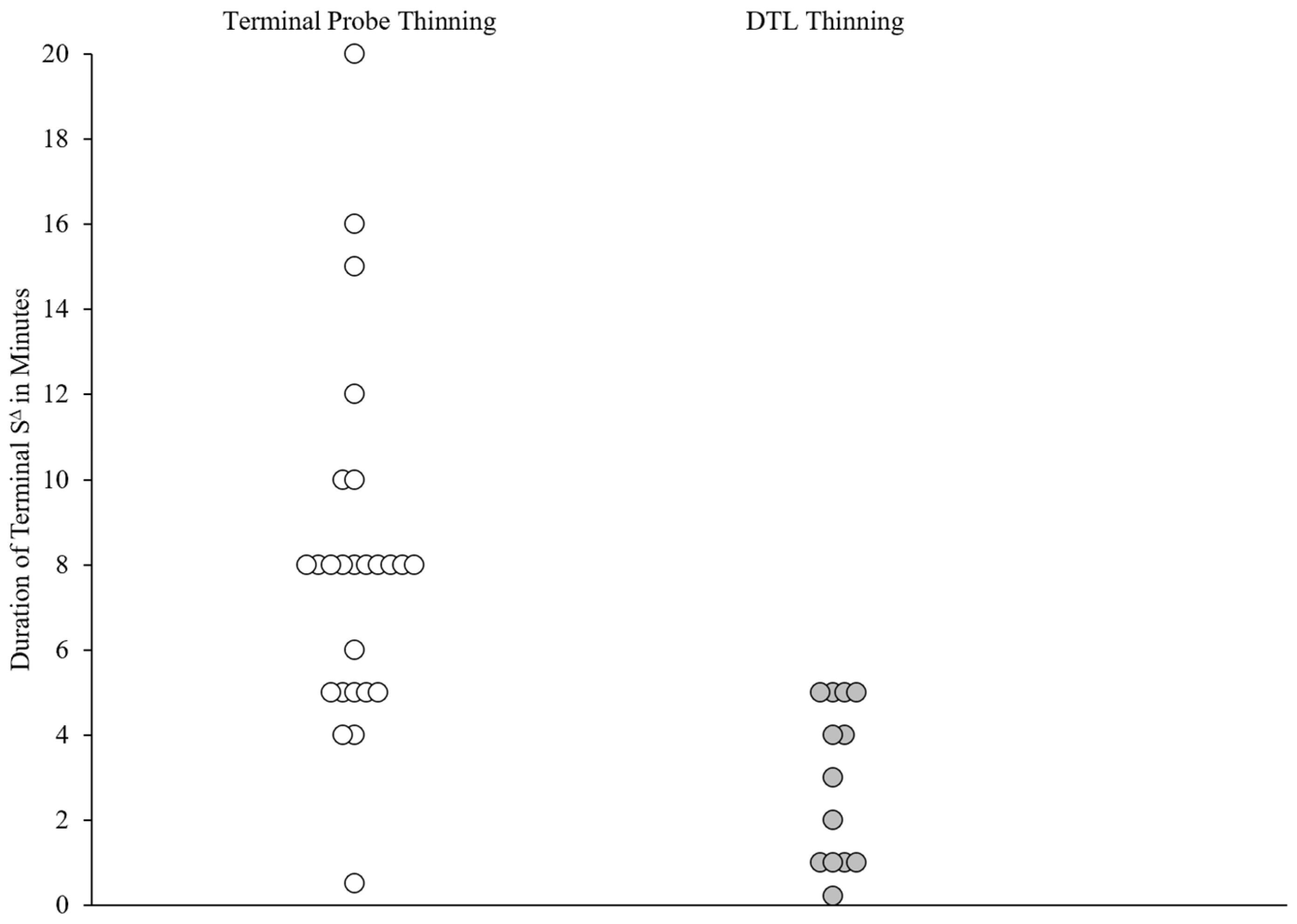
3.3. TP Thinning and DTL Thinning
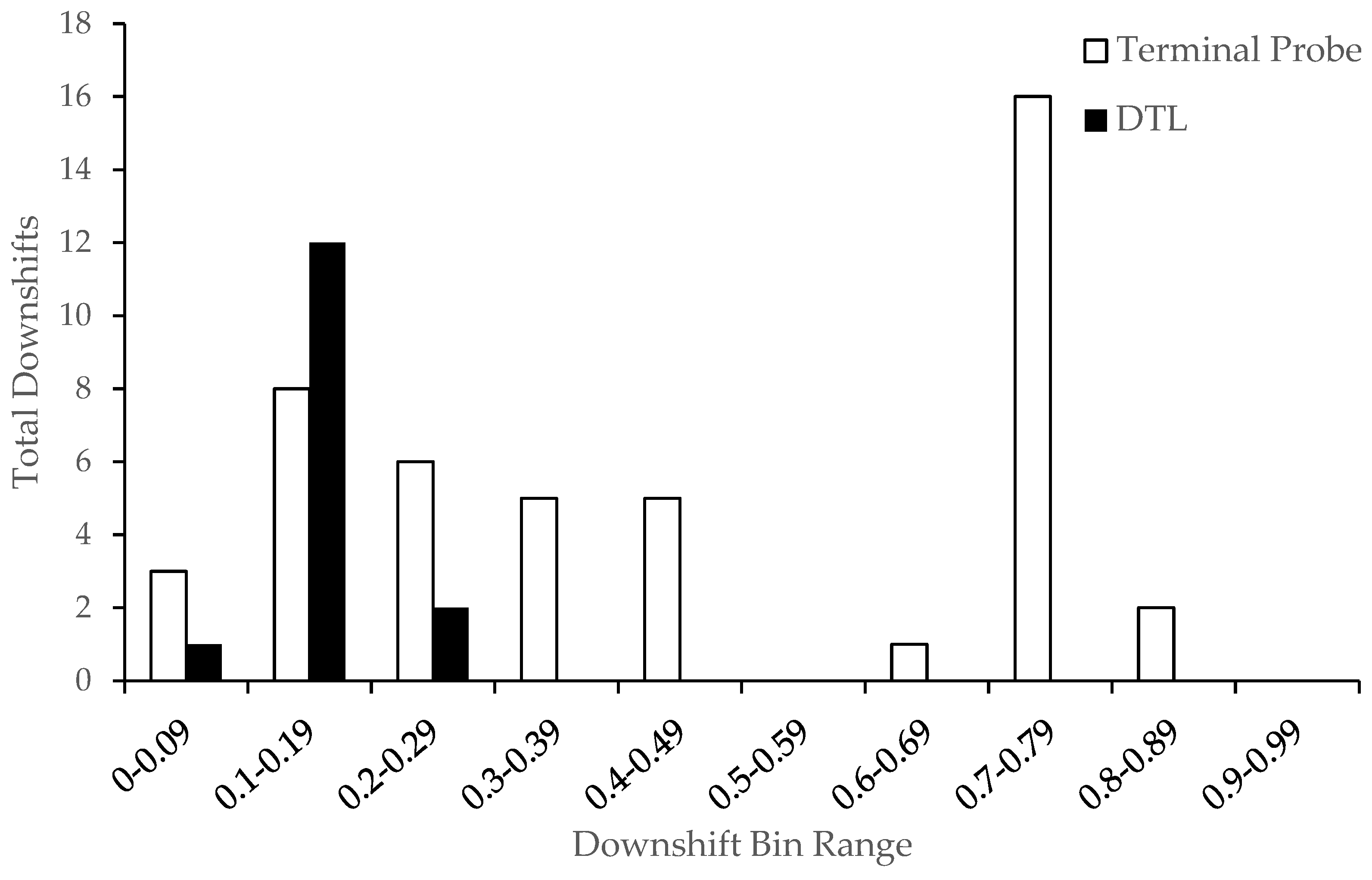
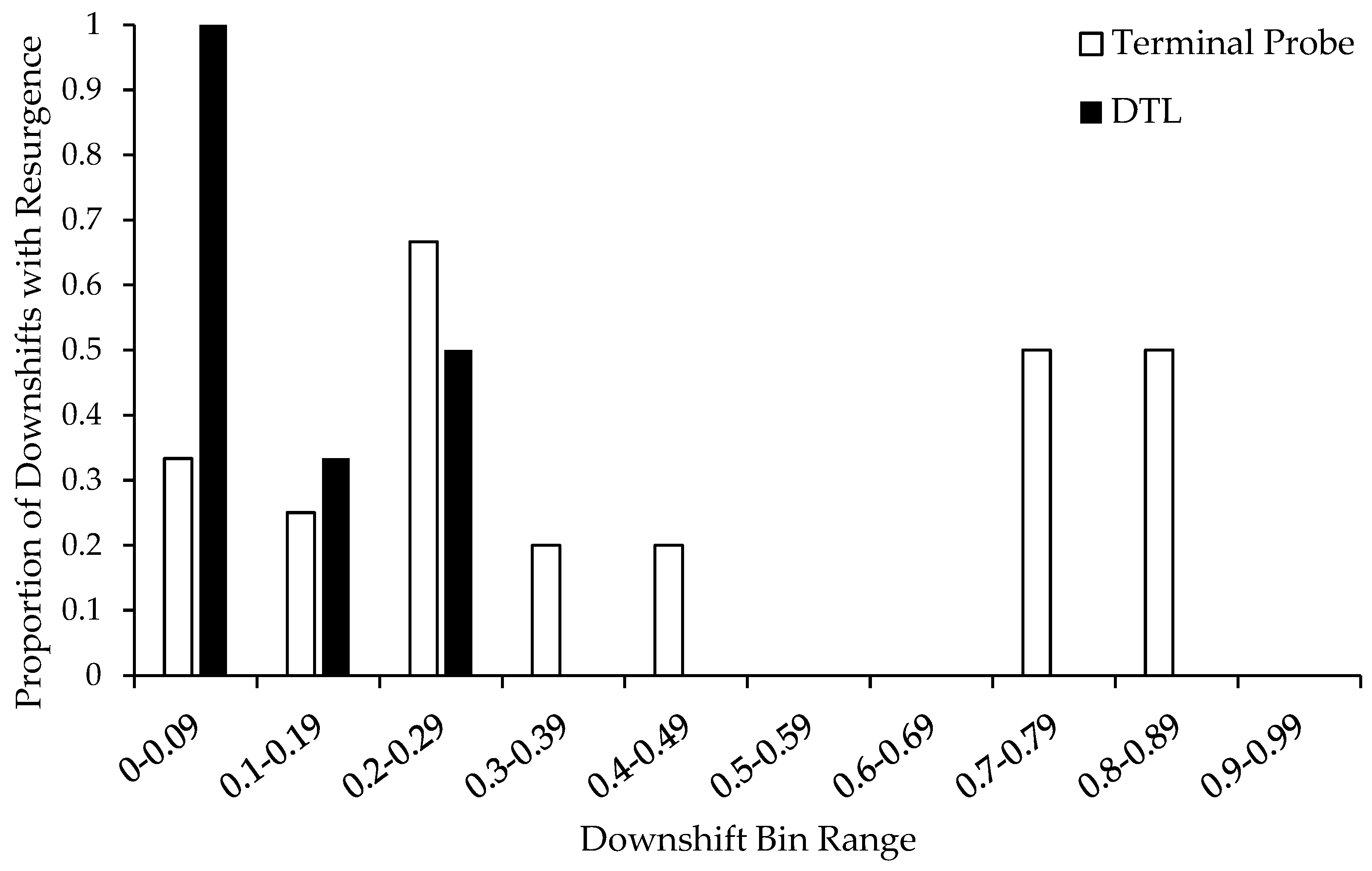
3.4. Resurgence Analysis Outcomes
4. Discussion
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Betz, A. M., Fisher, W. W., Roane, H. S., Mintz, J. C., & Owen, T. M. (2013). A component analysis of schedule thinning during functional communication training. Journal of Applied Behavior Analysis, 46(1), 219–241. [Google Scholar] [CrossRef] [PubMed]
- Bowman, L. G., Fisher, W. W., Thompson, R. H., & Piazza, C. C. (1997). On the relation of mands and the function of destructive behavior. Journal of Applied Behavior Analysis, 30(2), 251–265. [Google Scholar] [CrossRef]
- Briggs, A. M., Fisher, W. W., Greer, B. D., & Kimball, R. T. (2018). Prevalence of resurgence of destructive behavior when thinning reinforcement schedules during functional communication training. Journal of Applied Behavior Analysis, 51(3), 620–633. [Google Scholar] [CrossRef]
- Bullock, C. E., Fisher, W. W., & Hagopian, L. P. (2017). Description and validation of a computerized behavioral data program: “BDataPro”. The Behavior Analyst, 40, 275–285. [Google Scholar] [CrossRef]
- Carr, E. G., & Durand, V. M. (1985). Reducing behavior problems through functional communication training. Journal of Applied Behavior Analysis, 18(2), 111–126. [Google Scholar] [CrossRef] [PubMed]
- Cengher, M., O’Connor, J. T., & Strohmeier, C. W. (2022). Assessment and treatment of problem behavior maintained by escape from attention. Behavioral Interventions, 37(2), 204–221. [Google Scholar] [CrossRef]
- Chesbrough, E. A., King, H., Fornah, M., Quigley, S., & Falligant, J. M. (2024). Further analysis of fixed-lean approaches to reinforcement schedule thinning. Behavioral Interventions, 39(4), e2055. [Google Scholar] [CrossRef]
- Falligant, J. M., Chin, M. D., & Kurtz, P. F. (2022). Renewal and resurgence of severe problem behavior in an intensive outpatient setting: Prevalence, magnitude, and implications for practice. Behavioral Interventions, 37(3), 909–924. [Google Scholar] [CrossRef]
- Falligant, J. M., McNulty, M. K., Kranak, M. P., Hausman, N. L., & Rooker, G. W. (2020). Evaluating sources of baseline data using dual-criteria and conservative dual-criteria methods: A quantitative analysis. Journal of Applied Behavior Analysis, 53(4), 2330–2338. [Google Scholar] [CrossRef]
