
Implications of Cash Transfer Programs for Mental Health Promotion among Families Facing Significant Stressors: Using Ecological Systems Theory to Explain Successes of Conditional and Unconditional Programs

{kind=link}
Abstract
1. Introduction
2. Implications of Cash Transfer Programs for Mental Health
2.1. Conditional Cash Transfer Programs
2.2. Unconditional Cash Transfer Programs
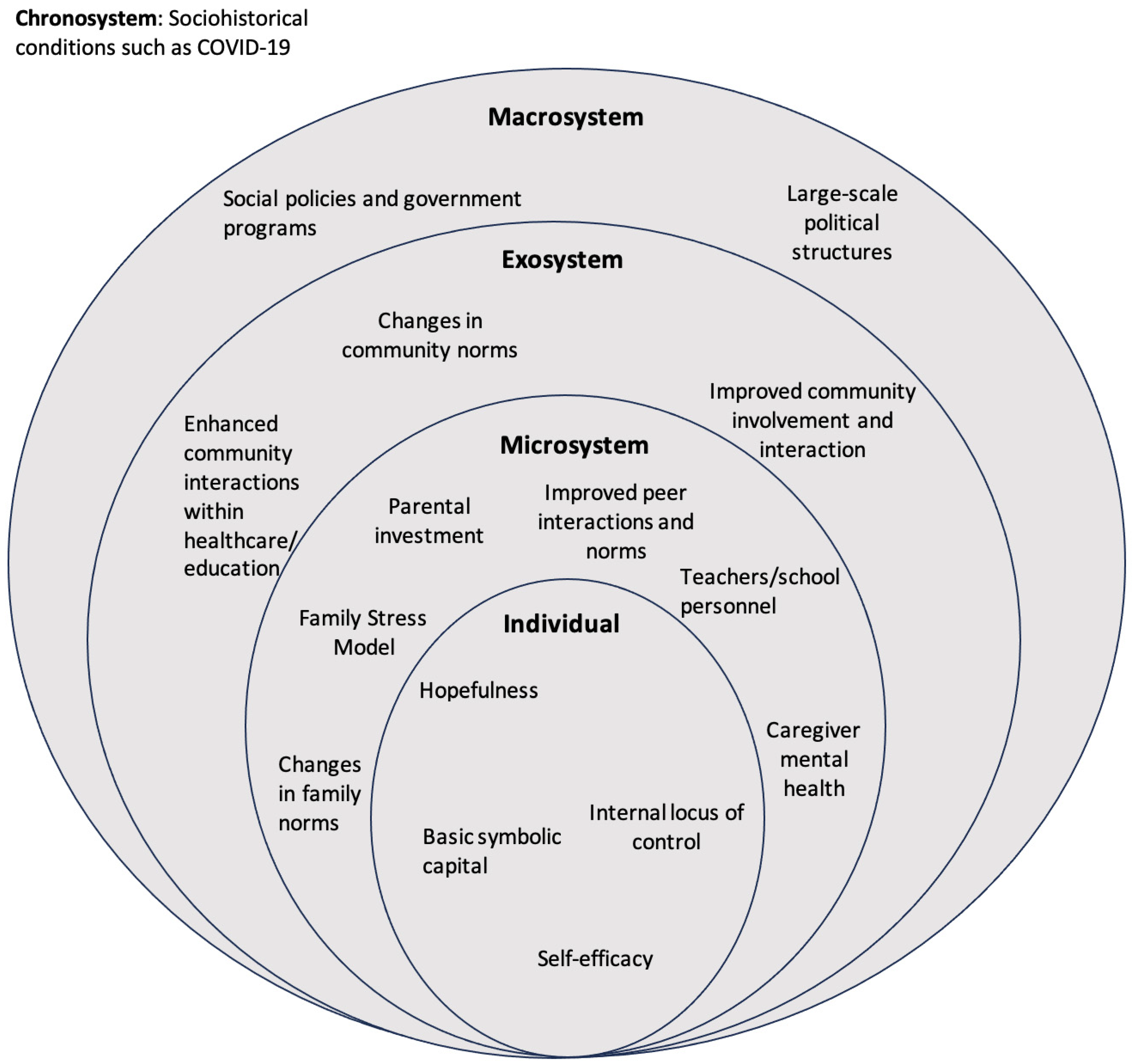
3. Applying Ecological Systems Theory to Child Development and Family Well-Being: Implications for Cash Transfer Programs
3.1. Individual Level
3.2. Microsystem
3.3. Exosystem and Macrosystem
4. A Need to Address Stigma and Consider Structural Factors
5. Overview and Summary
6. A Call for Transnational Research to Explore Connections between Cash Transfer Programs and Mental Health Outcomes among Families
6.1. Research Agenda
6.1.1. Line of Inquiry
6.1.2. Multi-Country Study
6.2. Policy Agenda
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Salmeron-Gomez, D.; Engilbertsdottir, S.; Antonio, J.; Leiva, C.; Newhouse, D.; Stewart, D. Global Trends in Child Monetary Poverty According to International Poverty Lines. 2023. Available online: https://www.unicef.org/mena/media/23631/file/Global%20trends%20in%20child%20monetary%20poverty.pdf (accessed on 22 August 2024).
