
From Bad to Worse: Safety Behaviors Exacerbate Eating Disorder Fears

Abstract
1. Introduction
2. Methods
2.1. Study Design
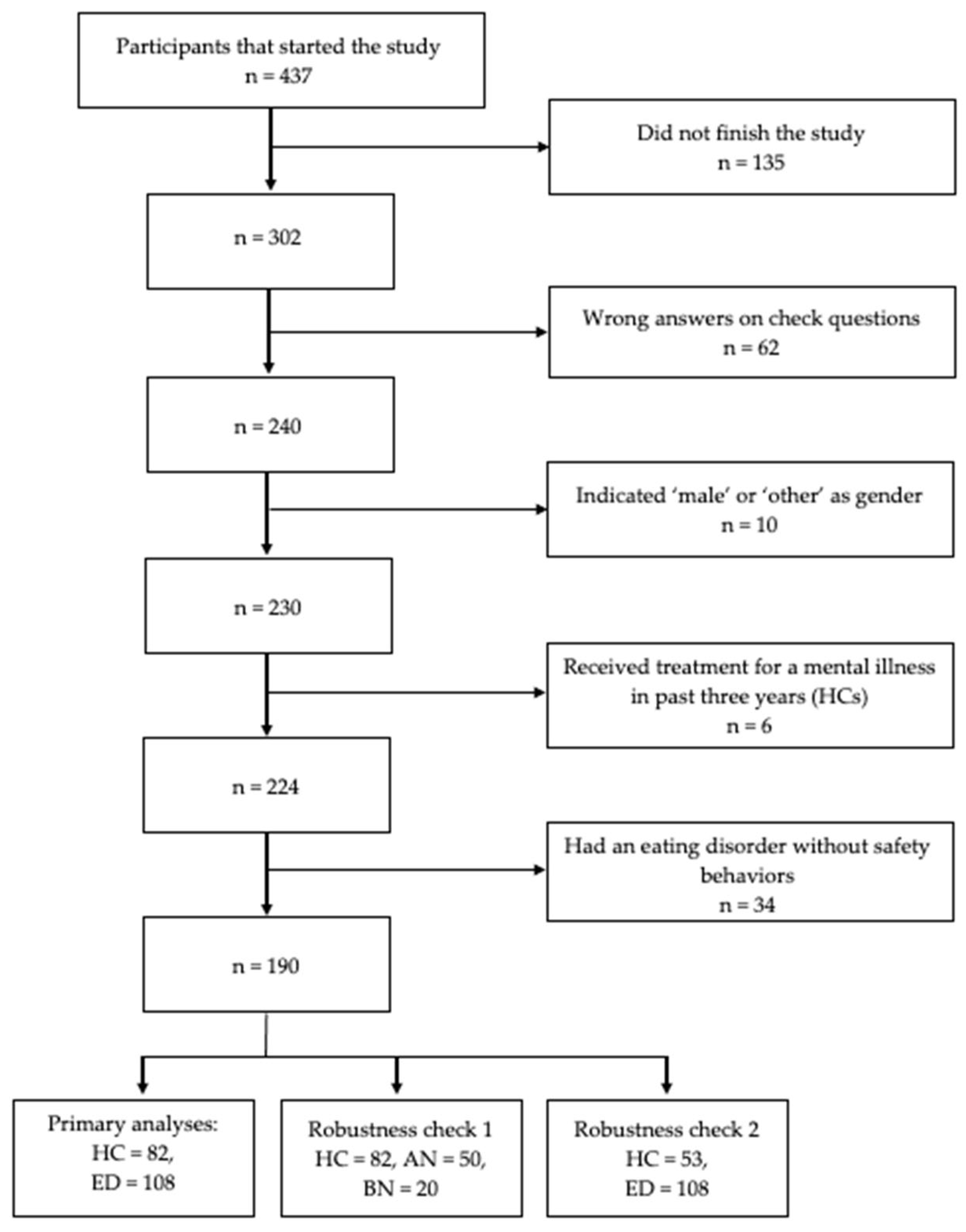
2.2. Participants
2.3. Materials
2.3.1. Vignette Task
“Below several events are described. We ask you to evaluate these events as if they are happening to you. There are no right or wrong answers; we are interested in the way you evaluate them. Try to identify with the events as much as possible and to imagine how you would feel. The descriptions sometimes resemble each other. Therefore, it is important that you read all descriptions very carefully from beginning to end.”
“You come home after a long day. In the kitchen you see a large box of your favorite chocolate.”
