Telemedicine Management: Approaches and Perspectives—A Review of the Scientific Literature of the Last 10 Years



Abstract
1. Introduction
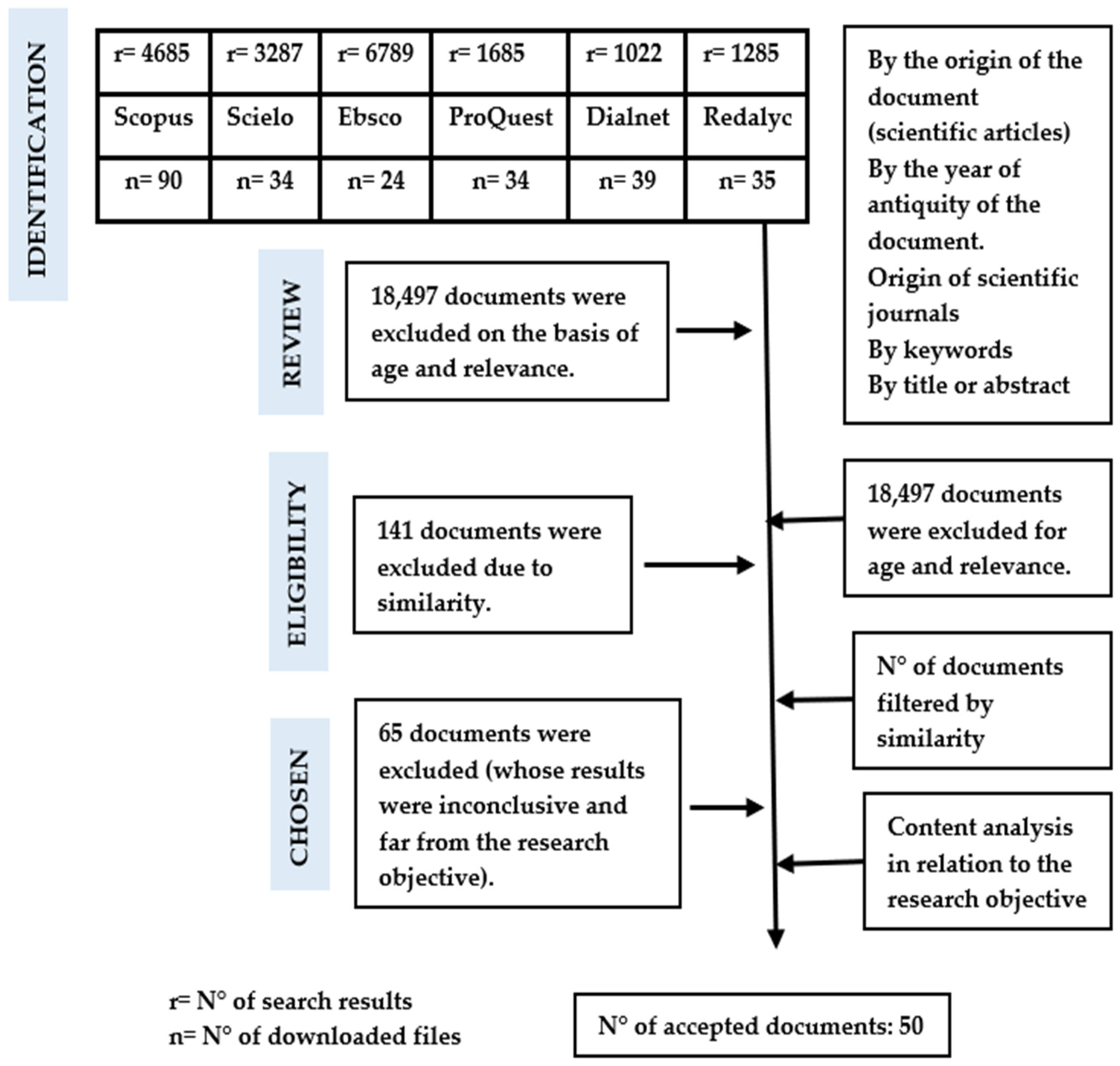
2. Materials and Methods
3. Results
3.1. Approaches
3.1.1. Ethical Approach
3.1.2. Humanistic Approach
3.1.3. Contingency Approach
3.1.4. Socioeconomic Approach
3.1.5. Medical Approach: Experiences of Interventions around the World
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Quispe-Juli, C.U. Ethical Considerations for the Practice of Telemedicine in Peru: Challenges in the Times of COVID-19. Rev. Cuba. Inf. Cienc. Salud (ACIMED) 2021, 32, 1–22. [Google Scholar]
- García Saiso, S.; Marti, M.C.; Malek Pascha, V.; Pacheco, A.; Luna, D.; Plazzotta, F.; Nelson, J.; Tejerina, L.; Bagolle, A.; Savignano, M.C.; et al. Barreras y facilitadores a la implementación de la telemedicina en las Américas. Rev. Panam. Salud Publica Pan Am. J. Public Health 2021, 45, 131. [Google Scholar] [CrossRef] [PubMed]
- Daragó, L.; Jung, Z.; Ispán, F.; Bendes, R.; Dinya, E. Beneficios y desventajas de la telemedicina. Orv. Hetil. 2013, 154, 1167–1171. [Google Scholar] [CrossRef]
- Hillán García, L.; Setién Dodero, F.; Del Real Colomo, A. El Sistema de Telemedicina Militar en España: Una aproximación histórica. Sanid. Mil. 2014, 70, 121–131. [Google Scholar] [CrossRef]
- Narvaja, R. Historia de la Telemedicina. Rev. Asoc. Iberoam. Telesalud Telemed. 2021, 8, 7–11. [Google Scholar]
- Parrasi Castaño, Y.C.; Celis Carvajal, L.J.; García, B.; Rengifo, P.S. Estado actual de la telemedicina: Una revisión de literatura. Ingeniare 2016, 20, 105–120. [Google Scholar] [CrossRef]
- Chá Ghiglia, M.M. Telemedicina: Su rol en las organizaciones de salud. Rev. Méd. Urug. 2020, 36, 185–203. [Google Scholar]
- Begoña, M.; Muñoz, M.; Cuellar, J.; Domancic, S.; Villanueva, J. Revisiones Sistemáticas: Definición y nociones básicas. Rev. Clín. Periodoncia Implantol. Rehabil. Oral 2018, 11, 184–186. [Google Scholar] [CrossRef]
- Torres-Fonseca, A.; López-Hernández, D. Criterios para publicar artículos de revisión sistemática. Rev. Espec. Méd.-Quir. 2014, 19, 393–399. [Google Scholar]
- Page, M.J.; McKenzie, J.E.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Akl, E.A.; Brennan, S.E.; et al. The PRISMA 2020 statement: An updated guideline for reporting systematic reviews. Rev. Esp. Cardiol. 2021, 74, 790–799. [Google Scholar] [CrossRef]
- Mair, F.S.; May, C.; O’Donnell, C.; Finch, T.; Sullivan, F.; Murray, E. Factors that promote or inhibit the implementation of e-health systems: An explanatory systematic review. Bull. World Health Organ. 2012, 90, 357–364. [Google Scholar] [CrossRef] [PubMed]
- Roig, F.; Saigi, F. Barreras para la Normalización de la Telemedicina en un Sistema de Salud Basado en la Concertación de Servicios. Gac. Sanit. 2012, 25, 397–402. [Google Scholar] [CrossRef]
- Prados Castillejo, J.A. Telemedicina, una herramienta también para el médico de familia. Aten. Prim. 2012, 45, 129–132. [Google Scholar] [CrossRef] [PubMed]