- Reiss, F. Socioeconomic inequalities and mental health problems in children and adolescents: A systematic review. Soc. Sci. Med. 2013, 90, 24–31. [Google Scholar] [CrossRef]
- Tracy, M.; Zimmerman, F.J.; Galea, S.; McCauley, E.; Stoep, A.V. What explains the relation between family poverty and childhood depressive symptoms? J. Psychiatr. Res. 2008, 42, 1163–1175. [Google Scholar] [CrossRef]
- McLaughlin, K.A.; Breslau, J.; Green, J.G.; Lakoma, M.D.; Sampson, N.A.; Zaslavsky, A.M.; Kessler, R.C. Childhood socio-economic status and the onset, persistence, and severity of DSM-IV mental disorders in a US national sample. Soc. Sci. Med. 2011, 73, 1088–1096. [Google Scholar] [CrossRef]
- Hatcher, A.M.; Gibbs, A.; Jewkes, R.; McBride, R.S.; Peacock, D.; Christofides, N. Effect of childhood poverty and trauma on adult depressive symptoms among young men in peri-urban South African settlements. J. Adolesc. Health 2019, 64, 79–85. [Google Scholar] [CrossRef] [PubMed]
- Evans, G.W.; De France, K. Childhood poverty and psychological well-being: The mediating role of cumulative risk exposure. Dev. Psychopathol. 2022, 34, 911–921. [Google Scholar] [CrossRef] [PubMed]
- Lee, K.; Zhang, L. Cumulative effects of poverty on children’s social-emotional development: Absolute poverty and relative poverty. Community Ment. Health J. 2022, 58, 930–943. [Google Scholar] [CrossRef]
- Wolf, K.; Schmitz, J. Scoping review: Longitudinal effects of the COVID-19 pandemic on child and adolescent mental health. Eur. Child Adolesc. Psychiatry 2023, 33, 1257–1312. [Google Scholar] [CrossRef]
- Fegert, J.M.; Vitiello, B.; Plener, P.L.; Clemens, V. Challenges and burden of the Coronavirus 2019 (COVID-19) pandemic for child and adolescent mental health: A narrative review to highlight clinical and research needs in the acute phase and the long return to normality. Child Adolesc. Psychiatry Ment. Health 2020, 14, 20. [Google Scholar] [CrossRef] [PubMed]
- Santabárbara, J.; Lasheras, I.; Lipnicki, D.M.; Bueno-Notivol, J.; Pérez-Moreno, M.; López-Antón, R.; De la Cámara, C.; Lobo, A.; Gracia-García, P. Prevalence of anxiety in the COVID-19 pandemic: An updated meta-analysis of community-based studies. Prog. Neuropsychopharmacol. Biol. Psychiatry 2021, 109, 110207. [Google Scholar] [CrossRef]
- Hoagwood, K.E.; Kelleher, K.J. A marshall plan for children’s mental health after COVID-19. Psychiatr. Serv. 2020, 71, 1216–1217. [Google Scholar] [CrossRef]
- de Figueiredo, C.S.; Sandre, P.C.; Portugal, L.C.L.; Mázala-De-Oliveira, T.; da Silva Chagas, L.; Raony, Í.; Ferreira, E.S.; Giestal-De-Araujo, E.; dos Santos, A.A.; Bomfim, P.O.-S. COVID-19 pandemic impact on children and adolescents’ mental health: Biological, environmental, and social factors. Prog. Neuropsychopharmacol. Biol. Psychiatry 2021, 106, 110171. [Google Scholar] [CrossRef] [PubMed]
- Conger, R.D.; Conger, K.J. Resilience in midwestern families: Selected findings from the first decade of a prospective, longitudinal study. J. Marriage Fam. 2002, 64, 361–373. [Google Scholar] [CrossRef]
- Engle, P.L.; Black, M.M. The effect of poverty on child development and educational outcomes. Ann. N. Y. Acad. Sci. 2008, 1136, 243–256. [Google Scholar] [CrossRef] [PubMed]
- Clauss-Ehlers, C.S. In search of an evidence-based approach to understand and promote effective parenting practices. Couple Fam. Psychol. Res. Pract. 2017, 6, 135–153. [Google Scholar] [CrossRef]
- Wolfe, B.L.; Haveman, R. The determinants of Children Attainments: A Review of Methods and Findings. J. Econ. Lit. 1995, 33, 1829–1878. Available online: https://www.researchgate.net/publication/4901914 (accessed on 22 August 2024).
