
Assessing the Psychometric Properties of the Illness Management and Recovery Scale: A Systematic Review Using the Consensus-Based Standards for the Selection of Health Measurement Instruments (COSMIN)

 , , and
, , and
Abstract
1. Background
2. Methods
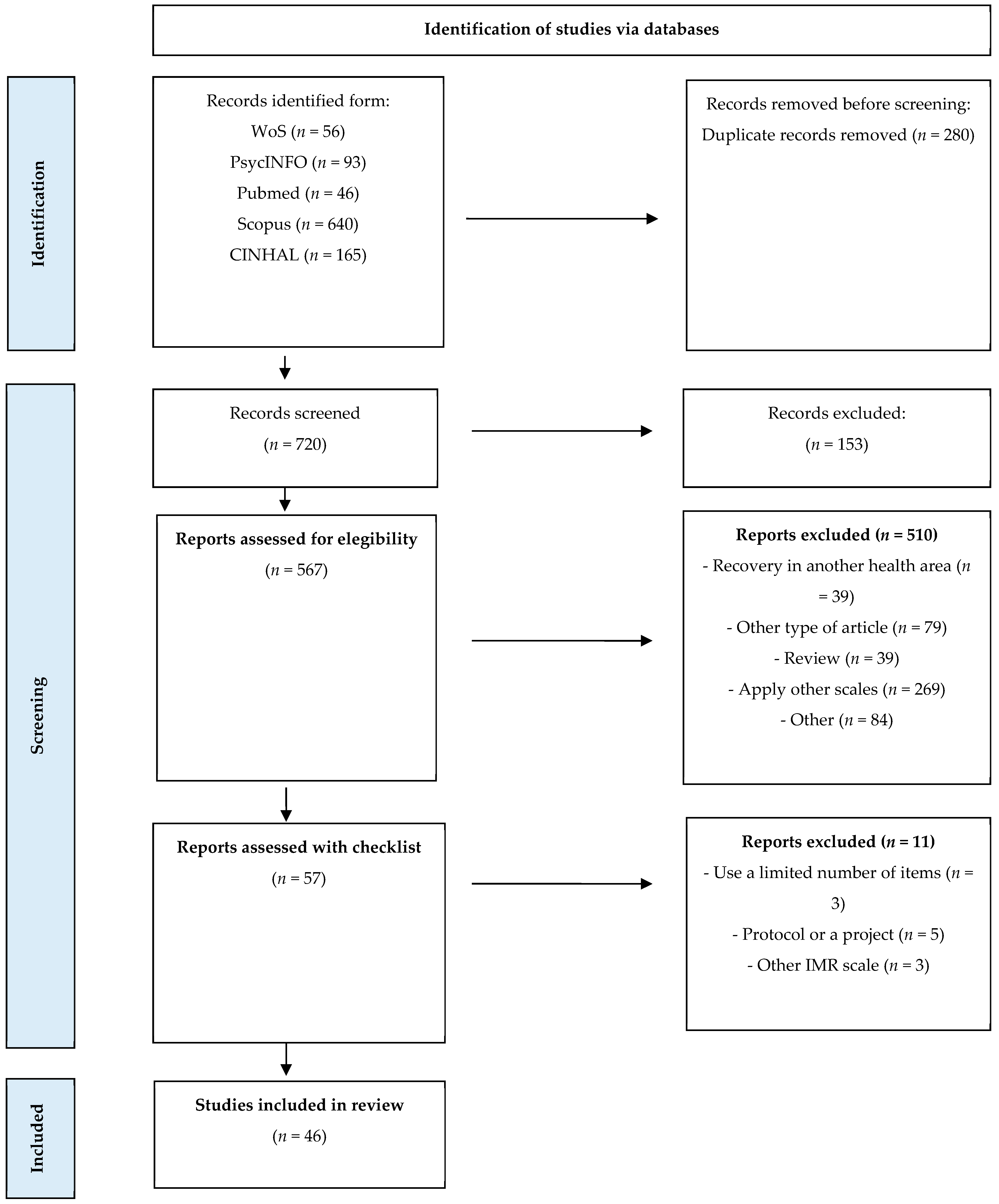
2.1. Search Strategy
2.2. Inclusion and Exclusion Criteria
2.3. Screening
2.4. Study Selection and Data Extraction
2.5. Evaluation of Selected Studies
- (a)
- Methodological Quality Assessment: As a first step, the methodological quality of the included studies was evaluated using the COSMIN Risk of Bias checklist, which comprises 10 domains describing a specific psychometric property (see Table 1). We systematically assessed each study against the defined criteria outlined in each domain (i.e., box) and assigned a rating of very good, adequate, doubtful, or inadequate methodological quality in each case, based on the degree of rigor in a study’s design and how it was conducted and reported. This phase allowed us to analyze each study individually, understanding the strengths and limitations of the selected studies.
