Abstract
The COVID-19 lockdown restrictions affected physical performance and cognitive function in older people as they were confined to their homes. There is an association between physical and cognitive functions. Mild Cognitive Impairment (MCI) is a condition that risks progressing to dementia. This study aimed to identify the relationship between handgrip strength (HGS), Timed Up-and-Go (TUG), and MCI in older people during the COVID-19 pandemic restrictions. The cross-sectional study recruited 464 eligible participants for an interview and anthropometric measurement. The Montreal Cognitive Assessment-Basic (MoCA-B), HGS, and TUG were measured in addition to demographic and health characteristics. A total of 398 participants (85.8%) were found to have MCI when screened with the MoCA-B. Their mean age was 71.09 ± 5.81 years. Forward multiple regression analysis demonstrated that HGS (β = 0.032, p < 0.001), education level (β = 2.801, p < 0.001), TUG (β = −0.022, p = 0.013), Thai Geriatric Depression Score, TGDS (β = −0.248, p = 0.011), and age (β = −1.677, p = 0.019) were associated with MCI. A decrease in HGS and an increased TUG might allow for the early detection of MCI and promote physical training in order to reduce the risk of MCI. Further studies can investigate multidomain indicators for MCI, for example, fine motor skills and pinch strength as components of the motor abilities.
1. Introduction
Mild cognitive impairment (MCI) is a condition that affects cognitive functions such as language, visuospatial, memory, and frontal executive functions [1]. The prevalence of MCI has varied depending on the methods of screening or the diagnosis process, areas of study, and the different participants’ characteristics. One study showed that the prevalence of MCI worldwide ranged from 5–36.7%, which included the USA, Europe (e.g., UK, France, Italy, and Spain), Asia (e.g., Hong Kong and Singapore), and Australia [2]. In Thailand, a high prevalence of MCI was found in older people in a rural community of 71.4% [3]. People who have MCI are often found to have a slight deficit in the performance of the instrumental activities of daily living (IADL), but the basic activities of daily living (BADL) remain independent. It is possible for MCI to progress to dementia [4].
Identifying the indicators of MCI may help in the early detection of people who are at risk so that support can be given at an early stage to reduce the chance that the MCI will progress to dementia [5]. A previous study reported that the Montreal Cognitive Assessment meets the criteria for screening tests for the detection of MCI in people over 60 years of age and is better than the Mini-Mental State Examination (MMSE) [6]. The Montreal Cognitive Assessment-Basic (MoCA-B) is one of the screening tools that has been developed for screening for MCI in older people with low education and literacy. It has been developed based on the original MoCA, which was validated in people who had an education of approximately 13 years. Low education and literacy may influence cognitive performance; therefore, the MoCA-B has been validated in people with an education of less than 5 years [7,8].
The evidence shows that there is an association between physical and cognitive function. Low physical activity increases the risk of MCI and dementia [9]. Physical frailty is one of the geriatric syndromes that can develop into dependency and/or mortality and is a predictor of disability [10]. Older people who are physically frail and also have cognitive impairment are considered to be cognitively frail [11]. Handgrip strength (HGS) and walking speed are used as part of the criteria to measure physical frailty in older people using a modified Fried frailty phenotype measure [12]. Studies have reported the association between HGS and the risk of cognition decline [13,14]. Weaker handgrip is found to be associated with cognitive decline over a 7 year period [15]. This suggests that measuring grip strength may be a simple and inexpensive method to identify people who are at risk of cognitive decline. Similarly, people with MCI exhibit more gait and balance impairment [16]. Timed Up-and-Go (TUG) is one of the tests that can be used to assess mobility impairment. TUG can be conducted quickly and it is widely used [17,18,19]. It may be useful as a marker for the early detection of cognitive impairment.
Likewise, there are several common risk factors for cognitive and physical impairment in older people that may increase their risk of developing these diseases. These factors can be evaluated using screening tools, including poor nutrition using the Mini Nutritional Assessment-Short Form (MNA-SF) tool [20,21], difficulties with the daily activities using the ADL assessment tool [22,23,24], depression using the Geriatric Depression Scale (GDS) [25,26,27], and poor sleep quality using the Pittsburgh Sleep Quality Index (PSQI) [28,29]. Preventing or delaying cognitive decline in older persons may be practical with the early detection of these risk factors.
During the COVID-19 pandemic, the lockdown or activity restrictions were in place for more than two years to protect the vulnerable populations who were at high risk [30,31]. As a result, older people spent a long time at home. This worsened physical performance and induced muscular atrophy of the extremities [32]. There is a lack of evidence on cognitive decline among older Thai people in the community in relation to physical parameters such as handgrip strength and TUG. During the restrictions enforced by the nationwide lockdown following the second COVID-19 pandemic in Thailand, we conducted this study on older Thai people who lived in the community and were exposed to the restrictions (June to December 2021) [33]. This study aimed to identify a relationship between HGS and TUG and MCI in older adults, aged over 65 years and living in northern Thailand.
2. Methods
2.1. Study Design and Participants
The methods and results of this study are reported in accordance with the Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) guidelines for cross-sectional studies [34]. The participant recruitment, sampling design, and inclusion and exclusion criteria can be found in our previous study [21]. We briefly provide them again in this study. The cross-sectional study was conducted in Khua Mung Subdistrict, Saraphi District, Chiang Mai Province, Thailand, in July 2021. Sample size was calculated using EpiInfoTM version 7.2 [35] based on the population survey or descriptive study. We used the population size of 934 persons. The expected frequency using the prevalence of cognitive impairment was 10.9% [36]. A confidence interval of 97%, an acceptable margin of error of 4%, and a design effect of 2.0 was set. The total sample size was determined to be 438. We aimed for 10% oversampling, and thus a minimum of 482 people were needed. We used cluster sampling methods in ten villages to recruit the participants. The self-reported history of disease was confirmed with medical records in the health-promoting hospital database. We excluded those who had been diagnosed with dementia, depression, end-stage kidney disease, hepatitis, cirrhosis, autoimmune diseases, cancer, acute trauma, acute illnesses, and those who took steroids. In total, 464 participants were included in the data analysis (Figure 1).
