



What Sustains Mask-Wearing Behavior among Elders in a Rural Community in the Post-COVID-19 Era: An Exploratory Mixed-Methods Study
 ,
,
Abstract
1. Introduction
2. Materials and Methods
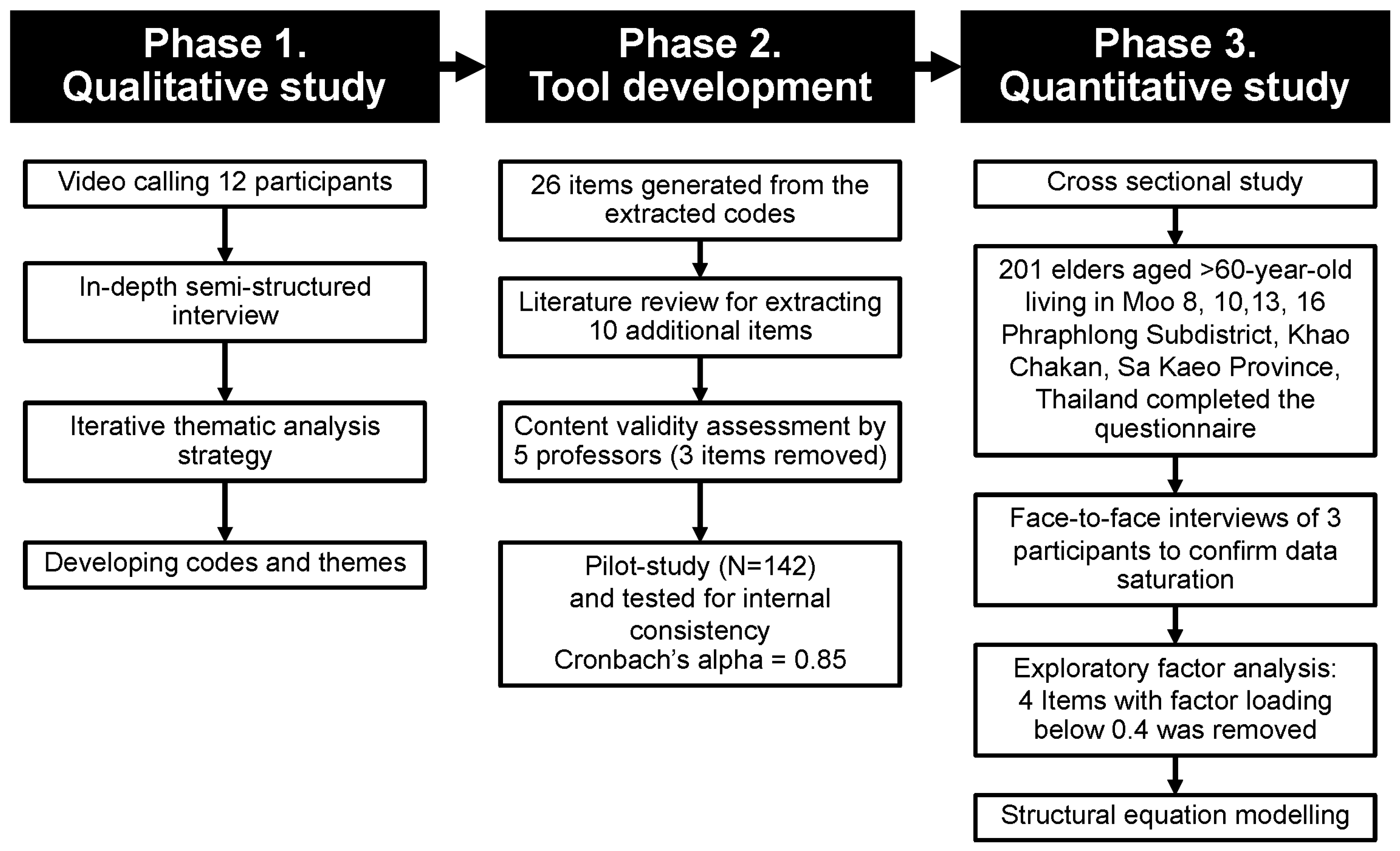
2.1. Study Design and Subjects
2.1.1. Qualitative Phase
2.1.2. Questionnaire’s Development Phase
2.1.3. Quantitative Phase
2.2. Data Collection
2.2.1. Qualitative Phase
2.2.2. Quantitative Phase
2.3. Statistical Analysis
2.3.1. Qualitative Phase
2.3.2. Quantitative Phase
3. Results
3.1. Qualitative Phase
3.1.1. Facilitators/Motivators
3.1.2. Barriers/Obstacles
3.2. Quantitative Phase
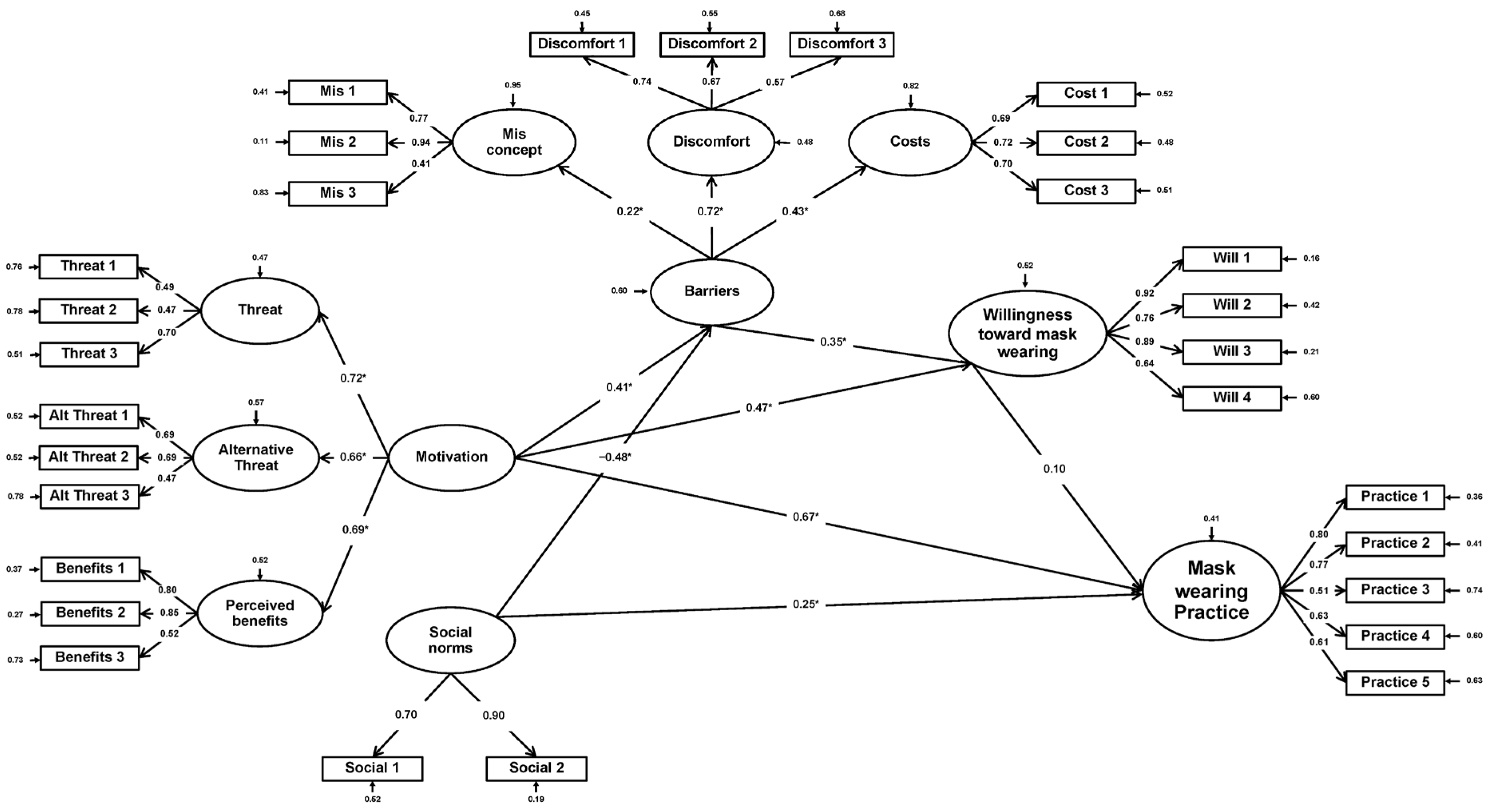
3.3. Structural Equation Modelling
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Eikenberry, S.E.; Mancuso, M.; Iboi, E.; Phan, T.; Eikenberry, K.; Kuang, Y.; Kostelich, E.; Gumel, A.B. To Mask or Not to Mask: Modeling the Potential for Face Mask Use by the General Public to Curtail the COVID-19 Pandemic. Infect. Dis. Model. 2020, 5, 293–308. [Google Scholar] [CrossRef] [PubMed]
- Lubega, G.B.; Mendoza, H.; Nkeramahame, J.; Niyongabo, F.; Gonza, J.; Nakachwa, B.; Musoke, D. Community Mask Wearing as a COVID-19 Preventive Measure, Its Barriers, and Motivators among Rural Households of Uganda: A Mixed Methods Approach. PLoS Glob. Public Health 2022, 2, e0000485. [Google Scholar] [CrossRef] [PubMed]
- Arunnart, M. Efficiency of Commercial Face Masks in PM2.5 Prevention. Ramathibodi Med. J. 2021, 44, 11–17. [Google Scholar] [CrossRef]
- Fold, N.R.; Allison, M.R.; Wood, B.C.; Thao, P.T.B.; Bonnet, S.; Garivait, S.; Kamens, R.; Pengjan, S. An Assessment of Annual Mortality Attributable to Ambient PM2.5 in Bangkok, Thailand. Int. J. Environ. Res. Public Health 2020, 17, 7298. [Google Scholar] [CrossRef] [PubMed]