- Fisher, W. W., Greer, B. D., Fuhrman, A. M., & Querim, A. C. (2015). Using multiple schedules during functional communication training to promote rapid transfer of treatment effects. Journal of Applied Behavior Analysis, 48(4), 713–733. [Google Scholar] [CrossRef]
- Fisher, W. W., Piazza, C., Cataldo, M., Harrell, R., Jefferson, G., & Conner, R. (1993). Functional communication training with and without extinction and punishment. Journal of Applied Behavior Analysis, 26(1), 23–36. [Google Scholar] [CrossRef] [PubMed]
- Greer, B. D., & Shahan, T. A. (2019). Resurgence as Choice: Implications for promoting durable behavior change. Journal of Applied Behavior Analysis, 52(3), 816–846. [Google Scholar] [CrossRef]
- Greer, B. D., Shahan, T. A., Irwin Helvey, C., Fisher, W. W., Mitteer, D. R., & Fuhrman, A. M. (2024). Resurgence of destructive behavior following decreases in alternative reinforcement: A prospective analysis. Journal of Applied Behavior Analysis, 57, 599–614. [Google Scholar] [CrossRef]
- Hagopian, L. P. (2020). The consecutive controlled case series: Design, data-analytics, and reporting methods supporting the study of generality. Journal of Applied Behavior Analysis, 53(2), 596–619. [Google Scholar] [CrossRef]
- Hagopian, L. P., Boelter, E. W., & Jarmolowicz, D. P. (2011). Reinforcement schedule thinning following functional communication training: Review and recommendations. Behavior Analysis in Practice, 4, 4–16. [Google Scholar] [CrossRef]
- Hagopian, L. P., Bruzek, J. L., Bowman, L. G., & Jennett, H. K. (2007). Assessment and treatment of problem behavior occasioned by interruption of free-operant behavior. Journal of Applied Behavior Analysis, 40(1), 89–103. [Google Scholar] [CrossRef] [PubMed]
- Hagopian, L. P., Falligant, J. M., Frank-Crawford, M. A., Yenokyan, G., Piersma, D. E., & Kaur, J. (2023). Simplified methods for identifying subtypes of automatically maintained self-injury. Journal of Applied Behavior Analysis, 56(3), 575–592. [Google Scholar] [CrossRef] [PubMed]
- Hagopian, L. P., Fisher, W. W., Sullivan, M. T., Acquisto, J., & LeBlanc, L. A. (1998). Effectiveness of functional communication training with and without extinction and punishment: A summary of 21 inpatient cases. Journal of Applied Behavior Analysis, 31(2), 211–235. [Google Scholar] [CrossRef]
