
Preventive Effect of a 7-Week App-Based Passive Psychoeducational Stress Management Program on Students


Abstract
1. Introduction
2. Materials and Methods
2.1. Measurements
2.1.1. Mental Health
2.1.2. Coping Style
2.1.3. Emotion Regulation
2.1.4. Questionnaire about Satisfaction with Each Module and Adherence to Psychoeducation
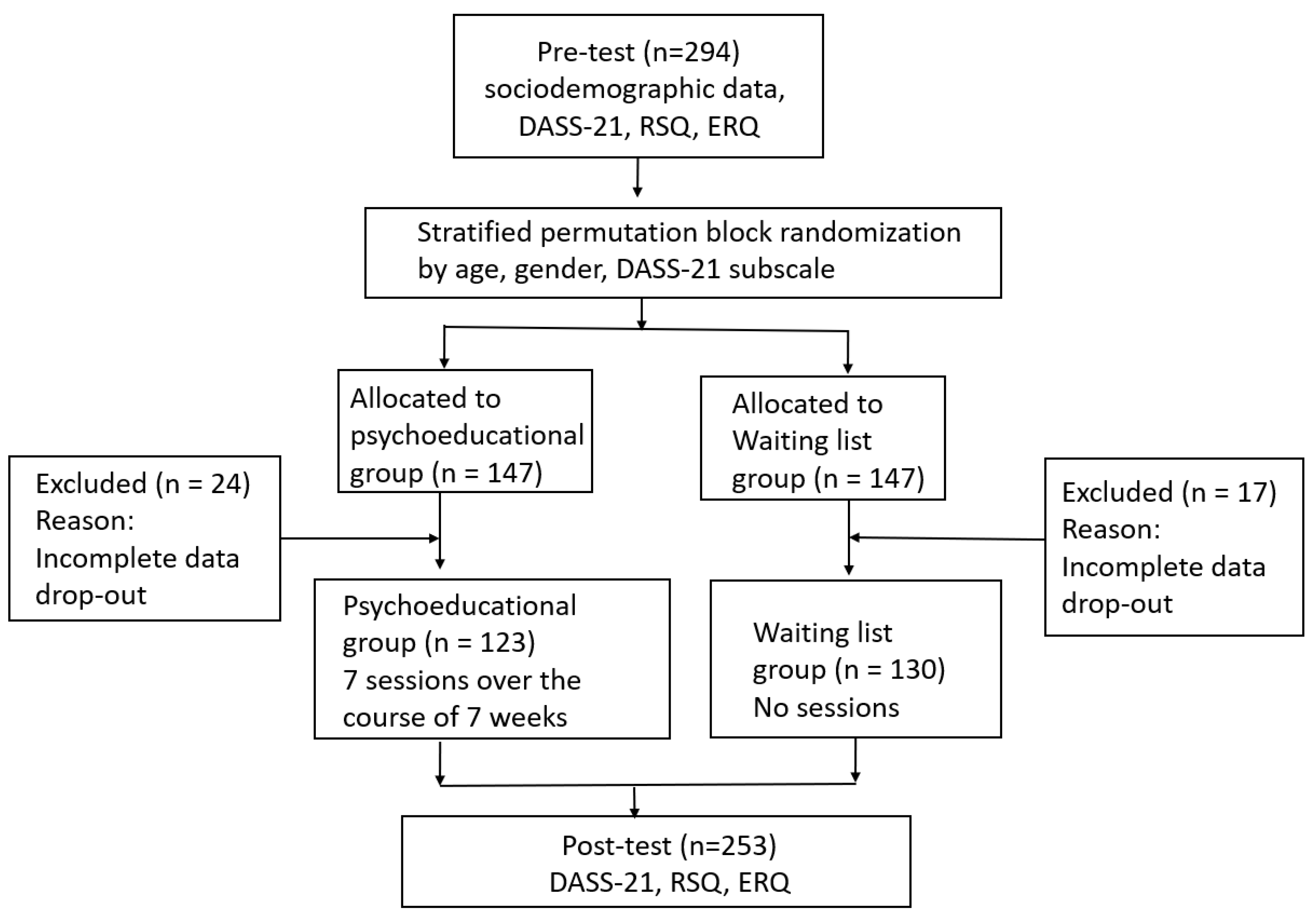
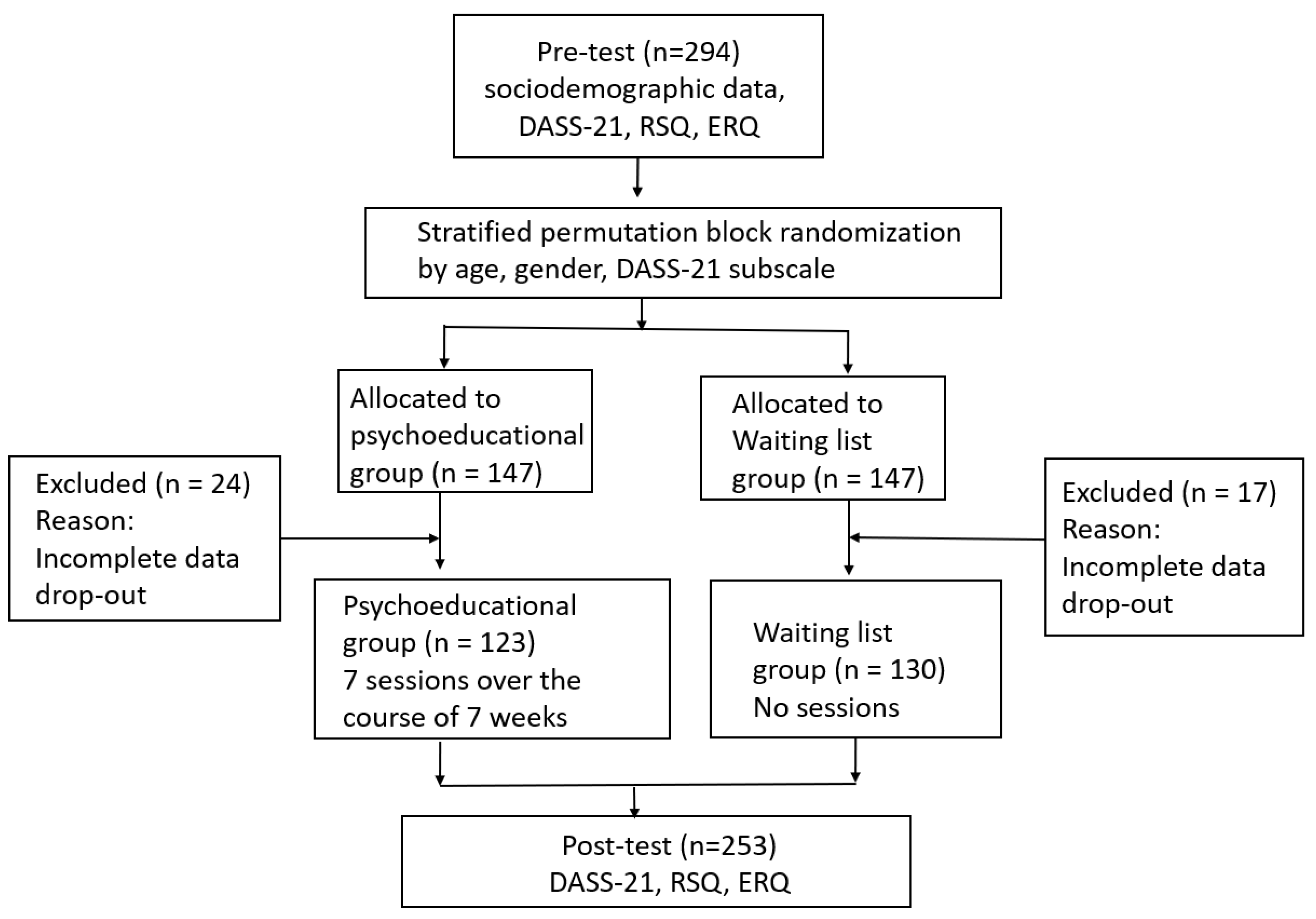
2.2. Procedure
2.3. Statistical Analyses
3. Results
3.1. Mental Health
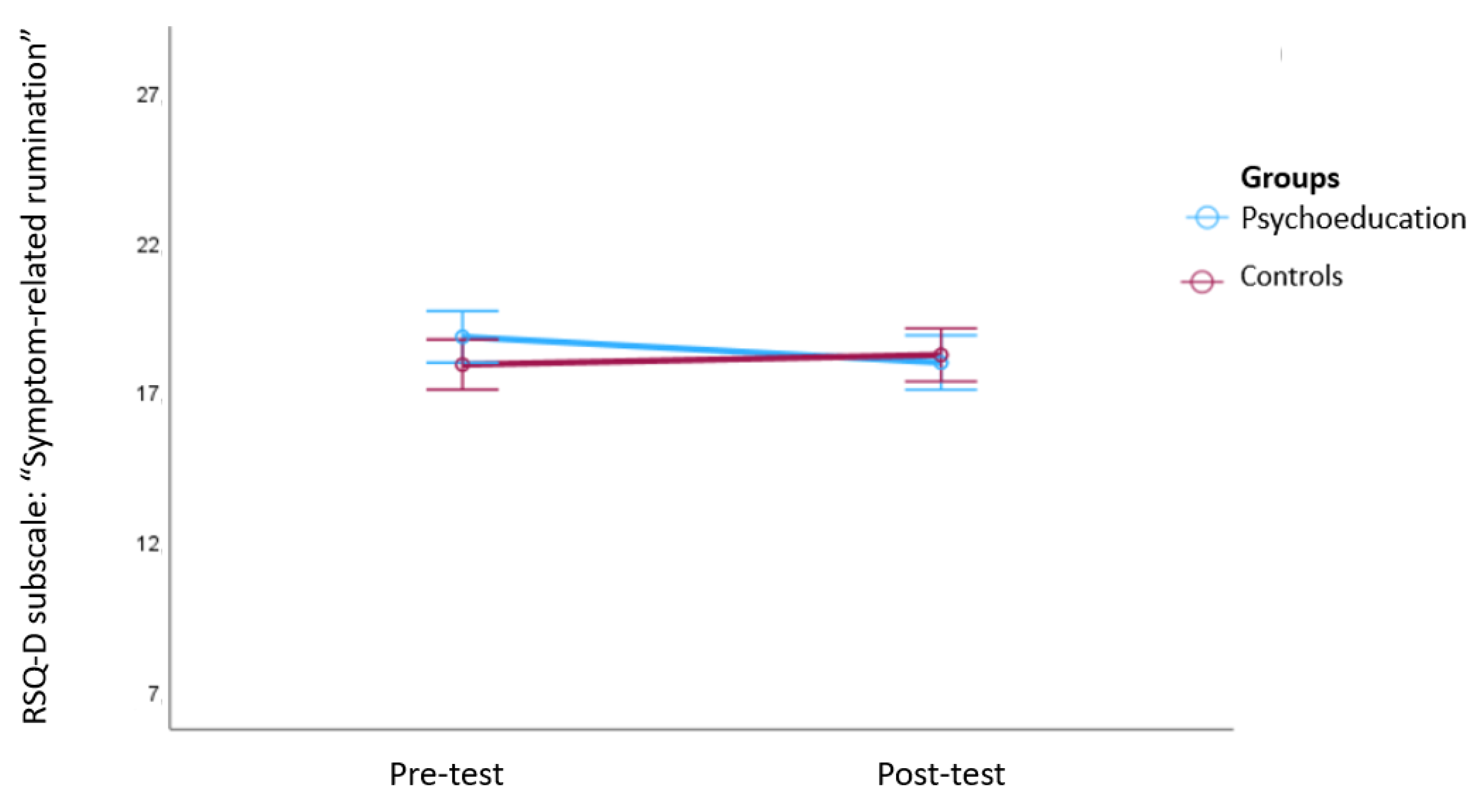
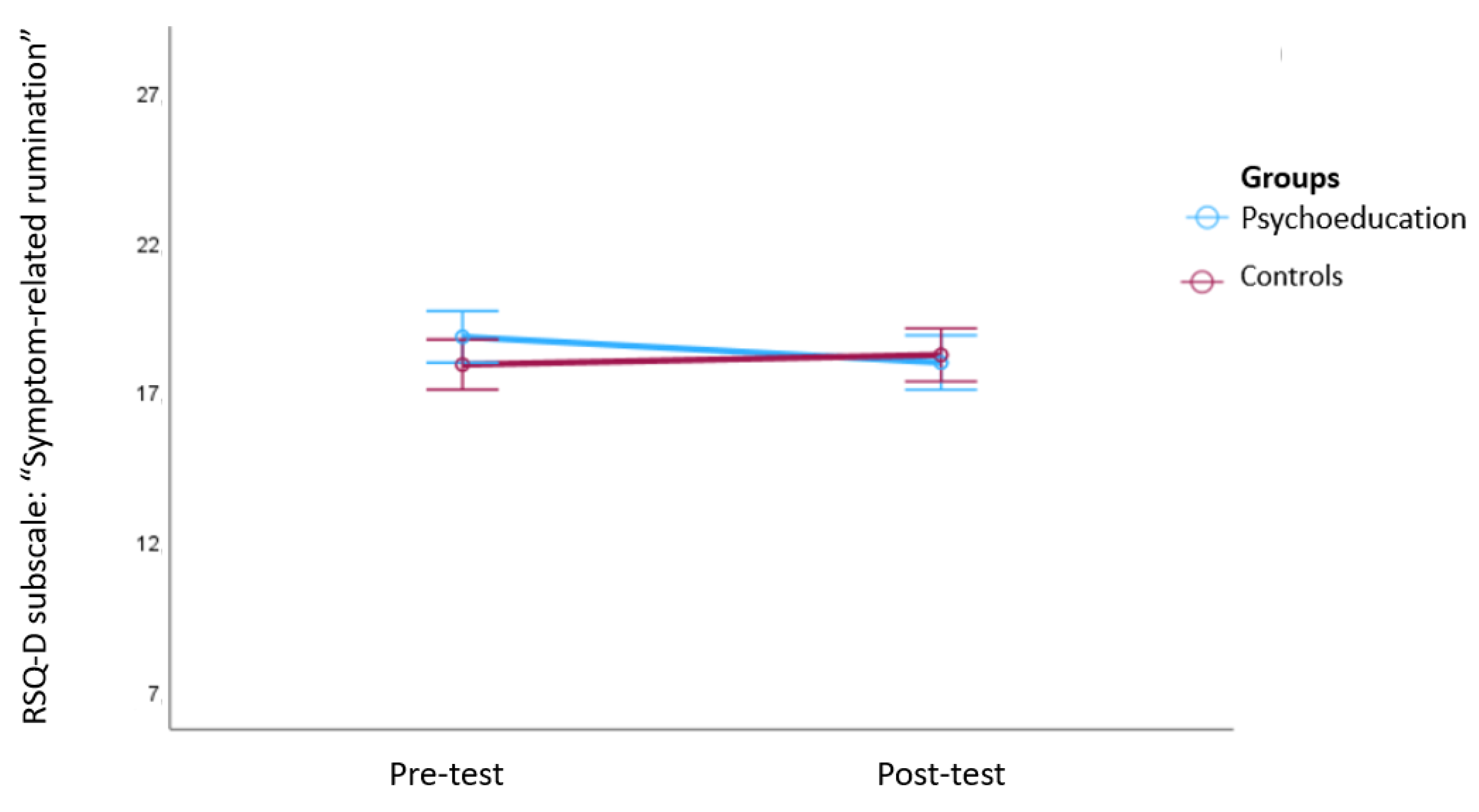
3.2. Coping Style
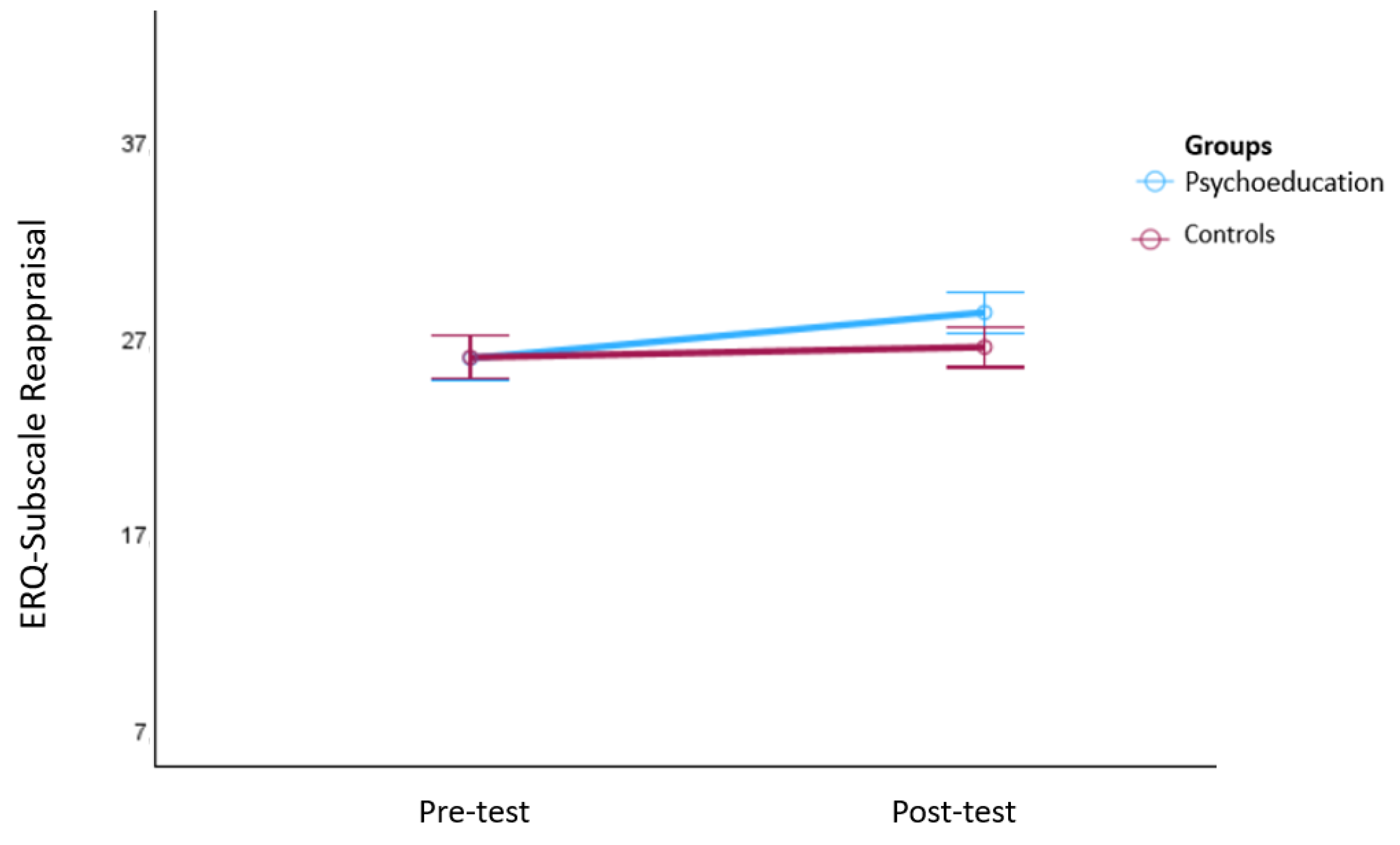
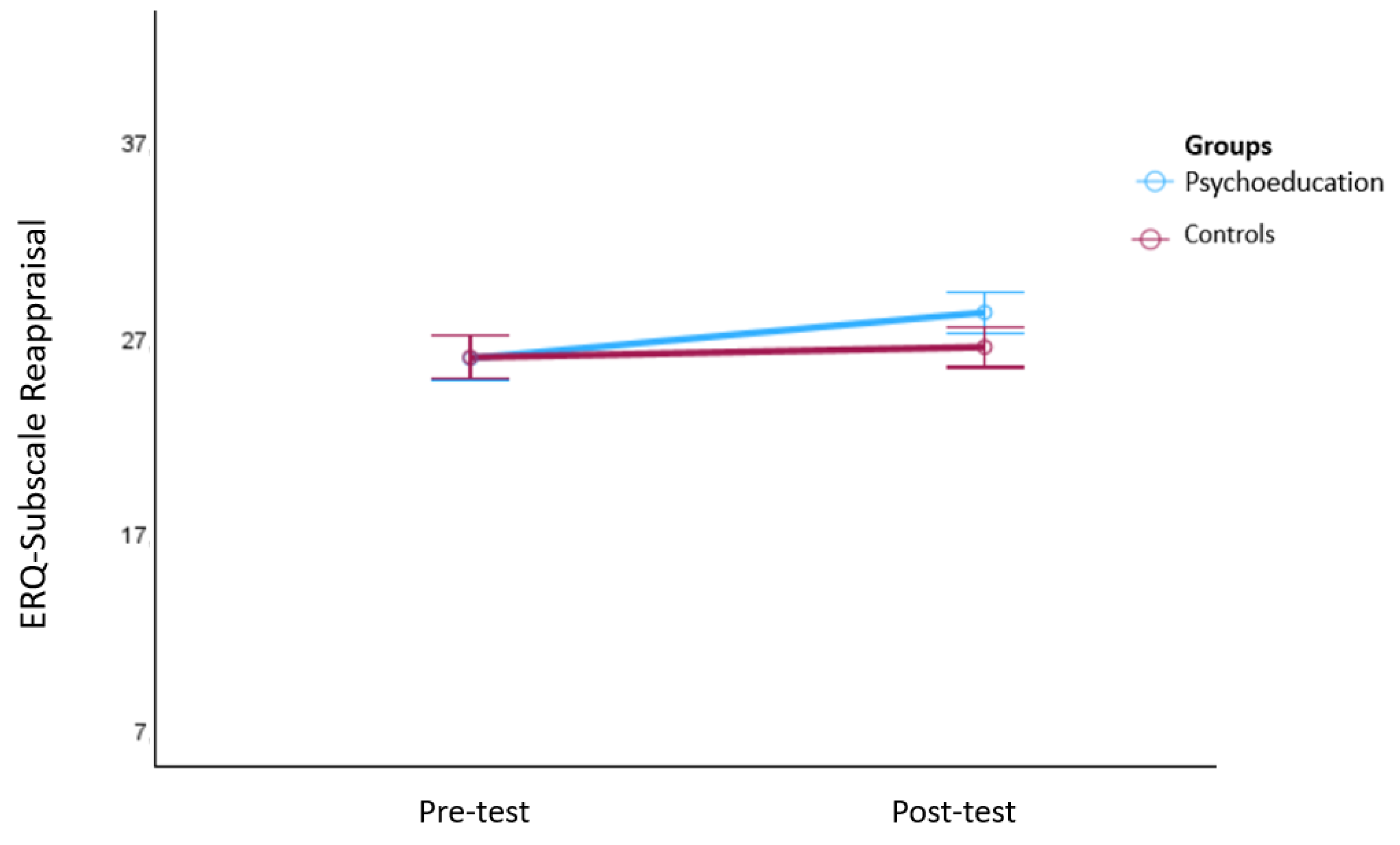
3.3. Emotion Regulation