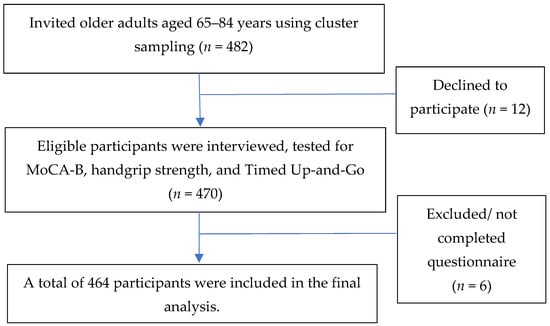
Figure 1.
Diagram of the study participant selection.
2.2. Data Collection and Measurement
Assessments of the participants using MoCA-B were conducted by ten medical students who were trained and supervised to screen for MCI by an occupational therapist who had the Montreal Cognitive Assessment (MoCA) certification (The certification number was THGRIJI69617-02 and it was given by Dr. Nasreddine Ziad).
A questionnaire was used to collect information on demographic and health characteristics, such as age, sex, marital status, education level, living situation, smoking and alcohol use, as well as the participant’s history of hypertension, type 2 diabetes mellitus, dyslipidemia, coronary artery disease, stroke, gout, asthma, chronic obstructive pulmonary disease (COPD), and chronic kidney disease. The participants were interviewed for BADL [37]. Depression was estimated using the Thai Geriatric Depression Scale (TGDS) [25,38]. The Mini Nutritional Assessment-Short Form (MNA-SF) [39,40], Pittsburgh Sleep Quality Index (PSQI) [28,41], Montreal Cognitive Assessment-Basic (MoCA-B) [7,8], Handgrip Strength (HGS), Timed Up-and-Go (TUG), and Body Mass Index (BMI) were also evaluated.
We used the Thai version of the Montreal Cognitive Assessment-Basic (MoCA-B), which was able to identify MCI in individuals who had a low level of education and literacy; literacy-dependent tasks were eliminated. The MoCA-B was validated among community-dwelling elderly Thai persons with low education levels and demonstrated excellent discrimination performance for MCI screening (cutoff score of 24, 81% sensitivity and 86% specificity) [8]. The maximum score was 30. For MCI, the cutoff score was ≤24. For individuals who had <4 years of education, one point was added to the overall score and two points were added for individuals who had <4 years of education and were illiterate. Illiteracy was defined as the inability to read or write fluently in daily living.
Handgrip strength (HGS) was measured using a digital standard dynamometer (T.K.K.5401 GRIP D; Takei Scientific Instruments Co., Ltd., Niigata, Japan). Two measurements were obtained for each hand and the higher value was used [42]. According to the Asian Working Group for Sarcopenia, low grip strength was defined as <28 kg in males and <18 kg in females [43]. We also calculated the %HGS normalized for 28 kg in males and 18 kg in females.
To perform the TUG test, the participants were first asked to stand from a seated position, walk at a comfortable and safe pace to a line on the floor three meters away, turn and walk back to the chair and sit down again [44,45]. TUG in this study adopted the age-specific reference values proposed in a meta-analysis: 9.0 s (65–69 years old), 10.2 s (70–79 years old), and 12.7 s (≥80 years old). Using these cutoff values, subjects were classified as better or worse than the age-specific cutoff value [46].
2.3. Statistical Analysis
The data were analyzed using the IBM SPSS statistical package version 28.0 for Windows (IBM Corp., Armonk, NY, USA). The data were expressed as mean ±SD for normally distributed continuous values (Shapiro–Wilk test), and median [IQR] for non-normally distributed continuous variables. Demographic and health characteristics were reported as frequencies and with percentages. The comparison of mean value of HGS and TUG between non-MCI and MCI was performed using independent sample t-test and Mann–Whitney U test. The association between HGS, TUG, and cognitive function as MoCA-B scores and non-MCI and MCI were analyzed with Pearson correlation and Chi-square tests. Simple linear regression was used to test the association between HGS, TUG, and MoCA-B with pre-defined, potentially associated factors as confounders, e.g., demographic and health characteristics, MNA-SF, ADL, TGDS, and PSQI. Forward multiple linear regression was performed to analyze the association of significant factors in simple linear regression. All statistical tests were two-sided, and a p-value of 0.05 or lower was regarded as statistically significant.
3. Results
3.1. Participants’ Characteristics
A total of 464 older adults were recorded. Table 1 shows the participants’ characteristics. The mean age was 70.76 ± 5.59 years. A total of 58.4% of the participants were female. They had a low level of education (1–3 years (36.6%) or 4–6 years (49.8%), and 93.1% of them did not smoke. Only 55 participants (11.8%) had three or more chronic diseases. There were no significant differences in the baseline characteristics between the non-MCI and MCI groups except age, marital status, and education level. The screening for the score of parameters, such as MNA-SF, BMI, ADL, TGDS, and PSQI, showed that there were no significant differences between the two groups.

Table 1.
Participants’ characteristics by subjective cognitive decline status.
3.2. MoCA-B Scores and Difference between the Non-MCI and MCI Groups
A total of 398 participants (85.8%) were identified as having MCI, with a MoCA-B score of ≤24 (Table 2). The median and interquartile range for all participants’ MoCA-B scores was 20.0 [7.0]. There was a significant difference in the MoCA-B median scores between the non-MCI (median = 26.0, IQR = 2.25) and MCI groups (median = 19.0, IQR = 6.0) (Table 2). Figure S1 shows that the highest failure of cognitive function impairments in each domain among all participants were executive function (94.5%), alternating attention (45.2%), delayed recall (44.5%), and attention (40.5%), respectively. The Figure S2 histogram shows that for all participants, the MoCA-B scores ranged between 4 and 30 points, and the mean ±SD was 19.35 (±4.86).