- (b)
- Measurement Property Assessment: As a second step, we assessed the measurement properties using predefined quality criteria in alignment with COSMIN guidelines. Each psychometric property was rated as sufficient (+), insufficient (−), or indeterminate (?), based on the applied quality criteria. This phase allowed us to assess the quality of each psychometric property of the IMR-S analyzed.
- (c)
- Evidence Synthesis and Quality Grading: As a final step, we summarized the evidence, considering both the methodological quality and measurement property assessments, using the Grading of Recommendations Assessment, Development and Evaluation (GRADE) approach [24] to evaluate the quality of evidence, considering factors such as risk of bias, inconsistency, indirectness, imprecision, and publication bias. The resulting quality level of the evidence in each domain was categorized as high, moderate, low, or very low, indicating the confidence in the results and the trustworthiness of the scale. This phase allowed us to obtain a comprehensive assessment of the evidence studied.
3. Results
3.1. Study Characteristics
3.2. Study Assessment: Methodological Quality, Psychometric Properties, and Quality of Evidence of the Scale
3.2.1. Content Validity
3.2.2. Structural Validity
3.2.3. Internal Consistency
3.2.4. Reliability
3.2.5. Measurement Error
3.2.6. Hypothesis Testing
3.2.7. Responsiveness
4. Discussion
5. Conclusions
Supplementary Materials
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Maone, A.; D’Avanzo, B. Recuperación: Nuevos Paradigmas de Salud Mental; Psimática: Madrid, Spain, 2017. [Google Scholar]
- Deegan, P.E. Recovery: The lived experience of rehabilitation. Psychosoc. Rehabil. J. 1988, 11, 11–19. [Google Scholar]
- Roosenschoon, B.; van Weeghel, J.; Deen, M.L.; van Esveld, E.W.; Kamperman, A.M.; Mulder, C.L. Effects of Illness Management and Recovery: A Multicentric Randomized Controlled Trial. Front. Psychiatry 2021, 12, 723435. [Google Scholar] [CrossRef]
- Bendel-Rozow, T. Recovery-oriented dance movement therapy group with adults coping with severe mental health conditions: A controlled trial. Arts Psychother. 2021, 75, 101830. [Google Scholar] [CrossRef]
- Mueser, K.; Gingerich, S.; Salyers, M.; McGuire, A.; Reyes, R.; Cunningham, H. Illness Management and Recovery Scales. Psyctests Dataset 2005. [Google Scholar] [CrossRef]
- Polat, S.; Kutlu, Y. The effectiveness of illness management and recovery program in patients with schizophrenia. Arch. Psychiatr. Nurs. 2021, 35, 162–167. [Google Scholar] [CrossRef]
- Mueser, K. The Illness Management and Recovery Program: Rationale, Development, and Preliminary Findings. Schizophr. Bull. 2006, 32 (Suppl. S1), S32–S43. [Google Scholar] [CrossRef]
- Davidson, L.; Rowe, M.; DiLeo, P.; Bellamy, C.; Delphin-Rittmon, M. Recovery-Oriented Systems of Care: A Perspective on the Past, Present, and Future. Alcohol Res. 2021, 41, 9. [Google Scholar] [CrossRef]
- Mueser, K.T.; Gingerich, S. Illness Management and Recovery (IMR) Scales. In Measuring the Promise: A Compendium of Recovery Measures; Campbell-Orde, T., Chamberlin, J., Carpenter, J., Leff, H.S., Eds.; Human Services Research Institute, Evaluation Center: Cambridge, MA, USA, 2005; Volume 2. [Google Scholar]
- MacMillan, G.; St Clair-Thompson, H. The relationship between mental toughness and subjective mental illness recovery. New Ideas Psychol. 2021, 63, 100881. [Google Scholar] [CrossRef]
