
Empathy and Schizotypy: A Network Comparison of the Interpersonal Reactivity Index in High and Low Schizotypy Groups
 , ,
, ,  ,
, {kind=link}
{kind=link}
{kind=link}
Abstract
1. Introduction
2. Methods
2.1. Participants and Procedure
2.2. Measures
2.2.1. Schizotypy
2.2.2. Empathy
2.3. Data Analysis
2.3.1. Network Analysis
2.3.2. Network Centrality
2.3.3. Network Stability and Accuracy
2.3.4. Network Comparison
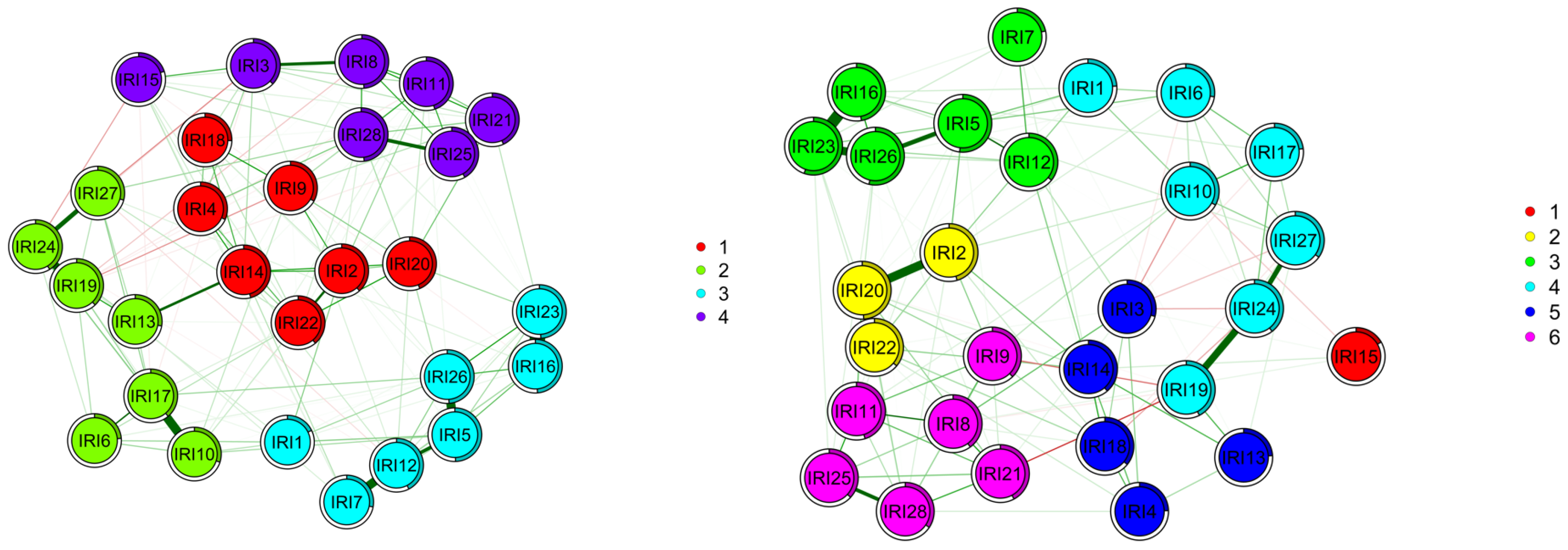
2.3.5. Network Community Detection
3. Results
3.1. Descriptive Statistics
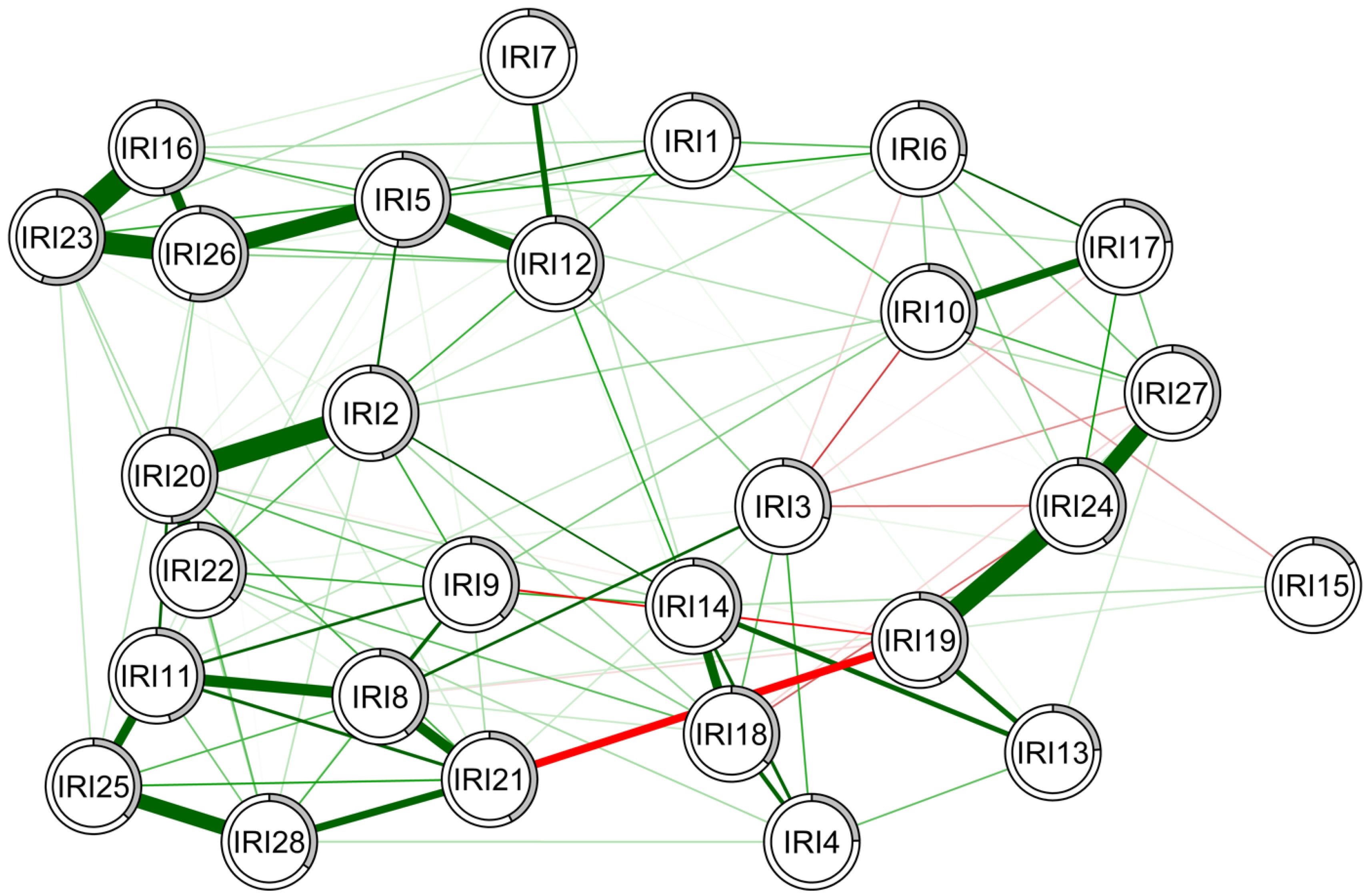
3.2. Network of Interpersonal Reactivity Index Items in the Low Schizotypy Group
3.3. Network of Interpersonal Reactivity Index Items in the High Schizotypy Group
3.4. Network Comparison of the Interpersonal Reactivity Index Items between the High and Low Schizotypy Groups
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Davis, M.H. A multidimensional approach to individual differences in empathy. JSAS Cat. Sel. Doc. Psychol. 1980, 10, 85. [Google Scholar]
- Davis, M.H. Empathy: A Social Psychological Approach; Routledge: London, UK, 2018. [Google Scholar]
- Thompson, N.M.; Van Reekum, C.M.; Chakrabarti, B. Cognitive and affective empathy relate differentially to emotion regulation. Affect. Sci. 2022, 3, 118–134. [Google Scholar] [CrossRef]
- Coll, M.-P.; Viding, E.; Rütgen, M.; Silani, G.; Lamm, C.; Catmur, C.; Bird, G. Are we really measuring empathy? Proposal for a new measurement framework. Neurosci. Biobehav. Rev. 2017, 83, 132–139. [Google Scholar] [CrossRef]
- Decety, J.; Jackson, P.L. The functional architecture of human empathy. Behav. Cogn. Neurosci. Rev. 2004, 3, 71–100. [Google Scholar] [CrossRef] [PubMed]
- Decety, J.; Jackson, P.L. A social-neuroscience perspective on empathy. Curr. Dir. Psychol. Sci. 2006, 15, 54–58. [Google Scholar] [CrossRef]
- Stosic, M.D.; Fultz, A.A.; Brown, J.A.; Bernieri, F.J. What is your empathy scale not measuring? The convergent, discriminant, and predictive validity of five empathy scales. J. Soc. Psychol. 2022, 162, 7–25. [Google Scholar] [CrossRef] [PubMed]
- Davis, M.H. Measuring individual differences in empathy: Evidence for a multidimensional approach. J. Personal. Soc. Psychol. 1983, 44, 113. [Google Scholar] [CrossRef]