Table 2.
MoCA-B scores, handgrip strength and Timed Up-and-Go between non-MCI and MCI groups.
3.3. Handgrip Strength and Timed Up-and-Go
The average HGS in males was 24.70 (±7.49) kg and in females was 16.46 kg (±4.67). Between the non-MCI and MCI groups, the mean percent HGS was significantly different (p < 0.001) (Table 2). There were also significant differences in the percent HGS below 100% (poor HGS) between the MCI (86.6%) and non-MCI group (71.2%) (p < 0.001) (Figure S3). The average TUG (s) for all participants aged 65–69 years, 70–79 years, and ≥80 years was 11.38 (±2.70), 12.83 (±3.65), and 14.20 (±3.61), respectively. There was a significantly different mean percent TUG between the MCI and non-MCI groups (p < 0.001) (Table 2). The MCI group’s percent TUG > 100% (bad TUG) was significantly lower than that of the non-MCI group (p = 0.008) (Figure S3).
3.4. Relationship between Handgrip Strength, Timed Up-and-Go, and Mild Cognitive Impairment
The MoCA-B scores were positively associated with the percent HGS (r = 0.281, p < 0.001) (Figure 2a), while they were negatively associated with the percent TUG (r = −0.256, p < 0.001) (Figure 2b). In Figure S3, 86.6% of the participants in the MCI group had a percent HGS < 100% (decreased HGS) and 35.9% had a percent TUG ≥ 100% (increased TUG). In the non-MCI group, 71.2% had a percent HGS < 100% (decreased HGS), and 16.7% had a percent TUG ≥ 100% (increased TUG).
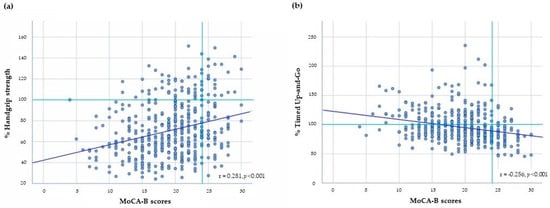
Figure 2.
The relationship between (a) % Handgrip Strength (HGS) and Montreal Cognitive Assessment-Basic (MoCA-B) scores, and (b) % Timed Up-and-Go (TUG) and MoCA-B scores; Significant p-values were analyzed using Pearson correlation coefficient.
3.5. The Factors Associated with MoCA-B Scores
Table 3 presents the factors associated with the MoCA-B scores when using simple linear regression analysis. The following results were all found to be associated with the MoCA-B scores: age (β = −2.987, p < 0.001), marital status (β = −1.004, p = 0.030), education level (β = 4.139, p < 0.001), MNA-SF score (β = 0.137, p = 0.003), TGDS score (β = −0.1404, p < 0.001), percent HGS (β = 0.053, p < 0.001), and percent TUG (β = −0.047, p < 0.001).
Table 3.
Factors associated with mild cognitive impairment using MoCA-B score in older people.
A forward multiple linear regression was performed on the full exploratory model, to identify the factors associated with the MoCA-B scores using the factors that were found to be significant in the simple linear regression. The data were tested for the assumption of collinearity and indicated that multicollinearity was not a concern (Table S1). Age, marital status, education level, MNA-SF score, TGDS score, percent HGS, and percent TUG were entered. The results showed that the MoCA-B score and all factors except marital status and MNA-SF were significantly associated. The significance of these factors in descending order was: percent HGS (β = 0.032, p < 0.001), education level (β = 2.801, p < 0.001), percent TUG (β = −0.022, p = 0.013), TGDS score (β = −0.248, p = 0.011), and age (β = −1.677, p = 0.019). Approximately 15.5% of the variance in the MoCA-B scores was explained by these factors (adjusted R2 = 0.155, p < 0.001) (Table 4).
Table 4.
The exploratory model of factors associated with mild cognitive impairment using MoCA-B scores in older people.
4. Discussion
Mild cognitive impairment (MCI) is a syndrome that risks progressing to dementia in older people [47]. Older people tend to become more inactive as they age, resulting in a deterioration in their physical condition and cognitive function [48,49]. The prevalence of MCI in our study was high at 85.8% and low education was associated with MCI. This was consistent with a previous study, which used the MoCA-B as a screening tool in a rural community in Thailand and found a high prevalence of MCI of 71.4%. The authors found that a low education and diabetes mellitus were significant risk factors [3]. Our study found that there was no difference between males and females in the MCI and non-MCI groups. We excluded older people with depression as depression is commonly found in MCI. Another study reported that the prevalence of depression in MCI ranged between 16.9–55% [50].
Identifying the physical indicators of MCI helps to enable screening and allows preventive intervention programs to support the independence of people at risk of dementia. This study determined that HGS and TUG, which are widely used in research and clinical settings to assess the strength of the handgrip and the balance from sitting to standing as indicators of cognitive function. Using the MoCA-B to screen for MCI in this study showed that alternating attention, delayed recall, and executive function were the most common problems. Our study found that the MoCA-B score was associated with HGS and TUG. In addition, the HGS and TUG scores in the MCI group were significantly poorer than in the non-MCI group. HGS in the MCI group was significantly lower than in the non-MCI group and the TUG in the people with MCI was significantly longer than in the people with non-MCI. These studies demonstrated that there was an association between HGS, functional mobility, and executive function [48,51].
Our study showed that HGS and TUG were physical indicators of cognitive impairment. We found that approximately 15.5% of the variance related to cognitive impairment was explained by the handgrip strength and TUG measures. This was consistent with previous studies showing that low handgrip strength was associated with a risk of cognitive decline [14,15,52,53,54]. HGS could be one of the indicators for cognitive impairment. HGS was found to be associated with cognition especially in executive function tasks [55,56,57]. Our study found that the association between cognitive function and TUG was consistent with previous studies [58,59,60]. TUG measures have been associated with lower levels of cognition. TUG is longer in older people with mild–moderate cognitive impairment or those with Parkinson’s disease. The TUG test is a particularly suitable tool for detecting subtle movement deficits [61].