- Davis-Kean, P.E. The influence of parent education and family income on child achievement: The indirect role of parental expectations and the home environment. J. Fam. Psychol. 2005, 19, 294–304. [Google Scholar] [CrossRef]
- Bauer, A.; Baltra, R.A.; Pabon, M.A.; Díaz, Y.; Garman, E.; Hessel, P.; Lund, C.; Malvasi, P.; Matijasevich, A.; McDaid, D.; et al. Examining the dynamics between young people’s mental health, poverty and life chances in six low- and middle-income countries: Protocol for the CHANCES-6 study. Soc. Psychiatry Psychiatr. Epidemiol. 2021, 56, 1687–1703. [Google Scholar] [CrossRef]
- Thompson, H. Cash transfer programs can promote child protection outcomes. Child. Abus. Negl. 2014, 38, 360–371. [Google Scholar] [CrossRef]
- Arnold, C.; Conway, T.; Greenslade, M. Cash Transfers: Evidence Paper; Department for International Development: London, UK, 2011; Available online: https://gsdrc.org/document-library/cash-transfers-evidence-paper/ (accessed on 22 August 2024).
- Wolf, S.; Aber, L.J.; Morris, P.A. Drawing on psychological theory to understand and improve antipoverty policies: The case of conditional cash transfers. Psychol. Public Policy Law 2013, 19, 3–14. [Google Scholar] [CrossRef]
- Palomar-Lever, J.; Victorio-Estrada, A. Determinants of subjective well-being in adolescent children of recipients of the oportunidades human development program in Mexico. Soc. Indic. Res. 2014, 118, 103–124. [Google Scholar] [CrossRef]
- Hunter, W.; Patel, L.; Sugiyama, N.B. How family and child cash transfers can empower women: Comparative lessons from Brazil and South Africa. Glob. Soc. Policy 2021, 21, 258–277. [Google Scholar] [CrossRef]
- Neufeld, L.M. The Oportunidades Program and child growth: Mexico perspectives. In Handbook of Growth and Growth Monitoring in Health and Disease; Springer: Berlin/Heidelberg, Germany, 2011; pp. 1659–1671. [Google Scholar] [CrossRef]
- Neves, J.A.; de Vasconcelos, F.d.A.C.; Machado, M.L.; Recine, E.; Garcia, G.S.; de Medeiros, M.A.T. The Brazilian cash transfer program (Bolsa Família): A tool for reducing inequalities and achieving social rights in Brazil. Glob. Public. Health 2022, 17, 26–42. [Google Scholar] [CrossRef]
- Fernald, L.C.; Gertler, P.J.; Neufeld, L.M. Role of cash in conditional cash transfer programmes for child health, growth, and development: An analysis of Mexico’s Oportunidades. Lance 2008, 371, 828–837. [Google Scholar] [CrossRef]
- Ozer, E.J.; Fernald, L.C.H.; Manley, J.G.; Gertler, P.J. Effects of a conditional cash transfer program on children’s behavior problems. Pediatrics 2009, 123, e630–e637. [Google Scholar] [CrossRef]
- Fernald, L.C.H.; Gunnar, M.R. Poverty-alleviation program participation and salivary cortisol in very low-income children. Soc. Sci. Med. 2009, 68, 2180–2189. [Google Scholar] [CrossRef] [PubMed]
- Ozer, E.J.; Fernald, L.C.H.; Weber, A.; Flynn, E.P.; VanderWeele, T.J. Does alleviating poverty affect mothers’ depressive symptoms? A quasi-experimental investigation of Mexico’s Oportunidades programme. Int. J. Epidemiol. 2011, 40, 1565–1576. [Google Scholar] [CrossRef] [PubMed]
- Ziebold, C.; Paula, C.S.; Santos, I.S.; Barros, F.C.; Munhoz, T.N.; Lund, C.; McDaid, D.; Araya, R.; Bauer, A.; Garman, E.; et al. Conditional cash transfers and adolescent mental health in Brazil: Evidence from the 2004 Pelotas Birth Cohort. J. Glob Health 2021, 11, 04066. [Google Scholar] [CrossRef] [PubMed]
