The Impact of Nutrition Education, Strength Training, and Body Image Perception on Orthorexia Nervosa Risk: A Cross-Sectional Study in Women

 ,
, 
 , ,
, ,  , ,
, , 

Abstract
1. Introduction
1.1. Background and Definition of Orthorexia Nervosa
1.2. Diagnostic Classification and Challenges
1.3. Risk Factors, At-Risk Groups, and Body Image Concerns
1.4. Psychodynamic Perspectives on Orthorexia Nervosa
1.5. Research Gap, Objectives, and Hypothesis
2. Materials and Methods
2.1. Survey Design
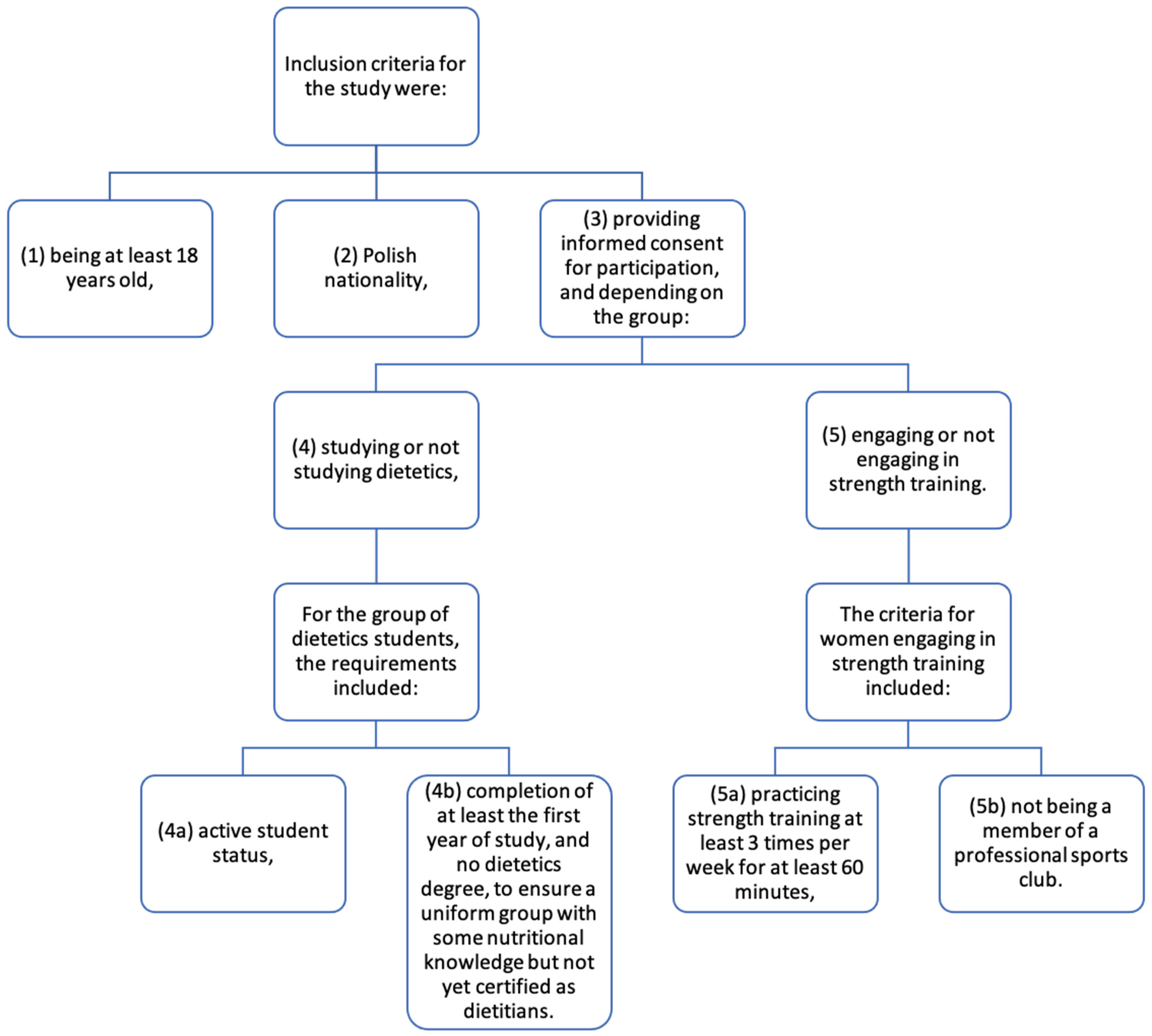
2.2. Study Participants
- SDNTS—dietetics students who do not engage in strength training (N = 46);
- SDTS—dietetics students who engage in strength training (N = 48);
- NDNTS—women who are not studying dietetics and do not engage in strength training (N = 50);
- NDTS—women who are not studying dietetics but engage in strength training (N = 46).