According to previous studies, the correlation between poor physical condition and cognitive decline might be explained by reduced gray and white matter volumes in multiple brain regions. Muscle strength, volumetric brain measures, and the reduction in handgrip strength have been linked to age markers in the brain [62]. A study explored whether muscle strength, mainly handgrip strength and gait speed, were linked to brain volumetrics and white matter hyperintensity accumulation. The authors found some association between HGS and white matter volume and reported evidence that gait speed was positively related to the whole brain volume [63]. The networks in the brain that control walking involve areas for attention, executive function, and visuospatial functions, as well as motor task control. The cerebellum, basal ganglia, hippocampus, and parietal and frontal cortices have all been linked to executive processes and gait in previous studies [64,65]. Another study found that gait and walking were related to cognitive function, and a decline in gait speed occurred earlier in men than in women [66].
There is little literature on the association between HGS and TUG on cognition decline using the MoCA-B during the COVID-19 restrictions in Thailand. The COVID-19 pandemic has had a significant impact on older adults, particularly in terms of physical activities. Older adults were advised or required to socially distance. This limited their opportunities for social engagement, physical activity, and access to healthcare [67,68]. Older adults with poorer HGS and TUG showed a higher risk of developing MCI. There may be a potential to use muscle strength and mobility tests to identify MCI in older persons because these indicators typically appear considerably earlier than a decline in cognitive function. It is hoped that these simple tests can indicate a difference between those with and without MCI. In addition, future studies with a broader range of cognitive functions and other physical functions are needed to better describe the associations between cognitive and physical function. Other indicators should be investigated to evaluate the common mechanisms for the decline in both cognitive and physical functions. HGS and TUG can be a used to screen as risk factors of MCI and the information can be used to promote physical activities in order to reduce the risk of MCI and dementia. Muscle strength and balance are associated with cognitive functions. This association suggests that there may be potential benefits to physical training and physical activities, such as hand strength training, balance training, and that functional mobility may delay mild cognitive impairment.
This study was strengthened using cluster sampling of the participants. Moreover, we excluded participants who were diagnosed with dementia and depression by doctors, which could cause an incorrect diagnosis of cognitive impairment. However, there were limitations. Firstly, a causal relationship could be established as this was a cross-sectional study. Secondly, the results might not be generalizable to other settings due to the limitations of using data from one sub-district. Thirdly, we did not measure physical activity due to the COVID-19 pandemic restrictions that limited the activities of the participants.
5. Conclusions
Our study shows evidence that HGS and TUG are associated with MCI measured using the MoCA-B in community-dwelling older adults, aged 65–84 years. Given that there is a bidirectional relationship between physical and cognitive functioning, we suggest that these two parameters may be used to screen in order to provide programs that may help in delaying MCI and dementia. Primary care units should establish physical training to delay MCI as early as possible. In the future, it will be useful to screen multidomain parameters to identify the stronger indicators of MCI. Further studies should also identify the fine motor skills and pinch strength as components of the motor abilities to determine if they are associated with a decline in cognitive function.
Supplementary Materials
The following supporting information can be downloaded at: https://www.mdpi.com/article/10.3390/bs13050410/s1, Figure S1: The percentage of cognitive impairment in each domain of the Montreal Cognitive Assessment-Basic (MoCA-B) among all participants (n = 464); Figure S2: Histogram illustrates (a) the Handgrip strength (HGS), 100% muscle strength was determined as 28 kg for males and 18 kg for females; (b) the Timed Up-and-Go (TUG), 100% TUG was determined as 9.0 s (65–69 years), 10.2 s (70–79 years), and 12.7 s (≥80 years); (c) MoCA-B, Montreal Cognitive Assessment-Basic; MoCA-B scores, normal cognitive function MoCA-B scores >24; MCI, mild cognitive impairment MoCA-B scores ≤24. Figure S3: The differences in the prevalence of percent HGS and percent TUG in non-MCI and MCI groups; Table S1: Correlations among scores of MoCA-B, MNA-SF, ADL, TGDS, PSQI, HGS, and TUG.
Author Contributions
Conceptualization, M.S., J.G., W.S. and P.S.; methodology, M.S., P.S., J.G. and W.S.; software, J.G. and P.S.; data validation, M.S., W.S. and P.S.; formal analysis, J.G. and P.S.; investigation, M.S., J.G., W.S. and P.S.; resources, M.S., P.S. and J.G.; data curation, M.S., W.S. and P.S.; writing—original draft preparation, J.G. and P.S.; writing—review and editing, M.S., J.G., W.S. and P.S.; visualization, J.G. and P.S.; supervision, P.S.; project administration, M.S. and P.S.; funding acquisition, M.S. All authors have read and agreed to the published version of the manuscript.
Funding
This research was funded by CMU Junior Research Fellowship Program, Chiang Mai University, Thailand, grant number JRCMU2564_018 and the APC was funded by the Faculty of Medicine, Chiang Mai University, Thailand.
Institutional Review Board Statement
The study was conducted in accordance with the Declaration of Helsinki, and approved by the Research Ethics Committee of the Faculty of Medicine, Chiang Mai University, Thailand (Ethical number: COM-2564-08031).
Informed Consent Statement
Informed consent was obtained from all subjects involved in the study. Written informed consent has been obtained from the patient(s) to publish this paper.
Data Availability Statement
The data presented in this study are available from the corresponding author on reasonable request.
Acknowledgments
We are grateful for the assistance of Khua Mung Health Promoting hospital, village health volunteers, and community leaders. We would like to thank the participants who provided the information for the project.