- Penas, P.; Iraurgi, I.; Moreno, M.C.; Uriarte, J. How is evaluated mental health recovery? A systematic review. Actas Españolas Psiquiatr. 2019, 47, 23–32. [Google Scholar]
- Sklar, M.; Groessl, E.; O′Connell, M.; Davidson, L.; Aarons, G. Instruments for measuring mental health recovery: A systematic review. Clin. Psychol. Rev. 2013, 33, 1082–1095. [Google Scholar] [CrossRef]
- Corrigan, P.W.; Giffort, D.; Rashid, F.; Leary, M.; Okele, I. Recovery as a psychological construct. Community Ment. Health J. 1999, 35, 231–239. [Google Scholar] [CrossRef]
- Young, S.L.; Bullock, W.A. The Mental Health Recovery Measure; University of Toledo, Department of Psychology: Toledo, OH, USA, 2003. [Google Scholar]
- Hasson-Ohayon, I.; Roe, D.; Kravetz, S. A Randomized Controlled Trial of the Effectiveness of the Illness Management and Recovery Program. Psychiatr. Serv. 2007, 58, 1461–1466. [Google Scholar] [CrossRef]
- Levitt, A.J.; Mueser, K.T.; DeGenova, J.; Lorenzo, J.; Bradford-Watt, D.; Barbosa, A.; Karlin, M.; Chernick, M. Randomized Controlled Trial of Illness Management and Recovery in Multiple-Unit Supportive Housing. Psychiatr. Serv. 2009, 60, 1629–1636. [Google Scholar] [CrossRef]
- Salyers, M.; McGuire, A.; Kukla, M.; Fukui, S.; Lysaker, P.; Mueser, K. A Randomized Controlled Trial of Illness Management and Recovery with an Active Control Group. Psychiatr. Serv. 2014, 65, 1005–1011. [Google Scholar] [CrossRef]
- Dalum, H.; Waldemar, A.; Korsbek, L.; Hjorthøj, C.; Mikkelsen, J.; Thomsen, K.; Kistrup, K.; Olander, M.; Lindschou, J.; Nordentoft, M.; et al. Participants’ and staffs’ evaluation of the Illness Management and Recovery program: A randomized clinical trial. J. Ment. Health 2016, 27, 30–37. [Google Scholar] [CrossRef]
- Roosenschoon, B.; Mulder, C.; Deen, M.; van Weeghel, J. Effectiveness of illness management and recovery (IMR) in the Netherlands: A randomised clinical trial. BMC Psychiatry 2016, 16, 73. [Google Scholar] [CrossRef]
- Egeland, K.M.; Ruud, T.; Ogden, T.; Färdig, R.; Lindstrøm, J.C.; Heiervang, K.S. How to implement Illness Management and Recovery (IMR) in mental health service settings: Evaluation of the implementation strategy. Int. J. Ment. Health Syst. 2017, 11, 13. [Google Scholar] [CrossRef]
- Barbic, S.; Kidd, S.; Durisko, Z.; Yachouh, R.; Rathitharan, G.; McKenzie, K. What Are the Personal Recovery Needs of Community-Dwelling Individuals with Mental Illness? Preliminary Findings from the Canadian Personal Recovery Outcome Measurement (C-PROM) Study. Can. J. Community Ment. Health 2018, 37, 29–47. [Google Scholar] [CrossRef]
- Mokkink, L.; de Vet, H.; Prinsen, C.; Patrick, D.; Alonso, J.; Bouter, L.; Terwee, C. COSMIN Risk of Bias checklist for systematic reviews of Patient-Reported Outcome Measures. Qual. Life Res. 2018, 27, 1171–1179. [Google Scholar] [CrossRef]
- Terwee, C.B.; Prinsen, C.A.C.; Chiarotto, A.; Westerman, M.J.; Patrick, D.L.; Alonso, J.; Bputer, L.M.; de Vet, H.C.W.; Mokkink, L.B. COSMIN methodology for evaluating the content validity of patient-reported outcome measures: A Delphi study. Qual. Life Res. 2018, 27, 1159–1170. [Google Scholar]
- Prinsen, C.; Mokkink, L.B.; Bouter, L.M.; Alonso, J.; Patrick, D.L.; De Vet, H.C. COSMIN guidelines for systematic reviews of Patient-Reporterd Outcomes Measures. Qual. Life Res. 2018, 27, 1147–1157. [Google Scholar]
- PRISMA Transparent Reporting of Systematic Reviews and Meta-Analyses. PRISMA 2020 Checklist. Available online: http://www.prisma-statement.org/ (accessed on 23 January 2024).
