Does Decreased Vitamin D Level Trigger Bipolar Manic Attacks?


Abstract
:1. Introduction
2. Material and Methods
2.1. Ethical Approval and Participants
2.2. Design and Procedure
2.3. Collection of Blood Samples and Laboratory Analysis
2.4. Statistical Analysis
3. Results
4. Discussion
5. Limitations of the Study
6. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Kessing, L.V.; González-Pinto, A.; Fagiolini, A.; Bechdolf, A.; Reif, A.; Yildiz, A.; Etain, B.; Henry, C.; Severus, E.; Reininghaus, E.Z.; et al. DSM-5 and ICD-11 criteria for bipolar disorder: Implications for the prevalence of bipolar disorder and validity of the diagnosis—A narrative review from the ECNP bipolar disorders network. Eur. Neuropsychopharmacol. 2021, 47, 54–61. [Google Scholar] [CrossRef]
- Collins, P.Y.; Patel, V.; Joestl, S.S.; March, D.; Insel, T.R.; Daar, A.S.; Bordin, I.A.; Costello, E.J.; Durkin, M.; Fairburn, C.; et al. Grand challenges in global mental health. Nature 2011, 475, 27–30. [Google Scholar] [CrossRef]
- Kessler, R.C.; Akiskal, H.S.; Ames, M.; Birnbaum, H.; Greenberg, P.; A, R.M.; Jin, R.; Merikangas, K.R.; Simon, G.E.; Wang, P.S. Prevalence and Effects of Mood Disorders on Work Performance in a Nationally Representative Sample of U.S. Workers. Am. J. Psychiatry 2006, 163, 1561–1568. [Google Scholar] [CrossRef]
- Kessing, L.V.; Vradi, E.; Andersen, P.K. Life expectancy in bipolar disorder. Bipolar Disord. 2015, 17, 543–548. [Google Scholar] [CrossRef] [PubMed]
- Howes, O.D.; Thase, M.E.; Pillinger, T. Treatment resistance in psychiatry: State of the art and new directions. Mol. Psychiatry 2022, 27, 58–72. [Google Scholar] [CrossRef] [PubMed]
- Fries, G.R.; Walss-Bass, C.; Bauer, M.E.; Teixeira, A.L. Revisiting inflammation in bipolar disorder. Pharmacol. Biochem. Behav. 2019, 177, 12–19. [Google Scholar] [CrossRef]
- Rantala, M.J.; Luoto, S.; Borráz-León, J.I.; Krams, I. Bipolar disorder: An evolutionary psychoneuroimmunological approach. Neurosci. Biobehav. Rev. 2021, 122, 28–37. [Google Scholar] [CrossRef] [PubMed]
- İmre, O.; Yılmaz, İ.V.G. Neutrophil-Lymphocyte Ratio, Monocyte-Lymphocyte Ratio and Platelet-Lymphocyte Ratio in Manic Episode Patients with Bipolar Disorder. Eur. J. Ther. 2023, 29, 110–115. [Google Scholar] [CrossRef]
- Altunsoy, N.; Yüksel, R.N.; Cingi Yirun, M.; Kılıçarslan, A.; Aydemir, Ç. Exploring the relationship between vitamin D and mania: Correlations between serum vitamin D levels and disease activity. Nord. J. Psychiatry 2018, 72, 221–225. [Google Scholar] [CrossRef] [PubMed]