Conflicts of Interest
The authors declare no conflict of interests.
References
- Jung, Y.H.; Park, S.; Jang, H.; Cho, S.H.; Kim, S.J.; Kim, J.P.; Kim, S.T.; Na, D.L.; Seo, S.W.; Kim, H.J. Frontal-executive dysfunction affects dementia conversion in patients with amnestic mild cognitive impairment. Sci. Rep. 2020, 10, 772. [Google Scholar] [CrossRef] [PubMed]
- Sachdev, P.S.; Lipnicki, D.M.; Kochan, N.A.; Crawford, J.D.; Thalamuthu, A.; Andrews, G.; Brayne, C.; Matthews, F.E.; Stephan, B.C.; Lipton, R.B.; et al. The Prevalence of Mild Cognitive Impairment in Diverse Geographical and Ethnocultural regions: The COSMIC Collaboration. PLoS ONE 2015, 10, e0142388. [Google Scholar] [CrossRef] [PubMed]
- Griffiths, J.; Thaikruea, L.; Wongpakaran, N.; Munkhetvit, P. Prevalence of Mild Cognitive Impairment in Rural Thai Older People, Associated Risk Factors and their Cognitive Characteristics. Dement. Geriatr. Cogn. Dis. Extra 2020, 10, 38–45. [Google Scholar] [CrossRef] [PubMed]
- Jekel, K.; Damian, M.; Wattmo, C.; Hausner, L.; Bullock, R.; Connelly, P.J.; Dubois, B.; Eriksdotter, M.; Ewers, M.; Graessel, E.; et al. Mild cognitive impairment and deficits in instrumental activities of daily living: A systematic review. Alzheimer’s Res. Ther. 2015, 7, 17. [Google Scholar] [CrossRef] [PubMed]
- Brasure, M.; Desai, P.; Davila, H.; Nelson, V.A.; Calvert, C.; Jutkowitz, E.; Butler, M.; Fink, H.A.; Ratner, E.; Hemmy, L.S.; et al. Physical Activity Interventions in Preventing Cognitive Decline and Alzheimer-Type Dementia: A Systematic Review. Ann. Intern. Med. 2018, 168, 30–38. [Google Scholar] [CrossRef]
- Ciesielska, N.; Sokołowski, R.; Mazur, E.; Podhorecka, M.; Polak-Szabela, A.; Kędziora-Kornatowska, K. Is the Montreal Cognitive Assessment (MoCA) test better suited than the Mini-Mental State Examination (MMSE) in mild cognitive impairment (MCI) detection among people aged over 60? Meta-analysis. Psychiatr. Pol. 2016, 50, 1039–1052. [Google Scholar] [CrossRef]
- Nasreddine, Z.S.; Phillips, N.A.; Bédirian, V.; Charbonneau, S.; Whitehead, V.; Collin, I.; Cummings, J.L.; Chertkow, H. The Montreal Cognitive Assessment, MoCA: A brief screening tool for mild cognitive impairment. J. Am. Geriatr. Soc. 2005, 53, 695–699. [Google Scholar] [CrossRef]
- Julayanont, P.; Tangwongchai, S.; Hemrungrojn, S.; Tunvirachaisakul, C.; Phanthumchinda, K.; Hongsawat, J.; Suwichanarakul, P.; Thanasirorat, S.; Nasreddine, Z.S. The Montreal Cognitive Assessment-Basic: A Screening Tool for Mild Cognitive Impairment in Illiterate and Low-Educated Elderly Adults. J. Am. Geriatr. Soc. 2015, 63, 2550–2554. [Google Scholar] [CrossRef]
- Huang, Q.; Zhao, J.; Jiang, W.; Wang, W. The Association between Physical Activity and Cognitive Function: Data from the China Health and Nutrition Survey. Behav Neurol. 2022, 2022, 3438078. [Google Scholar] [CrossRef]
- Tavares, J.; Sa-Couto, P.; Reis, J.D.; Boltz, M.; Capezuti, E. The Role of Frailty in Predicting 3 and 6 Months Functional Decline in Hospitalized Older Adults: Findings from a Secondary Analysis. Int. J. Environ. Res. Public Health 2021, 18, 7126. [Google Scholar] [CrossRef]
- Kelaiditi, E.; Cesari, M.; Canevelli, M.; van Kan, G.A.; Ousset, P.J.; Gillette-Guyonnet, S.; Ritz, P.; Duveau, F.; Soto, M.E.; Provencher, V.; et al. Cognitive frailty: Rational and definition from an (I.A.N.A./I.A.G.G.) international consensus group. J. Nutr. Health Aging 2013, 17, 726–734. [Google Scholar] [CrossRef]
- Lee, L.; Patel, T.; Costa, A.; Bryce, E.; Hillier, L.M.; Slonim, K.; Hunter, S.W.; Heckman, G.; Molnar, F. Screening for frailty in primary care: Accuracy of gait speed and hand-grip strength. Can. Fam. Physician 2017, 63, e51–e57. [Google Scholar]
- Su, H.; Sun, X.; Li, F.; Guo, Q. Association between handgrip strength and cognition in a Chinese population with Alzheimer’s disease and mild cognitive impairment. BMC Geriatr. 2021, 21, 459. [Google Scholar] [CrossRef]
- Cui, M.; Zhang, S.; Liu, Y.; Gang, X.; Wang, G. Grip Strength and the Risk of Cognitive Decline and Dementia: A Systematic Review and Meta-Analysis of Longitudinal Cohort Studies. Front. Aging Neurosci. 2021, 13, 625551. [Google Scholar] [CrossRef]
- Alfaro-Acha, A.; Al Snih, S.; Raji, M.A.; Kuo, Y.F.; Markides, K.S.; Ottenbacher, K.J. Handgrip strength and cognitive decline in older Mexican Americans. J. Gerontol. A Biol. Sci. Med. Sci. 2006, 61, 859–865. [Google Scholar] [CrossRef]
