

Is Formal Social Participation Associated with Cognitive Function in Middle-Aged and Older Adults? A Systematic Review with Meta-Analysis of Longitudinal Studies

Abstract
1. Introduction
2. Materials and Methods
2.1. Eligibility Criteria
2.2. Search Strategy
2.3. Study Selection and Data Extraction
2.4. Risk of Bias
2.5. Data Synthesis
2.6. Certainty of Evidence
3. Results
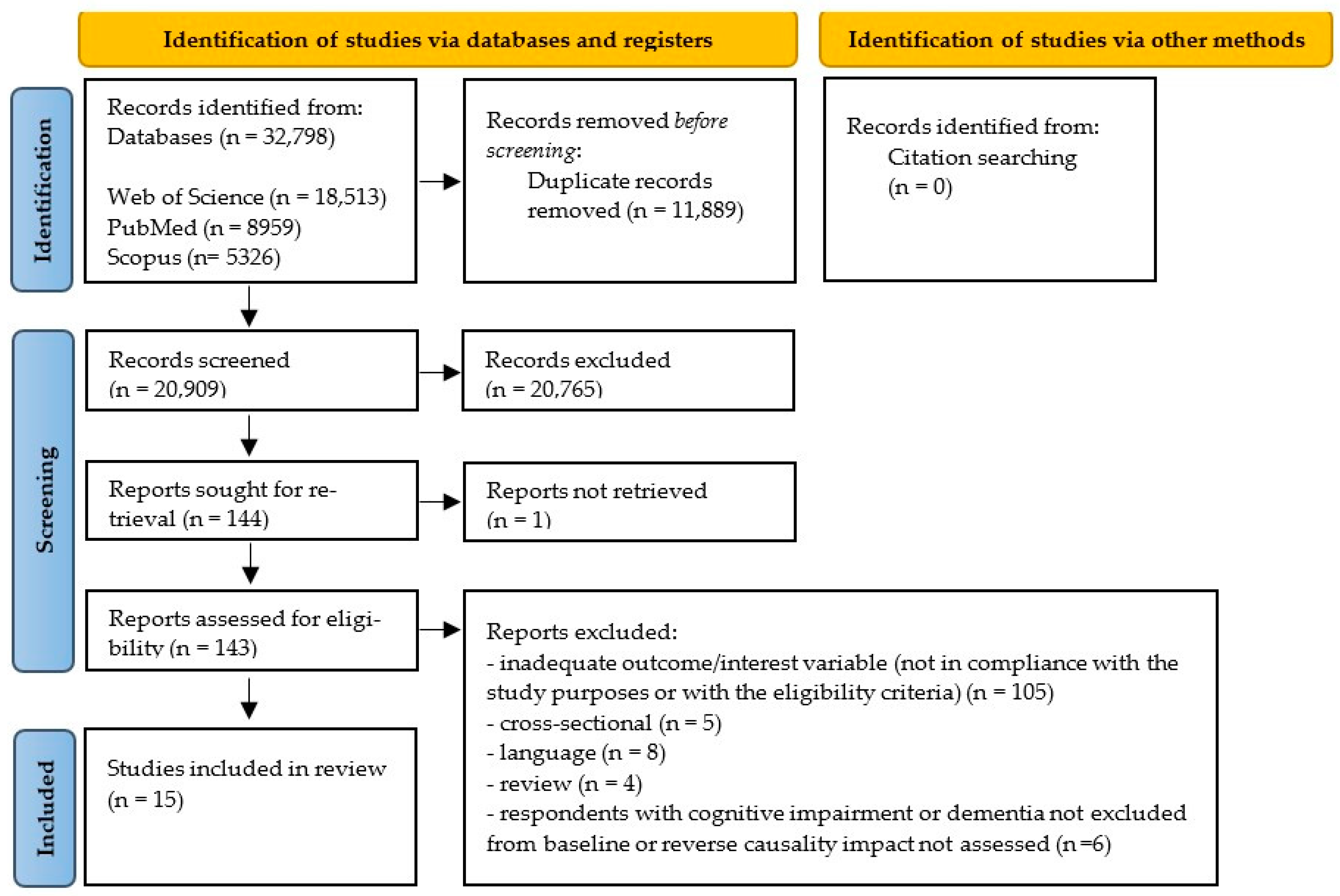
3.1. Search Results and Study Characteristics
3.2. Risk of Bias
3.3. Outcome Characteristics
3.4. Formal Social Participation Characteristics
3.5. Confounding Variables
3.6. Quantitative Synthesis on the Dichotomous Measurement of Cognitive Function
4. Discussion
4.1. Findings in the Context of Existing Knowledge
4.2. Limitations
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Plassman, B.L.; Williams, J.W.; Burke, J.R.; Holsinger, T.; Benjamin, S. Systematic Review: Factors Associated with Risk for and Possible Prevention of Cognitive Decline in Later Life. Ann. Intern. Med. 2010, 153, 182–193. [Google Scholar] [CrossRef]
- Duan, J.; Sam, N.B.; Wang, S.J.; Liu, Y. Exploring the Association between Cognitive Decline and All-Cause Mortality with Blood Pressure as a Potential Modifier in Oldest Old Individuals. Sci. Rep. 2022, 12, 17108. [Google Scholar] [CrossRef]
- Lv, X.; Li, W.; Ma, Y.; Chen, H.; Zeng, Y.; Yu, X.; Hofman, A.; Wang, H. Cognitive Decline and Mortality among Community-Dwelling Chinese Older People. BMC Med. 2019, 17, 63. [Google Scholar] [CrossRef]
- Calderón-Larrañaga, A.; Vetrano, D.L.; Ferrucci, L.; Mercer, S.W.; Marengoni, A.; Onder, G.; Eriksdotter, M.; Fratiglioni, L. Multimorbidity and Functional Impairment–Bidirectional Interplay, Synergistic Effects and Common Pathways. J. Intern. Med. 2019, 285, 255–271. [Google Scholar] [CrossRef]
- Khandker, R.K.; Ritchie, C.W.; Black, C.M.; Wood, R.; Jones, E.; Hu, X.; Ambegaonkar, B.M. Multi-National, Cross-Sectional Survey of Healthcare Resource Utilization in Patients with All Stages of Cognitive Impairment, Analyzed by Disease Severity, Country, and Geographical Region. J. Alzheimer’s Dis. 2020, 75, 1141–1152. [Google Scholar] [CrossRef] [PubMed]
- Corrêa, L.; Ottaviani, A.C.; Bregola, A.G.; de Oliveira, N.A.; Bento, S.R.; Pavarini, S.C.I. Cognitive Performance, Burden and Stress in Aged Caregivers of Older Adults with and without Cognitive Impairment. Dement. Neuropsychol. 2023, 17, e20220073. [Google Scholar] [CrossRef] [PubMed]
- Harris, M.L.; Errickson, J.; Ha, J.; Hoffman, G.J. Depressive Symptoms and Caregiving Intensity before and after Onset of Dementia in Partners: A Retrospective, Observational Study. Med. Care 2022, 60, 844–851. [Google Scholar] [CrossRef]
- Lenart, M.; Luc, M.; Pawlowski, M.; Seifert, I.; Wiegelmann, H.; Szczesniak, D.; Gerhardus, A.; Wolf-Ostermann, K.; Rouwette, E.; Rymaszewska, J. Protective and Risk Factors of Cognitive Decline and Dementia with a Special Emphasis on Social Health: A Systematic Mapping Review. Alzheimer’s Dement. 2020, 16, e041898. [Google Scholar] [CrossRef]
- Cai, S. Does Social Participation Improve Cognitive Abilities of the Elderly? J. Popul. Econ. 2022, 35, 591–619. [Google Scholar] [CrossRef]