“You eat a small piece of chocolate and leave the kitchen. After a few minutes, you find yourself again in the kitchen. You have an intense craving for chocolate. This time you get out the whole box and start to eat. You only stop once the box is empty. You put away the box, walk to the bathroom and make yourself throw up into the toilet.”
“You take the chocolate bars and eat two small pieces. You put away the box, walk to the bathroom and make yourself throw up into the toilet.”
“You eat a small piece of chocolate and leave the kitchen. After a few minutes, you find yourself again in the kitchen. You have an intense craving for chocolate. This time you get out the whole box and start to eat. You only stop once the box is empty. You put away the box and sit down in front of the tv in the living room in order to watch your favorite tv show.”
“You take the chocolate bars and eat two small pieces. You put away the box and sit down in front of the tv in the living room in order to watch your favorite tv show.”
2.3.2. Questionnaires
2.4. Procedure
2.5. Statistical Analysis Plan
3. Results
3.1. Participants
3.2. Manipulation Check
3.3. How Do Safety Behaviors Affect Threat Perception in Individuals with an Eating Disorder and Healthy Controls? (Hypothesis 1 and 2)
3.4. Do Safety Behaviors Affect Threat Perception Differently in Dangerous vs. Safe Situations? (Hypothesis 3)
3.5. Robustness Checks
4. Discussion
Limitations and Future Research
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- American Psychiatric Association. Diagnostic and Statistical Manual of Mental Disorders. 2013. Available online: https://doi.org/10.1176/appi.books.9780890425596 (accessed on 14 December 2022).
- Crisp, A.H.; Hsu, L.K.; Harding, B.; Hartshorn, J. Clinical features of anorexia nervosa. A study of a consecutive series of 102 female patients. J. Psychosom. Res. 1980, 24, 179–191. [Google Scholar] [CrossRef] [PubMed]
- Melles, H.; Spix, M.; Jansen, A. Avoidance in Anorexia Nervosa: Towards a research agenda. Physiol. Behav. 2021, 238, 113478. [Google Scholar] [CrossRef] [PubMed]
- Levinson, C.A.; Vanzhula, I.A.; Christian, C. Development and validation of the eating disorder fear questionnaire and interview: Preliminary investigation of eating disorder fears. Eat. Behav. 2019, 35, 101320. [Google Scholar] [CrossRef] [PubMed]
- Levinson, C.A.; Byrne, M. The fear of food measure: A novel measure for use in exposure therapy for eating disorders: The Fear of Food Measure. Int. J. Eat. Disord. 2015, 48, 271–283. [Google Scholar] [CrossRef] [PubMed]
- Levinson, C.A.; Williams, B.M. Eating disorder fear networks: Identification of central eating disorder fears. Int. J. Eat. Disord. 2020, 53, 1960–1973. [Google Scholar] [CrossRef] [PubMed]
- Melles, H.; Jansen, A. Transdiagnostic fears and avoidance behaviors in self-reported eating disorders. J. Eat. Disord. 2023, 11, 19. [Google Scholar] [CrossRef] [PubMed]
- Schaumberg, K.; Reilly, E.E.; Gorrell, S.; Levinson, C.A.; Farrell, N.R.; Brown, T.A.; Smith, K.M.; Schaefer, L.M.; Essayli, J.H.; Haynos, A.F.; et al. Conceptualizing eating disorder psychopathology using an anxiety disorders framework: Evidence and implications for exposure-based clinical research. Clin. Psychol. Rev. 2021, 83, 101952. [Google Scholar] [CrossRef]
- Brand-Gothelf, A.; Leor, S.; Apter, A.; Fennig, S. The impact of comorbid depressive and anxiety disorders on severity of anorexia nervosa in adolescent girls. J. Nerv. Ment. Dis. 2014, 202, 759–762. [Google Scholar] [CrossRef]
- Murray, S.B.; Strober, M.; Craske, M.G.; Griffiths, S.; Levinson, C.A.; Strigo, I.A. Fear as a translational mechanism in the psychopathology of anorexia nervosa. Neurosci. Biobehav. Rev. 2018, 95, 383–395. [Google Scholar] [CrossRef]
