Abstract
The presence of less healthy lifestyle habits among individuals diagnosed with schizophrenia which can contribute to the escalation of physical disorders and exacerbation of psychological symptoms is well documented. The present scoping review aims to synthesize and evaluate the available evidence regarding the impact of regular physical exercise on psychopathology, cognition, and quality of life (QoL) in patients diagnosed with schizophrenia. A literature search was performed across Web of Science, SCOPUS, PubMed, and SPORTDiscus for randomized control trials published up to April 2022. Two independent reviewers applied the selection criteria and a third reviewer resolved discrepancies. A total of twelve studies were included, of which nine used endurance training and three used concurrent training (one of these additionally used resistance training). The results reveal benefits of various modalities of supervised regular exercise in the psychopathology of schizophrenia. Furthermore, regular endurance training seems to improve cognitive function in patients with schizophrenia and promote their QoL; however, results are inconclusive with respect to this last variable. The assessment of methodological quality in the reviewed articles indicates a high overall risk of bias, particularly in relation to deviations from intended interventions and the selection of reported results. Furthermore, an assessment of exercise reporting revealed that only 5 out of 19 items were fulfilled in more than 50% of the articles. Future research is needed to evaluate the effects of different training modalities and the optimal dose–response relationship in patients diagnosed with schizophrenia.
1. Introduction
According to the International Classification of Diseases (ICD-11), schizophrenia is a mental disease that produces alterations in different brain areas affecting mental health, including thinking, self-experience, perception, volition, and occasionally perturbing behavior [1]. In addition, these alterations commonly concur with associated symptoms such as delusions, hallucinations, disorganized speech or behavior, and decreased emotional expression [2]. Updated prevalence data show that schizophrenia affected 23.59 million people (0.32%) worldwide in 2019, while in Europe this prevalence rises to 2.8 million people (0.35%) [3]. Further, this mental illness is associated with a high economic burden regarding public health [4,5]. For instance, the economic burden of schizophrenia in the United States is estimated to be nearly USD 150 billion [5,6] entailing more than USD 12,000 per patient when hospitalization is required [7]. In England, that annual cost in 2012 was approximately GBP 11.8 billion, equivalent to around USD 15.8 billion [8].
One of the crucial factors that affect health-related domains other than the mental health (i.e., physical fitness or social behaviors) of individuals diagnosed with schizophrenia is their lifestyle patterns. Compared to the general population, people with schizophrenia tend to have less healthy habits. Specifically, they engage in less physical exercise, have a smoking prevalence that is about 50% higher, and follow a less healthy diet characterized by increased fat intake and decreased consumption of fruits and vegetables [9,10,11]. Scientific evidence has widely demonstrated predominantly sedentary behavior in the daily routine of individuals diagnosed with schizophrenia [12,13,14,15,16]. Specifically, between 50 and 70% of patients fail to meet the physical activity recommendations of at least 150 min of moderate intensity exercise per week, which classifies them as physically inactive [12,16]. This context, along with disease-specific circumstances such as the lack of motivation, cognitive and psychopathological symptoms, and medication side effects, make it difficult to reach an optimal level of physical activity [10,12,14,16]. Even though lower levels of physical activity (i.e., ≥90 min per week) may produce positive effects on overall cognition [17], it has been consistently demonstrated that physical inactivity and sedentary behavior lead to an increased risk of developing cardiovascular diseases and metabolic disorders in these patients [10,14,15,16], and can even aggravate some psychological symptoms.
In this sense, antipsychotics can aggravate this situation by causing weight gain [11,18]. This increase in body weight creates a detrimental cycle of effects, perpetuating the negative health outcomes [11,18] associated with antipsychotic use. This context leads to a reduction in life expectancy by approximately 10–20 years [11,16,19,20], as well as a two- to threefold rise in mortality prevalence compared to the general population [9,19,21]. The aforementioned situation underscores the need to contemplate the effect of this specific pathology on patients’ quality of life (QoL). The World Health Organization (WHO) defines QoL as an individual’s perception or their position in life in the context of the culture and value systems in which they live and concerning their goals, expectations, standards, and concerns [22]. Therefore, it is imperative to analyze how this pathology influences various aspects of an individual’s QoL in order to improve overall patient care and well-being. Previous studies have demonstrated that the deterioration of different health areas experienced by patients with schizophrenia can lead to a decrease in their QoL [23,24]. This situation can be aggravated with age, as the prevalence of chronic physical diseases such as hypertension or diabetes increases [23].