- Kuiper, J.S.; Zuidersma, M.; Zuidema, S.U.; Burgerhof, J.G.M.; Stolk, R.P.; Oude Voshaar, R.C.; Smidt, N. Social Relationships and Cognitive Decline: A Systematic Review and Meta-Analysis of Longitudinal Cohort Studies. Int. J. Epidemiol. 2016, 45, 1169–1206. [Google Scholar] [CrossRef] [PubMed]
- Miceli, S.; Maniscalco, L.; Matranga, D. Social Networks and Social Activities Promote Cognitive Functioning in Both Concurrent and Prospective Time: Evidence from the SHARE Survey. Eur. J. Ageing 2019, 16, 145–154. [Google Scholar] [CrossRef]
- Kelly, M.E.; Duff, H.; Kelly, S.; Power, J.E.M.; Brennan, S.; Lawlor, B.A.; Loughrey, D.G. The Impact of Social Activities, Social Networks, Social Support and Social Relationships on the Cognitive Functioning of Healthy Older Adults: A Systematic Review. Syst. Rev. 2017, 6, 259. [Google Scholar] [CrossRef]
- Piolatto, M.; Bianchi, F.; Rota, M.; Marengoni, A.; Akbaritabar, A.; Squazzoni, F. The Effect of Social Relationships on Cognitive Decline in Older Adults: An Updated Systematic Review and Meta-Analysis of Longitudinal Cohort Studies. BMC Public. Health 2022, 22, 278. [Google Scholar] [CrossRef] [PubMed]
- Aroogh, M.D.; Shahboulaghi, F.M. Social Participation of Older Adults: A Concept Analysis. Int. J. Community Based Nurs. Midwifery 2020, 8, 55–72. [Google Scholar] [CrossRef]
- Levasseur, M.; Richard, L.; Gauvin, L.; Raymond, É. Inventory and Analysis of Definitions of Social Participation Found in the Aging Literature: Proposed Taxonomy of Social Activities. Soc. Sci. Med. 2010, 71, 2141–2149. [Google Scholar] [CrossRef] [PubMed]
- Lee, H.; Ang, S. Productive Activities and Risk of Cognitive Impairment and Depression: Does the Association Vary by Gender? Sociol. Perspect. 2020, 63, 608–629. [Google Scholar] [CrossRef] [PubMed]
- Santini, Z.I.; Jose, P.E.; Koyanagi, A.; Meilstrup, C.; Nielsen, L.; Madsen, K.R.; Koushede, V. Formal Social Participation Protects Physical Health through Enhanced Mental Health: A Longitudinal Mediation Analysis Using Three Consecutive Waves of the Survey of Health, Ageing and Retirement in Europe (SHARE). Soc. Sci. Med. 2020, 251, 112906. [Google Scholar] [CrossRef] [PubMed]
- Choi, Y.J.; Hong, Y.C.; Do, Y.K. The Effects of Social Activities and Living Arrangements on Cognitive Functions in Middle-Aged and Elderly Adults: A Panel Study Using the 2006-2018 Korean Longitudinal Study of Aging. J. Prev. Med. Public Health 2021, 54, 395–403. [Google Scholar] [CrossRef] [PubMed]
- Cohn-Schwartz, E. Pathways from Social Activities to Cognitive Functioning: The Role of Physical Activity and Mental Health. Innov. Aging 2020, 4, igaa015. [Google Scholar] [CrossRef] [PubMed]
- Corrêa, J.C.; Ávila, M.P.W.; Lucchetti, A.L.G.; Lucchetti, G. Altruism, Volunteering and Cognitive Performance Among Older Adults: A 2-Year Longitudinal Study. J. Geriatr. Psychiatry Neurol. 2022, 35, 66–77. [Google Scholar] [CrossRef]
- Kail, B.L.; Carr, D.C. More than Selection Effects: Volunteering Is Associated with Benefits in Cognitive Functioning. J. Gerontol. Ser. B 2020, 75, 1741–1746. [Google Scholar] [CrossRef] [PubMed]
- Tsuji, T.; Kanamori, S.; Miyaguni, Y.; Hanazato, M.; Kondo, K. Community-Level Sports Group Participation and the Risk of Cognitive Impairment. Med. Sci. Sports Exerc. 2019, 51, 2217–2223. [Google Scholar] [CrossRef]