- García, L.F. Cooperación para la innovación europea en el envejecimiento activo y saludable: De la política a la acción. Gac. Sanit. 2013, 27, 459–462. [Google Scholar] [CrossRef]
- Yance, L.; Núñez, V.; Barros, D.; Peña, C.J. Seguimiento de pacientes en estado postoperatorio de cirugías ambulatorias a través de la Web Salud Uninorte. Rev. Salud Uninorte 2013, 29, 384–393. [Google Scholar]
- Poropatich, R.; Lai, E.; McVeigh, F.; Bashshur, R. El Programa de Telemedicina y Salud Móvil del Ejército de EE. UU.: Marcando la Diferencia en el País y en el Extranjero. Telemed. E-Salud 2019, 19, 380–386. [Google Scholar] [CrossRef]
- Orzuza, G.B. Información en el Primer Nivel de Atención. Vis. Futuro 2013, 17, 95–113. [Google Scholar]
- Abo-Zahhad, M.; Ahmed, S.M.; Elnahas, O. A wireless emergency telemedicine system for patients monitoring and diagnosis. Int. J. Telemed. Appl. 2014, 2014, 380787. [Google Scholar] [CrossRef]
- Mira-Solves, J.; Orozco-Beltrán, D.; Sánchez-Molla, M.; García, J.S. Evaluación de la satisfacción de los pacientes crónicos con los dispositivos de telemedicina y con el resultado de la atención recibida. Programa ValCrònic. Aten. Prim. 2014, 46, 16–23. [Google Scholar] [CrossRef]
- Garvi Soler, P.; Villanueva Rodríguez, C.; Andrés Martínez, E. Puesta en marcha de una consulta por correo electrónico, para dar soluciones y no para crear problemas. Pediatr. Aten. Prim. 2014, 16, 311–316. [Google Scholar] [CrossRef]
- Cortés-Ramírez, J.M.; Montoya-Rodarte, J.M.; Argüelles Robles, E.; Salazar-de Santiago, A. Telemedicina: Opinión de dos generaciones. Med. Interna Mex. 2014, 30, 191–194. [Google Scholar]
- Díez, C.; María, J. Humanismo, salud y tecnologías de acercamiento. Index Enferm. 2014, 23, 197–199. [Google Scholar] [CrossRef]
- Gozzer Infante, E. Una visión panorámica de las experiencias de telesalud en Perú. Rev. Perú Med. Exp. Salud Publica 2015, 32, 385–390. [Google Scholar] [CrossRef]
- Brown Cooper, S. Opinion Leaders’ Perspective of the Benefits and Barriers in Telemedicine: A Grounded Theory Study of Telehealth in the Midwest. Quarterly Review of Distance. Education 2015, 16, 25–53. [Google Scholar]
- Pérez-Manchón, D. Telemedicina, una Red Social Médica de Ayuda Humanitaria entre España y Camerún. Gac. Sanit. 2015, 29, 59–61. [Google Scholar] [CrossRef] [PubMed]
- Jiménez Barbosa, W.G.; Acuña Gómez, J.S. Avances en telesalud y telemedicina: Estrategia para acercar los servicios de salud a los usuarios. Acta Odontol. Colomb. 2015, 5, 1. [Google Scholar]
- Islam, S.S.M.; Tabassum, R. Implementation of information and communication technologies for health in Bangladesh. Bull. World Health Organ. 2015, 93, 806–809. [Google Scholar] [CrossRef]
- Luna Gómez, I.F.; Torres Silva, E.A.; Tamayo Correa, C.; Vélez Zuluaga, S.; Ramírez Morales, M.M.; González Serna, C.; Durango Araque, L.V.; Smith, J.; Flórez-Arango, J.F. Uso de las tecnologías de información y comunicación para el cuidado del binomio materno-fetal: Revisión de tema. Med. UPB 2015, 34, 138–147. [Google Scholar] [CrossRef]