- Raney, T.J.; Thornton, L.M.; Berrettini, W.; Brandt, H.; Crawford, S.; Fichter, M.M.; Halmi, K.A.; Johnson, C.; Kaplan, A.S.; LaVia, M.; et al. Influence of overanxious disorder of childhood on the expression of anorexia nervosa. Int. J. Eat. Disord. 2008, 41, 326–332. [Google Scholar] [CrossRef]
- Swinbourne, J.; Hunt, C.; Abbott, M.; Russell, J.; St Clare, T.; Touyz, S. The comorbidity between eating disorders and anxiety disorders: Prevalence in an eating disorder sample and anxiety disorder sample. Aust. N. Z. J. Psychiatry 2012, 46, 118–131. [Google Scholar] [CrossRef]
- Buckner, J.D.; Silgado, J.; Lewinsohn, P.M. Delineation of differential temporal relations between specific eating and anxiety disorders. J. Psychiatr. Res. 2010, 44, 781–787. [Google Scholar] [CrossRef] [PubMed]
- Zerwas, S.; Lund, B.C.; Von Holle, A.; Thornton, L.M.; Berrettini, W.H.; Brandt, H.; Crawford, S.; Fichter, M.M.; Halmi, K.A.; Johnson, C.; et al. Factors associated with recovery from anorexia nervosa. J. Psychiatr. Res. 2013, 47, 972–979. [Google Scholar] [CrossRef] [PubMed]
- Craske, M.G.; Rauch, S.L.; Ursano, R.; Prenoveau, J.; Pine, D.S.; Zinbarg, R.E. What is an anxiety disorder? Depress. Anxiety 2009, 26, 1066–1085. [Google Scholar] [CrossRef] [PubMed]
- Cuming, S.; Rapee, R.M.; Kemp, N.; Abbott, M.J.; Peters, L.; Gaston, J.E. A self-report measure of subtle avoidance and safety behaviors relevant to social anxiety: Development and psychometric properties. J. Anxiety Disord. 2009, 23, 879–883. [Google Scholar] [CrossRef]
- Deacon, B.; Maack, D.J. The effects of safety behaviors on the fear of contamination: An experimental investigation. Behav. Res. Ther. 2008, 46, 537–547. [Google Scholar] [CrossRef]
- Meulders, A.; Van Daele, T.; Volders, S.; Vlaeyen, J.W.S. The use of safety-seeking behavior in exposure-based treatments for fear and anxiety: Benefit or burden? A meta-analytic review. Clin. Psychol. Rev. 2016, 45, 144–156. [Google Scholar] [CrossRef]
- Christian, C.; Levinson, C.A. An integrated review of fear and avoidance learning in anxiety disorders and application to eating disorders. New Ideas Psychol. 2022, 67, 100964. [Google Scholar] [CrossRef]
- Garcia-Burgos, D.; Wilhelm, P.; Vögele, C.; Munsch, S. Nahrungsvermeidung versus Nahrungsaversion bei restriktiven Essstörungen. Z. Für Psychiatr. Psychol. Psychother. 2019, 67, 30–38. [Google Scholar] [CrossRef]
- Hildebrandt, T.; Grotzinger, A.; Reddan, M.; Greif, R.; Levy, I.; Goodman, W.; Schiller, D. Testing the disgust conditioning theory of food-avoidance in adolescents with recent onset anorexia nervosa. Behav. Res. Ther. 2015, 71, 131–138. [Google Scholar] [CrossRef]
- Pittig, A.; Wong, A.H.K.; Glück, V.M.; Boschet, J.M. Avoidance and its bi-directional relationship with conditioned fear: Mechanisms, moderators, and clinical implications. Behav. Res. Ther. 2020, 126, 103550. [Google Scholar] [CrossRef]
- Summers, B.J.; Cougle, J.R. An experimental test of the role of appearance-related safety behaviors in body dysmorphic disorder, social anxiety, and body dissatisfaction. J. Abnorm. Psychol. 2018, 127, 770–780. [Google Scholar] [CrossRef]
- Olatunji, B.O.; Etzel, E.N.; Tomarken, A.J.; Ciesielski, B.G.; Deacon, B. The effects of safety behaviors on health anxiety: An experimental investigation. Behav. Res. Ther. 2011, 49, 719–728. [Google Scholar] [CrossRef] [PubMed]
- van Uijen, S.L.; Toffolo, M.B.J. Safety Behavior Increases Obsession-Related Cognitions About the Severity of Threat. Behav. Ther. 2015, 46, 521–531. [Google Scholar] [CrossRef] [PubMed]
- van Vliet, C.M.; Meulders, A.; Vancleef, L.M.G.; Vlaeyen, J.W.S. The Opportunity to Avoid Pain May Paradoxically Increase Fear. J. Pain 2018, 19, 1222–1230. [Google Scholar] [CrossRef]
- van Vliet, C.M.; Meulders, A.; Vancleef, L.M.G.; Vlaeyen, J.W.S. The Perceived Opportunity to Avoid Pain Paradoxically Increases Pain-Related Fear Through Increased Threat Appraisals. Ann. Behav. Med. 2021, 55, 216–227. [Google Scholar] [CrossRef]