- Lee, H.J.; Jang, J.; Choi, D.W.; Chae, W.; Park, E.C.; Jang, S.I. Association between Change in Lifestyle and Cognitive Functions among Elderly Koreans: Findings from the Korean Longitudinal Study of Aging (2006–2016). BMC Geriatr. 2020, 20, 317. [Google Scholar] [CrossRef] [PubMed]
- Min, J.W. A Longitudinal Study of Cognitive Trajectories and Its Factors for Koreans Aged 60 and over: A Latent Growth Mixture Model. Int. J. Geriatr. Psychiatry 2018, 33, 755–762. [Google Scholar] [CrossRef]
- Kim, Y. Risk and Protective Factors for the Onset of Cognitive Impairment in Korea: A 10-Year Longitudinal Panel Study. Psychiatry Investig. 2020, 17, 769–776. [Google Scholar] [CrossRef] [PubMed]
- Villalonga-Olives, E.; Majercak, K.R.; Almansa, J.; Khambaty, T. Longitudinal Impact of Volunteering on the Cognitive Functioning of Older Adults: A Secondary Analysis from the US Health and Retirement Study. Int. J. Nurs. Sci. 2023, 10, 373–382. [Google Scholar] [CrossRef]
- Litwin, H.; Stoeckel, K.J. Social Network, Activity Participation, and Cognition: A Complex Relationship. Res. Aging 2016, 38, 76–97. [Google Scholar] [CrossRef] [PubMed]
- Mackenzie, C.S.; Abdulrazaq, S. Social Engagement Mediates the Relationship between Participation in Social Activities and Psychological Distress among Older Adults. Aging Ment. Health 2021, 25, 299–305. [Google Scholar] [CrossRef]
- Hussain, B.; Mirza, M.; Baines, R.; Burns, L.; Stevens, S.; Asthana, S.; Chatterjee, A. Loneliness and Social Networks of Older Adults in Rural Communities: A Narrative Synthesis Systematic Review. Front. Public. Health 2023, 11, 1113864. [Google Scholar] [CrossRef]
- Umberson, D. Family Status and Health Behaviors: Social Control as a Dimension of Social Integration. J. Health Soc. Behav. 1987, 28, 306–319. [Google Scholar] [CrossRef]
- Cohn-Schwartz, E.; Levinsky, M.; Litwin, H. Social Network Type and Subsequent Cognitive Health among Older Europeans. Int. Psychogeriatr. 2021, 33, 495–504. [Google Scholar] [CrossRef]
- Hwang, J.; Park, S.; Kim, S. Effects of Participation in Social Activities on Cognitive Function Among Middle-Aged and Older Adults in Korea. Int. J. Environ. Res. Public. Health 2018, 15, 2315. [Google Scholar] [CrossRef] [PubMed]
- Yen, C.H.; Yeh, C.J.; Wang, C.C.; Liao, W.C.; Chen, S.C.; Chen, C.C.; Liang, J.; Lai, T.J.; Lin, H.S.; Lee, S.H.; et al. Determinants of Cognitive Impairment over Time among the Elderly in Taiwan: Results of the National Longitudinal Study. Arch. Gerontol. Geriatr. 2010, 50, S53–S57. [Google Scholar] [CrossRef] [PubMed]
- Tomioka, K.; Kurumatani, N.; Hosoi, H. Social Participation and Cognitive Decline among Community-Dwelling Older Adults: A Community-Based Longitudinal Study. J. Gerontol. Ser. B Psychol. Sci. Soc. Sci. 2018, 73, 799–806. [Google Scholar] [CrossRef]
- Page, M.J.; McKenzie, J.E.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Akl, E.A.; Brennan, S.E.; et al. The PRISMA 2020 Statement: An Updated Guideline for Reporting Systematic Reviews. BMJ 2021, 372, n71. [Google Scholar] [CrossRef] [PubMed]
- Kim, S.Y.; Park, J.E.; Lee, Y.J.; Seo, H.J.; Sheen, S.S.; Hahn, S.; Jang, B.H.; Son, H.J. Testing a Tool for Assessing the Risk of Bias for Nonrandomized Studies Showed Moderate Reliability and Promising Validity. J. Clin. Epidemiol. 2013, 66, 408–414. [Google Scholar] [CrossRef] [PubMed]