- Holick, M.F. Vitamin D Deficiency. N. Engl. J. Med. 2007, 357, 266–281. [Google Scholar] [CrossRef] [PubMed]
- Holick, M.F. The vitamin D deficiency pandemic: Approaches for diagnosis, treatment and prevention. Rev. Endocr. Metab. Disord. 2017, 18, 153–165. [Google Scholar] [CrossRef] [PubMed]
- Sassi, F.; Tamone, C.; D’Amelio, P. Vitamin D: Nutrient, Hormone, and Immunomodulator. Nutrients 2018, 10, 1656. [Google Scholar] [CrossRef] [PubMed]
- Ao, T.; Kikuta, J.; Ishii, M. The Effects of Vitamin D on Immune System and Inflammatory Diseases. Biomolecules 2021, 11, 1624. [Google Scholar] [CrossRef]
- Garcion, E.; Sindji, L.; Montero-Menei, C.; Andre, C.; Brachet, P.; Darcy, F. Expression of inducible nitric oxide synthase during rat brain inflammation: Regulation by 1,25-dihydroxyvitamin D3. Glia 1998, 22, 282–294. [Google Scholar] [CrossRef]
- Umar, M.; Sastry, K.S.; Chouchane, A.I. Role of Vitamin D Beyond the Skeletal Function: A Review of the Molecular and Clinical Studies. Int. J. Mol. Sci. 2018, 19, 1618. [Google Scholar] [CrossRef] [PubMed]
- Yang, J.; Joe, S.H.; Lee, M.S.; Ko, Y.H.; Jung, I.K.; Kim, S.H. Effects of long-term combination treatment with valproate and atypical antipsychotics on bone mineral density and bone metabolism in premenopausal patients with bipolar disorder: A preliminary study. Psychiatry Investig. 2011, 8, 256–261. [Google Scholar] [CrossRef]
- Cereda, G.; Enrico, P.; Ciappolino, V.; Delvecchio, G.; Brambilla, P. The role of vitamin D in bipolar disorder: Epidemiology and influence on disease activity. J. Affect. Disord. 2021, 278, 209–217. [Google Scholar] [CrossRef] [PubMed]
- Akdemir, A.; Örsel, D.S.; Dağ, İ.; Türkçapar, M.H.; İşcan, N.; Özbay, H. Hamilton depresyon derecelendirme ölçeği (HDDÖ)’nin geçerliliği-güvenirliliği ve klinikte kullanımı. Psikiyatr. Psikol. Psikofarmakol. Derg. 1996, 4, 251–259. [Google Scholar]
- Karadağ, F.; Oral, E.T.; Aran Yalçın, F.; Erten, E. Young mani derecelendirme ölçeğinin Türkiye’de geçerlik ve güvenilirliği. Türk Psikiyatr. Derg. 2001, 13, 107–114. [Google Scholar]
- Belzeaux, R.; Boyer, L.; Ibrahim, E.C.; Féron, F.; Leboyer, M.; Fond, G. Mood disorders are associated with a more severe hypovitaminosis D than schizophrenia. Psychiatry Res. 2015, 229, 613–616. [Google Scholar] [CrossRef]
- Patrick, R.P.; Ames, B.N. Vitamin D and the omega-3 fatty acids control serotonin synthesis and action, part 2: Relevance for ADHD, bipolar disorder, schizophrenia, and impulsive behavior. FASEB J. 2015, 29, 2207–2222. [Google Scholar] [CrossRef]