- Kodros, J.K.; O’Dell, K.; Samet, J.M.; L’Orange, C.; Pierce, J.R.; Volckens, J. Quantifying the Health Benefits of Face Masks and Respirators to Mitigate Exposure to Severe Air Pollution. Geohealth 2021, 5, e2021GH000482. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization. Coronavirus Disease (COVID-19): Masks. 13 January 2023. Available online: https://www.who.int/Emergencies/Diseases/Novel-Coronavirus-2019/Question-and-Answers-Hub/q-a-Detail/Coronavirus-Disease-COVID-19-Masks (accessed on 25 March 2023).
- Rojpaisarnkit, K.; Kaewpan, W.; Pengpid, S.; Peltzer, K. COVID-19 Preventive Behaviors and Influencing Factors in the Thai Population: A Web-Based Survey. Front. Public Health 2022, 10, 816464. [Google Scholar] [CrossRef] [PubMed]
- Vicerra, P.M.M. Disparity between Knowledge and Practice Regarding COVID-19 in Thailand: A Cross-Sectional Study of Older Adults. PLoS ONE 2021, 16, e0259154. [Google Scholar] [CrossRef]
- Kaewpan, W.; Rojpaisarnkit, K.; Pengpid, S.; Peltzer, K. Factors Affecting Face Mask-Wearing Behaviors to Prevent COVID-19 among Thai People: A Binary Logistic Regression Model. Front. Psychol. 2022, 13, 996189. [Google Scholar] [CrossRef]
- He, W.; Cai, D.; Geng, G.; Klug, D. Factors Influencing Wearing Face Mask in Public during COVID-19 Outbreak: A Qualitative Study. Disaster Med. Public Health Prep. 2023, 17, e141. [Google Scholar] [CrossRef]
- Badillo-Goicoechea, E.; Chang, T.-H.; Kim, E.; LaRocca, S.; Morris, K.; Deng, X.; Chiu, S.; Bradford, A.; Garcia, A.; Kern, C.; et al. Global Trends and Predictors of Face Mask Usage during the COVID-19 Pandemic. BMC Public Health 2021, 21, 2099. [Google Scholar] [CrossRef]