2.3. Research Tools
2.3.1. DOS
2.3.2. BESAA
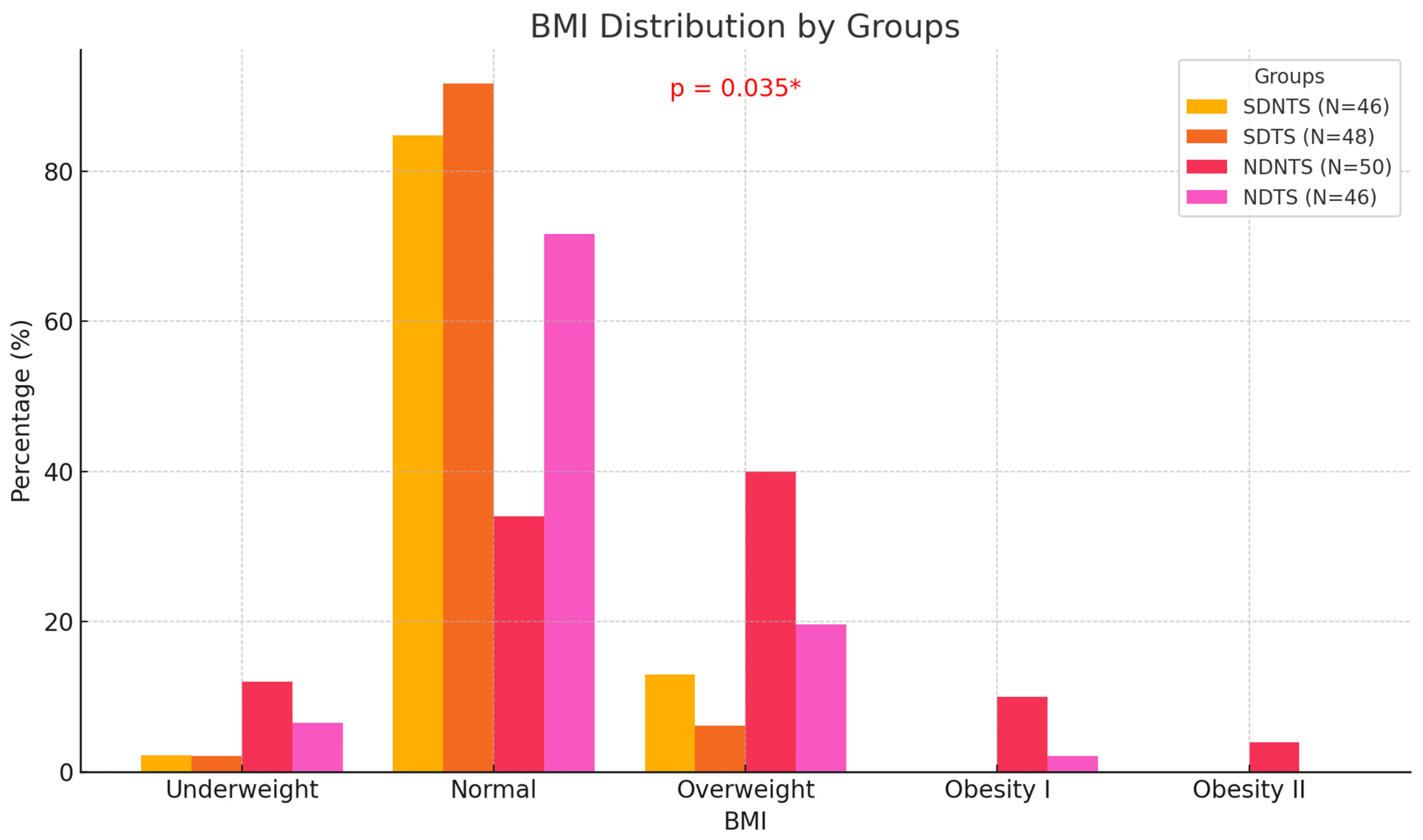
2.3.3. BMI (Body Mass Index)
2.3.4. Statistical Analysis
3. Results
- SDNTS—dietetics students not engaged in strength training (n = 46);
- SDTS—dietetics students engaged in strength training (n = 48);
- NDNTS—non-dietetics students not engaged in strength training (n = 50);
- NDTS—non-dietetics students engaged in strength training (n = 46).