Considering the impact of schizophrenia on public health and individuals’ health and QoL, the treatment of this pathology is of particular interest. The commonly used pharmacological treatment of schizophrenia can be categorized into first-generation antipsychotics (e.g., haloperidol, levomepromazine, or chlorpromazine) and second-generation antipsychotics (e.g., clozapine, olanzapine, or risperidone) [25,26,27]. The objective of these drugs is to reduce symptoms and improve patients functioning. However, such treatments can cause various side effects, including extrapyramidal effects (i.e., dyskinesia, dystonia, akathisia, tremor, or rigidity), cardiovascular effects (i.e., tachycardia, palpitations or arrhythmias), and severe adverse effects that affect metabolism (i.e., obesity and diabetes) [25,26,27], as well as sexual dysfunction that can reduce patients’ QoL and satisfaction [27].
In light of these challenges, physical activity and regular exercise have emerged as a promising and effective alternative for mitigating collateral effects and improving psychopathological and cognitive symptoms, thereby promoting societal functioning and QoL [16,18]. As with pharmacological treatment, exercise should be carefully prescribed for its clinical application as well as to ensure its replicability, allowing researchers to better assess and compare the results and conclusions derived from scientific evidence [28]. In accordance with this, the American College of Sports Medicine (ACSM), in its 10th edition of Guidelines for Exercise Testing and Prescription (GETP10), described the six components that should be detailed and reported in the prescription of physical exercise: Frequency, Intensity, Time, Type, Volume of exercise and Progression component (FITT−VP) [29].
In recent years, a growing body of scientific research has focused on investigating the effects of physical exercise among people with schizophrenia. One recent study concluded that endurance exercise produces important health benefits with minimal negative effects [30]. Similarly, a review of combined endurance and resistance exercise interventions (i.e., concurrent training) for individuals with schizophrenia found that they promoted mental and physical health [31]. In another systematic review, the authors reported that regular exercise enhances physical fitness and lowers cardiometabolic risk factors [32]. Along the same lines, Bredin and colleagues [33] demonstrated the benefits of exercise training on psychiatric symptoms and health-related physical measures in an interesting meta-analysis. However, there is controversy about which exercise modalities have positive effects on QoL, cognition, and psychopathological symptoms [34,35].
While the scientific evidence suggests a favorable impact of exercise on health-related parameters in individuals diagnosed with schizophrenia, serious concerns arise regarding the comprehensive understanding of the most influential factors and the methods employed to ensure reproducibility. This is especially relevant when contemplating the description of the independent variable, that is, physical exercise. The reviewed literature lacks both clear inclusion criteria and adequate information pertaining to adherence to the FITT-VP parameters, which are essential for the purposes of prescribing exercise and facilitating the replicability of research findings [28,29]. These deficiencies persist in recent reviews published within the last year [36,37,38,39,40]. Thus, for this new review it is imperative to incorporate elements addressing these issues into the selection criteria.
On the other hand, certain reviews [31,32,33] have failed to differentiate between distinct pathologies, encompassing patients with an initial episode of psychosis. This lack of differentiation may introduce confounding factors when analyzing outcomes, especially considering that schizophrenia embodies a more intricate diagnostic construct characterized by severe deterioration and enduring symptoms [1]. Furthermore, it is essential to consider the severity of symptoms and the treatment settings, as emphasized by Cella et al. [36]. In fact, one of the reviews published in 2023 [37] concluded that the positive effects were more pronounced among outpatients. Taking these factors into consideration along with the observation that recent reviews in this area have failed to address this differentiation [36,37,38,39], it becomes imperative to direct our focus exclusively toward outpatients. Such an approach holds the potential to generate a more consistent study cohort, thereby enhancing the applicability of our findings to clinical practice. Therefore, this scoping review aims to synthesize and assess the available evidence regarding the effects of regular physical exercise on psychopathology, cognition, and QoL in outpatients diagnosed with schizophrenia.