- Irfan, M.; Akhtar, N.; Ahmad, M.; Shahzad, F.; Elavarasan, R.M.; Wu, H.; Yang, C. Assessing Public Willingness to Wear Face Masks during the COVID-19 Pandemic: Fresh Insights from the Theory of Planned Behavior. Int. J. Environ. Res. Public Health 2021, 18, 4577. [Google Scholar] [CrossRef] [PubMed]
- Esmaeilzadeh, P. Public Concerns and Burdens Associated with Face Mask-Wearing: Lessons Learned from the COVID-19 Pandemic. Progress. Disaster Sci. 2022, 13, 100215. [Google Scholar] [CrossRef]
- Pramaunururut, P.; Anuntakulnathee, P.; Wangroongsarb, P.; Vongchansathapat, T.; Romsaithong, K.; Rangwanich, J.; Nukaeow, N.; Chansaenwilai, P.; Greeviroj, P.; Worawitrattanakul, P.; et al. Alcohol Consumption and Its Associated Factors among Adolescents in a Rural Community in Central Thailand: A Mixed-Methods Study. Sci. Rep. 2022, 12, 19605. [Google Scholar] [CrossRef] [PubMed]
- Braun, V.; Clarke, V. To saturate or not to saturate? Questioning data saturation as a useful concept for thematic analysis and sample-size rationales. Qual. Res. Sport Exerc. Health 2021, 13, 201–216. [Google Scholar] [CrossRef]
- Kwon, M.; Yang, W. Mask-Wearing Behaviors after Two Years of Wearing Masks Due to COVID-19 in Korea: A Cross-Sectional Study. Int. J. Environ. Res. Public Health 2022, 19, 14940. [Google Scholar] [CrossRef]
- Sharma, P.; Kaur, N. Investment Attitude of Working Women: A Study of Education Sector in Punjab. J. Technol. Manag. Grow. Econ. 2019, 10, 81–87. [Google Scholar] [CrossRef]
- Department of Disease Control Recommendation of COVID-19 Prevention in Post Pandemic for Citizen. Available online: https://ddc.moph.go.th/viralpneumonia/int_protection.php (accessed on 24 March 2023).