- Auyeung, T.W.; Lee, J.S.; Kwok, T.; Woo, J. Physical frailty predicts future cognitive decline—A four-year prospective study in 2737 cognitively normal older adults. J. Nutr. Health Aging 2011, 15, 690–694. [Google Scholar] [CrossRef]
- Ansai, J.H.; Andrade, L.P.; Nakagawa, T.H.; Rebelatto, J.R. Performances on the Timed Up and Go Test and subtasks between fallers and non-fallers in older adults with cognitive impairment. Arq. Neuropsiquiatr. 2018, 76, 381–386. [Google Scholar] [CrossRef]
- Cruz-Jentoft, A.J.; Baeyens, J.P.; Bauer, J.M.; Boirie, Y.; Cederholm, T.; Landi, F.; Martin, F.C.; Michel, J.P.; Rolland, Y.; Schneider, S.M.; et al. Sarcopenia: European consensus on definition and diagnosis: Report of the European Working Group on Sarcopenia in Older People. Age Ageing 2010, 39, 412–423. [Google Scholar] [CrossRef]
- Chen, L.K.; Liu, L.K.; Woo, J.; Assantachai, P.; Auyeung, T.W.; Bahyah, K.S.; Chou, M.Y.; Chen, L.Y.; Hsu, P.S.; Krairit, O.; et al. Sarcopenia in Asia: Consensus report of the Asian Working Group for Sarcopenia. J. Am. Med. Dir. Assoc. 2014, 15, 95–101. [Google Scholar] [CrossRef]
- Zanetti, M.; Gortan Cappellari, G.; Ratti, C.; Ceschia, G.; Murena, L.; De Colle, P.; Barazzoni, R. Poor nutritional status but not cognitive or functional impairment per se independently predict 1 year mortality in elderly patients with hip-fracture. Clin. Nutr. 2019, 38, 1607–1612. [Google Scholar] [CrossRef]
- Seesen, M.; Sirikul, W.; Ruangsuriya, J.; Griffiths, J.; Siviroj, P. Cognitive Frailty in Thai Community-Dwelling Elderly: Prevalence and Its Association with Malnutrition. Nutrients 2021, 13, 4239. [Google Scholar] [CrossRef] [PubMed]
- Pashmdarfard, M.; Azad, A. Assessment tools to evaluate Activities of Daily Living (ADL) and Instrumental Activities of Daily Living (IADL) in older adults: A systematic review. Med. J. Islam. Repub. Iran 2020, 34, 33. [Google Scholar] [CrossRef] [PubMed]
- Katayama, O.; Lee, S.; Bae, S.; Makino, K.; Shinkai, Y.; Chiba, I.; Harada, K.; Shimada, H. Lifestyle changes and outcomes of older adults with mild cognitive impairment: A 4-year longitudinal study. Arch. Gerontol. Geriatr. 2021, 94, 104376. [Google Scholar] [CrossRef] [PubMed]
- Lee, M.-T.; Jang, Y.; Chang, W.-Y. How do impairments in cognitive functions affect activities of daily living functions in older adults? PLoS ONE 2019, 14, e0218112. [Google Scholar] [CrossRef]
- Yesavage, J.A.; Sheikh, J.I. 9/Geriatric Depression Scale (GDS). Clin. Gerontol. 1986, 5, 165–173. [Google Scholar] [CrossRef]
- Ownby, R.L.; Crocco, E.; Acevedo, A.; John, V.; Loewenstein, D. Depression and risk for Alzheimer disease: Systematic review, meta-analysis, and metaregression analysis. Arch. Gen. Psychiatry 2006, 63, 530–538. [Google Scholar] [CrossRef]
- Jiang, R.; Westwater, M.L.; Noble, S.; Rosenblatt, M.; Dai, W.; Qi, S.; Sui, J.; Calhoun, V.D.; Scheinost, D. Associations between grip strength, brain structure, and mental health in >40,000 participants from the UK Biobank. BMC Med. 2022, 20, 286. [Google Scholar] [CrossRef]
- Buysse, D.J.; Reynolds, C.F., 3rd; Monk, T.H.; Berman, S.R.; Kupfer, D.J. The Pittsburgh Sleep Quality Index: A new instrument for psychiatric practice and research. Psychiatry Res. 1989, 28, 193–213. [Google Scholar] [CrossRef]
- Chien, M.Y.; Chen, H.C. Poor sleep quality is independently associated with physical disability in older adults. J. Clin. Sleep Med. 2015, 11, 225–232. [Google Scholar] [CrossRef]
- Brown, L.; Mossabir, R.; Harrison, N.; Brundle, C.; Smith, J.; Clegg, A. Life in lockdown: A telephone survey to investigate the impact of COVID-19 lockdown measures on the lives of older people (≥75 years). Age Ageing 2021, 50, 341–346. [Google Scholar] [CrossRef]
- Yamada, K.; Yamaguchi, S.; Sato, K.; Fuji, T.; Ohe, T. The COVID-19 outbreak limits physical activities and increases sedentary behavior: A possible secondary public health crisis for the elderly. J. Orthop. Sci. 2020, 25, 1093–1094. [Google Scholar] [CrossRef]
- Pagano, A.F.; Brioche, T.; Arc-Chagnaud, C.; Demangel, R.; Chopard, A.; Py, G. Short-term disuse promotes fatty acid infiltration into skeletal muscle. J. Cachexia Sarcopenia Muscle 2018, 9, 335–347. [Google Scholar] [CrossRef]
- World Health Organization. WHO Health Emergengy Dash Board. WHO (COVID-19) Thailand Situation. Available online: https://covid19.who.int/region/searo/country/th (accessed on 16 December 2022).