- Hagopian, L. P., Fisher, W. W., Thompson, R. H., Owen-DeSchryver, J., Iwata, B. A., & Wacker, D. P. (1997). Toward the development of structured criteria for interpretation of functional analysis data. Journal of Applied Behavior Analysis, 30(2), 313–326. [Google Scholar] [CrossRef]
- Hagopian, L. P., & Frank-Crawford, M. A. (2018). Classification of self-injurious behaviour across the continuum of relative environmental–biological influence. Journal of Intellectual Disability Research, 62(12), 1108–1113. [Google Scholar] [CrossRef]
- Hagopian, L. P., Kuhn, S. A. C., Long, E. S., & Rush, K. S. (2005). Schedule thinning following communication training: Using competing stimuli to enhance tolerance to decrements in reinforcer density. Journal of Applied Behavior Analysis, 38(2), 177–193. [Google Scholar] [CrossRef]
- Hagopian, L. P., Toole, L. M., Long, E. S., Bowman, L. G., & Lieving, G. A. (2004). A comparison of dense-to-lean and fixed lean schedules of alternative reinforcement and extinction. Journal of Applied Behavior Analysis, 37(3), 323–338. [Google Scholar] [CrossRef] [PubMed]
- Hanley, G. P., Iwata, B. A., & Thompson, R. H. (2001). Reinforcement schedule thinning following treatment with functional communication training. Journal of Applied Behavior Analysis, 34(1), 17–38. [Google Scholar] [CrossRef]
- Heyvaert, M., Saenen, L., Campbell, J. M., Maes, B., & Onghena, P. (2014). Efficacy of behavioral interventions for reducing problem behavior in persons with autism: An updated quantitative synthesis of single-subject research. Research in Developmental Disabilities, 35(10), 2463–2476. [Google Scholar] [CrossRef]
- Hill, A. P., Zuckerman, K. E., Hagen, A. D., Kriz, D. J., Duvall, S. W., Van Santen, J., Nigg, J., Fair, D., & Fombonne, E. (2014). Aggressive behavior problems in children with autism spectrum disorders: Prevalence and correlates in a large clinical sample. Research in Autism Spectrum Disorders, 8(9), 1121–1133. [Google Scholar] [CrossRef] [PubMed]
- Hurl, K., Wightman, J., Haynes, S. N., & Virues-Ortega, J. (2016). Does a pre-intervention functional assessment increase intervention effectiveness? A meta-analysis of within-subject interrupted time-series studies. Clinical Psychology Review, 47, 71–84. [Google Scholar] [CrossRef] [PubMed]