3.1. Düsseldorf Orthorexia Scale (DOS-PL)
3.2. Body Self-Assessment Scale for Adolescents and Adults (BESAA)
3.3. Risk of ON and Assessment of One’s Own Body
4. Discussion
4.1. Key Findings and Group Comparisons
4.2. Social Media, Societal Influences, and Nutritional Status
4.3. Self-Esteem, Body Image, and Eating Behaviors
4.4. Theoretical Implications and Underlying Mechanisms
4.5. Practical Implications and Recommendations
4.6. Strengths and Limitations of the Study
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Barthels, F., Fischer, M., Keskini, R., Schöl, A. M., & Pietrowsky, R. (2024). The various facets of orthorexic eating behavior: Five case reports of individuals with supposed orthorexia nervosa. Journal of Eating Disorders, 12, 31. [Google Scholar] [CrossRef] [PubMed]
- Barthels, F., Meyer, F., & Pietrowsky, R. (2015). Die Düsseldorfer orthorexie skala–konstruktion und evaluation eines fragebogens zur erfassung ortho-rektischen ernährungsverhaltens. Zeitschrift für Klinische Psychologie und Psychotherapie, 44, 97–105. [Google Scholar] [CrossRef]
- Brytek-Matera, A. (2021). The Polish version of the Düsseldorf Orthorexia Scale (PL-DOS) and its comparison with the English version of the DOS (E-DOS). Eating and Weight Disorders, 26, 1223–1232. [Google Scholar] [CrossRef] [PubMed]
- Brytek-Matera, A., Donini, L. M., Krupa, M., Poggiogalle, E., & Hay, P. (2015). Orthorexia nervosa and self-attitudinal aspects of body image in female and male university students. Journal of Eating Disorders, 3(1), 2. [Google Scholar] [CrossRef] [PubMed]
- Bujarska, P., & Koza, W. (2020). Media społecznościowe a samoocena i sposób postrzegania własnego ciała u młodych użytkowniczek. In Seksualność i zdrowie psychiczne człowieka—Wyzwania współczesnej medycyny i społeczeństwa (p. 71). Wydawnictwo Naukowe. [Google Scholar]
- Cragun, D., DeBate, R. D., Ata, R. N., & Thompson, J. K. (2013). Psychometric properties of the Body Esteem Scale for Adolescents and Adults in an early adolescent sample. Eating and Weight Disorders-Studies on Anorexia, Bulimia and Obesity, 18, 275–282. [Google Scholar] [CrossRef] [PubMed]
- Dell’Osso, L., Carpita, B., Muti, D., Cremone, I. M., Massimetti, G., Diadema, E., & Carmassi, C. (2018). Prevalence and characteristics of orthorexia nervosa in a sample of university students in Italy. Eating and Weight Disorders-Studies on Anorexia, Bulimia and Obesity, 23, 55–65. [Google Scholar] [CrossRef] [PubMed]
- Donini, L. M., Barrada, J. R., Barthels, F., Dunn, T. M., Babeau, C., Brytek-Matera, A., Cena, H., Cerolini, S., Cho, H.-H., Coimbra, M., Cuzzolaro, M., Ferreira, C., Galfano, V., Grammatikopoulou, M. G., Hallit, S., Håman, L., Hay, P., Jimbo, M., Lasson, C., … Lombardo, C. (2022). A consensus document on definition and diagnostic criteria for orthorexia nervosa. Eating and Weight Disorders, 27, 3695–3711. [Google Scholar] [CrossRef] [PubMed]
- Dunn, T. M., & Bratman, S. (2016). On orthorexia nervosa: A review of the literature and proposed diagnostic criteria. Eating Behaviors, 21, 11–17. [Google Scholar] [CrossRef]
- Ephrem, C., Rizk, R., Saadeh, D., Hallit, S., Obeid, S., & Martijn, C. (2024). Orthorexia nervosa in dietitians and dietetics students—Prevalence, risk factors, and interventions: A scoping review using a systematic approach. Nutrition Reviews, 83(2), 382–396. [Google Scholar] [CrossRef]
- Gadsby, S. (2017). Distorted body representations in anorexia nervosa. Consciousness and Cognition, 51, 17–33. [Google Scholar] [CrossRef]
- Glashouwer, K. A., Van der Veer, R. M. L., Adipatria, F., De Jong, P. J., & Vocks, S. (2019). The role of body image disturbance in the onset, maintenance, and relapse of anorexia nervosa: A systematic review. Clinical Psychology Review, 74, 101771. [Google Scholar] [CrossRef]
- Gortat, M. (2021). Ortoreksja jako zagrożenie dla zdrowia i psychospołecznego funkcjonowania człowieka. Uniwersytet Medyczny w Lublinie. [Google Scholar]
- Grabe, S., Ward, L. M., & Hyde, J. S. (2008). The role of the media in body image concerns among women: A meta-analysis of experimental and correlational studies. Psychological Bulletin, 134(3), 460–476. [Google Scholar] [CrossRef]
- Gubiec, E., Stetkiewicz-Lewandowicz, A., Rasmus, P., & Sobów, T. (2015). Orthorexia in a group of dietetics students. Medycyna Ogólna i Nauki o Zdrowiu, 21(1), 95–100. [Google Scholar] [CrossRef]
- Hafstad, S. M., Bauer, J., Harris, A., & Pallesen, S. (2023). The prevalence of orthorexia in exercising populations: A systematic review and meta-analysis. Journal of Eating Disorders, 11, 15. [Google Scholar] [CrossRef] [PubMed]
- Jabłońska, E., Błądkowska, K., & Bronkowska, M. (2019). Zaburzenia odżywiania jako problem zdrowotny i psychospołeczny. Kosmos, 68(1), 121–132. [Google Scholar] [CrossRef]