2. Methods
2.1. Literature Search
The present scoping review protocol was registered on the Open-Source Framework (OSF) on 8 February 2023 (https://osf.io/tvbr6/ (accessed on 8 February 2023)) and followed the recommendations proposed by Tricco and colleagues using the Preferred Items for Systematic Reviews and Meta-Analyses extension for Scoping Reviews (PRISMA-ScR) [41].
The literature search was performed independently by three blinded investigators on 5 April 2022 across four electronic databases (Web of Science, SCOPUS, PubMed, and SPORTDiscus). The search strategy (Supplementary Materials File S1) used was a combination of keywords and Boolean operators, resulting in the following search equation: (“power exercise*” OR “strength exercise*” OR “resistance train*” OR “strength train*” OR “power train*” OR “resistance exercise*” OR “regular exercise” OR “exercise program” OR “physical activity” OR “endurance” OR “human walking” OR “physical exercise*” OR “fitness train*” OR “plyometric*” OR “aerobic exercise*” OR “aerobic train*” OR “muscle stretching” OR “tai chi*” OR “yoga” OR “physical condition*”) AND (“schizo*”).
2.2. Eligibility Criteria
We followed a PICOS approach to select studies eligible for inclusion (Table 1). Studies in a language other than Spanish, English, or Portuguese were excluded.

Table 1.
Inclusion and exclusion criteria according to PICOS.
2.3. Study Selection and Data Extraction
Two researchers (L.V.B and A.V.-S.) independently and blindly screened records obtained from the electronic databases for data inclusion and identified and removed duplicated studies using Zotero [42]. Subsequently, an exhaustive manual review of the remainder articles was performed to avoid potential errors. After that, the same reviewers screened the articles with the help of Rayyan [43] by analyzing the title and abstract, identifying those that met the inclusion criteria, and removing those with characteristics described in the exclusion criteria. In the final stage, the same researchers independently conducted a comprehensive examination of the full text to determine the final eligibility of the studies. These latter two phases were overseen by a third reviewer (X.D.-C.), who resolved discrepancies that arose from disagreements due to the individual decisions made by the researchers.
The following data were extracted from the included full-text publications (Table 2): (1) author and year of publication; (2) participants’ characteristics (sex, body mass index, race/ethnicity, pharmacological treatment, previous physical exercise experience); (3) design of the study, sample size, and intervention period; (4) exercise protocol, supervision, and training familiarization; and (5) outcomes of interest.
2.4. Critical Appraisal
To critically assess the studies included in the present review, we individually evaluated the methodological quality and quality of reporting of training protocols for each intervention.
2.4.1. Risk of Bias
The risk of bias in the included studies was assessed according to the Revised Cochrane risk-of-bias tool for randomized trials (RoB 2) [44]. The following domains were scored for each included study: (1) bias arising from the randomization process; (2) bias due to deviations from intended interventions; (3) bias due to missing outcome data; (4) bias in the measurement of the outcome; and (5) bias in the selection of the reported results. Each of these domains was judged as having a low risk of bias, some concerns, and a high risk of bias, respectively [44].
2.4.2. Quality Reporting of Exercise Intervention in the Training Programs
To assess the quality of the independent variable of the eligible studies, i.e., exercise intervention, we used the Consensus on Exercise Reporting Template (CERT) tool [28].
Table 2.
Characteristics of the included studies.
Table 2.