- Fortuna, K.; DiMilia, P.; Lohman, M.; Bruce, M.; Zubritsky, C.; Halaby, M.; Walker, R.; Brooks, J.; Bartels, S. Feasibility, Acceptability, and Preliminary Effectiveness of a Peer-Delivered and Technology Supported Self-Management Intervention for Older Adults with Serious Mental Illness. Psychiatr. Q. 2018, 89, 293–305. [Google Scholar] [CrossRef]
- Sklar, M.; Sarkin, A.; Gilmer, T.; Groessl, E. The psychometric properties of the Illness Management and Recovery scale in a large American public mental health system. Psychiatry Res. 2012, 199, 220–227. [Google Scholar] [CrossRef]
- Bartels, S.; Pratt, S.; Mueser, K.; Naslund, J.; Wolfe, R.; Santos, M.; Xie, H.; Riera, E. Integrated IMR for Psychiatric and General Medical Illness for Adults Aged 50 or Older with Serious Mental Illness. Psychiatr. Serv. 2014, 65, 330–337. [Google Scholar] [CrossRef]
- Beentjes, T.A.A.; Goossens, P.J.J.; Vermeulen, H.; Teerenstra, S.; Nijhuis-Van Der Sanden, M.W.G.; Van Gaal, B.G.I. E-IMR: E-health added to face-to-face delivery of Illness Management & Recovery programme for people with severe mental illness, an exploratory clustered randomized controlled trial. BMC Health Serv. Res. 2018, 18, 962. [Google Scholar] [CrossRef]
- Beentjes, T.A.A.; Teerenstra, S.; Vermeulen, H.; Goossens, P.J.J.; der Sanden, M.W.G.N.-V.; van Gaal, B.G.I. Identifying the minimal important difference in patient-reported outcome measures in the field of people with severe mental illness: A pre–post-analysis of the Illness Management and Recovery Programme. Qual. Life Res. 2021, 30, 1723–1733. [Google Scholar] [CrossRef]
- Ben-Zeev, D.; Buck, B.; Meller, S.; Hudenko, W.; Hallgren, K. Augmenting Evidence-Based Care with a Texting Mobile Interventionist: A Pilot Randomized Controlled Trial. Psychiatr. Serv. 2020, 71, 1218–1224. [Google Scholar] [CrossRef]
- Buck, B.; Nguyen, J.; Porter, S.; Ben-Zeev, D.; Reger, G.M. FOCUS mHealth Intervention for Veterans with Serious Mental Illness in an Outpatient Department of Veterans Affairs Setting: Feasibility, Acceptability, and Usability Study. Psychiatr. Q. 2022, 28, e26049. [Google Scholar] [CrossRef]
- Casey, R.; Wiener, J.C.; Krupa, T.; Lysaght, R.; Le Ber, M.J.; Ruhara, R.; Price, E.; Pervez, R.; Kidd, S.; Mutiso, V.; et al. Evaluating the feasibility and potential impacts of a recovery-oriented psychosocial rehabilitation toolkit in a health care setting in Kenya: A mixed-methods study. Psychiatr. Rehabil. J. 2023, 46, 55–64. [Google Scholar] [CrossRef]
- Chinman, M.; Oberman, R.S.; Hanusa, B.H.; Cohen, A.N.; Salyers, M.P.; Twamley, E.W.; Young, A.S. A cluster randomized trial of adding peer specialists to intensive case management teams in the Veterans Health Administration. J. Behav. Health Serv. Res. 2015, 42, 109–121. [Google Scholar] [CrossRef]
- Daass-Iraqi, S.; Mashiach-Eizenberg, M.; Garber-Epstein, P.; Roe, D. Impact of a culturally adapted version of illness management and recovery on Israeli Arabs with serious mental illness. Psychiatr. Serv. 2020, 71, 951–954. [Google Scholar] [CrossRef]
- Färdig, R.; Lewander, T.; Fredriksson, A.; Melin, L. Evaluation of the Illness Management and Recovery Scale in schizophrenia and schizoaffective disorder. Schizophr. Res. 2011, 132, 157–164. [Google Scholar] [CrossRef]
- Färdig, R.; Lewander, T.; Melin, L.; Folke, F.; Fredriksson, A. A randomized controlled trial of the illness management and recovery program for persons with schizophrenia. Psychiatr. Serv. 2011, 62, 606–612. [Google Scholar] [CrossRef]