- Hojat, M.; DeSantis, J.; Shannon, S.C.; Mortensen, L.H.; Speicher, M.R.; Bragan, L.; LaNoue, M.; Calabrese, L.H. The Jefferson Scale of Empathy: A Nationwide Study of Measurement Properties, Underlying Components, Latent Variable Structure, and National Norms in Medical Students. Adv. Health Sci. Educ. 2018, 23, 899–920. [Google Scholar] [CrossRef]
- Braun, V.; Clarke, V. Using Thematic Analysis in Psychology. Qual. Res. Psychol. 2006, 3, 77–101. [Google Scholar] [CrossRef]
- Hair, J.F.; Ringle, C.M.; Sarstedt, M. PLS-SEM: Indeed a Silver Bullet. J. Mark. Theory Pract. 2011, 19, 139–152. [Google Scholar] [CrossRef]
- Diamantopoulos, A.; Siguaw, J. Introducing LISREL; SAGE Publications, Ltd.: London, UK, 2000; ISBN 9780761951711. [Google Scholar]
- Schumacker, R.; Lomax, R. A Beginner’s Guide to Structural Equation Modeling; Routledge: London, UK, 2012; ISBN 9781136968563. [Google Scholar]
- Cohen, J. Statistical Power Analysis for the Behavioral Sciences; Routledge: London, UK, 2013; ISBN 9781134742707. [Google Scholar]
- Kingston, A.; Wohland, P.; Wittenberg, R.; Robinson, L.; Brayne, C.; Matthews, F.E.; Jagger, C.; Green, E.; Gao, L.; Barnes, R.; et al. Is Late-Life Dependency Increasing or Not? A Comparison of the Cognitive Function and Ageing Studies (CFAS). Lancet 2017, 390, 1676–1684. [Google Scholar] [CrossRef]
- Padua, L.; Castelli, L.; Gatto, D.M.; Hokkoku, K.; Reale, G.; Pastorino, R.; Loreti, C.; Giovannini, S. Discomfort and Pain Related to Protective Mask-Wearing during COVID-19 Pandemic. J. Pers. Med. 2022, 12, 1443. [Google Scholar] [CrossRef] [PubMed]
- Zhang, S.X.; Looi, K.H.; Li, N.; Wan, X.; Li, J. Individual-Level Heterogeneity in Mask Wearing during the COVID-19 Pandemic in Malaysia. Am. J. Trop. Med. Hyg. 2021, 105, 1516–1518. [Google Scholar] [CrossRef] [PubMed]
- UBOS. The Uganda National Household Survey 19/20; UBOS: Kampala, Uganda, 2021. [Google Scholar]
- Sim, S.; Moey, K.; Tan, N. The Use of Facemasks to Prevent Respiratory Infection: A Literature Review in the Context of the Health Belief Model. Singap. Med. J. 2014, 55, 160. [Google Scholar] [CrossRef] [PubMed]
- Norman, P.; Conner, M. Health Behavior. Curated Ref. Collect. Neurosci. Biobehav. Psychol. 2016, 8, 1–37. [Google Scholar] [CrossRef]
- Asri, A.; Asri, V.; Renerte, B.; Föllmi-Heusi, F.; Leuppi, J.D.; Muser, J.; Nüesch, R.; Schuler, D.; Fischbacher, U. Wearing a Mask—For Yourself or for Others? Behavioral Correlates of Mask Wearing among COVID-19 Frontline Workers. PLoS ONE 2021, 16, e0253621. [Google Scholar] [CrossRef] [PubMed]
- Shelus, V.S.; Frank, S.C.; Lazard, A.J.; Higgins, I.C.A.; Pulido, M.; Richter, A.P.C.; Vandegrift, S.M.; Vereen, R.N.; Ribisl, K.M.; Hall, M.G. Motivations and Barriers for the Use of Face Coverings during the COVID-19 Pandemic: Messaging Insights from Focus Groups. Int. J. Environ. Res. Public Health 2020, 17, 9298. [Google Scholar] [CrossRef]
- Livingston, E.; Desai, A.; Berkwits, M. Sourcing Personal Protective Equipment During the COVID-19 Pandemic. JAMA 2020, 323, 1912. [Google Scholar] [CrossRef]
- Reid, A.E.; Cialdini, R.B.; Aiken, L.S. Social Norms and Health Behavior. In Handbook of Behavioral Medicine; Springer: New York, NY, USA, 2010; pp. 263–274. [Google Scholar]
- Jarernpanit, T. The Rural Constitution for Sustainable Thai Rural Community Development. Kasetsart J. Soc. Sci. 2022, 43, 669–676. [Google Scholar]
- Kaewdech, A.; Nawalerspanya, S.; Assawasuwannakit, S.; Chamroonkul, N.; Jandee, S.; Sripongpun, P. The Use of Andrographis Paniculata and Its Effects on Liver Biochemistry of Patients with Gastrointestinal Problems in Thailand during the COVID-19 Pandemic: A Cross Sectional Study. Sci. Rep. 2022, 12, 18213. [Google Scholar] [CrossRef] [PubMed]