- Prencipe, L.; Houweling, T.A.J.; van Lenthe, F.J.; Palermo, T. Do conditional cash transfers improve mental health? Evidence from Tanzania’s governmental social protection program. J. Adolesc. Health 2021, 69, 797–805. [Google Scholar] [CrossRef]
- Riccio, J.A.; Dechausay, N.; Greenberg, D.M.; Miller, C.; Rucks, Z.; Verma, N. Findings from New York City’s Conditional Cash Transfer Program; MDRC: New York, NY, USA, 2010; Available online: https://ssrn.com/abstract=1786981 (accessed on 22 August 2024).
- Morris, P.A.; Aber, J.L.; Wolf, S.; Berg, J. Impacts of family rewards on adolescents’ mental health and problem behavior: Understanding the full range of effects of a conditional cash transfer program. Prev. Sci. 2017, 18, 326–336. [Google Scholar] [CrossRef]
- Zaneva, M.; Guzman-Holst, C. Reeves, and L. Bowes. The impact of monetary poverty alleviation programs on children’s and adolescents’ mental health: A systematic review and meta-analysis across low-, middle-, and high-income countries. J. Adolesc. Health 2022, 71, 147–156. [Google Scholar] [CrossRef]
- Powell-Jackson, T.; Pereira, S.K.; Dutt, V.; Tougher, S.; Haldar, K.; Kumar, P. Cash transfers, maternal depression and emotional well-being: Quasi-experimental evidence from India’s Janani Suraksha Yojana programme. Soc. Sci. Med. 2016, 162, 210–218. [Google Scholar] [CrossRef] [PubMed]
- Ohrnberger, J.; Anselmi, L.; Fichera, E.; Sutton, M. The effect of cash transfers on mental health: Opening the black box—A study from South Africa. Soc. Sci. Med. 2020, 260, 113181. [Google Scholar] [CrossRef] [PubMed]
- Fernald, L.C.H.; Hidrobo, M. Effect of Ecuador’s cash transfer program (Bono de Desarrollo Humano) on child development in infants and toddlers: A randomized effectiveness trial. Soc. Sci. Med. 2011, 72, 1437–1446. [Google Scholar] [CrossRef] [PubMed]
- Natali, L.; Handa, S.; Peterman, A.; Seidenfeld, D.; Tembo, G. Does money buy happiness? Evidence from an unconditional cash transfer in Zambia. SSM Popul. Health 2018, 4, 225–235. [Google Scholar] [CrossRef] [PubMed]
- Rojas, N.M.; Yoshikawa, H.; Gennetian, L.; Lemus Rangel, M.; Melvin, S.; Noble, K.; Duncan, G.; Magunson, K. Exploring the experiences and dynamics of an unconditional cash transfer for low-income mothers: A mixed-methods study. J. Child. Poverty 2020, 26, 64–84. [Google Scholar] [CrossRef]
- de Walque, D.; Fernald, L.; Gertler, P.; Hidrobo, M. Cash transfers and child and adolescent development. In Child and Adolescent Health and Development Disease Control Priorities, 3rd ed.; Bundy, D.A.P., de Silva, N., Horton, S., Jamison, D.T., Patton, G.C., Eds.; World Bank: Washington, DC, USA, 2017; Volume 8, pp. 325–342. [Google Scholar] [CrossRef]
- Angeles, G.; de Hoop, J.; Handa, S.; Kilburn, K.; Milazzo, A.; Peterman, A. Government of Malawi’s unconditional cash transfer improves youth mental health. Soc. Sci. Med. 2019, 225, 108–119. [Google Scholar] [CrossRef]
- Kilburn, K.; Thirumurthy, H.; Halpern, C.T.; Pettifor, A.; Handa, S. Effects of a large-scale unconditional cash transfer program on mental health outcomes of young people in Kenya. J. Adolesc. Health 2016, 58, 223–229. [Google Scholar] [CrossRef]
- Marr, C.; Cox, K.; Hingtgen, S.; Windham, K.; Sherman, A. American Rescue Plan Act includes Critical Expansions of Child Tax Credit and EITC; Center on Budget and Policy Priorities: Washington, DC, USA, 2021; Available online: https://www.cbpp.org/research/federal-tax/american-rescue-plan-act-includes-critical-expansions-of-child-tax-credit-and (accessed on 22 August 2024).