- Jiotsa, B., Naccache, B., Duval, M., Rocher, B., & Grall-Bronnec, M. (2021). Social media use and body image disorders: Association between frequency of comparing one’s own physical appearance to that of people being followed on social media and body dissatisfaction and drive for thinness. International Journal of Environmental Research and Public Health, 18(6), 2880. [Google Scholar] [CrossRef] [PubMed]
- Kassier, S., & Veldman, F. (2014). Eating behavior, eating attitude and body mass index of dietetic students versus non-dietetic majors: A South African perspective. South African Journal of Clinical Nutrition, 27(3), 109–113. [Google Scholar] [CrossRef]
- Klocek, T. S., Witek, P., Wawrzonkowski, P., Binek, A., Woźniak, N., & Krzych, Ł. (2022). Styl życia studentów Śląskiego Uniwersytetu Medycznego w Katowicach w latach 2005 i 2020. Annales Academiae Medicae Silesiensis, 76, 112–117. [Google Scholar] [CrossRef]
- Krawczyk, P., & Święcicki, Ł. (2020). ICD-11 kontra ICD-10—A review of updates and novelties introduced in the latest version of the WHO International Classification of Diseases. Psychiatria Polska, 54(1), 7–20. [Google Scholar] [CrossRef] [PubMed]
- Mallaram, G. K., Sharma, P., Kattula, D., Singh, S., & Pavuluru, P. (2023). Body image perception, eating disorder behavior, self-esteem and quality of life: A cross-sectional study among female medical students. Journal of Eating Disorders, 11(1), 225. [Google Scholar] [CrossRef]
- Malmborg, J., Bremander, A., Olsson, M. C., & Bergman, S. (2017). Health status, physical activity, and orthorexia nervosa: A comparison between exercise science students and business students. Appetite, 109, 137–143. [Google Scholar] [CrossRef] [PubMed]
- Matusik, A., Grajek, M., Szlacheta, P., & Korzonek-Szlacheta, I. (2022). Comparison of the prevalence of eating disorders among dietetics students and students of other fields of study at selected universities (Silesia, Poland). Nutrients, 14(15), 3210. [Google Scholar] [CrossRef] [PubMed]
- Möllmann, A., Heinrichs, N., & Herwig, A. (2024). A conceptual framework on body representations and their relevance for mental disorders. Frontiers in Psychology, 14, 1231640. [Google Scholar] [CrossRef] [PubMed]
- Mróz, M. W., & Korek, E. (2020). Ortoreksja—Nowa jednostka chorobowa związana z zaburzonymi wzorcami odżywiania. Medycyna Ogólna i Nauki o Zdrowiu, 26(2), 102–105. [Google Scholar] [CrossRef]
- Polish Act on the Professions of Doctor and Dentist, of December 5, 1996. (1996). Dz.U. 2020 poz. 514. Available online: https://www.consciencelaws.org/law/laws/poland001.aspx (accessed on 12 December 2024).
- Rossi, A. A., Mannarini, S., Donini, L. M., Castelnuovo, G., Simpson, S., & Pietrabissa, G. (2024). Dieting, obsessive-compulsive thoughts, and orthorexia nervosa: Assessing the mediating role of worries about food through a structural equation model approach. Appetite, 193, 107164. [Google Scholar] [CrossRef] [PubMed]
- RSPH. (2024). #StatusOfMind. Royal society for public health. Available online: https://www.rsph.org.uk/our-work/campaigns/status-of-mind.html (accessed on 12 December 2024).
- Słomian, W., Wanot, B., & Kosior-Lara, A. (2020). Zdrowie a zaburzenia odżywiania. In Dieta a zdrowie i wiek (pp. 10–20). Wydawnictwo Naukowe Uniwersytetu Humanistyczno-Przyrodniczego im. Jana Długosza. [Google Scholar] [CrossRef]
- Słowińska, A. (2019). Skala Samooceny Ciała dla Adolescentów i Dorosłych (BESAA)—Polska adaptacja metody. Polish Journal of Applied Psychology, 17(1), 21–31. [Google Scholar]
- Song, H., Cai, Y., Cai, Q., Luo, W., Jiao, X., Jiang, T., & Liao, Y. (2023). Body image perception and satisfaction of junior high school students: Analysis of possible determinants. Children, 10(6), 1060. [Google Scholar] [CrossRef] [PubMed]
- Soohinda, G., Mishra, D., Sampath, H., & Dutta, S. (2019). Body dissatisfaction and its relation to Big Five personality factors and self-esteem in young adult college women in India. Indian Journal of Psychiatry, 61(4), 400–404. [Google Scholar] [CrossRef] [PubMed]
- Tokarz, A., Krupa, A. A., & Osmenda, E. (2014). Związki między typem motywacji, niezadowoleniem z własnego ciała a nastrojem u kobiet w trakcie aktywności fizycznej. Sport Humanities, 65, 10–20. [Google Scholar]
- Turner, P. G., & Lefevre, C. E. (2017). Instagram use is linked to increased symptoms of orthorexia nervosa. Eating and Weight Disorders-Studies on Anorexia, Bulimia and Obesity, 22(2), 277–284. [Google Scholar] [CrossRef] [PubMed]
- Valente, M., Renckens, S., Bunders-Aelen, J., & Syurina, E. V. (2022). The #orthorexia community on Instagram. Eating and Weight Disorders-Studies on Anorexia, Bulimia and Obesity, 27(2), 473–482. [Google Scholar] [CrossRef]
- Villa, M., Opawsky, N., Manriquez, S., Ananías, N., Vergara-Barra, P., & Leonario-Rodriguez, M. (2022). Orthorexia nervosa risk and associated factors among Chilean nutrition students: A pilot study. Journal of Eating Disorders, 10, 6. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization. (2019). Mean body mass index (BMI). Available online: https://www.who.int/data/gho/data/themes/topics/topic-details/GHO/body-mass-index (accessed on 9 August 2024).