- Sa-ngiamsuntorn, K.; Suksatu, A.; Pewkliang, Y.; Thongsri, P.; Kanjanasirirat, P.; Manopwisedjaroen, S.; Charoensutthivarakul, S.; Wongtrakoongate, P.; Pitiporn, S.; Chaopreecha, J.; et al. Anti-SARS-CoV-2 Activity of Andrographis Paniculata Extract and Its Major Component Andrographolide in Human Lung Epithelial Cells and Cytotoxicity Evaluation in Major Organ Cell Representatives. J. Nat. Prod. 2021, 84, 1261–1270. [Google Scholar] [CrossRef]
- Suwankesawong, W.; Saokaew, S.; Permsuwan, U.; Chaiyakunapruk, N. Characterization of Hypersensitivity Reactions Reported among Andrographis Paniculata Users in Thailand Using Health Product Vigilance Center (HPVC) Database. BMC Complement. Altern. Med. 2014, 14, 515. [Google Scholar] [CrossRef] [PubMed]
- Wechwithan, S.; Suwankesawong, W.; Sornsrivichai, V.; McNeil, E.B.; Jiraphongsa, C.; Chongsuvivatwong, V. Signal Detection for Thai Traditional Medicine: Examination of National Pharmacovigilance Data Using Reporting Odds Ratio and Reported Population Attributable Risk. Regul. Toxicol. Pharmacol. 2014, 70, 407–412. [Google Scholar] [CrossRef] [PubMed]
- Nagarajan, R.; Rubeshkumar, P.; Jagadeesan, M.; Raju, M.; Sakthivel, M.; Murali, S.; Sendhilkumar, M.; Ilangovan, K.; Harikrishnan, D.; Venkatasamy, V.; et al. Knowledge, Attitude, and Practice towards Face Mask Use among Residents of Greater Chennai Corporation, India, March 2021. Front. Public Health 2022, 10, 938642. [Google Scholar] [CrossRef] [PubMed]
- Cook, C. Mode of Administration Bias. J. Man. Manip. Ther. 2010, 18, 61–63. [Google Scholar] [CrossRef] [PubMed]
- Kaushal, K. Social Desirability Bias in Face to Face Interviews. J. Postgrad. Med. 2014, 60, 415. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Participants Code | Age | Gender | Mask Adherence |
|---|---|---|---|
| QL01 | 64 | Male | Not adhering |
| QL02 | 61 | Female | Adhering |
| QL03 | 65 | Female | Adhering |
| QL04 | 60 | Female | Adhering |
| QL05 | 66 | Female | Adhering |
| QL06 | 64 | Male | Adhering |
| QL07 | 63 | Male | Adhering |
| QL08 | 63 | Male | Not adhering |
| QL09 | 72 | Female | Not adhering |
| QL10 | 61 | Male | Adhering |
| QL11 | 64 | Male | Adhering |
| QL12 | 72 | Male | Adhering |
| QL13 | 67 | Male | Adhering |
| QL14 | 65 | Female | Not adhering |
| QL15 | 63 | Male | Not adhering |
| Subthemes | Quotes | Questionnaire Extraction |
|---|---|---|
| Facilitators/motivators subthemes | ||
| Perceived benefits of mask-wearing | “It provides good protection, and wearing it feels comfortable. Even though the COVID infection rate has decreased, a mask still helps protect our airways.” QL05 | 1. I believe in the effectiveness of face masks for COVID-19 protection. |
| “I wear a mask for dust protection. Dust is the main reason, as there is road construction and non-asphalt roads. When trucks drive by, dirt particles fly up, so I continue wearing a mask.” QL02 | 2. I wear a mask to protect myself from air pollution. | |
| “I am afraid that diseases will come again, not only COVID-19, but also other diseases.” QL08 | 3. I wear a mask to protect myself against other respiratory infections apart from COVID-19. | |
| “I believe that mask-wearing will reduce the spreading of COVID-19. It can protect us when we are close; when we talk, our saliva cannot spread out. Masks cover us individually.” QL12 | 4. I believe that mask-wearing helps reduce the spread of COVID-19. | |