- Iwata, B. A., Dorsey, M. F., Slifer, K. J., Bauman, K. E., & Richman, G. S. (1994). Toward a functional analysis of self-injury. Journal of Applied Behavior Analysis, 27(2), 197–209, (Reprint from “Toward a functional analysis of self-injury,” 1982, Analysis and Intervention in Developmental Disabilities, 2[1], 3–20, https://doi.org/10.1016/0270-4684(82)90003-9). [Google Scholar] [CrossRef]
- Kranak, M. P., & Brown, K. R. (2024). Updated recommendations for reinforcement schedule thinning following functional communication training. Behavior Analysis in Practice, 17(1), 87–106. [Google Scholar] [CrossRef]
- Kranak, M. P., & Falligant, J. M. (2022). Analysis of terminal schedule probes and schedule thinning effects following functional communication training. Behavioral Interventions, 37(2), 323–333. [Google Scholar] [CrossRef]
- Kurtz, P. F., Boelter, E. W., Jarmolowicz, D. P., Chin, M. D., & Hagopian, L. P. (2011). An analysis of functional communication training as an empirically supported treatment for problem behavior displayed by individuals with intellectual disabilities. Research in Developmental Disabilities, 32(6), 2935–2942. [Google Scholar] [CrossRef]
- Kurtz, P. F., Strohmeier, C. W., Becraft, J. L., & Chin, M. D. (2021). Collateral effects of behavioral treatment for problem behavior on caregiver stress. Journal of Autism and Developmental Disorders, 51, 2852–2865. [Google Scholar] [CrossRef] [PubMed]
- Mandell, D. S. (2008). Psychiatric hospitalization among children with autism spectrum disorders. Journal of Autism and Developmental Disorders, 38, 1059–1065. [Google Scholar] [CrossRef]
- Melanson, I. J., & Fahmie, T. A. (2023). Functional analysis of problem behavior: A 40-year review. Journal of Applied Behavior Analysis, 56(2), 262–281. [Google Scholar] [CrossRef]
- Mitteer, D. R., Greer, B. D., Fisher, W. W., Briggs, A. M., & Wacker, D. P. (2018). A laboratory model for evaluating relapse of undesirable caregiver behavior. Journal of the Experimental Analysis of Behavior, 110(2), 252–266. [Google Scholar] [CrossRef] [PubMed]
- Muething, C., Pavlov, A., Call, N., Ringdahl, J., & Gillespie, S. (2021). Prevalence of resurgence during thinning of multiple schedules of reinforcement following functional communication training. Journal of Applied Behavior Analysis, 54(2), 813–823. [Google Scholar] [CrossRef]