Characteristics of the included studies.
| Study | Participants Characteristics | Design | Exercise Protocol | Outcomes of Interest |
|---|---|---|---|---|
| Andrade e Silva et al. [45] | Sex: 100% male BMI (kg/m2): 27.98 ± 1.67 (RESEX), 29.42 ± 1.93 (CONCEX), 25.38 ± 1.60 (CTRL), Race/Ethnicity: N/A Other diseases: N/A Pharmacological treatment: Yes, antipsychotics, antidepressants (n = 15), benzodiazepine (n = 6), mood stabilizer (n = 6) and anticholinergic (n = 8) Previous physical exercise experience: No (sedentary lifestyle > 1 year) Males with a DSM-IV diagnosis of schizophrenia, 18–50 years (33.36 ± 7.6 years) with stable doses of medication and clinically stable disease. | Design: RCT RESEX CONCEX CTRL Sample size: (n = 47) RESEX: n = 12/CONCEX: n = 9/CTRL: n = 13 Intervention period: 20 weeks | Supervised: Yes Familiarization: 3 sessions RESEX: F: 2 sessions/week IL: 40% to 85% 1RM Ti: 55 min/session Ty: progressive RT. V: 7 exercises from 2 × 15 reps to 3 × 6–8 reps (r: 1–2 min between sets). From 210 reps at week 1 to 147 reps at week 20 P: 2.5% per week CONCEX: F: 2 sessions/week IL: RT: 40–85% 1RM/ET: 40–75% VO2max Ti: 55 min/session Ty: progressive RT + progressive ET. V: RT: 7 exercises from 1 × 15 reps to 2 × 6–8 reps (r: 1–2 min), 98–105 reps per week/ET: 50 min per week P: RT: +2.5% per week (RT)/ET: +1.75% per week CTRL: F: 2 sessions/week IL: minimum load IE: 7 exercise 2 × 15 reps (r: 1 min between sets) Ti: 55 min/session Ty: RT with minimum load V: 210 reps/week P: N/A Attrition of the study: 27.65% Adherence to the study: >75% | Analysis within group RESEX: ↓ PANSS total score after 10 weeks (p = 0.002) ↓ PANSS total score after 20 weeks (p ≤ 0.001) ↓ positive symptoms (PANSS) after 10 weeks (p = 0.039) ↓ positive symptoms (PANSS) after 20 weeks (p ≤ 0.001) ↓ negative symptoms (PANSS) after 10 weeks (p = 0.001) ↓ negative symptoms (PANSS) after 20 weeks (p = 0.002) ↑ SF- 36 (physical role dimension) after 20 weeks (p = 0.011) CONCEX: ↓ PANSS total score after 10 weeks (p = 0.026) ↓ PANSS total score after 20 weeks (p = 0.003) ↓ positive symptoms (PANSS) after 20 weeks (p = 0.016) = negative symptoms (PANSS) (p not reported) ↑ SF- 36 (physical role dimension) after 20 weeks (p = 0.014) CTRL: = PANSS total score (p not reported) = positive symptoms (PANSS) (p not reported) = negative symptoms (PANSS) (p not reported) Analysis between groups Not reported for these outcomes |
| Lo et al. [46] | Sex: 17.64% male (HIIT)/50% male (ENEX)/50% male (CTRL) BMI (kg/m2): 26.72 ± 5.31 (HIIT)/25.56 ± 4.09 (ENEX)/24.82 ± 2.83 (CTRL) Race/Ethnicity: N/A Other diseases: N/A Pharmacological treatment: 16 were prescribed atypical antipsychotics and 1 typical antipsychotic in HIIT group/13 were prescribed atypical antipsychotics, 2 typical antipsychotics and 1 was not prescribed with any antipsychotic in AE group/16 were prescribed atypical antipsychotics, 1 typical antipsychotic and 1 was not prescribed with any antipsychotic in control group Previous physical exercise experience: N/A Outpatients aged 18–55 years with a diagnosis of schizophrenia spectrum disorder (DSM V). | Design: RCT ENEX (HIIT) ENEX CTRL (Psychoeducation) Sample size: (n = 51) HIIT: n = 17/ENEX: n = 16/CTRL: n = 18 Intervention period: 12 weeks | Supervised: Yes Familiarization: N/A ENEX (HIIT): F: 3 sessions/week IL: number of bouts as long as possible). X > 105% FTP + 1–3 min < 91% FTP Ti: number of bouts up to participants expended 150 kJ Ty: cycling performance V: until reaching 150 kJ (not time, sets or reps reported) P: N/A ENEX: F: 3 sessions/week IL: <91% FTP Ti: X min until reaching 150 kJ Ty: cycling performance V: until reaching 150 kJ (not time, sets or reps reported) P: N/A CTRL (Psychoeducation): F: 3 sessions/week Ti: 15–30 min/session Ty: mental and physical health content was delivered to the participants Attrition of the study: 15.69% (2 drop out the study before participating in the interventions and 6 during the intervention) Adherence of the study: N/A | Analysis within group ENEX (HIIT):↑ procedural memory consolidation (sleep-dependent memory consolidation) (p < 0.001) ↑ logical memory (24 h delayed recall) (p < 0.001) = PANSS total score (p = 0.548) = positive symptoms (PANSS) (p = 0.824) = negative symptoms (PANSS) (p = 0.134) ENEX: ↑ procedural memory consolidation (sleep-dependent memory consolidation) (p < 0.05) = logical memory (24 h delayed recall) (p = 0.077) = PANSS total score (p = 0.460) = positive symptoms (PANSS) (p = 0.594) = negative symptoms (PANSS) (p = 0.700) CTRL: = procedural memory consolidation (sleep-dependent memory consolidation) (p = 0.023) = logical memory (24 h delayed recall) (p = 0.946) = PANSS total score (p = 0.806) = positive symptoms (PANSS) (p = 0.829) = negative symptoms (PANSS) (p = 0.713) Analysis between groups HIIT vs. CTRL HIIT > CTRL at procedural memory consolidation (sleep-dependent memory consolidation) after 12 weeks (p < 0.01) HIIT > CTRL at logical memory (24 h delayed recall) after 12 weeks (p < 0.05) |
| Kern et al. [47] | Sex: 94% male (ENEX)/100% male (CTRL) BMI (kg/m2): Intervention group 30.1/control group 30.0 Race/Ethnicity: Intervention group (66% Black, 11% White, 11% Asian, 11% Hispanic) and control group (67% Black, 17% White, 0% Asian, 11% Hispanic) Other diseases: yes, chronic diseases Pharmacological treatment: Yes, antipsychotics 92% in ENEX and 88% in CTRL. Previous physical exercise experience: No (no participation in an aerobic exercise program in the past 6 months) Veterans aged 40–65 with a psychiatric diagnosis of schizophrenia orschizoaffective disorder (DSM V). | Design: RCT ENEX CTRL Sample size: (n = 53) ENEX: n = 35/CTRL: n = 18 Intervention period: 12 weeks | Supervised: Yes Familiarization: N/A ENEX: F: 3 sessions/week IL: 60–70% HRmax Ti: 20–40 min/session Ty: progressive ET V: 20 min week 1–2, 30 min week 3–4, 40 min week 5–12 P: +10 min every 2 weeks CTRL: F: 3 sessions/week Ti: 40 min/session Ty: stretching exercise. Attrition of ENEX: 22.8% Attrition of CTRL: 27.8% Adherence of ENEX: 81.4% (29.3 of 36 sessions completed) Adherence of CTRL: 77.2% (27.8 of 36 sessions completed) | Analysis within group ENEX: = social functioning (p = 0.09) = social cognition (p = ns) = non-social cognition (p = ns) = BPRS scores for positive and negative symptoms (p = ns) CTRL: Not reported significant effects on the outcomes of interest Analysis between groups ENEX vs. CTRL ↑ ENEX vs. ↓ CTRL of social functioning after 12 weeks (d = 0.35, p = 0.06) |