- Zalewa, K., Kapłan, W., Rachwał, D., Bartoszek, L., Olszak, J., Rogowska, M., & Piątek, E. (2023). When does a healthy lifestyle turn into a disorder? Orthorexia—Diagnostic problems, methods of treatment. Journal of Education, Health and Sport, 33(1), 67–77. [Google Scholar] [CrossRef]


{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Variable | Group | X | SD | Min | Max | Med | Skew | Kurt | ε2 | p-Value |
|---|---|---|---|---|---|---|---|---|---|---|
| Age [Years] | Total (N = 190) | 23.93 | 5.80 | 18 | 54 | 23 | 3.45 | 12.0 | 0.00 | 0.970 |
| SDNTS (N = 46) | 22.67 | 1.44 | 20 | 27 | 23 | 0.56 | 1.12 | |||
| SDTS (N = 48) | 22.75 | 1.34 | 20 | 26 | 23 | −0.12 | 0.04 | |||
| NDNTS (N = 50) | 25.52 | 8.43 | 18 | 51 | 22 | 1.96 | 1.51 | |||
| NDTS (N = 46) | 24.71 | 7.31 | 18 | 54 | 23 | 2.93 | 8.44 | |||
| Body mass [kg] | Total (N = 190) | 63.03 | 9.82 | 42 | 100 | 62 | 0.80 | 1.37 | 0.04 | 0.126 |
| SDNTS (N = 46) | 61.28 | 7.12 | 48 | 80 | 60 | 0.46 | 0.18 | |||
| SDTS (N = 48) | 61.12 | 7.23 | 50 | 80 | 60 | 0.57 | 0.08 | |||
| NDNTS (N = 50) | 66.17 | 1.27 | 42 | 95 | 67 | 0.30 | −0.08 | |||
| NDTS (N = 46) | 63.34 | 1.02 | 46 | 100 | 65 | 0.35 | 2.32 | |||
| Height [cm] | Total (N = 190) | 166.02 | 5.77 | 150 | 185 | 166 | 0.15 | 0.17 | 0.02 | 0.415 |
| SDNTS (N = 46) | 166.21 | 6.29 | 150 | 178 | 166 | −0.30 | −0.22 | |||
| SDTS (N = 48) | 166.52 | 5.18 | 158 | 180 | 165 | 0.61 | −0.13 | |||
| NDNTS (N = 50) | 164.62 | 5.86 | 153 | 178 | 165 | 0.11 | −0.34 | |||
| NDTS (N = 46) | 166.84 | 5.64 | 155 | 185 | 167 | 0.58 | 1.60 | |||
| BMI [kg/m2] | Total (N = 190) | 22.85 | 3.37 | 16 | 37 | 22 | 1.13 | 0.35 | 0.05 | 0.031 * |
| SDNTS (N = 46) | 22.23 | 2.53 | 18 | 29 | 22 | 1.10 | 1.15 | |||
| SDTS (N = 48) | 21.95 | 1.77 | 18 | 27 | 22 | 0.33 | 0.38 | |||
| NDNTS (N = 50) | 24.42 | 4.7 | 16 | 37 | 24 | 0.47 | 0.15 | |||
| NDTS (N = 46) | 22.69 | 3.18 | 16 | 33 | 23 | 0.65 | 1.45 |
| Response | SDTS N (%) | NDTS N (%) | NDNTS N (%) | SDNTS N (%) | V-Cramer | p-Value |
|---|---|---|---|---|---|---|
| (N = 48) | (N = 46) | (N = 50) | (N = 46) | |||
| Eating healthy food is more important to me than the pleasure it brings. | ||||||
| Does not apply to me | 12 (25) | 18 (39.1) | 16 (32) | 15 (32.6) | 0.29 | <0.001 * |
| Somewhat applies to me | 27 (56.2) | 20 (43.5) | 8 (16) | 23 (50) | ||
| Definitely does not apply to me | 5 (10.4) | 3 (6.5) | 25 (50) | 4 (8.7) | ||