- Higgins, J.P.T.; Thomas, J.; Chandler, J.; Cumpston, M.; Li, T.; Page, M.J.; Welch, V.A. (Eds.) Cochrane Handbook for Systematic Reviews of Interventions, 2nd ed.; John Wiley & Sons: Chichester, UK, 2019; ISBN 9781119536628. [Google Scholar]
- DerSimonian, R.; Laird, N. Meta-Analysis in Clinical Trials. Control. Clin. Trials 1986, 7, 177–188. [Google Scholar] [CrossRef]
- Higgins, J.; Thompson, S.; Deeks, J.; Altman, D. Measuring Inconsistency in Meta-Analyses. Br. Med. J. 2003, 327, 557–560. [Google Scholar] [CrossRef]
- GRADE Working Group. Handbook for Grading the Quality of Evidence and the Strength of Recommendations: Using the GRADE Approach; Schünemann, H., Brożek, J., Guyatt, G., Oxman, A., Eds.; GRADE Working Group: Chicago, IL, USA, 2013. [Google Scholar]
- Afonso, J.; Ramirez-Campillo, R.; Clemente, F.M.; Büttner, F.C.; Andrade, R. The Perils of Misinterpreting and Misusing “Publication Bias” in Meta-Analyses: An Education Review on Funnel Plot-Based Methods. Sport. Med. 2024, 54, 257–269. [Google Scholar] [CrossRef]
- Choi, Y.; Park, S.; Cho, K.H.; Chun, S.Y.; Park, E.C. A Change in Social Activity Affect Cognitive Function in Middle-Aged and Older Koreans: Analysis of a Korean Longitudinal Study on Aging (2006–2012). Int. J. Geriatr. Psychiatry 2016, 31, 912–919. [Google Scholar] [CrossRef]
- Infurna, F.J.; Okun, M.A.; Grimm, K.J. Volunteering Is Associated with Lower Risk of Cognitive Impairment. J. Am. Geriatr. Soc. 2016, 64, 2263–2269. [Google Scholar] [CrossRef] [PubMed]
- Kim, D.H.; Arai, H.; Kim, S.H. Social Activities Are Associated with Cognitive Decline in Older Koreans. Geriatr. Gerontol. Int. 2017, 17, 1191–1196. [Google Scholar] [CrossRef] [PubMed]
- Lee, S.H.; Kim, Y.B. Which Type of Social Activities May Reduce Cognitive Decline in the Elderly?: A Longitudinal Population-Based Study. BMC Geriatr. 2016, 16, 165. [Google Scholar] [CrossRef] [PubMed]
- Proulx, C.M.; Curl, A.L.; Ermer, A.E. Longitudinal Associations Between Formal Volunteering and Cognitive Functioning. J. Gerontol. Ser. B 2018, 73, 522–531. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| Author (Year), Country | Data Source | Follow-Up Duration | Sample Size | Baseline Participant Characteristics | Cognitive Function Assessment (Outcome of Interest) | Formal Social Participation Assessment | Adjusted Confounders | Main Findings Reported in the Original Article | |
|---|---|---|---|---|---|---|---|---|---|
| Age (Mean ± SD; Range) | % Women | ||||||||
| Yen et al. (2010) [33], Taiwan | SHLSET | 10 | 1626 | 69.8 ± 4.9; 60+ | 59.2 | Dichotomous (no cognitive impairment/cognitive impairment); Measured with SPMSQ. | Dichotomous (no/yes); Assessment: joining an organized group activity; Assessed at baseline. | Age, sex, marital status, education, ethnicity, smoking, alcohol drinking, depression, hypertension, diabetes, cardiovascular disease, stroke, ADL disability, IADL disability, functional limitation, and self-perceived health. | Participating in organized group activities did not show any significant association with a decreased likelihood of cognitive impairment. |