- de Lima, F.F.; Osório, F.d.L. Empathy: Assessment instruments and psychometric quality—A systematic literature review with a meta-analysis of the past ten years. Front. Psychol. 2021, 12, 781346. [Google Scholar] [CrossRef] [PubMed]
- Beven, J.P.; O’Brien-Malone, A.; Hall, G. Using the interpersonal reactivity index to assess empathy in violent offenders. Int. J. Forensic Psychol. 2004, 1, 33–41. [Google Scholar]
- De Corte, K.; Buysse, A.; Verhofstadt, L.L.; Roeyers, H.; Ponnet, K.; Davis, M.H. Measuring empathic tendencies: Reliability and validity of the Dutch version of the Interpersonal Reactivity Index. Psychol. Belg. 2007, 47, 235. [Google Scholar] [CrossRef]
- Gilet, A.L.; Mella, N.; Studer, J.; Grühn, D.; Labouvie-Vief, G. Assessing dispositional empathy in adults: A French validation of the Interpersonal Reactivity Index (IRI). Can. J. Behav. Sci. Can. Sci. Comport. 2013, 45, 42. [Google Scholar] [CrossRef]
- Hawk, S.T.; Keijsers, L.; Branje, S.J.; der Graaff, J.V.; de Wied, M.; Meeus, W. Examining the interpersonal reactivity index (IRI) among early and late adolescents and their mothers. J. Personal. Assess. 2013, 95, 96–106. [Google Scholar] [CrossRef] [PubMed]
- Siu, A.M.; Shek, D.T. Validation of the interpersonal reactivity index in a Chinese context. Res. Soc. Work Pract. 2005, 15, 118–126. [Google Scholar] [CrossRef]
- Bonfils, K.A.; Longenecker, J.M.; Hammer, L.A.; Luther, L. Measuring empathy in groups with high schizotypy: Psychometric evaluation of the Interpersonal Reactivity Index. Psychol. Assess. 2022, 34, 459. [Google Scholar] [CrossRef] [PubMed]
- Pulos, S.; Elison, J.; Lennon, R. The hierarchical structure of the Interpersonal Reactivity Index. Soc. Behav. Personal. Int. J. 2004, 32, 355–359. [Google Scholar] [CrossRef]
- Eisenberg, N.; Miller, P.A. The relation of empathy to prosocial and related behaviors. Psychol. Bull. 1987, 101, 91. [Google Scholar] [CrossRef]
- Hoffman, M.L. Is altruism part of human nature? J. Personal. Soc. Psychol. 1981, 40, 121. [Google Scholar] [CrossRef]
- Hoffman, M.L. Empathy and Moral Development: Implications for Caring and Justice; Cambridge University Press: Cambridge, UK, 2001. [Google Scholar]