- Gangemi, A.; Mancini, F.; van den Hout, M. Behavior as information: “If I avoid, then there must be a danger”. J. Behav. Ther. Exp. Psychiatry 2012, 43, 1032–1038. [Google Scholar] [CrossRef]
- van den Hout, M.; Gangemi, A.; Mancini, F.; Engelhard, I.M.; Rijkeboer, M.M.; van Dams, M.; Klugkist, I. Behavior as information about threat in anxiety disorders: A comparison of patients with anxiety disorders and non-anxious controls. J. Behav. Ther. Exp. Psychiatry 2014, 45, 489–495. [Google Scholar] [CrossRef]
- van Uijen, S.L.; van den Hout, M.A.; Engelhard, I.M. Approach behavior as information. J. Behav. Ther. Exp. Psychiatry 2017, 57, 32–36. [Google Scholar] [CrossRef]
- van Dis, E.A.M.; Krypotos, A.-M.; Zondervan-Zwijnenburg, M.A.J.; Tinga, A.M.; Engelhard, I.M. Safety behaviors toward innocuous stimuli can maintain or increase threat beliefs. Behav. Res. Ther. 2022, 156, 104142. [Google Scholar] [CrossRef]
- Xia, W.; Eyolfson, E.; Lloyd, K.; Vervliet, B.; Dymond, S. Living in fear: Low-cost avoidance maintains low-level threat. J. Behav. Ther. Exp. Psychiatry 2019, 62, 57–64. [Google Scholar] [CrossRef] [PubMed]
- Bulik, C.M.; Sullivan, P.F.; Fear, J.L.; Joyce, P.R. Eating disorders and antecedent anxiety disorders: A controlled study. Acta Psychiatr. Scand. 1997, 96, 101–107. [Google Scholar] [CrossRef] [PubMed]
- Lloyd, E.C.; Haase, A.M.; Foster, C.E.; Verplanken, B. A systematic review of studies probing longitudinal associations between anxiety and anorexia nervosa. Psychiatry Res. 2019, 276, 175–185. [Google Scholar] [CrossRef]
- Steinhausen, H.-C.; Jakobsen, H.; Helenius, D.; Munk-Jørgensen, P.; Strober, M. A nation-wide study of the family aggregation and risk factors in anorexia nervosa over three generations. Int. J. Eat. Disord. 2015, 48, 1–8. [Google Scholar] [CrossRef] [PubMed]
- Yilmaz, Z.; Schaumberg, K.; Halvorsen, M.; Goodman, E.L.; Brosof, L.C.; Crowley, J.J.; Anorexia Nervosa Genetics Initiative; Eating Disorders Working Group of the Psychiatric Genomics Consortium; Tourette Syndrome/Obsessive-Compulsive Disorder Working Group of the Psychiatric Genomics Consortium; Mathews, C.A.; et al. Predicting eating disorder and anxiety symptoms using disorder-specific and transdiagnostic polygenic scores for anorexia nervosa and obsessive-compulsive disorder. Psychol. Med. 2022, 53, 3021–3035. [Google Scholar] [CrossRef]
- Anestis, M.D.; Holm-Denoma, J.M.; Gordon, K.H.; Schmidt, N.B.; Joiner, T.E. The Role of Anxiety Sensitivity in Eating Pathology. Cogn. Ther. Res. 2008, 32, 370–385. [Google Scholar] [CrossRef]
- Strober, M. Pathologic fear conditioning and anorexia nervosa: On the search for novel paradigms. Int. J. Eat. Disord. 2004, 35, 504–508. [Google Scholar] [CrossRef] [PubMed]
- Stoner, S.A.; Fedoroff, I.C.; Andersen, A.E.; Rolls, B.J. Food Preferences and Desire to Eat in Anorexia and Bulimia Nervosa. Int. J. Eat. Disord. 1996, 19, 13–22. [Google Scholar] [CrossRef]
- Fairburn, C.G.; Beglin, S. Eating disorder examination questionnaire (EDE–Q 6.0). In Cognitive Behavior Therapy and Eating Disorders; Fairburn, C.G., Ed.; Guilford Press: New York, NY, USA, 2008; pp. 309–314. [Google Scholar]
- Hilbert, A.; Karwautz, A.; Niederhofer, H.; Munsch, S. Eating Disorder Examination-Questionnaire: Evaluation der deutschsprachigen Übersetzung. / Eating Disorder Examination-Questionnaire: Psychometric properties of the German version. Diagnostica 2007, 53, 144–154. [Google Scholar] [CrossRef]
- Lovibond, S.H.; Lovibond, P.F. Psychology Foundation of Australia. Manual for the Depression Anxiety Stress Scales; Psychology Foundation of Australia: Sydney, Australia, 1995. [Google Scholar]
- Nilges, P.; Essau, C. DASS. Depressions-Angst-Stress-Skalen—Deutschsprachige Kurzfassung. 2021. Available online: https://www.psycharchives.org/en/item/5bcda8ff-b672-43e3-a6e8-6cbc598bf37e (accessed on 12 January 2022).