| Infurna et al. (2016) [43], USA | HRS | 14 | 13,262 | 71.3 ± 8.3; 60–106 | 58 | Dichotomous (no cognitive impairment/cognitive impairment); Measure adapted from TICS. | Continuous variable; Assessment: change in the likelihood of volunteering; Assessed over time. | Age, sex, ethnicity, marital status, education, employment status, physical exercise, smoking, functional limitations, self-rated health, cardiovascular illnesses, and depressive symptoms. | Volunteering regularly over time was significantly associated with a decreased likelihood of cognitive impairment. |
| Kim et al. (2017) [44], Republic of Korea | KLoSA | 6 | 2495 | 71.2; 65–79 | 53.39 | Dichotomous (no cognitive decline/cognitive decline); Measured with K-MMSE. | Variable levels: 1, 2, 3+ activities; Assessment: religious groups; senior café; sports and leisure clubs; alumni groups; volunteering; political and non-governmental organizations; Assessed at baseline. | Age, sex, education, employment status, depression, IADL, and weight loss. | Greater participation in formal social activities was significantly associated with a decreased likelihood of cognitive decline. |
| Min (2018) [24], Republic of Korea | KLoSA | 6 | 2445 | 67.5 ± 5.6; 60–91 | 46 | Dichotomous (no cognitive decline/cognitive decline); Measured with K-MMSE. | Continuous variable (0 to 6); Assessment: church/religious groups, social clubs, sports clubs, alumni societies, volunteer groups, and political organizations; Assessed at baseline. | Age, sex, marital status, and education. | Increased participation in formal social activities was significantly associated with a decreased likelihood of cognitive decline. |
| Tomioka et al. (2018) [34], Japan | ------ | 3 | 6093 | 72.8; 65–96 | 54.6 | Dichotomous (no cognitive decline/cognitive decline); Measured with CPS. | Variable levels: 0, 1, 2, 3+ activities; Assessment: neighborhood associations, hobby groups, local event groups, senior citizen clubs, and volunteer groups; Assessed at baseline. | Age, family structure, BMI, pensions, number of medications used, self-reported medical conditions, alcohol consumption, smoking, depression, self-rated health, and IADLs. | In women, participating in three or more formal social activities was significantly associated with a decreased likelihood of cognitive decline, while no other associations were found. |
| Tsuji et al. (2019) [22], Japan | JAGES | 6 | 40,308 | 65+ | 51.31 | Dichotomous (no cognitive impairment/cognitive impairment); Measured with The Activities of Daily Living Independence Assessment Criteria for Elderly Individuals. | Dichotomous (frequency: 1+ day per month; no participation); Assessment: sports group participation. Assessed over time. | Age, sex, population density, annual sunlight hours, stroke, hypertension, diabetes, hearing loss, obesity, social isolation, drinking status, smoking status, education, income, depression, and walking time. | Higher prevalence of sports group participation showed a statistically significant relationship with lower risk of cognitive impairment. |
| Kim (2020) [25], Republic of Korea | KLoSA | 10 | 7568 | 56.01; 45+ | 48.16 | Dichotomous (no cognitive impairment/cognitive impairment); Measured with K-MMSE. | Variable levels: participating never or almost never, once or twice a month, almost every week+; Assessment: religious, friendship, leisure/sports, alumni, volunteer, and political associations; Assessed over time. | Age, sex, education, income, employment, marital status, location, physical activity, contact with friends, smoking, hypertension, diabetes, cerebrovascular and heart diseases, obesity, hearing loss. | Participating in formal social activities was significantly associated with a decreased likelihood of cognitive impairment. |