| Huang et al. [48] | Sex: 45.45% male in ENEX/38.23% male in CTRL BMI (kg/m2): 27.6 ± 4.8 in ENEX/26.1 ± 6.1 in CTRL Race/Ethnicity: N/A Other diseases: N/A Pharmacological treatment: use of antipsychotics in 100% of participants, stable doses for at least 1 month before. Previous physical exercise experience: N/A Patients 20–60 years of age having a diagnosis of schizophrenia (DSM V) with stable psychotic symptoms. | Design: RCT ENEX (aerobic walking + treatment as usual) CTRL (treatment as usual, original lifestyle and psychotropic treatment) Sample size: (n = 67) ENEX: n = 33/CTRL: n = 34 Intervention period: 12 weeks | Supervised: Yes Familiarization: N/A ENEX: F: 3.2 ± 0.8 days /week IL: target 40–60% HRR Ti: 30–50 min/session Ty: walking program V: 128.7 ± 29.1 min P: N/A CTRL (treatment as usual): Ty: original lifestyle and psychotropic treatment. Attrition of ENEX: 15.4% Attrition of CTRL: 10.5% Adherence of groups or study: N/A | Analysis within group ENEX: ↑ performance verbal memory (time effect, p = 0.03; ∆ Z score = 0.52 ± 0.89) CTRL: ↑ performance verbal memory (time effect, p = 0.03; ∆ Z score = 0.47 ± 0.78) Analysis between groups ENEX vs. CTRL No significant time × group interaction effect on BACS scores or any dimension. ENEX: high-intensity vs. low-intensity (cutoff > 40% HRR for high-intensity) No significant time × group interaction effect on BACS score. ↑ ENEX high-intensity vs. ↓ ENEX low-intensity, significant time × group interaction effect on verbal fluency (p = 0.05) after adjusting for duration of illness (MANCOVA). No significant interaction for the rest of dimensions. |
| Kimhy et al. [49] | Sex: 63% male (ENEX)/65% male (CTRL) BMI (kg/m2): 31.60 (ENEX)/30.75 (CTRL) Race/ Ethnicity: 43% Hispanic (ENEX)/29% Hispanic (CTRL) Other diseases: N/A Pharmacological treatment: 100% were prescribed antipsychotics and 6% were prescribed beta-blockers. Previous physical exercise experience: N/A Patients 18–55 years, diagnosis of schizophrenia or related disorders (DSM IV), no changes in the treatment in the last 3 months. | Design: RCT ENEX CTRL (treatment as usual) Sample size: (n = 33) ENEX: n = 16/CTRL: n = 17 Intervention period: 12 weeks | Supervised: Yes Familiarization: N/A ENEX: F: 3 sessions/week IL: 60–70% HRmax Ti: 45 min/session Ty: progressive ET + standard psychiatric care. V: 135 min per week P: +5% HRmax first 4 weeks CTRL: Standard psychiatric, regular meetings with a psychiatrist, psychologists, social workers, and/or psychiatric nurses. Attrition of ENEX: 19% Attrition of CTRL: 23.5% Attrition of the study: 21% (3 dropped out in ENEX and 4 dropped out in CTRL) Adherence of ENEX: 79% (28.5 of 36 sessions) Adherence of CTRL: N/A Adherence of study: N/A | Analysis within group ENEX: Not reported significant effects on the outcomes of interest CTRL: Not reported significant effects on the outcomes of interest Analysis between groups ENEX vs. CTRL ↑ENEX (+23%) vs. ↓CTRL (−4.2%) in social functioning index PSRS (p = 0.012) No significant differences in social functioning index by SANS (p = 0.58) No significant differences in social functioning index by SLOF (p = 0.22) |