- Gloth, F.M.; Alam, W.; Hollis, B. Vitamin D vs. broad spectrum phototherapy in the treatment of seasonal affective disorder. J. Nutr. Health Aging 1999, 3, 5–7. [Google Scholar]
- Stumpf, W.E.; Privette, T.H. Light, vitamin D and psychiatry. Psychopharmacology 1989, 97, 285–294. [Google Scholar] [CrossRef]
- Sikoglu, E.M.; Navarro, A.A.L.; Starr, D.; Dvir, Y.; Nwosu, B.U.; Czerniak, S.M.; Rogan, R.C.; Castro, M.C.; Edden, R.A.E.; Frazier, J.A.; et al. Vitamin D3 Supplemental Treatment for Mania in Youth with Bipolar Spectrum Disorders. J. Child Adolesc. Psychopharmacol. 2015, 25, 415–424. [Google Scholar] [CrossRef]
- Bauer, M.E.; Teixeira, A.L. Inflammation in psychiatric disorders: What comes first? Ann. N. Y. Acad. Sci. 2019, 1437, 57–67. [Google Scholar] [CrossRef]
- Moghaddam, B.; Bolinao, M.L.; Stein-Behrens, B.; Sapolsky, R. Glucocortcoids mediate the stress-induced extracellular accumulation of glutamate. Brain Res. 1994, 655, 251–254. [Google Scholar] [CrossRef]
- Marazziti, D.; Mangiapane, P.; Carbone, M.G.; Morana, F.; Arone, A.; Massa, L.; Palermo, S.; Violi, M.; Bertini, G.; Massoni, L.; et al. Decreased Levels of Vitamin D in Bipolar Patients. Life 2023, 13, 883. [Google Scholar] [CrossRef]
- Mokhtari, Z.; Hekmatdoost, A.; Nourian, M. Antioxidant efficacy of vitamin D. J. Parathyr. Dis. 2017, 5, 11–16. [Google Scholar]
- Puchacz, E.; Stumpf, W.E.; Stachowiak, E.K.; Stachowiak, M.K. Vitamin D increases expression of the tyrosine hydroxylase gene in adrenal medullary cells. Mol. Brain Res. 1996, 36, 193–196. [Google Scholar] [CrossRef]
- Kaneko, I.; Sabir, M.S.; Dussik, C.M.; Whitfield, G.K.; Karrys, A.; Hsieh, J.-C.; Haussier, M.R.; Meyer, M.B.; Pike, J.W.; Jurutka, P.W. 1,25-Dihydroxyvitamin D regulates expression of the tryptophan hydroxylase 2 and leptin genes: Implication for behavioral influences of vitamin D. FASEB J. 2015, 29, 4023–4035. [Google Scholar] [CrossRef]
- Watson, S.; Mackin, P. HPA axis function in mood disorders. Psychiatry 2009, 8, 97–101. [Google Scholar] [CrossRef]
- Ressler, K.J.; Nemeroff, C.B. Role of norepinephrine in the pathophysiology and treatment of mood disorders. Biol. Psychiatry 1999, 46, 1219–1233. [Google Scholar] [CrossRef] [PubMed]
- Diehl, D.J.; Gershon, S. The role of dopamine in mood disorders. Compr. Psychiatry 1992, 33, 115–120. [Google Scholar] [CrossRef] [PubMed]
- Golden Robert, N.; Gilmore John, H. Serotonin and Mood Disorders. Psychiatr. Ann. 1990, 20, 580–586. [Google Scholar] [CrossRef]