- Maldonado, J.M.; Marques, A.B.; Cruz, A. Telemedicine: Challenges to dissemination in Brazil. Cad. Saúde Pública 2016, 32, e00155615. [Google Scholar] [CrossRef]
- Catalán, M.D.J.; López, V.A. La Telesalud y la sociedad actual: Retos y oportunidades. Rev. Esp. Comun. Salud 2016, 7, 336–345. [Google Scholar]
- Rodrigues Martinez Basile, F.; Cezar Amate, F.; Ramirez López, L.J. Desarrollo colaborativo en Telemedicina y Telesalud para la Educación, la atención y la investigación: Estudio de caso Lab.Sh-Brasil—Tigum-Colombia. Acad. Virtualidad 2016, 9, 123–141. [Google Scholar] [CrossRef]
- Ramírez, J.A. Telemedicina y telesalud en falla cardiaca. ¿Es una alternativa? Rev. Colomb. Cardiol. 2016, 23, 59–61. [Google Scholar]
- Narváez, F.; Marín-Castrillón, D.M.; Cuenca, M.; Latta, M. Desarrollo e implementación de tecnologías para telerehabilitación física en América Latina: Una revisión sistemática de literatura, programas y proyectos. TecnoLógicas 2016, 20, 155–176. [Google Scholar] [CrossRef]
- Correa-Díaz, A.M. Avances y barreras de la telemedicina en Colombia. Rev. Fac. Derecho Cienc. Políticas 2017, 47, 361–382. [Google Scholar] [CrossRef]
- McSwain, S.D.; Bernard, J.; Burke, B.L., Jr.; Cole, S.L.; Dharmar, M.; Hall-Barrow, J.; Herendeen, N.; Herendeen, P.; Krupinski, E.A.; Martin, A.; et al. American Telemedicine Association operating procedures for pediatric telehealth. Telemed. E-Health 2017, 23, 699–706. [Google Scholar] [CrossRef] [PubMed]
- Saraiva, A.; Branco Sousa, M.C.; Nunes, J. El Perfil Ideal del Usuario de Telemedicina—Experiencia de Portugal. Rev. Soc. Int. Telemed. EHealth 2017, 5, 1–5. [Google Scholar]
- Caffery Liam, J.; Bradford Natalie, K.; Smith Anthony, C.; Danette, L. How telehealth facilitates the provision of culturally appropriate healthcare for Indigenous Australians. Rev. Telemed Teleasist. 2021, 24, 676–682. [Google Scholar] [CrossRef]
- Rollin, A.; Ridout, B.; Campbell, A. Digital Health in Melanoma Posttreatment Care in Rural and Remote Australia: Systematic Review. J. Med. Internet Res. 2018, 20, e11547. [Google Scholar] [CrossRef]
- Palop Asunción, J.G.; Hernández Abadía de Bárbara, A.; Vázquez Prat, Á.; Nevado del Mazo, L. Aplicaciones de la telemedicina en montaña y entornos hostiles. Sanid. Mil. 2018, 74, 175–178. [Google Scholar]
- Linares, C.L.P.; Linares, C.L.B.; Herrera, F.A. Telemedicina, impacto y perspectivas para la sociedad actual. Univ. Méd. Pinareña 2018, 14, 289–303. [Google Scholar]
- Breskvar, M.; Vavpotič, T.V. Teletransfuzija—Uspešna telemedicina v sloveniji. Inform. Med. Slov. 2021, 1, 24–29. [Google Scholar]
- Fernández, M.J.; García-Cenador, M.B.; López-Valverde, N.; Muriel, C.; Sánchez-Ledesma, M.J. Las tecnologías de la información y la comunicación aplicadas entre los profesionales de la medicina que realizan tratamiento del dolor. Rev. Soc. Esp. Dolor 2019, 26, 175–183. [Google Scholar] [CrossRef] [PubMed]
- Da Luz, P.L. Telemedicine and the Doctor/Patient Relationship. Arq. Bras. Cardiol. 2019, 113, 100–102. [Google Scholar]