- McCullough, M.E.; Worthington, E.L., Jr.; Rachal, K.C. Interpersonal forgiving in close relationships. J. Personal. Soc. Psychol. 1997, 73, 321. [Google Scholar] [CrossRef]
- McCullough, M.E.; Rachal, K.C.; Sandage, S.J.; Worthington, E.L., Jr.; Brown, S.W.; Hight, T.L. Interpersonal forgiving in close relationships: II. Theoretical elaboration and measurement. J. Personal. Soc. Psychol. 1998, 75, 1586. [Google Scholar] [CrossRef]
- Sallquist, J.; Eisenberg, N.; Spinrad, T.L.; Eggum, N.D.; Gaertner, B.M. Assessment of preschoolers’ positive empathy: Concurrent and longitudinal relations with positive emotion, social competence, and sympathy. J. Posit. Psychol. 2009, 4, 223–233. [Google Scholar] [CrossRef]
- Bonfils, K.A.; Lysaker, P.H.; Minor, K.S.; Salyers, M.P. Affective empathy in schizophrenia: A meta-analysis. Schizophr. Res. 2016, 175, 109–117. [Google Scholar] [CrossRef]
- Bonfils, K.A.; Lysaker, P.H.; Minor, K.S.; Salyers, M.P. Empathy in schizophrenia: A meta-analysis of the Interpersonal Reactivity Index. Psychiatry Res. 2017, 249, 293–303. [Google Scholar] [CrossRef] [PubMed]
- Brissos, S.; Dias, V.V.; Balanzá-Martinez, V.; Carita, A.I.; Figueira, M.L. Symptomatic remission in schizophrenia patients: Relationship with social functioning, quality of life, and neurocognitive performance. Schizophr. Res. 2011, 129, 133–136. [Google Scholar] [CrossRef] [PubMed]
- Erol, A.; Delibas, H.; Bora, O.; Mete, L. The impact of insight on social functioning in patients with schizophrenia. Int. J. Soc. Psychiatry 2015, 61, 379–385. [Google Scholar] [CrossRef]
- Hooker, C.; Park, S. Emotion processing and its relationship to social functioning in schizophrenia patients. Psychiatry Res. 2002, 112, 41–50. [Google Scholar] [CrossRef]
- Meesters, P.D.; Stek, M.L.; Comijs, H.C.; de Haan, L.; Patterson, T.L.; Eikelenboom, P.; Beekman, A.T. Social functioning among older community-dwelling patients with schizophrenia: A review. Am. J. Geriatr. Psychiatry 2010, 18, 862–878. [Google Scholar] [CrossRef]
- Kuis, D.J.; van de Giessen, T.; de Jong, S.; Sportel, B.E.; Boonstra, N.; van Donkersgoed, R.; Lysaker, P.H.; Hasson-Ohayon, I.; Pijnenborg, G.H.M. Empathy and its relationship with social functioning in individuals at ultra-high risk for psychosis. Front. Psychiatry 2021, 12, 730092. [Google Scholar] [CrossRef]