| Perceived threat of COVID-19 | “I rate my anxiety related to COVID-19 as being at its lowest. My anxiety has decreased since there have been no new cases in our community.” QL05 | 5. I believe that COVID-19 is still spreading throughout my community. |
| “I am still worried though. The disease may come back again.” QL08 | 6. I believe that COVID-19 can reemerge in the future. | |
| Why do you choose to wear it even though it can make breathing difficult? “It’s because I am afraid. Afraid of the disease.” QL07 | 7. I still feel anxious about being infected with COVID-19. | |
| Mask-wearing enhancing attractiveness and self-confidence | “I’m confident. When I look in the mirror, I think I look beautiful.” QL09 | 8. I believe that using a face mask makes me look better. |
| “Wearing a mask makes me feel more confident.” QL02 | 9. Wearing a face mask improves my self-esteem. | |
| “… After eating, conversations often occur. Because we may not have brushed our teeth, we worry that there may be unclean substances in our mouths … Wearing a mask can make us smile brightly.” QL02 | 10. I wear a face mask to conceal my poor oral hygiene. | |
| Social norms and new-normal | “When I go out, I always wear a mask because if I don’t and I see other people, they might think that I’m weird or that I don’t care about my own health. Therefore, I make sure to bring a mask with me at all times so that I won’t be criticized by anyone.” QL14 | 11. I am worried about other people’s perspectives when I remove my face mask in public. |
| “I am familiar with masks and wearing them has become a habit. It no longer bothers me.” QL09 | 12. I am familiar with mask-wearing. | |
| “Not everyone wears masks to the event, but the host provides them for those who forget.” QL03 | 13. I wear a face mask because it is a social measure. | |
| “These days, I still see people wearing masks. However, if I am the only one wearing a mask, I will not want to wear it either. But since there are still people wearing masks, being in a group that wears masks is better.” QL07 | 14. I wear a face mask because others are also wearing them. | |
| “I don’t want to talk to or warn him (Mask-wearing) because he will accuse me of being disgusted with him. It’s better to keep my distance and let him figure it out on his own. Keeping my distance is the best option. If I were to warn him, he might accuse me of snubbing him.” QL02 | 15. I feel anxious or disgusted when someone not wearing a mask gets close to me. | |
| Barriers/obstacles subthemes | ||
| Misconceptions about COVID-19 prevention tools | “Don’t be afraid. I have taken green chiretta and been relieved of the disease. Because others believe it, they have also started planting green chiretta.” QL02 | 16. I trusted that Andrographis paniculata could effectively prevent COVID-19, so I reduced my mask-wearing. |
| “The COVID-19 virus can be found in uncooked food because animals that we eat may sometimes be infected with the virus. To prevent infection, it’s important to eat cooked food, use serving spoons, and wash your hands regularly.” QL02 | 17. I trusted that practices such as eating cooked food, using serving spoons, and washing hands could effectively prevent COVID-19, so I reduced my mask-wearing. | |
| “Wearing a cloth mask can protect me against various things, including dust and germs. It can also be washed and reused multiple times. Both cloth masks and surgical masks are similarly effective in preventing illness caused by germs.” QL11 | 18. I trusted that cloth face masks could effectively prevent COVID-19, so I reduced my mask-wearing. | |