- Petrov, B.; Aldoori, A.; James, C.; Yang, K.; Algorta, G.P.; Lee, A.; Zhang, L.; Lin, T.; Awadhi, R.A.; Parquette, J.R.; et al. Bipolar disorder in youth is associated with increased levels of vitamin D-binding protein. Transl. Psychiatry 2018, 8, 61. [Google Scholar] [CrossRef] [PubMed]
- Chen, W.-Y.; Huang, M.-C.; Chiu, C.C.; Cheng, Y.-C.; Kuo, C.-J.; Chen, P.-Y.; Kuo, P.-H. The interactions between vitamin D and neurofilament light chain levels on cognitive domains in bipolar disorder. BJPsych Open 2022, 8, e207. [Google Scholar] [CrossRef]
- Alagöl, F.; Shihadeh, Y.; Boztepe, H.; Tanakol, R.; Yarman, S.; Azizlerli, H.; Sandalci, Ö. Sunlight exposure and vitamin D deficiency in Turkish women. J. Endocrinol. Investig. 2000, 23, 173–177. [Google Scholar] [CrossRef]
- Menkes, D.B.; Lancaster, K.; Grant, M.; Marsh, R.W.; Dean, P.; du Toit, S.A. Vitamin D status of psychiatric inpatients in New Zealand’s Waikato region. BMC Psychiatry 2012, 12, 68. [Google Scholar] [CrossRef]
- Sylvia, L.G.; Shelton, R.C.; Kemp, D.E.; Bernstein, E.E.; Friedman, E.S.; Brody, B.D.; McElroy, S.L.; Singh, V.; Tohen, M.; Bowden, C.L.; et al. Medical burden in bipolar disorder: Findings from the Clinical and Health Outcomes Initiative in Comparative Effectiveness for Bipolar Disorder study (Bipolar CHOICE). Bipolar Disord. 2015, 17, 212–223. [Google Scholar] [CrossRef] [PubMed]
- SayuriYamagata, A.; Brietzke, E.; Rosenblat, J.D.; Kakar, R.; McIntyre, R.S. Medical comorbidity in bipolar disorder: The link with metabolic-inflammatory systems. J. Affect. Disord. 2017, 211, 99–106. [Google Scholar] [CrossRef]
- Li, S.; Qui, Y.; Teng, Z.; Chen, J.; Kang, D.; Tang, H.; Xiang, H.; Wu, C.; Tan, Y.; Wang, L.; et al. Association Between Bipolar Disorder and Low Bone Mass: A Cross-Sectional Study With Newly Diagnosed, Drug-Naïve Patients. Front. Psychiatry 2020, 11, 530. [Google Scholar] [CrossRef] [PubMed]
- Su, J.-A.; Cheng, B.-H.; Huang, Y.-C.; Lee, C.-P.; Yang, Y.-H.; Lu, M.-L.; Hsu, C.-Y.; Lee, Y.; McIntyre, R.S.; Chin Lin, T.; et al. Bipolar disorder and the risk of fracture: A nationwide population-based cohort study. J. Affect. Disord. 2017, 218, 246–252. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Bipolar Mania | Healthy Control | p-Value 2 | |
|---|---|---|---|
| n = 34 1 | n = 34 1 | ||
| Age | 37.82 ± 10.42 | 35.26 ± 10.79 | 0.32 |
| Gender | 0.81 | ||
| Female | 19.0 (55.9%) | 18.0 (52.9%) | |
| Male | 15.0 (44.1%) | 16.0 (47.1%) | |
| Number of manic episodes | 4.56 ± 2.51 | ||
| Disease duration(year) | 11.41 ± 7.86 | ||
| Psychotic | |||
| Psychotic | 12.0 (35.3%) | ||
| Non-psychotic | 22.0 (64.7%) | ||
| Treatment | |||
| Lit + antipsychotic | 17.0 (50.0%) | ||