- Färdig, R.; Fredriksson, A.; Lewander, T.; Melin, L.; Mueser, K. Neurocognitive functioning and outcome of the Illness Management and Recovery Program for clients with schizophrenia and schizoaffective disorder. Nord. J. Psychiatry 2016, 70, 430–435. [Google Scholar] [CrossRef]
- Firmin, R.L.; Luther, L.; Lysaker, P.H.; Salyers, M.P. Self-initiated helping behaviors and recovery in severe mental illness: Implications for work, volunteerism, and peer support. Psychiatr. Rehabil. J. 2015, 38, 336–341. [Google Scholar] [CrossRef]
- Fortuna, L.R.; Falgas-Bague, I.; Ramos, Z.; Porche, M.V.; Alegría, M. Development of a cognitive behavioral therapy with integrated mindfulness for Latinx immigrants with co-occurring disorders: Analysis of intermediary outcomes. Psychol. Trauma 2020, 12, 825–835. [Google Scholar] [CrossRef]
- Fortuna, K.L.; Myers, A.L.; Ferron, J.; Kadakia, A.; Bianco, C.; Bruce, M.L.; Bartels, S.J. Assessing a digital peer support self-management intervention for adults with serious mental illness: Feasibility, acceptability, and preliminary effectiveness. J. Ment. Health 2022, 31, 833–841. [Google Scholar] [CrossRef]
- Garber-Epstein, P.; Zisman-Ilani, Y.; Levine, S.; Roe, D. Comparative impact of professional mental health background on ratings of consumer outcome and fidelity in an illness management and recovery program. Psychiatr. Rehabil. J. 2013, 36, 236–242. [Google Scholar] [CrossRef]
- Gilmer, T.; Henwood, B.; Goode, M.; Sarkin, A.; Innes-Gomberg, D. Implementation of Integrated Health Homes and Health Outcomes for Persons with Serious Mental Illness in Los Angeles County. Psychiatr. Serv. 2016, 67, 1062–1067. [Google Scholar] [CrossRef]
- Goossens, P.; Beentjes, T.; Knol, S.; Salyers, M.; de Vries, S. Investigating the reliability and validity of the Dutch versions of the illness management and recovery scales among clients with mental disorders. J. Ment. Health 2017, 26, 489–495. [Google Scholar] [CrossRef][Green Version]
- Hasson-Ohayon, I.; Roe, D.; Kravetz, S. The psychometric properties of the illness management and recovery scale: Client and clinician versions. Psychiatry Res. 2008, 160, 228–235. [Google Scholar] [CrossRef]
- Jensen, S.; Dalum, H.; Korsbek, L.; Hjorthøj, C.; Mikkelsen, J.; Thomsen, K.; Kistrup, K.; Olander, M.; Lidnschou, J.; Mueser, K.; et al. Illness management and recovery: One-year follow-up of a randomized controlled trial in Danish community mental health centers: Long-term effects on clinical and personal recovery. BMC Psychiatry 2019, 19, 65. [Google Scholar] [CrossRef]
- Kukla, M.; Salyers, M.; Lysaker, P. Levels of Patient Activation Among Adults with Schizophrenia. J. Nerv. Ment. Dis. 2013, 201, 339–344. [Google Scholar] [CrossRef]
- Matthias, M.; Fukui, S.; Salyers, M. What Factors are Associated with Consumer Initiation of Shared Decision Making in Mental Health Visits? Adm. Policy Ment. Health Ment. Health Serv. Res. 2017, 44, 133–140. [Google Scholar] [CrossRef]
- Matthias, M.; Fukui, S.; Kukla, M.; Eliacin, J.; Bonfils, K.; Firmin, R. Consumer and Relationship Factors Associated with Shared Decision Making in Mental Health Consultations. Psychiatr. Serv. 2014, 65, 1488–1491. [Google Scholar] [CrossRef]
- McGuire, A.; Kean, J.; Bonfils, K.; Presnell, J.; Salyers, M. Rasch analysis of the illness management and recovery scale-clinician version. J. Eval. Clin. Pract. 2014, 20, 383–389. [Google Scholar] [CrossRef]