| Definitely applies to me | 4 (8.3) | 5 (10.9) | 1 (2) | 4 (8.7) | ||
| I have certain dietary rules that I follow. | ||||||
| Does not apply to me | 16 (33.3) | 20 (43.5) | 14 (28) | 32 (69.6) | 0.34 | <0.001 * |
| Somewhat applies to me | 27 (56.2) | 21 (45.6) | 8 (16) | 12 (26.1) | ||
| Definitely does not apply to me | 3 (6.2) | 0 (0) | 8 (16) | 1 (2.2) | ||
| Definitely applies to me | 2 (4.2) | 5 (10.9) | 20 (40) | 1 (2.2) | ||
| Eating only what is considered healthy gives me pleasure. | ||||||
| Does not apply to me | 5 (10.4) | 11 (23.9) | 21 (42) | 4 (8.7) | 0.29 | <0.001 * |
| Somewhat applies to me | 27 (56.2) | 11 (23.9) | 6 (12) | 11 (23.9) | ||
| Definitely does not apply to me | 16 (33.3) | 20 (43.5) | 21 (42) | 31 (67.4) | ||
| Definitely applies to me | 0 (0) | 4 (8.7) | 2 (4) | 0 (0) | ||
| I try to avoid being invited to dinner by friends if I know they don’t pay attention to healthy eating. | ||||||
| Does not apply to me | 9 (18.7) | 17 (40) | 39 (78) | 7 (15.2) | 0.34 | <0.001 * |
| Somewhat applies to me | 16 (33.3) | 16 (34.8) | 8 (16) | 28 (60.9) | ||
| Definitely does not apply to me | 20 (41.7) | 9 (19.6) | 3 (6) | 11 (23.9) | ||
| Definitely applies to me | 3 (6.2) | 4 (8.7) | 0 (0) | 0 (0) | ||
| I like that I pay more attention to healthy eating than others. | ||||||
| Does not apply to me | 10 (20.8) | 8 (17.4) | 4 (8) | 7 (15.2) | 0.38 | <0.001 * |
| Somewhat applies to me | 4 (8.3) | 16 (34.8) | 22 (44) | 5 (10.9) | ||
| Definitely does not apply to me | 4 (8.3) | 1 (2.2) | 20 (40) | 1 (2.2) | ||
| Definitely applies to me | 30 (62.5) | 21 (45.6) | 4 (8) | 33 (71.4) | ||
| I feel bad after eating something I consider unhealthy. | ||||||
| Does not apply to me | 5 (10.4) | 10 (21.7) | 22 (44) | 8 (17.4) | 0.27 | <0.001 * |
| Somewhat applies to me | 4 (8.3) | 6 (13) | 11 (22) | 0 (0) | ||
| Definitely does not apply to me | 36 (75) | 23 (50) | 12 (24) | 35 (76.1) | ||
| Definitely applies to me | 3 (6.2) | 7 (15.2) | 5 (10) | 3 (6.5) | ||
| I feel excluded from social circles due to my strict dietary rules. | ||||||
| Does not apply to me | 17 (35.4) | 22 (47.8) | 36 (72) | 8 (17.4) | 0.30 | <0.001 * |
| Somewhat applies to me | 19 (39.6) | 15 (32.6) | 14 (28) | 36 (78.3) | ||
| Definitely does not apply to me | 9 (18.7) | 7 (15.2) | 0 (0) | 2 (4.3) | ||
| Definitely applies to me | 3 (6.2) | 2 (4.3) | 0 (0) | 0 (0) | ||