- Villalobos, J. Telemedicina y Diabetes. Rev. Venez. Endocrinol. Metab. 2020, 18, 91–93. [Google Scholar]
- Padilla, K.M.; Ramos, R.R.; Reyes, R.A.; Rodas, G.H. A.; Rodas, G.H. La gestión del cambio en la atención médica tradicional: La telemedicina como nuevo enfoque de la atención médica al paciente en honduras. REV. Epistémica 2020, 4, 1344–1347. [Google Scholar]
- Hyder, M.A.; Razzak, J. Telemedicina en los Estados Unidos: Una introducción para estudiantes y residentes. Rev. Investig. Méd. Internet 2020, 22, e20839. [Google Scholar] [CrossRef]
- Rodríguez Feijóo, A.B.; Salgado Cotilla, B.; Rivera Rios, C.; Quintana Jambrina, M.I.; Civeira Pérez, V.; Rodríguez Araujo, J.; Cabanelas González, B. Implantación y gestión de la plataforma “TELEA” en el seguimiento de pacientes Covid-19 positivos. Index Enferm. 2020, 29, 244–248. [Google Scholar]
- Álvarez, D.J.A. Aspectos éticos de la telemedicina ante la pandemia de COVID-19. Med. Ética 2021, 32, 249–270. [Google Scholar] [CrossRef]
- Mendoza-Alonzo, P.; Mendoza-Alonzo, J. Telemedicina: Desafíos para Chile a la luz de la experiencia de Estados Unidos durante la pandemia. Rev. Méd. Chile 2021, 149, 1198–1204. [Google Scholar] [CrossRef]
- Silva de la Torre, T. La imperiosa necesidad de telemedicina en la atención de diabetes durante la pandemia de COVID-19. Un estudio de abordaje integral. Gac. Méd. Méx. 2021, 157, 3. [Google Scholar]
- Gil Membrado, C.; Barrios, V.; Cosín-Sales, J.; Gámez, J.M. Telemedicina, ética y derecho en tiempos de COVID-19. Una mirada hacia el futuro. Rev. Clín. Esp. 2021, 221, 408–410. [Google Scholar] [CrossRef] [PubMed]
- Villanova, T.M.P.; Mateu, H.C. Cruzando el puente tecnológico de la telemedicina. Aten. Prim. Práct. 2021, 3, 100–117. [Google Scholar] [CrossRef]
- Salinas, R.R.; Taboada, R.P.; Quintana, V.C.; Vacarezza, Y.R.; Rodríguez, S.M.A.; Borja, R.H. Una reflexión sobre las implicaciones éticas de la telemedicina. Rev. Méd. Chile 2021, 149, 928–933. [Google Scholar] [CrossRef]
- Ah, Y.K.; Woo, S.C. Considerations on the Implementation of the Telemedicine System Encountered with Stakeholders’ Resistance in COVID-19 Pandemic. Telemed. E-Salud 2021, 27, 475–480. [Google Scholar]
- Takahashi, M.; Koike, R.; Nagasawa, K.; Manabe, Y.; Hirana, H.; Takamura, M.; Hongawa, T.; Kimoto, I.; Ogawa-Ochi, K. Desarrollo de herramientas de telemedicina con énfasis en la observación visual. Artif. Life Robot. 2022, 27, 38–47. [Google Scholar] [CrossRef] [PubMed]
- Cervantes, L.M.J.; Llanes, C.A.; Sánchez, M.W.; Olvera, M.V. Telemedicina como estrategia innovadora en las instituciones de salud. Rev. Iber. Sist. Tecnol. Inf. 2021, 44, 330–338. [Google Scholar]
- Vidal-Alaball, J.; Descals Singla, E. Abordaje de la telemedicina entre proveedores: Ejemplos de uso. Aten. Prim. Práct. 2021, 3, 100–112. [Google Scholar] [CrossRef]
- Rodríguez, E.; García Lumbreras, S.; Buscemi, V.; Cortí Barberá, V. Experiencia del paciente oncológico durante la pandemia por el COVID-19 y su opinión sobre la telemedicina. Psicooncología 2022, 19, 27–43. [Google Scholar] [CrossRef]