| Perceived barriers to mask-wearing | “I cannot wear a mask all the time. It feels tight and makes it hard to breathe.” QL07 | 19. I feel uncomfortable when wearing a mask. |
| “It’s hot. I work in the sun, so it’s hot. I can’t wear it.” QL04 | 20. Wearing a mask impairs my work productivity. | |
| “It is uncomfortable and makes me feel uneasy. Going out is a challenge because it restricts my ability to speak loudly and clearly, which can make it hard for me to communicate with others.” QL07 | 21. Wearing a mask can be an obstacle to communication. | |
| “After wearing it for a while, the material can become irritating, and some children who wear masks develop rashes on their faces.” QL02 | 22. I think that I am allergic to face masks, e.g., itchy, acne, or rash. | |
| Resources to afford face masks | “The fact that they don’t want to wear it is that the mask they have doesn’t meet the standard.” QL02 | 23. I do not have enough high-quality face masks to meet the standard. |
| “I bought them only for my grandchildren who go to school because masks are expensive, whether they come in a pack or a box.” QL10 | 24. The high price is affecting my decision to purchase a face mask. | |
| “If there’s no control over the spread of the disease and contribution of masks, they may not have enough money to purchase them.” QL10 | 25. I do not have enough money to afford using a face mask daily. | |
| “Yes, it definitely increases expenses because people have to keep buying more masks when they run out. It’s definitely an added expense.” QL01 | 26. I think that buying face masks increases my financial burden. | |
| Characteristics | Adhering | Not Adhering | p-Value |
|---|---|---|---|
| n (%) | n (%) | ||
| Sex | 0.446 a | ||
| Male | 62 (78.5) | 17 (21.5) | |
| Female | 101 (82.8) | 21 (17.2) | |
| Age | |||
| Mean ± SD | 68.5 ± 7.8 | 70.6 ± 8.1 | 0.113 b |
| Median (IQR) | 69.5 (64.0–77.0) | 67 (62.0–73.0) | 0.582 c |
| Age groups | 0.479 a | ||
| 60–69 | 97 (83.6) | 19 (16.4) | |
| 70–79 | 46 (79.3) | 12 (20.7) | |
| ≥80 | 20 (74.1) | 7 (25.9) | |
| Status | 0.833 a | ||
| Single | 12 (85.7) | 2 (14.3) | |
| Married | 126 (80.3) | 31 (19.8) | |
| Divorced/widowed | 25 (83.3) | 5 (16.7) | |
| Ethnicity | 0.469 a | ||
| Thai | 161 (81.3) | 37 (18.7) | |
| Laos | 2 (66.7) | 1 (33.3) | |
| Educational level | 0.679 a | ||
| Below primary school | 38 (79.2) | 10 (20.8) | |
| Primary school | 117 (82.4) | 25 (17.6) | |
| Above primary school | 8 (72.7) | 3 (27.3) | |
| Occupation | 0.939 a | ||
| Unemployed | 43 (82.7) | 9 (17.3) | |
| Agriculture | 90 (80.4) | 22 (19.6) | |
| Others | 30 (81.1) | 7 (18.9) | |
| Scheme | 0.439 a | ||
| Universal coverage | 155 (81.6) | 35 (18.4) | |
| Others | 8 (72.7) | 3 (27.3) | |
| Monthly income (THB/month) | 0.555 a | ||
| <1000 | 70 (86.4) | 11 (13.6) | |
| 1000–4999 | 64 (77.1) | 19 (22.9) | |
| 5000–9999 | 11 (78.6) | 3 (21.4) | |
| 10,000–14,999 | 7 (77.8) | 2 (22.2) | |
| ≥15,000 | 11 (78.6) | 3 (21.4) | |
| Alcohol drinking | 0.697 a | ||
| Never | 57 (78.1) | 16 (21.9) | |
| Previous drinker | 36 (81.8) | 8 (18.2) | |
| Current drinker | 70 (83.3) | 14 (16.7) | |
| Smoking status | 0.831 a | ||
| Not-current smoker | 127 (81.4) | 29 (18.6) | |
| Current smoker | 36 (80.0) | 9 (20.0) | |
| Andrographis paniculate usage | 0.565 a | ||
| No | 48 (78.7) | 13 (21.3) | |
| Yes | 115 (82.1) | 25 (17.9) | |
| Score of COVID-19 quiz | 0.077 a | ||
| Less than 8 | 77 (76.2) | 24 (23.8) | |
| 8 or more | 86 (86.0) | 14 (14.0) | |
| Mean ± SD | 7.6 ± 1.4 | 7.1 ± 1.6 | 0.027 b |
| Question Domain | Mask Adherence | Mean ± SD | t | p-Value |
|---|---|---|---|---|