- de Beurs, E.; Van Dyck, R.; Marquenie, L.A.; Lange, A.; Blonk, R.W.B. De DASS: Een vragenlijst voor het meten van depressie, angst en stress. [The DASS: A questionnaire for the measurement of depression, anxiety, and stress.]. Gedragstherapie 2001, 34, 35–53. [Google Scholar]
- Brown, V.A. An Introduction to Linear Mixed-Effects Modeling in R. Adv. Methods Pract. Psychol. Sci. 2021, 4, 2515245920960351. [Google Scholar] [CrossRef]
- Gueorguieva, R.; Krystal, J.H. Move Over ANOVA: Progress in Analyzing Repeated-Measures Data and Its Reflection in Papers Published in the Archives of General Psychiatry. Arch. Gen. Psychiatry 2004, 61, 310–317. [Google Scholar] [CrossRef]
- Papalini, S.; Beckers, T.; Claes, L.; Vervliet, B. The drive for thinness: Towards a mechanistic understanding of avoidance behaviors in a non-clinical population. Behav. Res. Ther. 2021, 142, 103868. [Google Scholar] [CrossRef] [PubMed]
- Spix, M.; Schutzeichel, F.; Jansen, A. Can you learn to starve yourself? Inducing food avoidance in the laboratory. Behav. Res. Ther. 2023, 166, 104340. [Google Scholar] [CrossRef]
- Bates, D.; Mächler, M.; Bolker, B.; Walker, S. Fitting Linear Mixed-Effects Models Using lme4. J. Stat. Softw. 2015, 67, 1–48. [Google Scholar] [CrossRef]
- Lenth, R.V.; Buerkner, P.; Herve, M.; Love, J.; Miguez, F.; Riebl, H.; Singmann, H. emmeans: Estimated Marginal Means, aka Least-Squares Means 2022. Available online: https://CRAN.R-project.org/package=emmeans (accessed on 18 November 2021).
- Ben-Shachar, M.; Lüdecke, D.; Makowski, D. effectsize: Estimation of Effect Size Indices and Standardized Parameters. J. Open Source Softw. 2020, 5, 2815. [Google Scholar] [CrossRef]
- Meulders, A.; Franssen, M.; Fonteyne, R.; Vlaeyen, J.W.S. Acquisition and extinction of operant pain-related avoidance behavior using a 3 degrees-of-freedom robotic arm. Pain 2016, 157, 1094–1104. [Google Scholar] [CrossRef]
- Festinger, L. A Theory of Cognitive Dissonance; Stanford University Press: Stanford, CA, USA, 1962; ISBN 978-0-8047-0911-8. [Google Scholar]
- McMillan, W.; Stice, E.; Rohde, P. High- and low-level dissonance-based eating disorder prevention programs with young women with body image concerns: An experimental trial. J. Consult. Clin. Psychol. 2011, 79, 129–134. [Google Scholar] [CrossRef]
- Pittig, A.; Wong, A.H.K. Incentive-based, instructed, and social observational extinction of avoidance: Fear-opposite actions and their influence on fear extinction. Behav. Res. Ther. 2021, 137, 103797. [Google Scholar] [CrossRef]
- Treanor, M.; Barry, T.J. Treatment of avoidance behavior as an adjunct to exposure therapy: Insights from modern learning theory. Behav. Res. Ther. 2017, 96, 30–36. [Google Scholar] [CrossRef]
- Pittig, A. Incentive-based extinction of safety behaviors: Positive outcomes competing with aversive outcomes trigger fear-opposite action to prevent protection from fear extinction. Behav. Res. Ther. 2019, 121, 103463. [Google Scholar] [CrossRef] [PubMed]