- Muharib, R., & Wood, C. L. (2018). Evaluation of the empirical support of functional communication training for children with autism spectrum disorders. Review Journal of Autism and Developmental Disorders, 5, 360–369. [Google Scholar] [CrossRef]
- Newcomb, E. T., & Hagopian, L. P. (2018). Treatment of severe problem behaviour in children with autism spectrum disorder and intellectual disabilities. International Review of Psychiatry, 30(1), 96–109. [Google Scholar] [CrossRef]
- Podlesnik, C. A., Ritchey, C. M., Muething, C., & Falligant, J. M. (2024). Different criteria affect prevalence of relapse of behavior targeted for treatment. Journal of Applied Behavior Analysis, 58(1), 225–231. [Google Scholar] [CrossRef]
- Roane, H. S., Fisher, W., Kelley, M. E., Mevers, J. L., & Bouxsein, K. J. (2013). Using modified visual-inspection criteria to interpret functional analysis outcomes. Journal of Applied Behavior Analysis, 46(1), 130–146. [Google Scholar] [CrossRef]
- Rooker, G. W., Jessel, J., Kurtz, P. F., & Hagopian, L. P. (2013). Functional communication training with and without alternative reinforcement and punishment: An analysis of 58 applications. Journal of Applied Behavior Analysis, 46(4), 708–722. [Google Scholar] [CrossRef]
- Saini, V., Miller, S. A., & Fisher, W. W. (2016). Multiple schedules in practical application: Research trends and implications for future investigation. Journal of Applied Behavior Analysis, 49(2), 421–444. [Google Scholar] [CrossRef]
- Scheithauer, M., Schebell, S. M., Mevers, J. L., Martin, C. P., Noell, G., Suiter, K. C., & Call, N. A. (2020). A comparison of sources of baseline data for treatments of problem behavior following a functional analysis. Journal of Applied Behavior Analysis, 53(1), 102–120. [Google Scholar] [CrossRef]
- Shahan, T. A., Browning, K. O., Nist, A. N., & Sutton, G. M. (2020). Resurgence and downshifts in alternative reinforcement rate. Journal of the Experimental Analysis of Behavior, 114(2), 163–178. [Google Scholar] [CrossRef] [PubMed]
- Shahan, T. A., & Greer, B. D. (2021). Destructive behavior increases as a function of reductions in alternative reinforcement during schedule thinning: A retrospective quantitative analysis. Journal of the Experimental Analysis of Behavior, 116(2), 243–248. [Google Scholar] [CrossRef] [PubMed]