| Choi (2021) [18], Republic of Korea | KLoSA | 12 | 7568 | 45+ | 50.92 | Dichotomous (no cognitive decline/cognitive decline); Measured with K-MMSE. | Dichotomous (socially active: 1+ activity; socially inactive: none); Assessment: religious, social, sports/cultural/leisure groups, college programs, alumni groups, grand family associations, volunteering, political party, civil organizations, and interest groups. Assessed over time. | Age, sex, education, income, smoking, alcohol consumption, comorbidity, and depression. | Not participating in formal social activities showed a greater risk of overall cognitive decline. |
| Choi et al. (2016) [42], Republic of Korea | KLoSA | 6 | 6076 | 58.5 ± 9.5; 45–93 | 50.8 | Continuous (higher scores = better cognition); Measured with K-MMSE. | Variable levels: consistent non-participation, participation to no participation, no participation to participation, consistent participation; Assessment: religious, friendship, political organizations, leisure/ culture/sports clubs, family/school reunions, volunteer work; Assessed over time. | Age, sex, marital status, education, income, employment status, number of chronic diseases, regular exercise, and area of living. | The non-participation to participation and consistent participation groups exhibited significantly higher cognitive function scores than those with inconsistent participation in formal social activities. |
| Lee & Kim (2016) [45], Republic of Korea | KLoSA | 4 | 1568 | 71.06 ± 0.12; 65+ | 45.7 | Continuous (higher scores = better cognition); Measured with K-MMSE. | Variable levels: 0, 1, 2+ activities; Assessment: church or other religious groups; senior citizen clubs or senior centers; alumni societies or family councils; Assessed at baseline. | Age, sex, marital status, education, household income, living arrangement, residential area, comorbidities, ADL, IADL, quality of life, and depressive symptoms. | No significant association was found between participating in formal social activities and a decline in cognitive function scores. |
| Hwang et al. (2018) [32], Republic of Korea | KLoSA | 8 | 6706 | 58.1 ± 0.12; 45+ | 50.1 | Continuous (higher scores = better cognition); Measured with K-MMSE | Dichotomous variable (no/yes for each activity); Assessment: religious groups; social gatherings; alumni/clan gatherings; and volunteer work; Assessed at baseline. | Age, sex, education, income, employment status, marital status, region of residence, physical activity, smoking, alcohol use, limited activities of daily living, depression, and comorbidity. | No significant association was found between participating in formal social activities (all types) and cognitive function scores. |