- Montag, C.; Brandt, L.; Lehmann, A.; De Millas, W.; Falkai, P.; Gaebel, W.; Hasan, A.; Hellmich, M.; Janssen, B.; Gallinat, J.; et al. Cognitive and emotional empathy in individuals at clinical high risk of psychosis. Acta Psychiatr. Scand. 2020, 142, 40–51. [Google Scholar] [CrossRef] [PubMed]
- Henry, J.D.; Bailey, P.E.; Rendell, P.G. Empathy, social functioning and schizotypy. Psychiatry Res. 2008, 160, 15–22. [Google Scholar] [CrossRef] [PubMed]
- Pflum, M.J.; Gooding, D.C. Context matters: Social cognition task performance in psychometric schizotypes. Psychiatry Res. 2018, 264, 398–403. [Google Scholar] [CrossRef] [PubMed]
- Wang, Y.; Neumann, D.L.; Shum, D.H.; Liu, W.-H.; Shi, H.-S.; Yan, C.; Lui, S.S.; Zhang, Q.; Li, Z.; Cheung, E.F.; et al. Cognitive empathy partially mediates the association between negative schizotypy traits and social functioning. Psychiatry Res. 2013, 210, 62–68. [Google Scholar] [CrossRef] [PubMed]
- Grant, P.; Green, M.J.; Mason, O.J. Models of schizotypy: The importance of conceptual clarity. Schizophr. Bull. 2018, 44 (Suppl. S2), S556–S563. [Google Scholar] [CrossRef] [PubMed]
- Lenzenweger, M.F. Thinking clearly about schizotypy: Hewing to the schizophrenia liability core, considering interesting tangents, and avoiding conceptual quicksand. Schizophr. Bull. 2015, 41 (Suppl. S2), S483–S491. [Google Scholar] [CrossRef] [PubMed]
- Bora, E. Theory of mind and schizotypy: A meta-analysis. Schizophr. Res. 2020, 222, 97–103. [Google Scholar] [CrossRef] [PubMed]
- Borsboom, D. A network theory of mental disorders. World Psychiatry 2017, 16, 5–13. [Google Scholar] [CrossRef]
- Borsboom, D.; Cramer, A.O. Network analysis: An integrative approach to the structure of psychopathology. Annu. Rev. Clin. Psychol. 2013, 9, 91–121. [Google Scholar] [CrossRef]
- Dodell-Feder, D.; Saxena, A.; Rutter, L.; Germine, L. The network structure of schizotypal personality traits in a population-based sample. Schizophr. Res. 2019, 208, 258–267. [Google Scholar] [CrossRef]
- Van Borkulo, C.; Epskamp, S.; Milner, A. Network Comparison Test: Permutation-Based Test of Differences in Strength of Networks. Available online: https://cran.r-project.org/web/packages/NetworkComparisonTest/NetworkComparisonTest.pdf (accessed on 1 September 2023).