- McGuire, A.; White, D.; Bartholomew, T.; Flanagan, M.; McGrew, J.; Rollins, A.; Mueser, K.; Salyers, M. The Relationship Between Provider Competence, Content Exposure, and Consumer Outcomes in Illness Management and Recovery Programs. Adm. Policy Ment. Health Serv. Res. 2017, 44, 81–91. [Google Scholar] [CrossRef]
- Miyajima, M.; Hatakeyama, Y.; Ichiki, K.; Matsuzaki, Y.; Niyama, H.; Omiya, H. A pilot study of Illness Management and Recovery in patients acutely admitted to a psychiatric ward. J. Psychosoc. Rehabil. Ment. Health 2023, 10, 35–44. [Google Scholar] [CrossRef]
- Polat, S.; Kutlu, Y.; Gültekin, B. Psychometric properties of the Turkish version of Illness Management and Recovery Scale-Patient form. Perspect. Psychiatr. Care 2020, 57, 279–286. [Google Scholar] [CrossRef]
- Pratt, C.W.; Lu, W.; Swarbrick, M.; Murphy, A. Selective provision of illness management and recovery modules. Am. J. Psychiatr. Rehabil. 2011, 14, 245–258. [Google Scholar] [CrossRef]
- Pratt, S.I.; Naslund, J.A.; Wolfe, R.S.; Santos, M.; Bartels, S.J. Automated telehealth for managing psychiatric instability in people with serious mental illness. J. Ment. Health 2015, 24, 261–265. [Google Scholar] [CrossRef]
- Salyers, M.; Godfrey, J.; Mueser, K.; Labriola, S. Measuring Illness Management Outcomes: A Psychometric Study of Clinician and Consumer Rating Scales for Illness Self-Management and Recovery. Community Ment. Health J. 2007, 43, 459–480. [Google Scholar] [CrossRef]
- Salyers, M.; Matthias, M.; Spann, C.; Lydick, J.; Rollins, A.; Frankel, R. The Role of Patient Activation in Psychiatric Visits. Psychiatr. Serv. 2009, 60, 1535–1539. [Google Scholar] [CrossRef]
- Salyers, M.P.; McGuire, A.B.; Rollins, A.L.; Bond, G.R.; Mueser, K.; Macy, V.R. Integrating assertive community treatment and illness management and recovery for consumers with severe mental illness. Community Ment. Health J. 2010, 46, 319–329. [Google Scholar] [CrossRef]
- Tan, C.; Ishak, R.; Lim, T.; Marimuthusamy, P.; Kaurss, K.; Leong, J. Illness management and recovery program for mental health problems: Reducing symptoms and increasing social functioning. J. Clin. Nurs. 2017, 26, 3471–3485. [Google Scholar] [CrossRef]
- White, D.; McGuire, A.; Luther, L.; Anderson, A.; Phalen, P.; McGrew, J. Consumer factors predicting level of treatment response to illness management and recovery. Psychiatr. Rehabil. J. 2017, 40, 344–353. [Google Scholar] [CrossRef]
- Shanks, V.; Williams, J.; Leamy, M.; Bird, V.; Le Boutillier, C.; Slade, M. Measures of Personal Recovery: A Systematic Review. Psychiatr. Serv. 2013, 64, 974–980. [Google Scholar] [CrossRef]
- UN General Assembly, Convention on the Rights of Persons with Disabilities. Available online: https://www.refworld.org/docid/45f973632.html (accessed on 16 December 2023).
- Sampietro, H.M.; Rojo, J.E.; Gómez-Benito, J. Recovery-oriented care in public mental health policies in Spain: Opportunities and barriers. Clínica Salud 2023, 34, 35–40. [Google Scholar] [CrossRef]
- Bland, J.M.; Altman, D.G. Cronbach’s Alpha. Br. Med. J. 1997, 314, 572. [Google Scholar] [CrossRef]
- National Academies of Sciences, Engineering, and Medicine. Ending Discrimination Against People with Mental and Substance Use Disorders: The Evidence for Stigma Change; The National Academies Press: Washington, DC, USA, 2016. [Google Scholar] [CrossRef]