- Von Elm, E.; Altman, D.G.; Egger, M.; Pocock, S.J.; Gøtzsche, P.C.; Vandenbroucke, J.P. The Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) statement: Guidelines for reporting observational studies. J. Clin. Epidemiol. 2008, 61, 344–349. [Google Scholar] [CrossRef]
- Center of Disease Control and Prevention. Epi Info™ for Mobile Devices. 2022. Available online: https://www.cdc.gov/epiinfo/mobile.html (accessed on 16 December 2022).
- Chye, L.; Wei, K.; Nyunt, M.S.Z.; Gao, Q.; Wee, S.L.; Ng, T.P. Strong Relationship between Malnutrition and Cognitive Frailty in the Singapore Longitudinal Ageing Studies (SLAS-1 and SLAS-2). J. Prev. Alzheimer’s Dis. 2018, 5, 142–148. [Google Scholar] [CrossRef]
- Tantiritsak, T. (Ed.) Clinical Practice Guidelines: Dementia; Tana Press: Bangkok, Thailand, 2014. [Google Scholar]
- Wongpakaran, N.; Wongpakaran, T. Prevalence of major depressive disorders in long-term care facilities: A report northern Thailand. Psychogeriatrics 2012, 12, 11–17. [Google Scholar] [CrossRef]
- Rubenstein, L.Z.; Harker, J.O.; Salvà, A.; Guigoz, Y.; Vellas, B. Screening for undernutrition in geriatric practice: Developing the short-form mini-nutritional assessment (MNA-SF). J. Gerontol. A Biol. Sci. Med. Sci. 2001, 56, M366–M372. [Google Scholar] [CrossRef]
- Kaiser, M.J.; Bauer, J.M.; Ramsch, C.; Uter, W.; Guigoz, Y.; Cederholm, T.; Thomas, D.R.; Anthony, P.; Charlton, K.E.; Maggio, M.; et al. Validation of the Mini Nutritional Assessment short-form (MNA-SF): A practical tool for identification of nutritional status. J. Nutr. Health Aging 2009, 13, 782–788. [Google Scholar] [CrossRef]
- Methipisit, T.; Mungthin, M.; Saengwanitch, S.; Ruangkana, P.; Chinwarun, Y.; Ruangkanchanasetr, P.; Panichkul, S.; Ukritchon, S.; Mahakit, P.; Sithinamsuwan, P. The Development of Sleep Questionnaires Thai Version (ESS, SA-SDQ, and PSQI): Linguistic Validation, Reliability Analysis and Cut-Off Level to Determine Sleep Related Problems in Thai Population. J. Med. Assoc. Thai 2016, 99, 893–903. [Google Scholar]
- Fox, B.; Henwood, T.; Schaap, L.; Bruyère, O.; Reginster, J.Y.; Beaudart, C.; Buckinx, F.; Roberts, H.; Cooper, C.; Cherubini, A. Adherence to a standardized protocol for measuring grip strength and appropriate cut-off values in adults over 65 years with sarcopenia: A systematic review protocol. JBI Database Syst. Rev. Implement. Rep. 2015, 13, 50–59. [Google Scholar] [CrossRef]
- Chen, L.K.; Woo, J.; Assantachai, P.; Auyeung, T.W.; Chou, M.Y.; Iijima, K.; Jang, H.C.; Kang, L.; Kim, M.; Kim, S.; et al. Asian Working Group for Sarcopenia: 2019 Consensus Update on Sarcopenia Diagnosis and Treatment. J. Am. Med. Dir. Assoc. 2020, 21, 300–307.e2. [Google Scholar] [CrossRef]
- Podsiadlo, D.; Richardson, S. The timed “Up & Go”: A test of basic functional mobility for frail elderly persons. J. Am. Geriatr. Soc. 1991, 39, 142–148. [Google Scholar] [CrossRef] [PubMed]
- Kristensen, M.T.; Bloch, M.L.; Jønsson, L.R.; Jakobsen, T.L. Interrater reliability of the standardized Timed Up and Go Test when used in hospitalized and community-dwelling older individuals. Physiother. Res. Int. 2019, 24, e1769. [Google Scholar] [CrossRef] [PubMed]
- Bohannon, R.W. Reference values for the timed up and go test: A descriptive meta-analysis. J. Geriatr. Phys. Ther. 2006, 29, 64–68. [Google Scholar] [CrossRef] [PubMed]
- Dunne, R.A.; Aarsland, D.; O’Brien, J.T.; Ballard, C.; Banerjee, S.; Fox, N.C.; Isaacs, J.D.; Underwood, B.R.; Perry, R.J.; Chan, D.; et al. Mild Cognitive Impairment: The Manchester consensus. Age Ageing 2020, 50, 72–80. [Google Scholar] [CrossRef] [PubMed]
- Clouston, S.A.; Brewster, P.; Kuh, D.; Richards, M.; Cooper, R.; Hardy, R.; Rubin, M.S.; Hofer, S.M. The dynamic relationship between physical function and cognition in longitudinal aging cohorts. Epidemiol. Rev. 2013, 35, 33–50. [Google Scholar] [CrossRef]
- Cooper, C.; Hardy, R.; Aihie Sayer, A.; Ben-Shlomo, Y.; Birnie, K.; Cooper, C.; Kuh, D.; Craig, L.; Deary, I.J.; Demakakos, P.; et al. Age and gender differences in physical capability levels from mid-life onwards: The harmonisation and meta-analysis of data from eight UK cohort studies. PLoS ONE 2011, 6, e27899. [Google Scholar] [CrossRef]
- Ma, L. Depression, Anxiety, and Apathy in Mild Cognitive Impairment: Current Perspectives. Front. Aging Neurosci. 2020, 12, 9. [Google Scholar] [CrossRef]
- Fastame, M.C.; Mulas, I.; Putzu, V.; Asoni, G.; Viale, D.; Mameli, I.; Pau, M. Executive and Motor Functions in Older Individuals with Cognitive Impairment. Behav. Sci. 2022, 12, 214. [Google Scholar] [CrossRef]