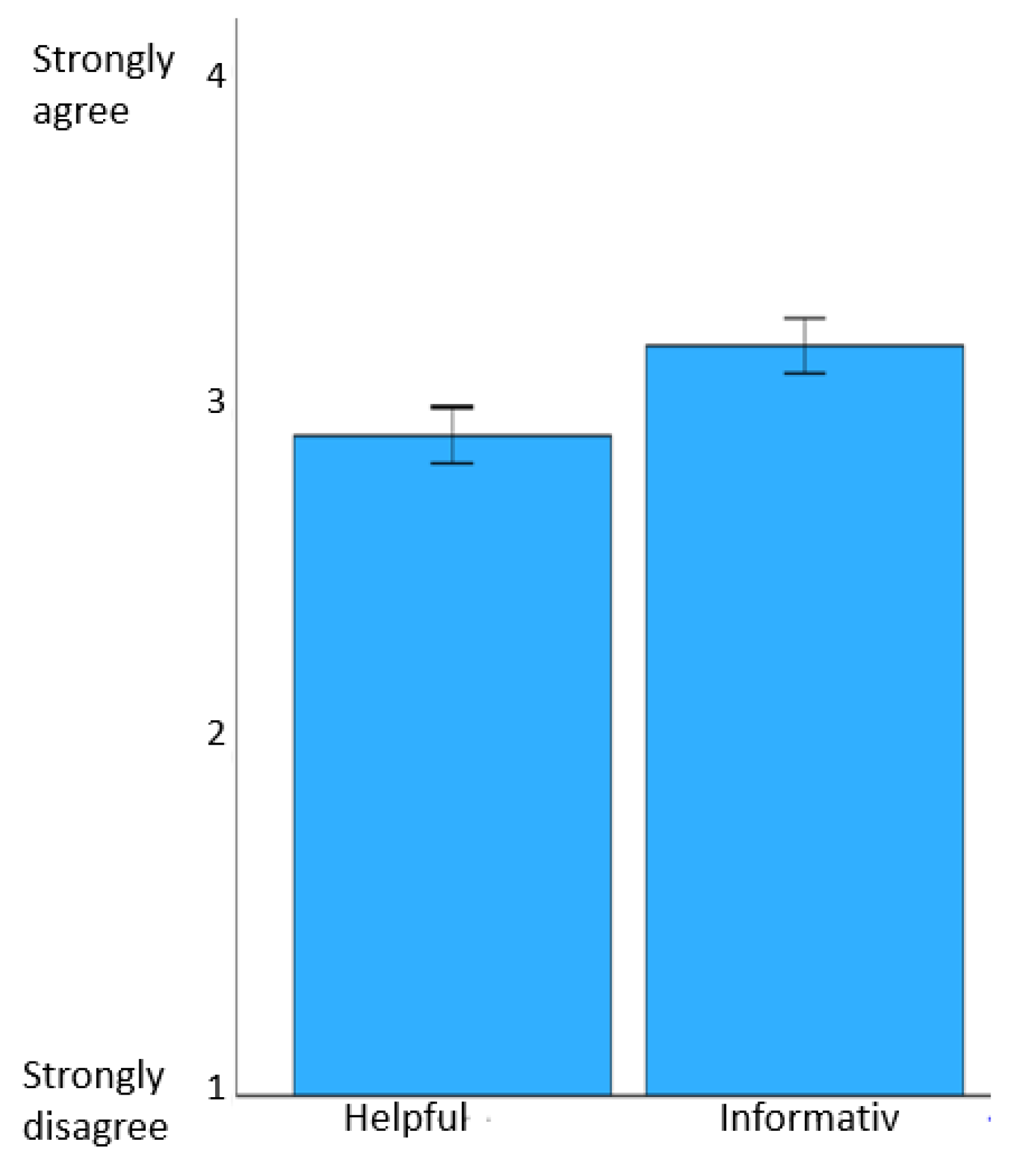
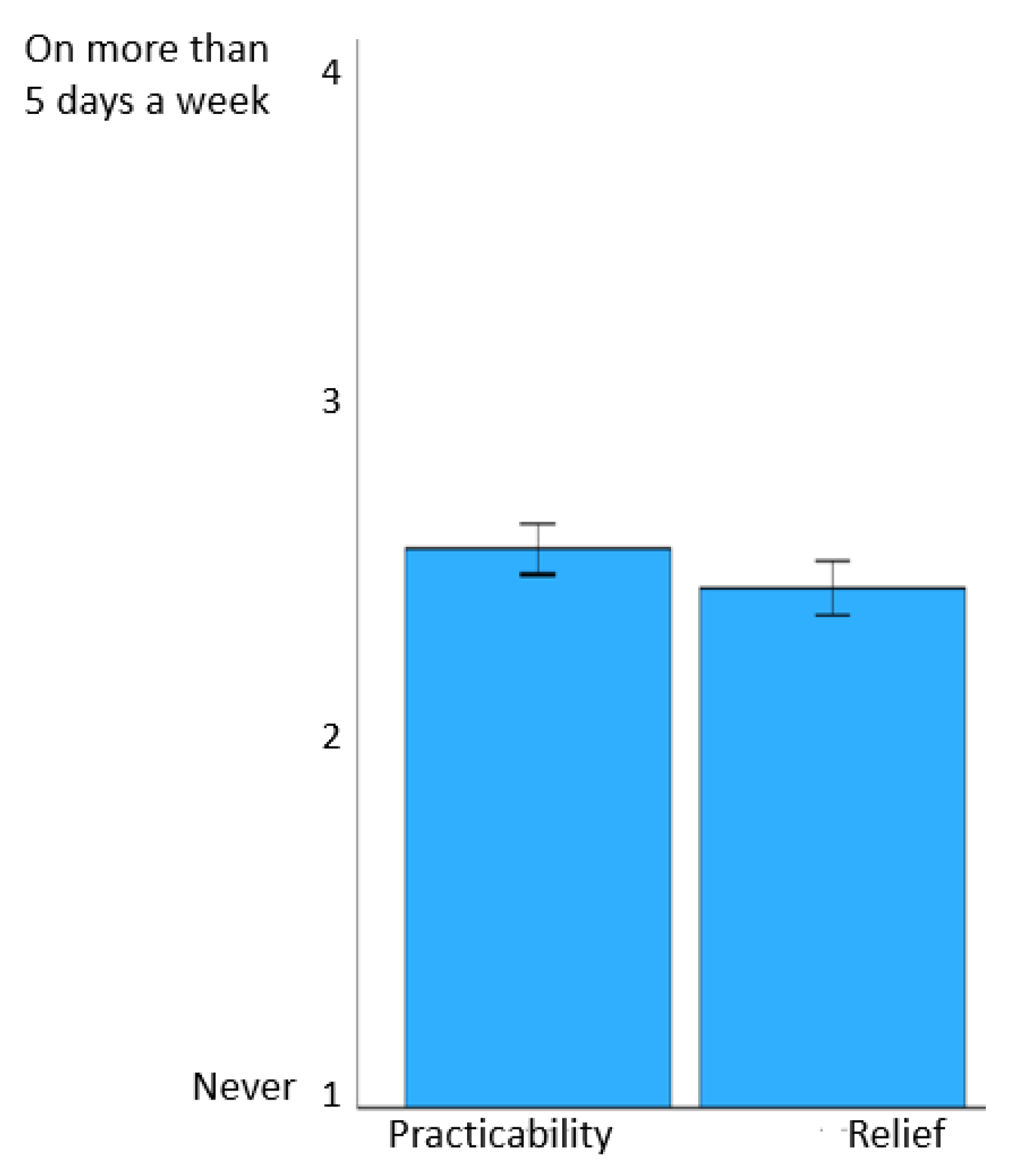
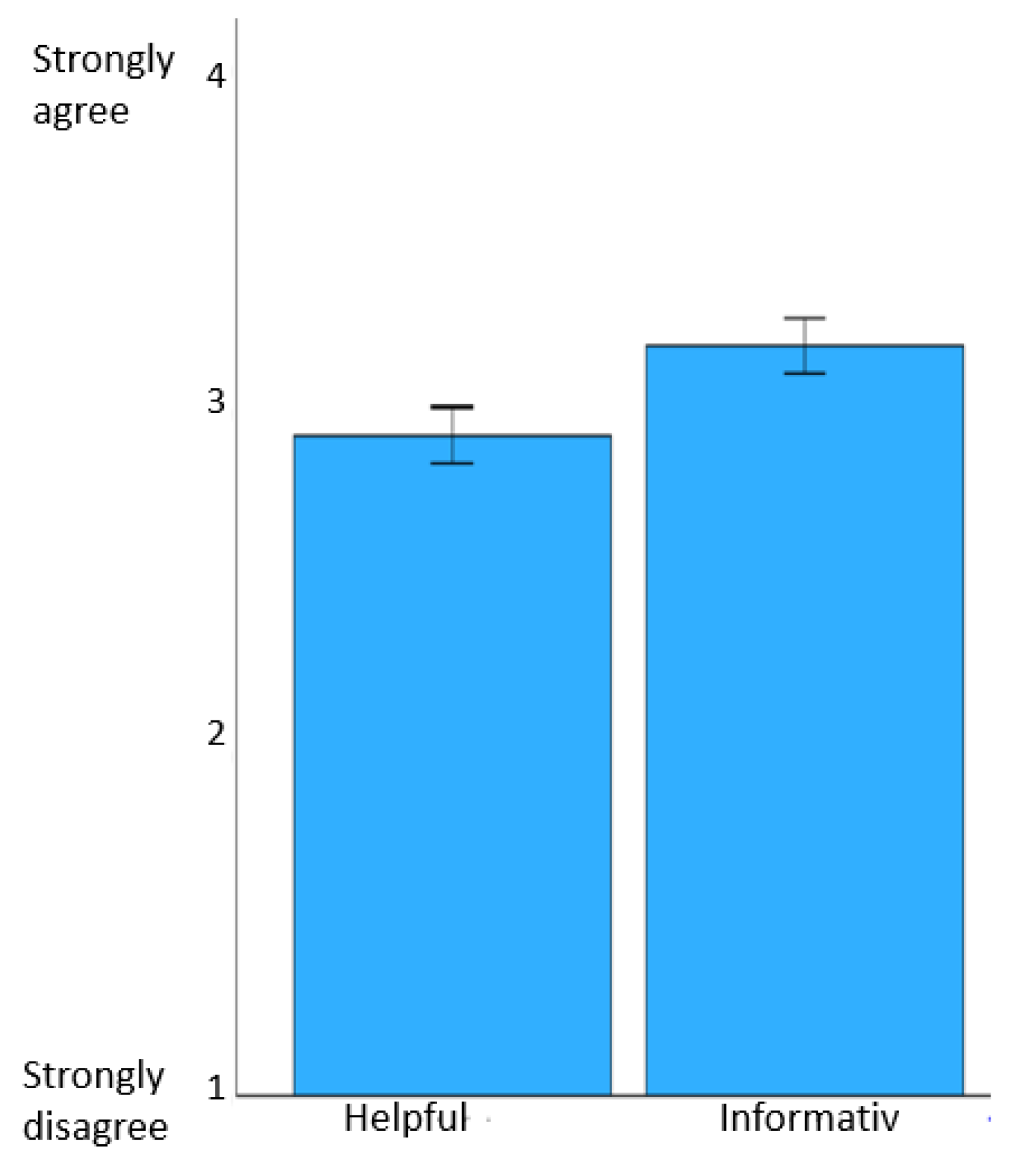
3.4. Satisfaction with and Adherence to the Passive Psychoeducation Program
4. Discussion
5. Limitations
6. Implications for Practice and Research
7. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Klein, E.M.; Brähler, E.; Dreier, M.; Reinecke, L.; Müller, K.W.; Schmutzer, G.; Wölfling, K.; Beutel, M.E. The German version of the Perceived Stress Scale–Psychometric characteristics in a representative German community sample. BMC Psychiatry 2016, 16, 159. [Google Scholar] [CrossRef]