- Amini, F.; Mousavi, S.M.; Yazdani, J. Compare social support in patients with schizophrenia or methamphetamine dependency with healthy individuals. Ment. Health Soc. Incl. 2023; in press. [Google Scholar] [CrossRef]
- Leamy, M.; Bird, V.J.; Le Boutillier, C.; Williams, J.; Slade, M. A conceptual framework for personal recovery in mental health: Systematic review and narrative synthesis. Br. J. Psychiatry 2011, 199, 445–452. [Google Scholar]


{kind=link}
| Content Validity | |
|---|---|
| Box 1 | Outcome measure tool development |
| Box 2 | Content validity |
| Internal Structure | |
| Box 3 | Structural validity |
| Box 4 | Internal consistency |
| Box 5 | Cross-cultural validity/measurement invariance |
| Remaining Measurement Properties | |
| Box 6 | Reliability |
| Box 7 | Measurement error |
| Box 8 | Criterion validity |
| Box 9 | Hypothesis testing for construct validity |
| Box 10 | Responsiveness |
| Authors | Sample Size | Females n (%) | Mean Sample Age | IMR-S | |
|---|---|---|---|---|---|
| Version Applied | No. of Items | ||||
| Barbic et al., 2018 b [21] | 228 | 112 (49.1%) | 45.8 | Client | 13 |
| Bartels et al., 2014 b [28] | 71 | 39 (43.7%) | 60.3 | Both | 15 |
| Beentjes et al., 2018 b [29] | 60 | 36 (60.0%) | 43.8 | Client | 15 |
| Beentjes et al., 2021 b [30] | 60 | 36 (60.0%) | 45 | Client | 15 |
| Bendel-Rozow, 2021 b [4] | 52 | 13 (25.0%) | 48 | Both | 15 |
| Ben-Zeev et al., 2020 b [31] | 49 | 22 (44.9%) | 44.8 | Client | 15 |
| Buck et al., 2022 b [32] | 17 | 5 (29.4%) | 55.1 | Client | 15 |
| Casey et al., 2023 b [33] | 23 | 7 (30.4%) | 35 | Client | 15 |
| Chinman et al., 2015 b [34] | 238 | 28 (11.8%) | 53.2 | Client | 15 |
| Daas-Iraqi et al., 2020 b [35] | 150 | NS | 40.9 | Both | 15 |
| Dalum et al., 2016 b [18] | 198 | 89 (44.9%) | 43 | Both | 15 |
| Egeland et al., 2017 b [20] | 44 | 16 (36.4%) | 40.7 | Both | 15 |
| Färdig et al., 2011 b [36] | 102 | 41 (38.3%) | 43 | Both | 15 |
| Färdig et al., 2011 b [37] | 41 | 19 (46.3%) | 40.4 | Both | 15 |
| Färdig et al., 2016 b [38] | 53 | 23 (43.4%) | 41.5 | Both | 15 |
| Firmin et al., 2015 b [39] | 46 | 11 (23.9%) | 48.5 | Client | 15 |
| Fortuna et al., 2018 b [26] | 8 | 7 (87.5%) | 68.8 | Client | 15 |
| Fortuna et al., 2020 b [40] | 341 | NS | NS | Client | 15 |
| Fortuna et al., 2022 b [41] | 21 | 15 (71.4%) | 39.9 | Client | 15 |
| Garber-Epstein et al., 2013 b [42] | 252 | 112 (44.4%) | 43.5 | Client | 13 |
| Gilmer et al., 2016 b [43] | 1279 | NS | NS | Clinician | 15 |
| Goosens et al., 2017 a [44] | 111 | 53 (47.7%) | Between 18 →65 | Both | 15 |
| Hasson-Ohayon et al., 2007 a [15] | 210 | 73 (34.8%) | 34.7 | Both | 15 |
| Hasson-Ohayon et al., 2008 a [45] | 210 | 73 (34.8%) | 34.6 | Both | 15 |
| Jensen et al., 2019 b [46] | 198 | 89 (44.9%) | 43 | Both | 15 |
| Kukla et al., 2013 b [47] | 119 | 25 (21.0%) | 47.6 | Both | 15 |
| Levitt et al., 2009 b [16] | 104 | 38 (36.5%) | 53.9 | Both | 15 |
| MacMillan et al., 2021 a [10] | 77 | 58 (75.3%) | Between 18 → 50 | Client | 14 |
| Matthias et al., 2017 b [48] | 63 | 9 (14.3%) | 53 | Client | 15 |
| Matthias et al., 2014 b [49] | 63 | 9 (14.3%) | 53 | Client | 15 |
| McGuire et al., 2014 a [50] | 697 | 331 (47.5%) | NS | Clinician | 15 |
| McGuire et al., 2017 b [51] | 236 | 97 (41.1%) | 45.2 | Client | 15 |
| Miyajima et al., 2023 b [52] | 10 | 7 (70.0%) | Median 50.5 | Both | 15 |
| Polat &Kutlu 2021 b [6] | 50 | 26 (52%) | 39.1 | Client | 15 |