| Marzolini et al. [50] | Sex: 51.14% male (CONCEX)/66.66% male (CTRL) BMI (kg/m2): 27.2 ± 1.2 (CONCEX)/29.3 ± 2.2 (CTRL) Race/Ethnicity: N/A Other diseases: At least cardiovascular risk. Pharmacological treatment: 6 used atypical antipsychotics, 5 used typical antipsychotics and 3 used antianxiety in CONCEX and 5 used atypical antipsychotics, 3 used typical antipsychotics, 2 used antidepressants and 4 used antianxiety in CTRL. Previous physical exercise experience: N/A Individuals with a diagnosis of schizophrenia/schizoaffective (DSM IV) and at least 1 cardiovascular risk. | Design: RCT CONCEX CTRL (usual care) Sample size: (n = 13) CONCEX: n = 7/CTRL: n = 6 Intervention period: 12 weeks | Supervised: Yes Familiarization: N/A CONCEX: F: 2 sessions/week IL: RT: starting 60% 1RM. 10–15 reps (last set repetition at RPE 15)/ET: 60–80% HRR (RPE 11–14) Ti: 20 min (RT) + 60 min (ET) each session Ty: CT V: RT: 4 exercises upper- and lower-limbs: 1–2 × 10–15 reps, r: >30 s/ET: 1.6km to 6.4 km P: RT: +1–2 kg based on RPE/ET: +3.33% HRR each 2 weeks CTRL: Usual care Attrition of study: 0% (all participants attended, at least, 50% of sessions; no participant dropped-out) Adherence of CONCEX: 72% (±4.4%) | Analysis within group CONCEX: ↑ MHI score after 12 weeks (p = 0.03) ↑ 6MWD = ↑ MHI total score (p = 0.09) ↓ depressive symptoms (MHI subscale) = ↑ 6MWD (p < 0.001) ↓ depressive symptoms (MHI subscale) = ↑ adherence to exercise (p = 0.02) CTRL: = MHI score after 12 weeks (p = 0.57) ↑ 6MWD = ↑ MHI total score (p = 0.09) ↓ depressive symptoms (MHI subscale) = ↑ 6MWD (p < 0.001) Analysis between groups CONCEX vs. CTRL No significant differences in MHI score (p = 0.33) |
| Ryu et al. [51] | Sex: 50% male in ENEX/56.66% male in CTRL BMI (kg/m2): N/A Race/Ethnicity: N/A Other diseases: N/A Pharmacological treatment: 100% were prescribed antipsychotics with a stable dose for at least 4 weeks before intervention. Previous physical exercise experience: No (exclusion of patients who participated in any exercise program 3 months before the study). Outpatients 18–65 years old, with a diagnosis of schizophrenia or schizoaffective disorder (DSM IV). | Design: Single blind RCT ENEX (outdoor cycling) CTRL (occupational therapy) Sample size: (n = 60) ENEX: n = 30/CTRL: n = 30 Intervention period: 16 weeks | Supervised: Yes Familiarization: N/A ENEX: F: 1 session/week IL: 16km/h Ti: 40 min of bike training each session Ty: outdoor cycling. V: 40 min per week P: N/A CTRL: F: 1 session/week Ty: daily living skills, social skills, or creative activities. Ti: 90 min/session Attrition of ENEX: 13.3% Attrition of CTRL: 20% Attrition of the study: 16.7% Adherence of groups or study: N/A | Analysis within group ENEX: ↓ psychotic symptoms (BPRS) (p = 0.042) ↓ thought disturbance (subscales of BPRS) (p = 0.002) ↓ BDI score (p < 0.001) ↓ STAI-state score (p = 0.001) ↓ STAI-trait score (p < 0.001) ↑ GAF score (p = 0.001) ↑ WCST CR (p < 0.001) ↑ WCST CC (p = 0.005) CTRL: = psychotic symptoms (BPRS) (p = 0.136) = BDI score (p = 0.945) = STAI-state score (p = 0.696) = STAI-trait score (p = 0.788) = GAF score (p = 0.556) = WCST CR (p = 0.406) = WCST CC (p = 0.838) Analysis between groups ENEX vs. CTRL No significant group × time interaction in RSES (p = 0.052) No significant group × time interaction in QoL score (p = 0.098) |