- Shahan, T. A., & Sweeney, M. M. (2011). A model of resurgence based on behavioral momentum theory. Journal of the Experimental Analysis of Behavior, 95(1), 91–108. [Google Scholar] [CrossRef] [PubMed]
- Storch, E. A., Arnold, E. B., Jones, A. M., Ale, C. M., Wood, J. J., Ehrenreich-May, J., Lewin, A. B., Mutch, P. J., & Murphy, T. K. (2012). The role of co-occurring disruptive behavior in the clinical presentation of children and adolescents with anxiety in the context of autism spectrum disorders. Child Psychiatry & Human Development, 43, 734–746. [Google Scholar] [CrossRef]
- Strohmeier, C. W., Cengher, M., Chin, M. D., & Falligant, J. M. (2024). Application of a terminal schedule probe method to inform schedule thinning with multiple schedules. Journal of Applied Behavior Analysis, 57(3), 676–694. [Google Scholar] [CrossRef]
- Tiger, J. H., Hanley, G. P., & Bruzek, J. (2008). Functional communication training: A review and practical guide. Behavior Analysis in Practice, 1, 16–23. [Google Scholar] [CrossRef]
- Ward-Horner, J., & Sturmey, P. (2012). Component analysis of behavior skills training in functional analysis. Behavioral Interventions, 27(2), 75–92. [Google Scholar] [CrossRef]
- Weber, J. K., Brown, K. R., Retzlaff, B. J., Hurd, A. M., Anderson, H. J., & Smallwood, K. (2024). Retrospective consecutive controlled case series of outcomes for functional analyses of severe destructive behavior. Journal of Applied Behavior Analysis, 57(3), 695–708. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Case | Age | Sex | Level of Functioning |
|---|---|---|---|
| 1 | 14 | M | Mild |
| 2 | 12 | M | Mild |
| 3 | 19 | F | Severe |
| 4 | 14 | M | Moderate |
| 5 | 14 | F | Mild |
| 6 | 12 | M | Severe |
| 7 | 9 | F | Mild |
| 8 | 14 | M | Severe |
| 9 | 11 | M | Severe |
| 10 | 15 | M | Severity unspecified |
| 11 | 11 | F | Moderate |
| 12 | 4 | M | Severe |
| 13 | 11 | F | Average |
| 14 | 7 | F | Severe |
| 15 | 8 | M | Severe |
| 16 | 13 | M | Severe |
| 17 | 9 | M | Severe |
| 18 | 8 | M | Average |
| 19 | 22 | M | Severe |
| 20 | 17 | F | Moderate |
| 21 | 5 | M | Developmental delay |
| 22 | 6 | M | Moderate |
| 23 | 13 | M | Moderate |
| 24 | 11 | M | Mild |
| Case | Age | Sex | Level of Functioning |
|---|---|---|---|
| 1 | 9 | M | Moderate |