| My thoughts constantly revolve around healthy eating and influence the organization of my day. | ||||||
| Does not apply to me | 7 (14.6) | 13 (28.3) | 36 (72) | 5 (10.9) | 0.40 | <0.001 * |
| Somewhat applies to me | 21 (43.7) | 14 (30.4) | 3 (6) | 2 (4.3) | ||
| Definitely does not apply to me | 17 (35.4) | 17 (37) | 9 (18) | 39 (84.8) | ||
| Definitely applies to me | 3 (6.2) | 2 (4.3) | 2 (4) | 0 (0) | ||
| It is hard for me to resist my dietary rules. | ||||||
| Does not apply to me | 5 (10.4) | 8 (17.4) | 14 (28) | 2 (4.3) | 0.24 | <0.001 * |
| Somewhat applies to me | 13 (27.1) | 16 (34.8) | 26 (52) | 17 (37) | ||
| Definitely does not apply to me | 30 (62.5) | 22 (47.8) | 8 (16) | 27 (58.7) | ||
| Definitely applies to me | 0 (0) | 0 (0) | 2 (4) | 0 (0) | ||
| I feel upset after eating unhealthy food. | ||||||
| Does not apply to me | 5 (10.4) | 10 (21.7) | 12 (24) | 1 (2.2) | 0.34 | <0.001 * |
| Somewhat applies to me | 33 (68.7) | 18 (39.1) | 3 (6) | 32 (69.6) | ||
| Definitely does not apply to me | 6 (12.5) | 14 (30.4) | 30 (60) | 6 (13) | ||
| Definitely applies to me | 4 (8.3) | 4 (8.7) | 5 (10) | 7 (15.2) | ||
| Variable | Group | X | SD | Min | Max | Med | ε2 | p-Value |
|---|---|---|---|---|---|---|---|---|
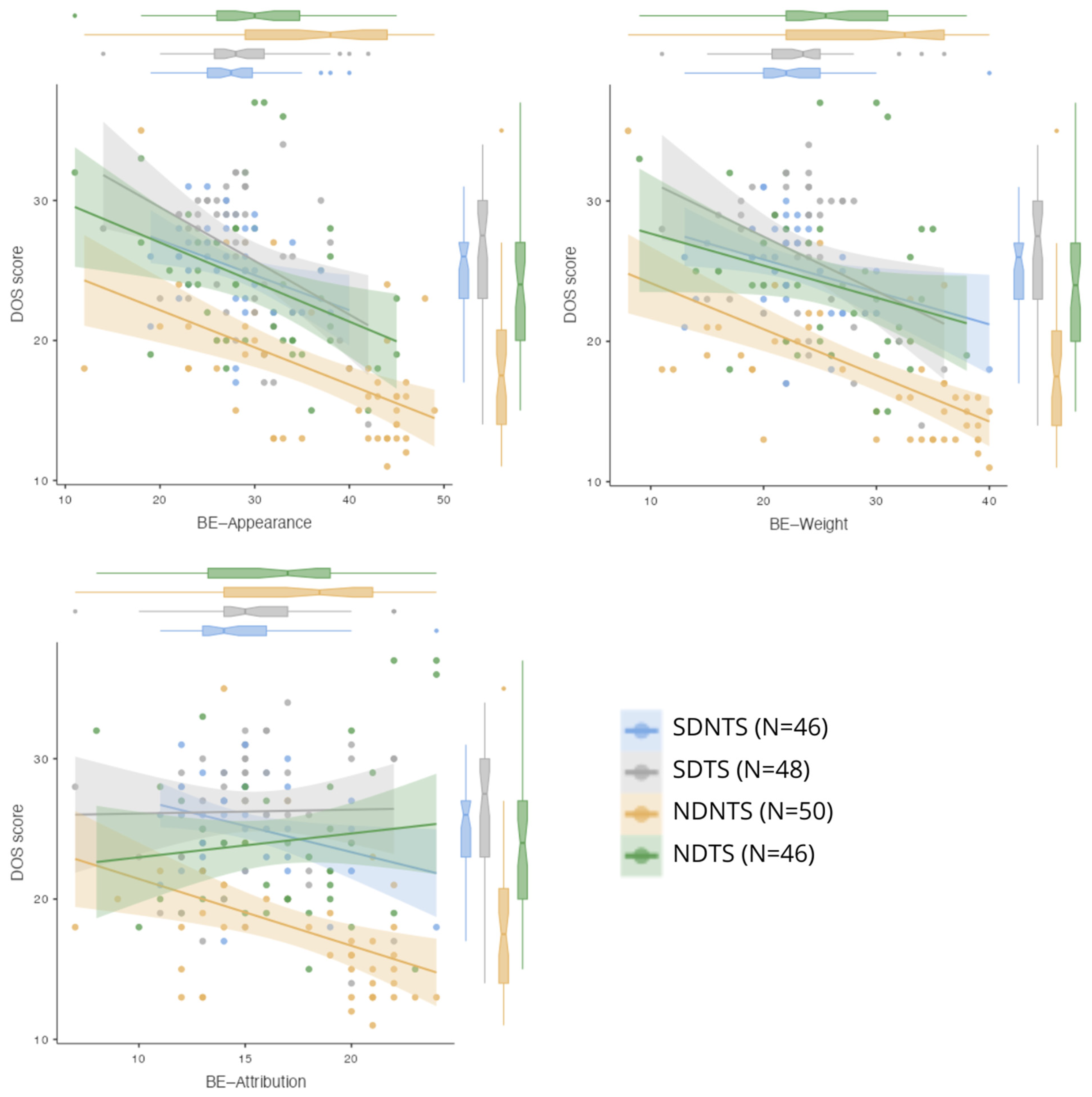
| BE—Appearance | Total (N = 190) | 30.7 | 7.6 | 11.0 | 49 | 29 | 0.14 | <0.001 * |
| SDNTS (N = 46) | 27.7 | 4.73 | 19 | 40 | 27.55 | |||
| SDTS (N = 48) | 28.5 | 5.21 | 14 | 42 | 28.0 | |||
| NDNTS (N = 50) | 35.9 | 9.48 | 12 | 49 | 38.0 | |||
| NDTS (N = 46) | 30.3 | 7.32 | 11 | 45 | 30.0 | |||
| BE—Weight | Total (N = 190) | 25.1 | 6.89 | 8.0 | 40 | 24 | 0.11 | <0.001 * |
| SDNTS (N = 46) | 22.6 | 4.68 | 13 | 40 | 22.0 | |||
| SDTS (N = 48) | 23.1 | 4.54 | 11 | 36 | 23.5 | |||
| NDNTS (N = 50) | 28.9 | 8.97 | 8 | 40 | 32.5 | |||
| NDTS (N = 46) | 25.7 | 6.42 | 9 | 38 | 25.5 | |||
| BE—Attribution | Total (N = 190) | 16.1 | 3.6 | 7.0 | 24 | 15 | 0.06 | 0.006 * |
| SDNTS (N = 46) | 14.9 | 2.79 | 11 | 24 | 14.0 | |||
| SDTS (N = 48) | 15.6 | 3.14 | 7 | 22 | 15.0 | |||
| NDNTS (N = 50) | 17.3 | 4.17 | 7 | 24 | 18.5 | |||
| NDTS (N = 46) | 16.5 | 3.79 | 8 | 24 | 17.0 |
| Model Coefficients—DOS Score; R = 0.693; R2 = 0.480 | |||||
|---|---|---|---|---|---|
| Predictor | Estimate | SE | t | p-Value | Standardized Estimate |
| Intercept | 31.727 | 1.5465 | 20.515 | <0.001 * | |
| BE—Appearance | −0.22 | 0.0853 | −2.575 | 0.011 * | −0.30 |