- Kim, K.H.; Park, S.K.; Lee, D.R.; Lee, J. The Relationship between Handgrip Strength and Cognitive Function in Elderly Koreans over 8 Years: A Prospective Population-Based Study Using Korean Longitudinal Study of Ageing. Korean J. Fam. Med. 2019, 40, 9–15. [Google Scholar] [CrossRef]
- Jang, J.Y.; Kim, J. Association between handgrip strength and cognitive impairment in elderly Koreans: A population-based cross-sectional study. J. Phys. Ther. Sci. 2015, 27, 3911–3915. [Google Scholar] [CrossRef]
- Zammit, A.R.; Piccinin, A.M.; Duggan, E.C.; Koval, A.; Clouston, S.; Robitaille, A.; Brown, C.L.; Handschuh, P.; Wu, C.; Jarry, V.; et al. A Coordinated Multi-study Analysis of the Longitudinal Association Between Handgrip Strength and Cognitive Function in Older Adults. J. Gerontol. B Psychol. Sci. Soc. Sci. 2021, 76, 229–241. [Google Scholar] [CrossRef]
- Duchowny, K.A.; Ackley, S.F.; Brenowitz, W.D.; Wang, J.; Zimmerman, S.C.; Caunca, M.R.; Glymour, M.M. Associations Between Handgrip Strength and Dementia Risk, Cognition, and Neuroimaging Outcomes in the UK Biobank Cohort Study. JAMA Netw. Open 2022, 5, e2218314. [Google Scholar] [CrossRef]
- Kunutsor, S.K.; Isiozor, N.M.; Voutilainen, A.; Laukkanen, J.A. Handgrip strength and risk of cognitive outcomes: New prospective study and meta-analysis of 16 observational cohort studies. GeroScience 2022, 44, 2007–2024. [Google Scholar] [CrossRef]
- Herold, F.; Labott, B.K.; Grässler, B.; Halfpaap, N.; Langhans, C.; Müller, P.; Ammar, A.; Dordevic, M.; Hökelmann, A.; Müller, N.G. A Link between Handgrip Strength and Executive Functioning: A Cross-Sectional Study in Older Adults with Mild Cognitive Impairment and Healthy Controls. Healthcare 2022, 10, 230. [Google Scholar] [CrossRef]
- Williams, J.M.; Nyman, S.R. Association between the instrumented timed up and go test and cognitive function, fear of falling and quality of life in community dwelling people with dementia. J. Frailty Sarcopenia Falls 2018, 3, 185–193. [Google Scholar] [CrossRef]
- Ibrahim, A.; Singh, D.K.A.; Shahar, S. ‘Timed Up and Go’ test: Age, gender and cognitive impairment stratified normative values of older adults. PLoS ONE 2017, 12, e0185641. [Google Scholar] [CrossRef]
- Muir, S.W.; Beauchet, O.; Montero-Odasso, M.; Annweiler, C.; Fantino, B.; Speechley, M. Association of executive function impairment, history of falls and physical performance in older adults: A cross-sectional population-based study in eastern France. J. Nutr. Health Aging 2013, 17, 661–665. [Google Scholar] [CrossRef]
- Van Uem, J.M.T.; Walgaard, S.; Ainsworth, E.; Hasmann, S.E.; Heger, T.; Nussbaum, S.; Markus, A.; Hobert, M.A.; Encarnación, M.; Micó-Amigo, E.M.; et al. Quantitative Timed-Up-and-Go Parameters in Relation to Cognitive Parameters and Health-Related Quality of Life in Mild-to-Moderate Parkinson’s Disease. PLoS ONE 2016, 11, e0151997. [Google Scholar] [CrossRef]
- Doi, T.; Makizako, H.; Shimada, H.; Yoshida, D.; Ito, K.; Kato, T.; Ando, H.; Suzuki, T. Brain atrophy and trunk stability during dual-task walking among older adults. J. Gerontol. A Biol. Sci. Med. Sci. 2012, 67, 790–795. [Google Scholar] [CrossRef]
- Kilgour, A.H.M.; Todd, O.M.; Starr, J.M. A systematic review of the evidence that brain structure is related to muscle structure and their relationship to brain and muscle function in humans over the lifecourse. BMC Geriatr. 2014, 14, 85. [Google Scholar] [CrossRef]
- Holtzer, R.; Epstein, N.; Mahoney, J.R.; Izzetoglu, M.; Blumen, H.M. Neuroimaging of mobility in aging: A targeted review. J. Gerontol. A Biol. Sci. Med. Sci. 2014, 69, 1375–1388. [Google Scholar] [CrossRef] [PubMed]
- Belghali, M.; Chastan, N.; Cignetti, F.; Davenne, D.; Decker, L.M. Loss of gait control assessed by cognitive-motor dual-tasks: Pros and cons in detecting people at risk of developing Alzheimer’s and Parkinson’s diseases. Geroscience 2017, 39, 305–329. [Google Scholar] [CrossRef] [PubMed]
- Buracchio, T.; Dodge, H.H.; Howieson, D.; Wasserman, D.; Kaye, J. The trajectory of gait speed preceding mild cognitive impairment. Arch. Neurol. 2010, 67, 980–986. [Google Scholar] [CrossRef] [PubMed]
- Lekamwasam, R.; Lekamwasam, S. Effects of COVID-19 Pandemic on Health and Wellbeing of Older People: A Comprehensive Review. Ann. Geriatr. Med. Res. 2020, 24, 166–172. [Google Scholar] [CrossRef]
- Lebrasseur, A.; Fortin-Bédard, N.; Lettre, J.; Raymond, E.; Bussières, E.L.; Lapierre, N.; Faieta, J.; Vincent, C.; Duchesne, L.; Ouellet, M.C.; et al. Impact of the COVID-19 Pandemic on Older Adults: Rapid Review. JMIR Aging 2021, 4, e26474. [Google Scholar] [CrossRef]
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).