- Wilver, N.L.; Summers, B.J.; Cougle, J.R. Effects of safety behavior fading on appearance concerns and related symptoms. J. Consult. Clin. Psychol. 2020, 88, 65–74. [Google Scholar] [CrossRef] [PubMed]
- Vogel, M.; Krüger, J.; Junne, F. Eating disorder related research using Amazon Mechanical Turk (MTurk): Friend or foe? Commentary on Burnette et al. (2021). Int. J. Eat. Disord. 2022, 55, 285–287. [Google Scholar] [CrossRef] [PubMed]
- Al-Salom, P.; Miller, C.J. The Problem with Online Data Collection: Predicting Invalid Responding in Undergraduate Samples. Curr. Psychol. 2019, 38, 1258–1264. [Google Scholar] [CrossRef]
- Erfanian, F.; Latifnejad Roudsari, R.; Heydari, A.; Noghani, M. A Narrative on Using Vignettes: Its Advantages and Drawbacks. J. Midwifery Reprod. Health 2020, 8, 2134–2145. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Factor | Description of Objective Danger | ||
|---|---|---|---|
| Dangerous | Safe | ||
| Description of safety behavior | Safety behavior | Safety behavior—Dangerous | Safety behavior—Safe |
| No safety behavior | No safety behavior—Dangerous | No safety behavior—Safe | |
| Variable | 1. | 2. | 3. |
|---|---|---|---|
| Danger | |||
| Threat | 0.86 * | ||
| Pleasantness | −0.51 * | −0.55 * | |
| Want for experience | −0.41 * | −0.44 * | 0.77 * |
| HC (n = 82) | ED (n = 108) | t | df | p | |
|---|---|---|---|---|---|
| Age | 25.11 (6.54) | 28.16 (10.17) | 2.51 | 183.40 | 0.013 |
| BMI | 23.13 (3.59) | 19.20 (3.54) | −7.46 | 185 | <0.001 |
| Lowest BMI After 18th Birthday | 20.71 (2.61) | 15.90 (3.22) | −10.93 | 186 | <0.001 |
| Illness Duration (Years) | - | 11.11 (8.86) | - | - | - |
| Currently in Treatment (%) | - | 69 (63.9%) | - | - | - |
| Treatment Duration (years) | - | 7.12 (6.48) | - | - | - |
| EDEQ Global Score | 1.56 (1.34) | 4.21 (1.13) | 14.47 | 157.87 | <0.001 |
| EDEQ Eating Restraint | 1.15 (1.26) | 4.11 (1.37) | 15.29 | 188 | <0.001 |
| EDEQ Eating Concerns | 0.99 (1.14) | 3.40 (1.37) | 13.19 | 185.94 | <0.001 |
| EDEQ Weight Concerns | 1.97 (1.68) | 4.50 (1.33) | 11.17 | 150.07 | <0.001 |
| EDEQ Shape Concerns | 2.11 (1.65) | 4.83 (1.14) | 12.73 | 136.64 | <0.001 |
| DASS Depression | 8.73 (9.35) | 24.67 (11.54) | 10.49 | 186.41 | <0.001 |
| DASS Anxiety | 7.02 (7.73) | 17.79 (10.90) | 7.94 | 185.95 | <0.001 |
| DASS Stress | 11.27 (9.80) | 23.87 (9.79) | 8.77 | 187 | <0.001 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Spix, M.; Melles, H.; Jansen, A. From Bad to Worse: Safety Behaviors Exacerbate Eating Disorder Fears. Behav. Sci. 2023, 13, 574. https://doi.org/10.3390/bs13070574
Spix M, Melles H, Jansen A. From Bad to Worse: Safety Behaviors Exacerbate Eating Disorder Fears. Behavioral Sciences. 2023; 13(7):574. https://doi.org/10.3390/bs13070574
Chicago/Turabian StyleSpix, Michelle, Hanna Melles, and Anita Jansen. 2023. "From Bad to Worse: Safety Behaviors Exacerbate Eating Disorder Fears" Behavioral Sciences 13, no. 7: 574. https://doi.org/10.3390/bs13070574
APA StyleSpix, M., Melles, H., & Jansen, A. (2023). From Bad to Worse: Safety Behaviors Exacerbate Eating Disorder Fears. Behavioral Sciences, 13(7), 574. https://doi.org/10.3390/bs13070574