- Briganti, G.; Kempenaers, C.; Braun, S.; Fried, E.I.; Linkowski, P. Network analysis of empathy items from the interpersonal reactivity index in 1973 young adults. Psychiatry Res. 2018, 265, 87–92. [Google Scholar] [CrossRef]
- Wang, Y.; Shi, H.-S.; Liu, W.-H.; Zheng, H.; Wong, K.K.-Y.; Cheung, E.F.; Chan, R.C. Applying network analysis to investigate the links between dimensional schizotypy and cognitive and affective empathy. J. Affect. Disord. 2020, 277, 313–321. [Google Scholar] [CrossRef] [PubMed]
- Chapman, L.J.; Chapman, J.P. Infrequency Scale; Unpublished Test; University of Wisconsin: Madison, WI, USA, 1983. [Google Scholar]
- Hammer, L.A.; Springfield, C.R.; Tighe, C.A.; Oswalt, S.; Bonfils, K.A. Schizotypy Moderates the Relationship Between Sleep Quality and Social Cognition. J. Nerv. Ment. Dis. 2023, 212, 133–140. [Google Scholar] [CrossRef] [PubMed]
- Luther, L.; Coffin, G.M.; Firmin, R.L.; Bonfils, K.A.; Minor, K.S.; Salyers, M.P. A test of the cognitive model of negative symptoms: Associations between defeatist performance beliefs, self-efficacy beliefs, and negative symptoms in a non-clinical sample. Psychiatry Res. 2018, 269, 278–285. [Google Scholar] [CrossRef]
- Cohen, A.S.; Matthews, R.A.; Najolia, G.M.; Brown, L.A. Toward a more psychometrically sound brief measure of schizotypal traits: Introducing the SPQ-Brief Revised. J. Personal. Disord. 2010, 24, 516–537. [Google Scholar] [CrossRef] [PubMed]
- Callaway, D.A.; Cohen, A.S.; Matthews, R.A.; Dinzeo, T. Schizotypal Personality Questionnaire—Brief Revised: Psychometric replication and extension. Personal. Disord. Theory Res. Treat. 2014, 5, 32. [Google Scholar] [CrossRef] [PubMed]
- Minor, K.S.; Firmin, R.L.; Bonfils, K.A.; Chun, C.A.; Buckner, J.D.; Cohen, A.S. Predicting creativity: The role of psychometric schizotypy and cannabis use in divergent thinking. Psychiatry Res. 2014, 220, 205–210. [Google Scholar] [CrossRef] [PubMed]
- Gooding, D.C.; Tallent, K.A.; Matts, C.W. Clinical status of at-risk individuals 5 years later: Further validation of the psychometric high-risk strategy. J. Abnorm. Psychol. 2005, 114, 170. [Google Scholar] [CrossRef] [PubMed]
- Korfine, L.; Lenzenweger, M.F. The taxonicity of schizotypy: A replication. J. Abnorm. Psychol. 1995, 104, 26. [Google Scholar] [CrossRef] [PubMed]
- Curran, P.J.; West, S.G.; Finch, J.F. The robustness of test statistics to nonnormality and specification error in confirmatory factor analysis. Psychol. Methods 1996, 1, 16–29. [Google Scholar] [CrossRef]
- Tibshirani, R. Regression shrinkage and selection via the lasso. J. R. Stat. Soc. Ser. B Stat. Methodol. 1996, 58, 267–288. [Google Scholar] [CrossRef]
- Chen, J.; Chen, Z. Extended Bayesian information criteria for model selection with large model spaces. Biometrika 2008, 95, 759–771. [Google Scholar] [CrossRef]
- Epskamp, S.; Borsboom, D.; Fried, E.I. Estimating psychological networks and their accuracy: A tutorial paper. Behav. Res. Methods 2018, 50, 195–212. [Google Scholar] [CrossRef]
- Epskamp, S.; Cramer, A.O.; Waldorp, L.J.; Schmittmann, V.D.; Borsboom, D. qgraph: Network visualizations of relationships in psychometric data. J. Stat. Softw. 2012, 48, 1–18. [Google Scholar] [CrossRef]
- R Core Team. R: A Language and Environment for Statistical Computing; R Foundation for Statistical Computing: Vienna, Austria, 2019. [Google Scholar]