| Overall willingness to wear face masks—Likert scale | Not adhering | 3.07 ± 1.50 | −3.610 | <0.001 |
| Adhering | 3.97 ± 1.36 | |||
| Overall mask-wearing practice—Likert scale | Not adhering | 2.93 ± 1.19 | −12.331 | <0.001 |
| Adhering | 4.41 ± 0.47 | |||
| Overall perceived threat—Likert scale | Not adhering | 2.25 ± 1.12 | −3.106 | <0.001 |
| Adhering | 2.97 ± 1.31 | |||
| Overall alternative perceived threat aside from COVID-19—Likert scale | Not adhering | 2.73 ± 1.57 | −3.551 | <0.001 |
| Adhering | 3.56 ± 1.22 | |||
| Overall misconception in COVID-19 prevention tools—Likert scale | Not adhering | 3.76 ± 1.35 | 0.727 | 0.234 |
| Adhering | 3.58 ± 1.38 | |||
| Overall perceived benefits of face mask—Likert scale | Not adhering | 3.21 ± 1.47 | −4.193 | <0.001 |
| Adhering | 4.08 ± 1.07 | |||
| Overall discomfort when wearing a face mask—Likert scale | Not adhering | 2.98 ± 1.44 | −1.132 | 0.130 |
| Adhering | 3.27 ± 1.38 | |||
| Overall social norms—Likert scale | Not adhering | 3.00 ± 1.69 | −2.498 | 0.007 |
| Adhering | 3.73 ± 1.60 | |||
| Overall budget resources for affording face masks—Likert scale | Not adhering | 3.20 ± 1.44 | −0.528 | 0.299 |
| Adhering | 3.34 ± 1.42 |
| Independent Variable | Barriers | Willingness | Practice | ||||||
|---|---|---|---|---|---|---|---|---|---|
| Dependent Variable | TE | DE | IE | TE | DE | IE | TE | DE | IE |
| Motivation | 0.41 | 0.41 ** | - | 0.61 | 0.47 *** | 0.14 * | 0.68 | 0.67 *** | 0.01 |
| Social norms | −0.48 | −0.48 *** | - | - | - | - | 0.23 | 0.25 ** | −0.02 |
| Barriers | - | - | - | 0.35 | 0.35 ** | - | 0.04 | - | 0.04 |
| Willingness | - | - | - | - | - | - | 0.10 | 0.10 | - |
| R-squared | 0.40 | 0.49 | 0.59 | ||||||
| χ2/df = 1.52, CFI = 0.91, TLI = 0.90, RMSEA = 0.05, and SRMR = 0.07. | |||||||||
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Lertsakulbunlue, S.; Kittisarapong, P.; Pikulkaew, S.; Pusayapaibul, P.; Tangtongsoonthorn, A.; Wichaiboon, C.; Amornchatchawankul, F.; Marsook, S.; Mahaisawariya, S.; Subwongcharoen, N.; et al. What Sustains Mask-Wearing Behavior among Elders in a Rural Community in the Post-COVID-19 Era: An Exploratory Mixed-Methods Study. Behav. Sci. 2023, 13, 678. https://doi.org/10.3390/bs13080678
Lertsakulbunlue S, Kittisarapong P, Pikulkaew S, Pusayapaibul P, Tangtongsoonthorn A, Wichaiboon C, Amornchatchawankul F, Marsook S, Mahaisawariya S, Subwongcharoen N, et al. What Sustains Mask-Wearing Behavior among Elders in a Rural Community in the Post-COVID-19 Era: An Exploratory Mixed-Methods Study. Behavioral Sciences. 2023; 13(8):678. https://doi.org/10.3390/bs13080678
Chicago/Turabian StyleLertsakulbunlue, Sethapong, Pinyada Kittisarapong, Sirikorn Pikulkaew, Pree Pusayapaibul, Apisit Tangtongsoonthorn, Chanunpisut Wichaiboon, Fasai Amornchatchawankul, Suranuch Marsook, Supakrit Mahaisawariya, Nattasit Subwongcharoen, and et al. 2023. "What Sustains Mask-Wearing Behavior among Elders in a Rural Community in the Post-COVID-19 Era: An Exploratory Mixed-Methods Study" Behavioral Sciences 13, no. 8: 678. https://doi.org/10.3390/bs13080678
APA StyleLertsakulbunlue, S., Kittisarapong, P., Pikulkaew, S., Pusayapaibul, P., Tangtongsoonthorn, A., Wichaiboon, C., Amornchatchawankul, F., Marsook, S., Mahaisawariya, S., Subwongcharoen, N., Petcharat, P., Luksanasup, B., Lortharaprasert, T., Tieantanyatip, B., Kantiwong, A., & Jongcherdchootrakul, K. (2023). What Sustains Mask-Wearing Behavior among Elders in a Rural Community in the Post-COVID-19 Era: An Exploratory Mixed-Methods Study. Behavioral Sciences, 13(8), 678. https://doi.org/10.3390/bs13080678