- McEwen, B.S. Protective and damaging effects of stress mediators. N. Engl. J. Med. 1998, 338, 171–179. [Google Scholar] [CrossRef]
- Hämmig, O.; Bauer, G. Work-life imbalance and mental health among male and female employees in Switzerland. Int. J. Public Health 2009, 54, 88–95. [Google Scholar] [CrossRef]
- Delfino, J.P.; Barragán, E.; Botella, C.; Braun, S.; Bridler, R.; Camussi, E.; Chafrat, V.; Lott, P.; Mohr, C.; Moragrega, I.; et al. Quantifying insufficient coping behavior under chronic stress: A cross-cultural study of 1303 students from Italy, Spain and Argentina. Psychopathology 2015, 48, 230–239. [Google Scholar] [CrossRef]
- Pozos-Radillo, B.E.; de Lourdes Preciado-Serrano, M.; Acosta-Fernández, M.; de los Ángeles Aguilera-Velasco, M.; Delgado-García, D.D. Academic stress as a predictor of chronic stress in university students. Psicol. Educ. 2014, 20, 47–52. [Google Scholar] [CrossRef]
- Beiter, R.; Nash, R.; McCrady, M.; Rhoades, D.; Linscomb, M.; Clarahan, M.; Sammut, S. The prevalence and correlates of depression, anxiety, and stress in a sample of college students. J. Affect. Dis. 2015, 173, 90–96. [Google Scholar] [CrossRef]
- Büttner, T.R.; Dlugosch, G.E. Stress im Studium. Prävent. Gesundheitsförd. 2013, 8, 106–111. [Google Scholar] [CrossRef]
- Grützmacher, J.; Gusy, B.; Lesener, T.; Sudheimer, S.; Willige, J. Gesundheit Studierender in Deutschland 2017. Ein Kooperationsprojekt Zwischen dem Deutschen Zentrum für Hochschul-und Wissenschaftsforschung, der Freien Universität Berlin und der Techniker-Krankenkasse; Techniker Krankenkasse: Hamburg, Germany, 2018; Available online: https://www.tk.de/resource/blob/2050660/8bd39eab37ee133a2ec47e55e544abe7/gesundheit-studierender-in-deutschland2017-studienband-data.pdf (accessed on 3 November 2023).
- Herbst, U.; Voeth, M.; Eidhoff, A.T.; Müller, M.; Stief, S. Studierendenstress in Deutschland–Eine Empirische Untersuchung; AOK-Bundesverband: Berlin, Germany, 2016; Available online: https://www.uni-heidelberg.de/md/journal/2016/10/08_projektbericht_stressstudie.pdf (accessed on 3 November 2023).