- Opsahl, T.; Agneessens, F.; Skvoretz, J. Node centrality in weighted networks: Generalizing degree and shortest paths. Soc. Netw. 2010, 32, 245–251. [Google Scholar] [CrossRef]
- Robinaugh, D.J.; Millner, A.J.; McNally, R.J. Identifying highly influential nodes in the complicated grief network. J. Abnorm. Psychol. 2016, 125, 747. [Google Scholar] [CrossRef]
- Csardi, G.; Nepusz, T. The igraph software package for complex network research. Int. J. Complex. Syst. 2006, 1695, 1–9. [Google Scholar]
- Reichardt, J.; Bornholdt, S. Statistical mechanics of community detection. Phys. Rev. E 2006, 74, 016110. [Google Scholar] [CrossRef]
- Smith, N.R.; Zivich, P.N.; Frerichs, L.M.; Moody, J.; Aiello, A.E. A guide for choosing community detection algorithms in social network studies: The question alignment approach. Am. J. Prev. Med. 2020, 59, 597–605. [Google Scholar] [CrossRef]
- Christensen, A.P.; Garrido, L.E.; Guerra-Peña, K.; Golino, H. Comparing community detection algorithms in psychometric networks: A Monte Carlo simulation. Behav. Res. Methods 2023, 1–21. [Google Scholar] [CrossRef] [PubMed]
- Chrysikou, E.G.; Thompson, W.J. Assessing cognitive and affective empathy through the interpersonal reactivity index: An argument against a two-factor model. Assessment 2016, 23, 769–777. [Google Scholar] [CrossRef] [PubMed]
- Blain, S.D.; Longenecker, J.M.; Grazioplene, R.G.; Klimes-Dougan, B.; DeYoung, C.G. Apophenia as the disposition to false positives: A unifying framework for openness and psychoticism. J. Abnorm. Psychol. 2020, 129, 279. [Google Scholar] [CrossRef]
- Kotov, R.; Jonas, K.G.; Carpenter, W.T.; Dretsch, M.N.; Eaton, N.R.; Forbes, M.K.; Forbush, K.T.; Hobbs, K.; Reininghaus, U.; Slade, T.; et al. Validity and utility of hierarchical taxonomy of psychopathology (HiTOP): I. Psychosis superspectrum. World Psychiatry 2020, 19, 151–172. [Google Scholar] [CrossRef] [PubMed]
- Tellegen, A.; Atkinson, G. Openness to absorbing and self-altering experiences (“absorption”), a trait related to hypnotic susceptibility. J. Abnorm. Psychol. 1974, 83, 268. [Google Scholar] [CrossRef]
- Horan, W.P.; Reise, S.P.; Kern, R.S.; Lee, J.; Penn, D.L.; Green, M.F. Structure and correlates of self-reported empathy in schizophrenia. J. Psychiatr. Res. 2015, 66, 60–66. [Google Scholar] [CrossRef]
- Karnick, A.T.; Fergerson, A.K.; Caulfield, N.M.; Buerke, M.; Albanese, B.J.; Schmidt, N.B.; Capron, D.W. Toward an integrative model of transdiagnostic risk factors and suicide: A network comparison of psychiatric outpatients. J. Psychiatr. Res. 2022, 154, 252–260. [Google Scholar] [CrossRef]
- Karyakina, M.; Shmukler, A. Network analysis of cognitive deficit in patients with schizophrenia spectrum disorders. Schizophr. Res. Cogn. 2021, 26, 100213. [Google Scholar] [CrossRef]
- Campellone, T.R.; Elis, O.; Mote, J.; Sanchez, A.H.; Kring, A.M. Negative symptoms in psychometrically defined schizotypy: The role of depressive symptoms. Psychiatry Res. 2016, 240, 181–186. [Google Scholar] [CrossRef] [PubMed]
- Dinzeo, T.J.; Thayasivam, U. Schizotypy, lifestyle behaviors, and health indicators in a young adult sample. Behav. Sci. 2021, 11, 179. [Google Scholar] [CrossRef] [PubMed]