| 2 | 9 | M | Moderate |
| 3 | 8 | F | Moderate |
| 4 | 8 | M | Moderate |
| 5 | 10 | M | Moderate |
| 6 | 13 | M | Mild |
| 7 | 8 | M | Severe |
| 8 | 13 | F | Moderate |
| 9 | 3 | F | Developmental delay |
| Case | Application | Treatment | Duration of Initial SΔ | Terminal Probe Duration | Derived SΔ | Duration of Final SΔ Achieved | Percentage of Session in SΔ | Percentage Reduction | Resurgence |
|---|---|---|---|---|---|---|---|---|---|
| 1 | 1 | Escape from Attn-Caregiver | 30 s | 8 min | 8 min | 8 min | 80% | 100% | N |
| 2 | 2 | Mands-Caregiver | 15 s | 8 min | 8 min | 20 min * | 67% | 100% | Y |
| 3 | 3 | Attention-Caregiver | 30 s | 8 min | 8 min | 16 min * | 80% | 96.39% | N |
| 4 | 4 | Interruption-Caregiver | 30 s | 8 min | 50 s | 5 min | 50% | 96.94% | Y |
| 5 | 5 | Escape | 30 s | 15 min | 15 min | 8 min | 67% | 96.91% | Y |
| 6 | 6 | Escape-Caregiver | 8 min | 8 min | 3 min 30 s | 8 min | 80% | 99.01% | N |
| 7 | 7 | Attention-Caregivers | 30 s | 8 min | 8 min | 10 min * | 80% | 93.56% | Y |
| 8 | 8 | Tangible-Caregiver | 30 s | 8 min | 8 min | 8 min | 80% | 100% | N |
| 9 | 9 | Tangible | 30 s | 5 min | 5 min | 5 min | 50% | 32% | Y |
| 10 | 10 | Tangible-Caregivers | 30 s | 8 min | 8 min | 8 min | 80% | 97.95% | Y |
| 11 | 11 | Tangible-Caregiver | 30 s | 3 min | 2 min 30 s | 30 s | 30% | 82.05% | Y |
| 12 | 12 | Escape-Caregivers | 30 s | 5 min | 5 min | 8 min * | 80% | 96.67% | N |
| 13 | 13 | Divided Attn-Caregivers | 30 s | 5min | 5 min | 5 min | 50% | 98.63% | Y |
| 14 | 14 | Tangible | 30 s | 8 min | 4 min | 4 min | 40% | 73.33% | Y |
| 15 | 15 | Tangible-Caregivers | 8 min | 8 min | 1 min | 6 min | 60% | 57.58% | Y |
| 16 | 16 | Tangible-Caregivers | 30 s | 5 min | 1 min | 5 min | 50% | 95.45% | Y |
| 16 | 17 | Divided Attn-Caregivers | 30 s | 5 min | 5 min | 5 min | 50% | 59.57% | N |
| 17 | 18 | Tangible-Caregivers | 30 s | 8 min | 50 s | 8 min | 80% | 96.67% | N |
| 18 | 19 | Interruption-Caregivers | 30 s | 8 min | 8 min | 15 min * | 78.95% | 86.67% | Y |
| 19 | 20 | Tangible-Caregiver | 30 s | 8 min | 1 min | 8 min | 80% | 96.67% | Y |
| 20 | 21 | Tangible-Caregiver | 30 s | 12 min | 7 min | 12 min | 80% | 99.07% | N |
| 21 | 22 | Tangible-Caregiver | 30 s | 4 min | 4 min | 4 min | 40% | 95.85% | Y |
| 22 | 23 | Tangible-Caregivers | 30 s | 8 min | 7 min | 8 min | 80% | 100% | Y |