| BE—Weight | −0.158 | 0.0906 | −1.747 | 0.082 | −0.19 |
| BE—Attribution | 0.212 | 0.1042 | 2.039 | 0.043 * | 0.14 |
| Group: SDTS vs. SDNTS | 1.13 | 0.8585 | 1.317 | 0.190 | 0.20 |
| Group: NDNTS vs. SDNTS | −5.019 | 0.9196 | −5.458 | <0.001 * | −0.89 |
| Group: NDTS vs. SDNTS | −0.427 | 0.8821 | −0.484 | 0.629 | −0.08 |
| Model Coefficients—DOS Score; R = 0.676; R2 = 0.457 | |||||
|---|---|---|---|---|---|
| Predictor | Estimate | SE | t | p-Value | Standardized Estimate |
| Intercept | 28.409 | 1.7623 | 16.12 | <0.001 * | |
| BE—Appearance | −0.266 | 0.0851 | −3.13 | 0.002 * | −0.36 |
| BE—Weight | −0.135 | 0.0918 | −1.47 | 0.144 | −0.16 |
| BE—Attribution | 0.216 | 0.1061 | 2.04 | 0.043 * | 0.14 |
| Dietetics: | |||||
| Yes-No | 3.183 | 0.6532 | 4.87 | <0.001 * | 0.56 |
| Strength Training: | |||||
| Yes-No | 2.797 | 0.62269 | 4.46 | <0.001 * | 0.49 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Staśkiewicz-Bartecka, W.; Tambor, L.; Kiciak, A.; Dobkowska-Szefer, D.; Kuczka, N.; Białek-Dratwa, A.; Bielaszka, A.; Kowalski, O.; Kardas, M. The Impact of Nutrition Education, Strength Training, and Body Image Perception on Orthorexia Nervosa Risk: A Cross-Sectional Study in Women. Behav. Sci. 2025, 15, 199. https://doi.org/10.3390/bs15020199
Staśkiewicz-Bartecka W, Tambor L, Kiciak A, Dobkowska-Szefer D, Kuczka N, Białek-Dratwa A, Bielaszka A, Kowalski O, Kardas M. The Impact of Nutrition Education, Strength Training, and Body Image Perception on Orthorexia Nervosa Risk: A Cross-Sectional Study in Women. Behavioral Sciences. 2025; 15(2):199. https://doi.org/10.3390/bs15020199
Chicago/Turabian StyleStaśkiewicz-Bartecka, Wiktoria, Laura Tambor, Agata Kiciak, Daria Dobkowska-Szefer, Natalia Kuczka, Agnieszka Białek-Dratwa, Agnieszka Bielaszka, Oskar Kowalski, and Marek Kardas. 2025. "The Impact of Nutrition Education, Strength Training, and Body Image Perception on Orthorexia Nervosa Risk: A Cross-Sectional Study in Women" Behavioral Sciences 15, no. 2: 199. https://doi.org/10.3390/bs15020199
APA StyleStaśkiewicz-Bartecka, W., Tambor, L., Kiciak, A., Dobkowska-Szefer, D., Kuczka, N., Białek-Dratwa, A., Bielaszka, A., Kowalski, O., & Kardas, M. (2025). The Impact of Nutrition Education, Strength Training, and Body Image Perception on Orthorexia Nervosa Risk: A Cross-Sectional Study in Women. Behavioral Sciences, 15(2), 199. https://doi.org/10.3390/bs15020199