- Bashshur, R.; Doarn, C.R.; Frenk, J.M.; Kvedar, J.C.; Woolliscroft, J.O. Telemedicine and the COVID-19 pandemic, lessons for the future. Telemed. E-Health 2020, 26, 571–573. [Google Scholar] [CrossRef]
- Temiz, S.A.; Dursun, R.; Daye, M.; Ataseven, A. Evaluation of dermatology consultations in the era of COVID-19. Dermatol. Ther. 2020, 33, e13642. [Google Scholar] [CrossRef]
- Albornoz-Chauca, M.; Gamboa-Cruzado, J.; Montero, J.N.; Pérez-Salcedo, R.; Plata CG, R.; Yauris-Silvera, C.; Atauje-Pariona, M.; Elias-Silupu, J. Telemedicine and its impact on rural health care in times of COVID-19: A systematic review. Bol. Malariol. Salud Ambient. 2022, 62, 171–182. [Google Scholar] [CrossRef]
- Mohammadi, R.; Tabanejad, Z.; Abhari, S.; Honarvar, B.; Lazem, M.; Maleki, M.; Garavand, A. A systematic review of the use of telemedicine in the military forces worldwide. Shiraz E-Med. J. 2020, 21, 1–8. [Google Scholar] [CrossRef]
- Nieblas, B.; Okoye, K.; Carrión, B.; Mehta, N.; Mehta, S. Impact and future of telemedicine amidst the COVID-19 pandemic: A systematic review of the state-of-the-art in Latin America. Ciênc. Saúde Colet. 2022, 27, 3013–3030. [Google Scholar] [CrossRef] [PubMed]
- Correia, J.C.; Meraj, H.; Teoh, S.H.; Waqas, A.; Ahmad, M.; Lapão, L.V.; Pataky, Z.; Golay, A. Telemedicine to deliver diabetes care in low-and middle-income countries: A systematic review and meta-analysis. Bull. World Health Organ. 2021, 99, 209B–219B. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Authors | Year | Country | Database |
|---|---|---|---|
| [11] | 2012 | France | Scielo |
| [12] | 20212 | Spain | Scielo |
| [13] | 2012 | Spain | Scopus |
| [14] | 2013 | Belgium | Scopus |
| [15] | 2013 | Colombia | ProQuest |
| [16] | 2013 | USA | Scopus |
| [3] | 2013 | Hungary | Scopus |
| [17] | 2013 | Argentina | Scielo |
| [18] | 2014 | Egypt | Scopus |
| [19] | 2014 | Spain | Scopus |
| [20] | 2014 | Spain | Scielo |
| [21] | 2014 | Mexico | Ebsco |
| [22] | 2014 | Spain | Scopus |
| [23] | 2015 | Peru | Ebsco |
| [24] | 2015 | USA | Ebsco |
| [25] | 2015 | Spain | Scopus |
| [26] | 2015 | Colombia | ProQuest |
| [27] | 2015 | Bangladesh | Scielo |
| [28] | 2015 | Colombia | Scopus |
| [29] | 2016 | Brazil | Scielo |
| [30] | 2016 | Spain | Dialnet |
| [31] | 2016 | Brazil | Dialnet |
| [32] | 2016 | Colombia | ProQuest |
| [33] | 2017 | Colombia | ProQuest |
| [34] | 2017 | Colombia | ProQuest |
| [35] | 2017 | USA | Ebsco |
| [36] | 2017 | Portugal | Scopus |
| [37] | 2018 | Australia | Scopus |
| [38] | 2018 | Australia | ProQuest |
| [39] | 2018 | Spain | Scielo |
| [40] | 2018 | Cuba | Redalyc |
| [41] | 2019 | Slovenia | Scielo |
| [42] | 2019 | Spain | Scielo |
| [43] | 2019 | Brazil | Scielo |
| [44] | 2020 | Venezuela | Redalyc |
| [45] | 2020 | Honduras | Redalyc |
| [46] | 2020 | USA | Scopus |
| [47] | 2020 | Spain | Scielo |
| [48] | 2021 | Mexico | Scielo |
| [49] | 2021 | Chile | Scopus |
| [50] | 2021 | Mexico | Scopus |
| [51] | 2021 | Spain | Scopus |
| [52] | 2021 | Spain | Scopus |
| [53] | 2021 | Chile | Scopus |
| [54] | 2021 | Korea | Redalyc |