| 23 | 24 | Attention-Caregivers | 30 s | 8 min | 8 min | 8 min | 80% | 85.11% | N |
| 24 | 25 | Divided Attn-Caregivers | 30 s | 10 min | 10 min | 10 min | 66.67% | 57.89% | N |
| Case | Application | Treatment | Duration of Initial SΔ | Duration of Final SΔ Achieved | Percentage of Session in SΔ | Percentage Reduction | Resurgence |
|---|---|---|---|---|---|---|---|
| 1 | 1 | Tangible-Caregiver | 15 s | 2 min | 20% | 92.68% | Y |
| 1 | 2 | Attention-Caregiver | 15 s | 1 min | 10% | 90% | Y |
| 1 | 3 | Tangible-Caregiver | 15 s | 1 min | 10% | 98.78% | Y |
| 1 | 4 | Attention-Caregiver | 15 s | 1 min | 10% | 98.96% | N |
| 2 | 5 | Tangible Edible | 15 s | 4 min | 40% | 96.08% | Y |
| 3 | 6 | Divided Attn | 15 s | 3 min | 30% | 9.52% | Y |
| 4 | 7 | Attention | 5 s | 5 min | 50% | 100% | Y |
| 5 | 8 | Escape from Attn | 30 s | 4 min | 40% | 84% | Y |
| 6 | 9 | Tangible | 15 s | 5 min | 50% | 91.52% | N |
| 7 | 10 | Tangible | 1 min 30 s | 5 min | 50% | 100% | Y |
| 8 | 11 | Tangible | 30 s | 5 min | 50% | 98.13% | Y |
| 9 | 12 | Tangible-Caregiver | 5 s | 30 s | 5% | 100% | N |
| 9 | 13 | Attention-Caregiver | 5 s | 10 s | 5% | 97.83% | N |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Strohmeier, C.W.; Thuman, E.; Falligant, J.M.; Cengher, M.; Chin, M.D.; Kurtz, P.F. Resurgence of Severe Challenging Behavior and Schedule Thinning with the Terminal Schedule Probe Method. Behav. Sci. 2025, 15, 382. https://doi.org/10.3390/bs15030382
Strohmeier CW, Thuman E, Falligant JM, Cengher M, Chin MD, Kurtz PF. Resurgence of Severe Challenging Behavior and Schedule Thinning with the Terminal Schedule Probe Method. Behavioral Sciences. 2025; 15(3):382. https://doi.org/10.3390/bs15030382
Chicago/Turabian StyleStrohmeier, Craig W., Elizabeth Thuman, John Michael Falligant, Mirela Cengher, Michelle D. Chin, and Patricia F. Kurtz. 2025. "Resurgence of Severe Challenging Behavior and Schedule Thinning with the Terminal Schedule Probe Method" Behavioral Sciences 15, no. 3: 382. https://doi.org/10.3390/bs15030382
APA StyleStrohmeier, C. W., Thuman, E., Falligant, J. M., Cengher, M., Chin, M. D., & Kurtz, P. F. (2025). Resurgence of Severe Challenging Behavior and Schedule Thinning with the Terminal Schedule Probe Method. Behavioral Sciences, 15(3), 382. https://doi.org/10.3390/bs15030382