- Ödéhn, N.; Goulding, A. Schizotypy and mental health in women and men from the general population. Nord. Psychol. 2018, 70, 198–208. [Google Scholar] [CrossRef]
- Chun, C.A.; Minor, K.S.; Cohen, A.S. Neurocognition in psychometrically defined college schizotypy samples: We are not measuring the “right stuff”. J. Int. Neuropsychol. Soc. 2013, 19, 324–337. [Google Scholar] [CrossRef] [PubMed]
- Wang, Y.; Shi, H.S.; Liu, W.H.; Xie, D.J.; Geng, F.L.; Yan, C.; Wang, Y.; Xiao, Y.H.; So, S.H.W.; Chan, R.C.; et al. Trajectories of schizotypy and their emotional and social functioning: An 18-month follow-up study. Schizophr. Res. 2018, 193, 384–390. [Google Scholar] [CrossRef] [PubMed]
- Chabrol, H.; Bronchain, J.; Debbané, M.; Chassagne, J.; Raynal, P. Borderline and schizotypal traits in college students: Relationship and personality profiles. Bull. Menn. Clin. 2020, 84, 299–318. [Google Scholar] [CrossRef] [PubMed]
- Yang, H.X.; Shi, H.S.; Ni, K.; Wang, Y.; Cheung, E.F.; Chan, R.C. Exploring the links between alexithymia, empathy and schizotypy in college students using network analysis. Cogn. Neuropsychiatry 2020, 25, 245–253. [Google Scholar] [CrossRef] [PubMed]
- Lawrence, E.J.; Shaw, P.; Baker, D.; Baron-Cohen, S.; David, A.S. Measuring empathy: Reliability and validity of the Empathy Quotient. Psychol. Med. 2004, 34, 911–920. [Google Scholar] [CrossRef] [PubMed]
- Reniers, R.L.; Corcoran, R.; Drake, R.; Shryane, N.M.; Völlm, B.A. The QCAE: A questionnaire of cognitive and affective empathy. J. Personal. Assess. 2011, 93, 84–95. [Google Scholar] [CrossRef] [PubMed]
- Batchelder, L.; Brosnan, M.; Ashwin, C. The development and validation of the empathy components questionnaire (ECQ). PLoS ONE 2017, 12, e0169185. [Google Scholar] [CrossRef]
- Drollinger, T.; Comer, L.B.; Warrington, P.T. Development and validation of the active empathetic listening scale. Psychol. Mark. 2006, 23, 161–180. [Google Scholar] [CrossRef]
- Dziobek, I.; Rogers, K.; Fleck, S.; Bahnemann, M.; Heekeren, H.R.; Wolf, O.T.; Convit, A. Multifaceted Empathy Test. J. Autism Dev. Disord. 2007, 38, 464–473. [Google Scholar] [CrossRef]
- Lindeman, M.; Koirikivi, I.; Lipsanen, J. Pictorial Empathy Test (PET). Eur. J. Psychol. Assess. 2016, 34, 421–431. [Google Scholar] [CrossRef]

Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Hammer, L.A.; Karnick, A.; Beals, K.; Luther, L.; Bonfils, K.A. Empathy and Schizotypy: A Network Comparison of the Interpersonal Reactivity Index in High and Low Schizotypy Groups. Behav. Sci. 2024, 14, 245. https://doi.org/10.3390/bs14030245
Hammer LA, Karnick A, Beals K, Luther L, Bonfils KA. Empathy and Schizotypy: A Network Comparison of the Interpersonal Reactivity Index in High and Low Schizotypy Groups. Behavioral Sciences. 2024; 14(3):245. https://doi.org/10.3390/bs14030245
Chicago/Turabian StyleHammer, Lillian A., Aleksandr Karnick, Kendall Beals, Lauren Luther, and Kelsey A. Bonfils. 2024. "Empathy and Schizotypy: A Network Comparison of the Interpersonal Reactivity Index in High and Low Schizotypy Groups" Behavioral Sciences 14, no. 3: 245. https://doi.org/10.3390/bs14030245
APA StyleHammer, L. A., Karnick, A., Beals, K., Luther, L., & Bonfils, K. A. (2024). Empathy and Schizotypy: A Network Comparison of the Interpersonal Reactivity Index in High and Low Schizotypy Groups. Behavioral Sciences, 14(3), 245. https://doi.org/10.3390/bs14030245