| [2] | 2021 | Argentina | Ebsco |
| [55] | 2021 | Japan | Scopus |
| [56] | 2021 | Mexico | ProQuest |
| [57] | 2021 | Spain | ProQuest |
| [58] | 2022 | Spain | Scopus |
| Author (s) | Origin and Year | Contributions |
|---|---|---|
| [16] | U.S.A 2013 | The U.S. Army Medical Department’s telemedicine network spans 50 countries and territories, from American Samoa to Afghanistan, in 19 time zones. In total, 22 service lines are available, of which behavioral health makes up 55% of all telemedicine services. |
| [39] | Spain 2018 | The experimentation of teleconsultation from the base camp of Gasherbrum II (Pakistani Himalayas) to the Military Hospital “Gomez Ulla” allowed the development of a telemedicine kit that will simplify the inconveniences for interventions in hostile camps. |
| [43] | Spain 2019 | Studies of international missions in which the Spanish Armed Forces and their allies have implemented a facility with Role 1 health capabilities to evaluate telemedicine as a key tool to support doctors deployed in missions. |
| [46] | U.S.A 2020 | In the United States, one of the first uses of telemedicine was established by the National Aeronautics and Space Administration (NASA) in 1960 to monitor astronauts in flight by physicians and medical teams during their Project Mercury mission. |
| Author (s) | Origin and Year | Contributions |
|---|---|---|
| [19] | Spain 2014 | In a telemedicine program, 410 patients were intervened by telephone. It was reported that for 288 patients (89.4%), the devices were easy to operate at home by themselves. Only in 12 cases (3.7%) did the patient consider the telemedicine device to be a difficult workload to integrate into their daily life. |
| [18] | Egypt 2014 | This work proposes the design and implementation of a wireless telemedicine system in which all physiological vital signs are transmitted to a remote medical server via mobile networks, in case of emergency, and the Internet, in the case of long-term monitoring. |
| [15] | Colombia 2013 | Positive perception by the medical team regarding the visual environment of the system, its functionality, and relevance for post-operative care in ambulatory surgery patients. |
| [20] | Spain 2014 | Parents or legal guardians in pediatrics use new technologies and find it convenient to be able to ask about health issues that do not require a face-to-face assessment with the professionals who regularly attend to their child without having to make an appointment and travel to the health center. |
| [28] | Colombia 2015 | Importance of evaluating the different models of telemedicine assistance for the maternal–fetal pairing to identify the lessons learned and the success factors necessary to implement new models. |
| [31] | Colombia 2016 | Through scientific and technological cooperation between Brazil and Colombia for practicing telemedicine. Currently, undergraduate and graduate students and professionals in the health field are integrated for developing models, strategies, and mechanisms to transmit information that takes into account distance and digital safety. |