| Polat et al., 2020 a [53] | 75 | 30 (40.0%) | 41.6 | Client | 15 |
| Pratt et al., 2011 b [54] | 44 | 29 (65.9%) | 46.4 | Client | 15 |
| Pratt et al., 2015 b [55] | 38 | 27 (71.0%) | 46.4 | Client | 15 |
| Roosenchoon et al., 2016 b [19] | 61 | 33 (54.1%) | 42.4 | Both | 15 |
| Roosenchoon et al., 2021 b [3] | 187 | 88 (47.1%) | 44.2 | Both | 15 |
| Salyers et al., 2007 a [56] | 59 | 20 (33.9%) | 43.5 | Both | 15 |
| Salyers et al., 2009 b [57] | 40 | 21 (52.5%) | 43.5 | Client | 15 |
| Salyers et al., 2010 b [58] | 324 | 148 (45.7%) | 42.3 | Both | 15 |
| Salyers et al., 2014 b [17] | 118 | 24 (20.3%) | 47.7 | Client | 15 |
| Sklar et al., 2012 a [27] | 10659 | 5283 (49.6%) | 43.2 | Clinician | 15 |
| Tan et al., 2017 b [59] | 50 | 31 (62.0%) | 44.2 | Both | 15 |
| White et al., 2017 b [60] | 236 | 97 (41.1%) | 45.2 | Client | 15 |
| IMR-S Client Version | IMR-S Clinician Version | ||
|---|---|---|---|
| Total Scale | Max | 0.85 [59] | 0.85 [59] |
| Min | 0.49 [40] | 0.69 [18] | |
| F1: Coping, recovery, and symptoms | Max | 0.73 [15] | 0.83 [15] |
| Min | 0.69 [44,53] | 0.67 [50] | |
| F2: Management and personal goals | Max | 0.69 [53] | 0.83 [27] |
| Min | 0.50 [15] | 0.61 [44] | |
| F3: Effective use of medication and substance abuse | Max | 0.74 [15] | 0.69 [27] |
| Min | 0.35 [53] | 0.28 [44] |
| Measurement Property | COSMIN Risk of Bias Checklist Ratings | Quality of Evidence | |||
|---|---|---|---|---|---|
| Very Good | Adequate | Doubtful | Inadequate | ||
| Content validity (n = 1) | 0 | 0 | 1 | 0 | Low |
| Structural validity (n = 3) | 2 | 1 | 0 | 0 | High (?) |
| Internal consistency (n = 20) | 18 | 0 | 2 | 0 | Moderate (−) |
| Reliability (n = 4) | 0 | 4 | 0 | 0 | Moderate (?) |
| Measurement error (n = 1) | 0 | 1 | 0 | 0 | Low (+) |
| Hypothesis testing (n = 14) | 8 | 4 | 2 | 0 | Moderate (+) |
| Responsiveness (n = 31) | 0 | 0 | 11 | 20 | Low (+) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Martín-Ordiales, N.; Hidalgo, M.D.; Martín-Chaparro, M.P.; Ballester-Plané, J.; Barrios, M. Assessing the Psychometric Properties of the Illness Management and Recovery Scale: A Systematic Review Using the Consensus-Based Standards for the Selection of Health Measurement Instruments (COSMIN). Behav. Sci. 2024, 14, 340. https://doi.org/10.3390/bs14040340
Martín-Ordiales N, Hidalgo MD, Martín-Chaparro MP, Ballester-Plané J, Barrios M. Assessing the Psychometric Properties of the Illness Management and Recovery Scale: A Systematic Review Using the Consensus-Based Standards for the Selection of Health Measurement Instruments (COSMIN). Behavioral Sciences. 2024; 14(4):340. https://doi.org/10.3390/bs14040340
Chicago/Turabian StyleMartín-Ordiales, Nuria, María Dolores Hidalgo, María Pilar Martín-Chaparro, Júlia Ballester-Plané, and Maite Barrios. 2024. "Assessing the Psychometric Properties of the Illness Management and Recovery Scale: A Systematic Review Using the Consensus-Based Standards for the Selection of Health Measurement Instruments (COSMIN)" Behavioral Sciences 14, no. 4: 340. https://doi.org/10.3390/bs14040340
APA StyleMartín-Ordiales, N., Hidalgo, M. D., Martín-Chaparro, M. P., Ballester-Plané, J., & Barrios, M. (2024). Assessing the Psychometric Properties of the Illness Management and Recovery Scale: A Systematic Review Using the Consensus-Based Standards for the Selection of Health Measurement Instruments (COSMIN). Behavioral Sciences, 14(4), 340. https://doi.org/10.3390/bs14040340