- Lipson, S.K.; Lattie, E.G.; Eisenberg, D. Increased rates of mental health service utilization by U.S. College students: 10-year population-level trends (2007–2017). Psychiatr. Serv. 2019, 70, 60–63. [Google Scholar] [CrossRef]
- Blume, C.; Schmidt, M.H.; Cajochen, C. Effects of the COVID-19 lockdown on human sleep and rest-activity rhythms. Curr. Biol. 2020, 30, R795–R797. [Google Scholar] [CrossRef]
- Chang, J.J.; Ji, Y.; Li, Y.H.; Pan, H.F.; Su, P.Y. Prevalence of anxiety symptom and depressive symptom among college students during COVID-19 pandemic: A metaanalysis. J. Affect. Disord. 2021, 292, 242–254. [Google Scholar] [CrossRef]
- Lin, L.Y.; Wang, J.; Ou-Yang, X.Y.; Miao, Q.; Chen, R.; Liang, F.X.; Zhang, Y.-P.; Tang, Q.; Wang, T. The immediate impact of the 2019 novel coronavirus (COVID-19) outbreak on subjective sleep status. Sleep Med. 2020, 77, 348–354. [Google Scholar] [CrossRef]
- Patelarou, A.; Mechili, E.A.; Galanis, P.; Zografakis-Sfakianakis, M.; Konstantinidis, T.; Saliaj, A.; Bucaj, J.; Alushi, E.; Carmona-Torres, J.M.; Cobo-Cuenca, A.I.; et al. Nursing students, mental health status during COVID-19 quarantine: Evidence from three European countries. J. Ment. Health 2021, 30, 164–169. [Google Scholar] [CrossRef]
- Son, C.; Hegde, S.; Smith, A.; Wang, X.; Sasangohar, F. Effects of COVID-19 on College Students’ Mental Health in the United States: Interview Survey Study. J. Med. Internet Res. 2020, 22, e21279. [Google Scholar] [CrossRef]
- Batchelor, R.; Pitman, E.; Sharpington, A.; Stock, M.; Cage, E. Student perspectives on mental health support and services in the UK. J. Furth. High. Educ. 2020, 44, 483–497. [Google Scholar] [CrossRef]
- Harrer, M.; Apolinário-Hagen, J.; Fritsche, L.; Salewski, C.; Zarski, A.C.; Lehr, D.; Baumeister, H.; Cuijpers, P.; Ebert, D.D. Effect of an internet- and app-based stress intervention compared to online psychoeducation in university students with depressive symptoms: Results of a randomized controlled trial. Internet Interv. 2021, 24, 100374. [Google Scholar] [CrossRef]
- Bruffaerts, R.; Mortier, P.; Auerbach, R.P.; Alonso, J.; De la Torre, A.E.H.; Cuijpers, P.; Demyttenaere, K.; Ebert, D.D.; Green, J.G.; Hasking, P.; et al. Lifetime and 12-month treatment for mental disorders and suicidal thoughts and behaviors among first year college students. Int. J. Methods Psychiatr. Res. 2019, 28, e1764. [Google Scholar] [CrossRef]
- Ramón-Arbués, E.; Gea-Caballero, V.; Granada-López, J.M.; Juárez-Vela, R.; Pellicer-García, B.; Antón-Solanas, I. The Prevalence of Depression, Anxiety and Stress and Their Associated Factors in College Students. Int. J. Environ. Res. Public Health 2020, 17, 7001. [Google Scholar] [CrossRef]
- Thorley, C. Not by Degrees: Improving Student Mental Health in the UK’s Universities; Institute for Public Policy Research: London, UK, 2017. [Google Scholar]
- Amanvermez, Y.; Zhao, R.; Cuijpers, P.; de Wit, L.M.; Ebert, D.D.; Kessler, R.C.; Bruffaerts, R.; Karyotaki, E. Effects of self-guided stress management interventions in college students: A systematic review and meta-analysis. Internet Interv. 2022, 28, 100503. [Google Scholar] [CrossRef]
- American Psychological Association. APA Dictionary of Psychology. Available online: https://dictionary.apa.org/preventive-stress-managent (accessed on 3 November 2023).
- Romano, J.L. Psychoeducational Interventions for Stress Management and Well-Being. J. Couns. Dev. 1992, 71, 199–202. [Google Scholar] [CrossRef]
- Huang, C.Y.; Lai, H.L.; Lu, Y.C.; Chen, W.K.; Chi, S.C.; Lu, C.Y.; Chen, C.I. Risk Factors and Coping Style Affect Health Outcomes in Adults With Type 2 Diabetes. Biol. Res. Nurs. 2016, 18, 82–89. [Google Scholar] [CrossRef]
- Pinkasavage, E.; Arigo, D.; Schumacher, L.M. Social comparison, negative body image, and disordered eating behavior: The moderating role of coping style. Eat. Behav. 2015, 16, 72–77. [Google Scholar] [CrossRef] [PubMed]
- Günaydin, N. Effect of group psychoeducation on depression, anxiety, stress and coping with stress of nursing students: A randomized controlled study. Perspect. Psychiatr. Care 2022, 58, 640–650. [Google Scholar] [CrossRef] [PubMed]
- Donker, T.; Griffiths, K.M.; Cuijpers, P.; Christensen, H. Psychoeducation for depression, anxiety and psychological distress: A meta-analysis. BMC Med. 2009, 7, 79. [Google Scholar] [CrossRef]
- Baourda, V.C.; Brouzos, A.; Mavridis, D.; Vassilopoulos, S.P.; Vatkali, E.; Boumpouli, C. Group Psychoeducation for Anxiety Symptoms in Youth: Systematic Review and Meta-analysis. J. Spec. Group Work. 2021, 47, 22–42. [Google Scholar] [CrossRef]
- Cheng, Q.; Xu, B.; Ng, M.S.N.; Duan, Y.; So, W.K.W. Effectiveness of psychoeducational interventions among caregivers of patients with cancer: A systematic review and meta-analysis. Int. J. Nurs. Stud. 2022, 127, 104162. [Google Scholar] [CrossRef] [PubMed]
- Okafor, A.J.; Monahan, M. Effectiveness of Psychoeducation on Burden among Family Caregivers of Adults with Schizophrenia: A Systematic Review and Meta-Analysis. Nurs. Res. Pract. 2023, 2023, 2167096. [Google Scholar] [CrossRef]
- Yu, Y.; Xiao, L.; Ullah, S.; Meyer, C.; Wang, J.; Pot, A.M.; Shifaza, F. The Experiences of Informal Caregivers of People with Dementia in Web-Based Psychoeducation Programs: Systematic Review and Metasynthesis. JMIR Aging 2023, 6, e47152. [Google Scholar] [CrossRef]
- Ahmad, T.H.B.; Meriç, M.; Ayasrah, M. The Effect of Psychoeducational Stress Management Interventions on Students Stress Reduction: Systematic Review. J. Educ. Cult. Psychol. Stud. 2022, 25, 41–57. [Google Scholar]
- Van Daele, T.; Welzijn, S.; En Gezin, V.; Hermans, D.; Van Audenhove, C.; Van Den Bergh, O. Stress Reduction through Psychoeducation: A Meta-Analytic Review. Health Educ. Behav. 2012, 39, 474–485. [Google Scholar] [CrossRef]
- Ahmad, T.; Meriç, M. The effect of an online psychoeducational stress management program on international students’ ability to cope and adapt. Perspect. Psychiatr. Care 2021, 57, 1673–1684. [Google Scholar] [CrossRef]
- Harrer, M.; Adam, S.H.; Fleischmann, R.J.; Baumeister, H.; Auerbach, R.; Bruffaerts, R.; Cuijpers, P.; Kessler, R.C.; Berking, M.; Lehr, D.; et al. Effectiveness of an internet- and app-based intervention for college students with elevated stress: Randomized controlled trial. J. Med. Internet Res. 2018, 20, e136. [Google Scholar] [CrossRef] [PubMed]
- Harrer, M.; Adam, S.H.; Baumeister, H.; Cuijpers, P.; Karyotaki, E.; Auerbach, R.P.; Kessler, R.C.; Bruffaerts, R.; Berking, M.; Ebert, D.D. Internet interventions for mental health in university students: A systematic review and meta-analysis. Int. J. Methods Psychiatr. Res. 2019, 28, e1759. [Google Scholar] [CrossRef]
- Andrews, G.; Cuijpers, P.; Craske, M.G.; McEvoy, P.; Titov, N. Computer therapy for the anxiety and depressive disorders is effective, acceptable and practical health care: A meta-analysis. PLoS ONE 2010, 5, e13196. [Google Scholar] [CrossRef]