| Proulx et al. (2018) [46], USA | HRS | 16 | 11,100 | 64.68 (0.12); 50+ | 51.97 | Continuous (higher scores = better cognition); Measure adapted from TICS. | Variable levels (hours volunteering in the past 12 months): 0 h, 1–99 h, 100–199 h, 200+ hours; Assessment: formal volunteering; Assessed over time. | Age, sex, race, ethnicity, marital status, household income, household wealth, IADL, self-rated health, depressive symptoms, and time. | Participating in formal volunteering is significantly associated with higher cognitive function scores. |
| Kail & Carr (2020) [21], USA | HRS | 16 | 27,485 | 66.66 ± 9.91; 50–105 | 59.8 | Continuous (higher scores = better cognition); Measure adapted from TICS. | Variable levels: no volunteering; low level; moderate level; and high level; Assessment: formal volunteering; Assessed over time. | Age, sex, ethnicity, education, marital status, self-rated health, disability, symptoms of depression, income, household wealth, and hours working per week. | A small portion of cognitive benefits from formal volunteering stems from volunteers’ higher cognitive levels. However, older volunteers maintain higher cognitive function scores even after accounting for this. |
| Lee et al. (2020) [23], Republic of Korea | KLoSA | 10 | 1806 | 65+ | ----- | Continuous (higher scores = better cognition); Measured with K-MMSE. | Variable levels: 0, 1, 2+ activities; Assessment: religious groups; friendship clubs; leisure or sports clubs; and political organizations; Assessed at baseline. | Age, employment, region of residence, marital status, living arrangement, education, income, chronic disease, depression, and disability status. | Participating in formal social activities is significantly associated with higher cognitive function scores in both men and women. |
| Corrêa et al. (2022) [20], Brazil | ------ | 2 | 291 | 69.64 ± 6.38; 65+ | 89.4 | Continuous (higher scores = better cognition); Measured with MMSE. | Continuous variable (number of days volunteered last month); Assessment: formal volunteering; Assessed at baseline. | Age, sex, marital status, education, family income, race, smoking, physical health, and mental health. | No significant association was found between volunteering and cognitive function scores. |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Cunha, C.; Voss, G.; Andrade, R.; Delerue-Matos, A. Is Formal Social Participation Associated with Cognitive Function in Middle-Aged and Older Adults? A Systematic Review with Meta-Analysis of Longitudinal Studies. Behav. Sci. 2024, 14, 262. https://doi.org/10.3390/bs14040262
Cunha C, Voss G, Andrade R, Delerue-Matos A. Is Formal Social Participation Associated with Cognitive Function in Middle-Aged and Older Adults? A Systematic Review with Meta-Analysis of Longitudinal Studies. Behavioral Sciences. 2024; 14(4):262. https://doi.org/10.3390/bs14040262
Chicago/Turabian StyleCunha, Cláudia, Gina Voss, Renato Andrade, and Alice Delerue-Matos. 2024. "Is Formal Social Participation Associated with Cognitive Function in Middle-Aged and Older Adults? A Systematic Review with Meta-Analysis of Longitudinal Studies" Behavioral Sciences 14, no. 4: 262. https://doi.org/10.3390/bs14040262
APA StyleCunha, C., Voss, G., Andrade, R., & Delerue-Matos, A. (2024). Is Formal Social Participation Associated with Cognitive Function in Middle-Aged and Older Adults? A Systematic Review with Meta-Analysis of Longitudinal Studies. Behavioral Sciences, 14(4), 262. https://doi.org/10.3390/bs14040262