| [32] | Colombia 2016 | Telemedicine and telehealth are not only an alternative for dealing with complex chronic pathologies such as heart failure; they have become a necessity in our environment. |
| [38] | Australia 2018 | Digital interventions can be used by clinicians as an adjunct service during post-treatment care for melanoma, especially in regions with fewer resources of healthcare professionals and infrastructure, such as rural and remote Australia. |
| [41] | Slovenia 2019 | A case of good practice that demonstrates that in Slovenia, as elsewhere, the combination of appropriate technology, qualified staff, good management, and sufficient funding can result in telemedicine delivering healthcare services more optimally than the traditional way. |
| [44] | Venezuela 2020 | Psychosocial and behavioral improvements in self-management efficacy have been demonstrated in young patients with type 1 diabetes who participate in telemedicine compared to those who attend face-to-face visits. |
| [42] | Spain 2019 | The use of clinical pain protocols in clinical practice is a good example of information processing in the healthcare field by applying the benefits of telemedicine. |
| [47] | Spain 2020 | TELEA appears to be a good tool for monitoring patients with COVID-19 in home confinement. Nursing care is essential to the success of telecare with TELEA. |
| [55] | Japan 2022 | The design and implementation of a wireless telemedicine system are proposed in Japan for remote monitoring. |
| [50] | Mexico 2021 | A redesign of the care model with the incorporation of technologies and telemedicine should be considered to mitigate chronic disease morbidity and mortality during the COVID-19 pandemic and in the post-COVID-19 era. |
| [58] | Spain 2022 | Most patients express a high degree of satisfaction with the health care received and with the possibilities of contact and accompaniment, emphasizing the effort made by health care providers to continue monitoring oncology patients. |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Aguirre-Sosa, J.; Vargas-Merino, J.A. Telemedicine Management: Approaches and Perspectives—A Review of the Scientific Literature of the Last 10 Years. Behav. Sci. 2023, 13, 255. https://doi.org/10.3390/bs13030255
Aguirre-Sosa J, Vargas-Merino JA. Telemedicine Management: Approaches and Perspectives—A Review of the Scientific Literature of the Last 10 Years. Behavioral Sciences. 2023; 13(3):255. https://doi.org/10.3390/bs13030255
Chicago/Turabian StyleAguirre-Sosa, Joaquín, and Jorge Alberto Vargas-Merino. 2023. "Telemedicine Management: Approaches and Perspectives—A Review of the Scientific Literature of the Last 10 Years" Behavioral Sciences 13, no. 3: 255. https://doi.org/10.3390/bs13030255
APA StyleAguirre-Sosa, J., & Vargas-Merino, J. A. (2023). Telemedicine Management: Approaches and Perspectives—A Review of the Scientific Literature of the Last 10 Years. Behavioral Sciences, 13(3), 255. https://doi.org/10.3390/bs13030255