- Botella, C.; Mira, A.; Herrero, R.; García Palacios, A.; Baños, R.M. Un programa de intervención autoaplicado a través de Internet para el tratamiento de la depresión: “Sonreír es divertido”. Aloma Rev. Psicol. 2015, 33, 39–48. [Google Scholar]
- Montero-Marín, J.; Araya, R.; Pérez-Yus, M.C.; Mayoral, F.; Gili, M.; Botella, C.; Baños, R.; Castro, A.; Romero-Sanchiz, P.; López-Del-Hoyo, Y.; et al. An internet-based intervention for depression in primary Care in Spain: A randomized controlled trial. J. Med. Internet Res. 2016, 18, e231. [Google Scholar] [CrossRef] [PubMed]
- Heber, E.; Ebert, D.D.; Lehr, D.; Cuijpers, P.; Berking, M.; Nobis, S.; Riper, H. The benefit of web- and computer-based interventions for stress: A systematic review and meta-analysis. J. Med. Internet Res. 2017, 19, e32. [Google Scholar] [CrossRef] [PubMed]
- Hennemann, S.; Beutel, M.E.; Zwerenz, R. Drivers and barriers to acceptance of web-based aftercare of patients in inpatient routine care: A cross-sectional survey. J. Med. Internet Res. 2016, 18, e337. [Google Scholar] [CrossRef]
- Sander, L.; Rausch, L.; Baumeister, H. Effectiveness of internet-based interventions for the prevention of mental disorders: A systematic review and meta-analysis. JMIR Ment. Health 2016, 3, e38. [Google Scholar] [CrossRef]
- Abbott, J.A.M.; Klein, B.; Ciechomski, L. Best practices in online therapy. J. Technol. Hum. Serv. 2008, 26, 360–375. [Google Scholar] [CrossRef]
- Baños, R.M.; Etchemendy, E.; Mira, A.; Riva, G.; Gaggioli, A.; Botella, C. Online positive interventions to promote well-being and resilience in the adolescent population: A narrative review. Front. Psychol. 2017, 8, 10. [Google Scholar] [CrossRef]
- Bolier, L.; Haverman, M.; Westerhof, G.J.; Riper, H.; Smit, F.; Bohlmeijer, E. Positive psychology interventions: A meta-analysis of randomized controlled studies. BMC Public Health 2013, 13, 119. [Google Scholar] [CrossRef] [PubMed]
- Lintvedt, O.K.; Griffiths, K.M.; Sorensen, K.; Ostvik, A.R.; Wang, C.E.A.; Eisemann, M.; Waterloo, K. Evaluating the effectiveness and efficacy of unguided internet-based self-help intervention for the prevention of depression: A randomized controlled trial. Clin. Psychol. Psychother. 2013, 20, 10–27. [Google Scholar] [CrossRef] [PubMed]
- Rose, R.D.; Buckey, J.C.; Zbozinek, T.D.; Motivala, S.J.; Glenn, D.E.; Cartreine, J.A.; Craske, M.G. A randomized controlled trial of a self-guided, multimedia, stress management and resilience training program. Behav. Res. Ther. 2013, 51, 106–112. [Google Scholar] [CrossRef]
- Lovibond, S.H.; Lovibond, P.F. Depression Anxiety Stress Scales (DASS–21, DASS–42); APA PsycTests: Washington, DC, USA, 1995. [Google Scholar]
- Nilges, P.; Essau, C. DASS. Depressions-Angst-Stress-Skalen-Deutschsprachige Kurzfassung; ZPID, Leibniz-Institut für Psychologie Open Test Archive: Trier, Germany, 2021. [Google Scholar]
- Henry, J.D.; Crawford, J.R. The short-form version of the Depression Anxiety Stress Scales (DASS-21): Construct validity and normative data in a large non-clinical sample. Br. J. Clin. Psychol. 2005, 44, 227–239. [Google Scholar] [CrossRef] [PubMed]
- Kühner, C.; Huffziger, S.; Nolen-Hoeksema, S. RSQ-D Response Styles Questionnaire–Deutsche Version; Hogrefe: Göttingen, Germany, 2007. [Google Scholar]
- Nolen-Hoeksema, S. Responses to depression and their effects on the duration of depressive episodes. J. Abnorm. Psychol. 1991, 100, 569–582. [Google Scholar] [CrossRef]
- Abler, B.; Kessler, H. Emotion Regulation Questionnaire–Eine deutschsprachige Fassung des ERQ von Gross und John. Diagnostica 2009, 55, 144–152. [Google Scholar] [CrossRef]
- Gross, J.J.; John, O.P. Individual differences in two emotion regulation processes: Implications for affect, relationships, and well-being. J. Pers. Soc. Psychol. 2003, 85, 348–362. [Google Scholar] [CrossRef]
- Hayes, C.; Morgan, M. Evaluation of a Psychoeducational Program to Help Adolescents Cope. J. Youth Adolesc. 2005, 34, 111–121. [Google Scholar] [CrossRef]
- McCarthy, B.; Trace, A.; O’Donovan, M.; O’Regan, P.; Brady-Nevin, C.; O’Shea, M.; Martin, A.M.; Murphy, M. Coping with stressful events: A pre-post-test of a psychoeducational intervention for undergraduate nursing and midwifery students. Nurse Educ. Today 2018, 61, 273–280. [Google Scholar] [CrossRef]
- Steinhardt, M.; Dolbier, C. Evaluation of a Resilience Intervention to Enhance Coping Strategies and Protective Factors and Decrease Symptomatology. J. Am. Coll. Health 2010, 56, 445–453. [Google Scholar] [CrossRef]
- Charbonnier, E.; Trémolière, B.; Baussard, L.; Goncalves, A.; Lespiau, F.; Philippe, A.G.; Le Vigouroux, S. Effects of an online self-help intervention on university students’ mental health during COVID-19: A non-randomized controlled pilot study. Comput. Hum. Behav. Rep. 2022, 5, 100175. [Google Scholar] [CrossRef]
- Küchler, A.M.; Schultchen, D.; Dretzler, T.; Moshagen, M.; Ebert, D.D.; Baumeister, H. A Three-Armed Randomized Controlled Trial to Evaluate the Effectiveness, Acceptance, and Negative Effects of StudiCare Mindfulness, an Internet- and Mobile-Based Intervention for College Students with No and “On Demand” Guidance. Int. J. Environ. Res. Public Health 2023, 20, 3208. [Google Scholar] [CrossRef]
- Long, R.; Halvorson, M.; Lengua, L.J. A mindfulness-based promotive coping program improves well-being in college undergraduates. Anxiety Stress Coping 2021, 34, 690–703. [Google Scholar] [CrossRef]
- Sanilevici, M.; Reuveni, O.; Lev-Ari, S.; Golland, Y.; Levit-Binnun, N. Mindfulness-Based Stress Reduction Increases Mental Wellbeing and Emotion Regulation during the First Wave of the COVID-19 Pandemic: A Synchronous Online Intervention Study. Front. Psychol. 2021, 12, 720965. [Google Scholar] [CrossRef]
- Stächele, T.; Domes, G.; Wekenborg, M.; Penz, M.; Kirschbaum, C.; Heinrichs, M. Effects of a 6-Week Internet-Based Stress Management Program on Perceived Stress, Subjective Coping Skills, and Sleep Quality. Front. Psychiatry 2020, 11, 463. [Google Scholar] [CrossRef] [PubMed]
- Ebert, D.D.; Lehr, D.; Heber, E.; Riper, H.; Cuijpers, P.; Berking, M. Internet- and mobile-based stress management for employees with adherence-focused guidance: Efficacy and mechanism of change. Scand. J. Work. Environ. Health 2016, 42, 382–394. [Google Scholar] [CrossRef]
- Palmqvist, B.; Carlbring, P.; Andersson, G. Internet-delivered treatments with or without therapist input: Does the therapist factor have implications for efficacy and cost? Expert Rev. Pharmacoecon. Outcomes Res. 2007, 7, 291–297. [Google Scholar] [CrossRef]
- Lattie, E.G.; Adkins, E.C.; Winquist, N.; Stiles-Shields, C.; Wafford, Q.E.; Graham, A.K. Digital Mental Health Interventions for Depression, Anxiety, and Enhancement of Psychological Well-Being Among College Students: Systematic Review. J. Med. Internet Res. 2019, 21, e12869. [Google Scholar] [CrossRef]