- Goldin, J.; Michelmore, K. Who benefits from the child tax credit? Natl. Tax. J. 2022, 75, 123–147. [Google Scholar] [CrossRef]
- Glasner, B.; Jiménez-Solomon, O.; Collyer, S.M.; Garfinkel, I.; Wimer, C.T. No evidence the Child Tax Credit expansion had An effect on the well-being and mental health of parents. Health Aff. 2022, 41, 1607–1615. [Google Scholar] [CrossRef]
- Batra, A.; Jackson, K.; Hamad, R. Effects of the 2021 Expanded Child Tax Credit on adults’ mental health: A quasi-experimental study. Health Aff. 2023, 42, 74–82. [Google Scholar] [CrossRef]
- Kovski, N.; Pilkauskas, N.V.; Michelmore, K.; Shaefer, H.L. Unconditional cash transfers and mental health symptoms among parents with low incomes: Evidence from the 2021 child tax credit. SSM Popul. Health 2021, 22, 101420. [Google Scholar] [CrossRef] [PubMed]
- Collyer, S.; Gandhi, J.; Garfinkel, I.; Ross, S.; Waldfogel, J.; Wimer, C. The Effects of the 2021 Monthly Child Tax Credit on Child and Family Well-Being: Evidence from New York City. Socius 2022, 8, 23780231221141165. [Google Scholar] [CrossRef]
- Kauhanen, L.; Yunus, W.M.A.W.M.; Lempinen, L.; Peltonen, K.; Gyllenberg, D.; Mishina, K.; Gilbert, S.; Bastola, K.; Brown, J.S.L.; Sourander, A. A systematic review of the mental health changes of children and young people before and during the COVID-19 pandemic. Eur. Child. Adolesc. Psychiatry 2023, 32, 995–1013. [Google Scholar] [CrossRef] [PubMed]
- Clauss-Ehlers, C.S.; Sood, A.B.; Weist, M.D. Social Justice for Children and Young People: International Perspectives; Cambridge University Press: Cambridge, UK, 2020. [Google Scholar]
- Adato, M.; Devereux, S.; Sabates-Wheeler, R. Accessing the ‘Right’ Kinds of Material and Symbolic Capital: The Role of Cash Transfers in Reducing Adolescent School Absence and Risky Behaviour in South Africa. J. Dev. Stud. 2016, 52, 1132–1146. [Google Scholar] [CrossRef]
- Bourdieu, P. The forms of capital. In Handbook of Theory and Research for the Sociology of Education; Richardson, J., Ed.; Greenwood: New York, NY, USA, 1986; pp. 241–258. [Google Scholar]
- Heinrich, C.; Hoddinott, J. Reducing adolescent risky behaviors in a high-risk context: The effects of unconditional cash transfers in South Africa. Econ. Dev. Cult. Chang. 2017, 65, 619–652. [Google Scholar] [CrossRef]
- Bronfenbrenner, U. Toward an experimental ecology of human development. Am. Psychol. 1977, 32, 513–531. [Google Scholar] [CrossRef]
- Bronfenbrenner, U. Developmental research, public policy, and the ecology of childhood. Child. Dev. 1974, 45, 1–5. [Google Scholar] [CrossRef]
- Bronfenbrenner, U. The Ecology of Human Development: Experiments by Nature and Design; Harvard University Press: Cambridge, UK, 1979. [Google Scholar]
- Morris, P.; Aber, J.L.; Wolf, S.; Berg, J. Using Incentives to Change How Teenagers Spend Their Time: The Effect of New York City’s Conditional Cash Transfer Program; MDRC: New York, NY, USA, 2012. [Google Scholar]
- Clauss-Ehlers, C.S.; Garagiola, E.R. Cultural competence and cultural humility as foundations for meaningful engagement among an educational system of care for school stakeholders. In Handbook of School Mental Health: Innovations in Science and Practice; Springer International Publishing: Berlin/Heidelberg, Germany, 2023; pp. 265–282. [Google Scholar] [CrossRef]