| Valp + antipsychotic | 10.0 (29.4%) | ||
| Other mood stabilizers + antipsychotic | 5.0 (14.7%) | ||
| Lit + valp + antipsychotic | 2.0 (5.9%) | ||
| Vit D supplement | 19 (55.9%) |
| Bipolar Mania | Healthy Control | p-Value 2 | |
|---|---|---|---|
| n = 34 1 | n = 34 1 | ||
| Vit D (ng/mL) | 10.46 ± 4.93 | 16.43 ± 5.28 | <0.001 |
| Ca (mg/dL) | 9.69 ± 0.37 | 9.70 ± 0.47 | 0.89 |
| P (mg/dL) | 3.31 ± 0.57 | 3.46 ± 0.46 | 0.27 |
| Bipolar Euthymic | Healthy Control | p-Value 2 | |
|---|---|---|---|
| n = 34 1 | n = 34 1 | ||
| Vit D (ng/mL) | 15.53 ± 7.90 | 16.43 ± 5.28 | 0.58 |
| Ca (mg/dL) | 9.79 ± 0.44 | 9.70 ± 0.47 | 0.44 |
| P (mg/dL) | 3.43 ± 0.62 | 3.46 ± 0.46 | 0.86 |
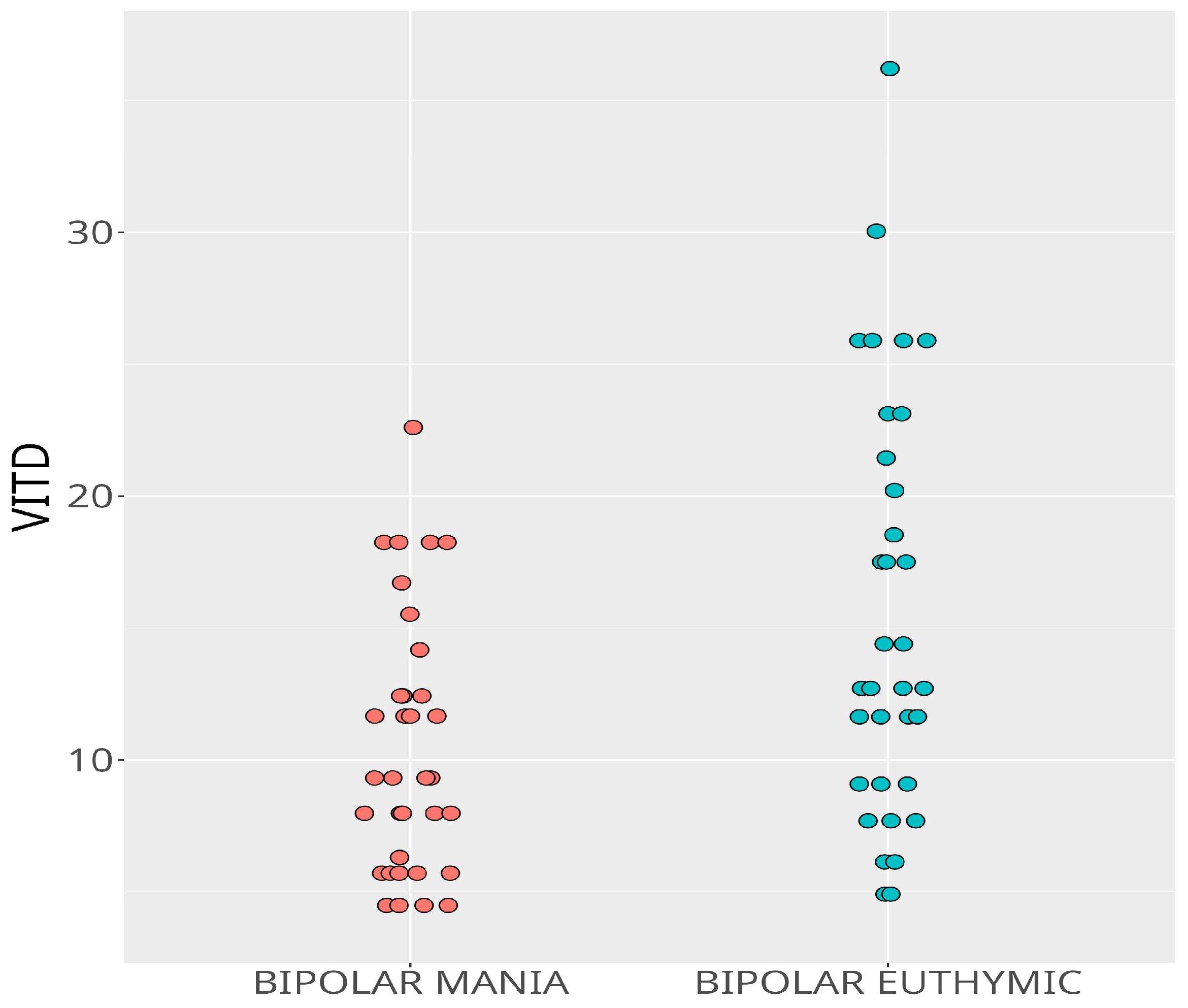
| Bipolar Mania | Bipolar Euthymic | p-Value 2 | |
|---|---|---|---|
| n = 34 1 | n= 34 1 | ||
| Vit D (ng/mL) | 10.46 ± 4.93 | 15.53 ± 7.90 | <0.001 |
| Ca (mg/dL) | 9.69 ± 0.37 | 9.79 ± 0.44 | 0.19 |
| P (mg/dL) | 3.31 ± 0.57 | 3.43 ± 0.62 | 0.16 |
| Age | Number of Manic Episodes | Disease Duration | Vit D | ||
|---|---|---|---|---|---|
| 1 | Age | ||||
| 2 | Number of manic episodes | 0.46 ** | |||
| 3 | Disease duration | 0.81 *** | 0.72 *** | ||
| 4 | Vit D | 0.08 | 0.12 | −0.05 |
| Bipolar Mania | Bipolar Euthymic | Healthy Control | p-Value | |
|---|---|---|---|---|
| n = 34 | n= 34 | n = 34 | ||
| Vit D | <0.001 | |||
| Deficient < 10 ng/mL | 19 (55.8%) | 10 (29.4%) | 0 (0%) | |
| Insufficient 10–20 ng/mL | 14 (41.2%) | 14 (41.2%) | 26 (76.4%) | |
| Sufficient > 20 ng/mL | 1 (3%) | 10 (29.4%) | 8 (23.6%) | |
| Ca | ||||
| Low < 8.8 mg/dL | 0 (0%) | 0 (0%) | 0 (0%) | |
| High > 10.6 mg/dL | 0 (0%) | 0 (0%) | 0 (0%) | |
| P | ||||
| Low < 2.6 mg/dL | 2 (5.8%) | 2 (5.8%) | 2 (5.8%) | |
| High > 4.5 mg/dL | 0 (0%) | 0 (0%) | 0 (0%) | |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
İmre, O.; Karaağaç, M.; Caglayan, C. Does Decreased Vitamin D Level Trigger Bipolar Manic Attacks? Behav. Sci. 2023, 13, 779. https://doi.org/10.3390/bs13090779
İmre O, Karaağaç M, Caglayan C. Does Decreased Vitamin D Level Trigger Bipolar Manic Attacks? Behavioral Sciences. 2023; 13(9):779. https://doi.org/10.3390/bs13090779
Chicago/Turabian Styleİmre, Okan, Mustafa Karaağaç, and Cuneyt Caglayan. 2023. "Does Decreased Vitamin D Level Trigger Bipolar Manic Attacks?" Behavioral Sciences 13, no. 9: 779. https://doi.org/10.3390/bs13090779
APA Styleİmre, O., Karaağaç, M., & Caglayan, C. (2023). Does Decreased Vitamin D Level Trigger Bipolar Manic Attacks? Behavioral Sciences, 13(9), 779. https://doi.org/10.3390/bs13090779