- Bacchi, S.; Licinio, J. Qualitative literature review of the prevalence of depression in medical students compared to students in non-medical degrees. Acad. Psychiatry 2015, 39, 293–299. [Google Scholar] [CrossRef] [PubMed]
- Puthran, R.; Zhang, M.W.B.; Tam, W.W.; Ho, R.C. Prevalence of depression amongst medical students: A meta-analysis. Med. Educ. 2016, 50, 456–468. [Google Scholar] [CrossRef] [PubMed]
- Holm-Hadulla, R.M.; Hofmann, F.H.; Sperth, M.; Funke, J. Psychische Beschwerden und Störungen von Studierenden. Psychotherapeut 2009, 54, 346–356. [Google Scholar] [CrossRef]
- Cerolini, S.; Zagaria, A.; Franchini, C.; Maniaci, V.G.; Fortunato, A.; Petrocchi, C.; Speranza, A.M.; Lombardo, C. Psychological Counseling among University Students Worldwide: A Systematic Review. Eur. J. Investig. Health Psychol. Educ. 2023, 13, 1831–1849. [Google Scholar] [CrossRef] [PubMed]
- Osborn, T.G.; Li, S.; Saunders, R.; Fonagy, P. University students’ use of mental health services: A systematic review and meta-analysis. Int. J. Ment. Health Syst. 2022, 16, 57. [Google Scholar] [CrossRef] [PubMed]
- Kato, T. Frequently Used Coping Scales: A Meta-Analysis. Stress Health 2015, 31, 315–323. [Google Scholar] [CrossRef] [PubMed]
- Klauer, T. Stressbewältigung. Psychotherapeut 2012, 57, 263–278. [Google Scholar] [CrossRef]

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Module | Content |
|---|---|
| Stress (week 1) | The first psychoeducation module focuses on stress, including stress reactions and the effects of prolonged stress on the body. It also covers the benefits of recovery for the body and provides a brief introduction to self-management strategies. |
| Daily routine (week 2) | The second psychoeducation module aims to provide guidance on time management and prioritizing tasks. Effective planning strategies are recommended, e.g., creating to-do lists, analyzing daily performance highs and lows, or creating realistic plans with short breaks before and after each activity. |
| Emotion regulation/problem solving (week 3) | The third psychoeducation module analyses the importance of emotional self-regulation and emotional skills training. It explains the difference between maladaptive strategies for emotion regulation, such as suppression of thoughts/emotions, avoidance, or rumination, and adaptive emotional skills, such as high emotion recognition skills (e.g., acceptance, reappraisal, focusing on positive aspects of the situation). In addition, the six-step problem-solving model is discussed. |
| Sleep (week 4) | The fourth psychoeducation module focuses on the importance of healthy sleep–wake behavior and rules for sleep hygiene. It provides information on a range of practices and habits that promote healthy sleep. These include keeping regular bedtimes and wake-up times, avoiding naps, getting enough exercise during the day, and creating a comfortable and peaceful sleep environment. |
| Pleasurable activities (week 5) | The fifth psychoeducational module informs about the health benefits of pleasurable activities. It lists different types of pleasurable activities and gives instructions on how to plan them effectively. |
| Physical activity (week 6) | The sixth psychoeducation module focuses on the importance of physical activity for physical and mental health. It contains detailed information on suitable sports and exercises to reduce stress, strengthen muscles, and improve mobility, as well as advice on how to incorporate more exercise into your everyday life. |
| Nutrition (week 7) | The final psychoeducational module provides an overview of dietary guidelines (e.g., the importance of drinking enough water and opting for vegetables, fruit, whole grains, and low-fat dairy products while reducing sugar and salt intake). The module also provides additional information for vegetarians and vegans as well as various links for meal preparation. |
| Psychoeducation Group | Waiting List Control Group | Total | |
|---|---|---|---|
| n = 123 | n = 130 | n = 253 | |
| Age [years]: mean (SD) | 22.04 (2.8) | 22.42 (3.59) | 22.24 (3.23) |
| Sex | |||
| Female: n (%) | 95 (77.2%) | 99 (76.2%) | 194 (76.7%) |
| Male: n (%) | 28 (22.8%) | 29 (22.3%) | 57 (22.5%) |
| Gender-diverse: n (%) | 2 (1.5%) | 2 (0.8%) | |
| Level of education | |||
| Bachelor students: n (%) | 103 (83.7%) | 116 (89.2%) | 219 (86.6%) |
| Master students: n (%) | 18 (14.7%) | 13 (10%) | 31 (12.2%) |
| PhD students n (%) | 2 (1.6%) | 1 (0.8%) | 3 (1.2%) |
| University courses | |||
| Social sciences Psychology students | 10 (8,1%) 95 (77.2%) | 8 (6.1%) 108 (83.1%) | 18 (7.1%) 203 (80.2%) |
| Natural science | 8 (6.5%) | 6 (4.6%) | 14 (5.5%) |
| Medical and health science | 1 (0.8%) | 1 (0.8%) | 2 (0.8%) |
| Humanities | 5 (4.1%) | 4 (3.1%) | 9 (3.6%) |
| Engineering and Technology | 4 (3.3) | 3 (2.3%) | 7 (2.8%) |
| Mental illness | |||
| Psychotherapeutic treatment | 26 (21.1%) | 20 (15.4%) | 46 (18.2%) |
| Mental illness | 28 (22.8%) | 24 (18.5%) | 52 (20.6%) |
| Psychoeducation Group | Waiting List Control Group | |||
|---|---|---|---|---|
| Pre M (SD) | Post M (SD) | Pre M (SD) | Post M (SD) | |
| DASS-21 | ||||
| Depression | 5.64 (4.25) | 5.45 (4.48) | 5.55 (4.21) | 5.28 (4.00) |
| Anxiety | 5.10 (3.64) | 4.24 (3.33) | 4.55 (3.68) | 4.02 (3.49) |
| Stress | 7.59 (4.18) | 7.33 (4.25) | 7.31 (3.84) | 7.10 (3.67) |
| RSQ | ||||
| Symptom-related rumination | 18.85 (5.05) | 18 (5.08) | 17.93 (4.58) | 18.25 (5.10) |
| Self-related rumination | 16.89 (4.37) | 16.60 (4.31) | 17.33 (4.19) | 16.82 (4.33) |
| Distraction | 17.75 (3.38) | 18.15 (3.56) | 17.25 (4.29) | 17.71 (4.01) |
| ERQ | ||||
| Reappraisal | 26.03 (6.11) | 28.39 (5.66) | 26.08 (6.81) | 26.61 (6.17) |
| Suppression | 13.59 (4.96) | 13.25 (4.99) | 13.65 (4.95) | 13.92 (5.17) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Weiss, E.M.; Staggl, S.; Holzner, B.; Rumpold, G.; Dresen, V.; Canazei, M. Preventive Effect of a 7-Week App-Based Passive Psychoeducational Stress Management Program on Students. Behav. Sci. 2024, 14, 180. https://doi.org/10.3390/bs14030180
Weiss EM, Staggl S, Holzner B, Rumpold G, Dresen V, Canazei M. Preventive Effect of a 7-Week App-Based Passive Psychoeducational Stress Management Program on Students. Behavioral Sciences. 2024; 14(3):180. https://doi.org/10.3390/bs14030180
Chicago/Turabian StyleWeiss, Elisabeth M., Siegmund Staggl, Bernhard Holzner, Gerhard Rumpold, Verena Dresen, and Markus Canazei. 2024. "Preventive Effect of a 7-Week App-Based Passive Psychoeducational Stress Management Program on Students" Behavioral Sciences 14, no. 3: 180. https://doi.org/10.3390/bs14030180
APA StyleWeiss, E. M., Staggl, S., Holzner, B., Rumpold, G., Dresen, V., & Canazei, M. (2024). Preventive Effect of a 7-Week App-Based Passive Psychoeducational Stress Management Program on Students. Behavioral Sciences, 14(3), 180. https://doi.org/10.3390/bs14030180