- Cookson, T. Unjust Conditions: Women’s Work and the Hidden Cost of Cash Transfer Programs; University of California Press: Oakland, CA, USA, 2018. [Google Scholar]
- Roelen, K. Receiving social assistance in low- And middle-income countries: Negating shame or producing stigma? J. Soc. Policy 2020, 49, 705–723. [Google Scholar] [CrossRef]
- Samuels, F.; Stavropoulou, M. ‘Being able to breathe again’: The effects of cash transfer programmes on psychosocial wellbeing. In The Social and Political Potential of Cash Transfers; Routledge: London, UK, 2018; pp. 13–28. [Google Scholar] [CrossRef]
- Gaarder, M. Conditional versus unconditional cash: A commentary. J. Dev. Eff. 2012, 4, 130–133. [Google Scholar] [CrossRef]
- Haman, O.B. Conditional and unconditional cash transfer programs: The recent experiences around the world. Int. J. Res. Innov. Soc. Sci. 2019, 3, 210–219. Available online: https://hdl.handle.net/102.100.100/555946 (accessed on 22 August 2024).
- Ladhani, S.; Sitter, K.C. Conditional cash transfers: A critical review. Dev. Policy Rev. 2020, 38, 28–41. [Google Scholar] [CrossRef]
- Swiss Academy of Sciences (SCNAT). Commission for Research Partnerships with Developing Countries (KFPE). Available online: https://kfpe.scnat.ch/en/about_kfpe (accessed on 22 August 2024).
- Stöckli, B.; Wiesmann, U.; Lys, J.-A. A Guide for Transboundary Research Partnerships: 11 Principles, 3rd ed. (1st ed. 2012); Swiss Commission for Research Partnerships with Developing Countries (KFPE): Bern, Switzerland, 2018; Available online: https://portal-cdn.scnat.ch/asset/4d8372ee-27d7-558a-b9db-77bf409ceef4/KFPE-11P-7Q-3d2018.pdf?b=370a2788-58f3-581e-85d7-2418b87c662e&v=8ef687bc-7b14-5a4f-ad9e-bf494cddc1d7_0&s=gLwVbtPON190F6auadVe-DPd_IOknFA_pssGzeBGB68h8nfbZIcnUaztPkFbUOKFef8V2w2-5NzkK61J2WEdN4JXXheHl2gX1f6cLTTro8WFmDkhlKvHQjqRQDZdPmPo3whl0-P3PWWEWWinhvJ5hWLGC5hYwVTAPC0kLEC-F7g (accessed on 22 August 2024).
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Lesser, T.L.; Matalon, M.; Clauss-Ehlers, C.S. Implications of Cash Transfer Programs for Mental Health Promotion among Families Facing Significant Stressors: Using Ecological Systems Theory to Explain Successes of Conditional and Unconditional Programs. Behav. Sci. 2024, 14, 770. https://doi.org/10.3390/bs14090770
Lesser TL, Matalon M, Clauss-Ehlers CS. Implications of Cash Transfer Programs for Mental Health Promotion among Families Facing Significant Stressors: Using Ecological Systems Theory to Explain Successes of Conditional and Unconditional Programs. Behavioral Sciences. 2024; 14(9):770. https://doi.org/10.3390/bs14090770
Chicago/Turabian StyleLesser, Tali L., Maya Matalon, and Caroline S. Clauss-Ehlers. 2024. "Implications of Cash Transfer Programs for Mental Health Promotion among Families Facing Significant Stressors: Using Ecological Systems Theory to Explain Successes of Conditional and Unconditional Programs" Behavioral Sciences 14, no. 9: 770. https://doi.org/10.3390/bs14090770
APA StyleLesser, T. L., Matalon, M., & Clauss-Ehlers, C. S. (2024). Implications of Cash Transfer Programs for Mental Health Promotion among Families Facing Significant Stressors: Using Ecological Systems Theory to Explain Successes of Conditional and Unconditional Programs. Behavioral Sciences, 14(9), 770. https://doi.org/10.3390/bs14090770