| Battaglia et al. [52] | Sex: 100% male BMI (kg/m2): 28.55 ± 4.06 in ENEX/28.65 ± 2.62 in CTRL Race/ Ethnicity: N/A Other diseases: N/A Pharmacological treatment: 100% were prescribed antipsychotics (clozapine, olanzapine or risperidone) with a stable dose. Previous physical exercise experience: at least 1 year of soccer experience. Male patients with a diagnosis of schizophrenia or schizoaffective disorders (DSM IV) > 18 years old. | Design: Double- blind RCT ENEX CTRL Sample size: (n = 18) ENEX: n = 10/CTRL: n = 8 Intervention period: 12 weeks | Supervised: Yes Familiarization: N/A ENEX: F: 2 sessions/week IL: 50–85% HRmax Ti: 40–60 min of training period each session Ty: progressive soccer technical-tactical exercises and soccer games V: 80–120 min per week P: +5 min each game after week 5 and +5 min each game after week 8. CTRL: not performed any organized physical activity. Attrition/Adherence: N/A | Analysis within group ENEX: ↑ MCS-12 score (+10.8%, p < 0.0001) CTRL: Not reported significant effects on the outcomes of interest Analysis between groups ENEX vs. CTRL ENEX > CTRL in MCS-12 score after 12 weeks (p < 0.0001) |
| Nygård et al. [53] | Sex: 58.33% male BMI (kg/m2): 29.7 (CONCEX)/30 (CTRL) Race/Ethnicity: N/A Other diseases: 11 smokers in TG and 8 in CG (without any other chronic disease). Pharmacological treatment: 24 were prescribed antipsychotics, 3 antiepileptics, 8 benzodiazepine, 2 biperiden, 1 levaxine, 1 lithium and 1 SSRI in ENEX/21 were prescribed antipsychotics, 3 antiepileptics, 6 benzodiazepine, 1 levaxine, 2 lithium and 3 SSRI in CTRL. Previous physical exercise experience: N/A Outpatients, 22–59 years old with a diagnosis of schizophrenia spectrum disorders (ICD-10). | Design: RCT CONCEX CTRL Sample size: (n = 36) CONCEX: n = 17/CTRL: n = 19 Intervention period: 12 weeks | Supervised: Yes Familiarization: 1 day with a familiarization session on treadmill and leg press. CONCEX: F: 2 sessions/week IL: RT: 90% of 1RM/ET: 85–95% of HRpeak Ti: 35 min (ET) Ty: endurance interval training on treadmill + leg press MST V: RT: 4 × 4 reps, r: 3–4 min. 8 reps per session/ET: 4 × 4 min, r: 3 min (at 70% of HRpeak). 70 min per week P: +5 kg each session the patient managed to complete 5 reps (RT) CTRL: 2 training sessions; participants were encouraged to train on their own. Attrition of ENEX: 32% Attrition of CTRL: 17% Adherence of groups or study: N/A | Analysis within group CONCEX: = mental health index by SF-36 (p = 0.158) CTRL: = mental health index by SF-36 (p = 0.934) Analysis between groups CONCEX vs. CTRL No group × time significant differences in mental health index by SF-36 (p = 0.277) |
| Massa et al. [54] | Sex: 76.19% male (ENEX) /88.23% male (CTRL) BMI (kg/m2): 31.11 ± 6.87 (ENEX)/29.31 ± 4 (CTRL) Race/Ethnicity: 19 African American (ENEX)/17 African American (CTRL). Other diseases: N/A Pharmacological treatment: 14 were prescribed atypical antipsychotics, 1 typical antipsychotics, 2 both, 6 antidepressants and 4 were not prescribed with any antipsychotic in ENEX/ 13 were prescribed atypical antipsychotics, 2 typical antipsychotics, 1 both, 4 antidepressants and 1 were not prescribed with any antipsychotic in CTRL. Previous physical exercise experience: No, sedentary lifestyle for the last month. Outpatients with a diagnosis of schizophrenia, 18–70 years old. | Design: RCT (assessments were completed by an assessor-blinded to the treatment group): ENEX CTRL Sample size: (n = 38) (only completed 15) ENEX: n = 21 (completed the study 9) CTRL: n = 17 (completed the study 6) Intervention period: 12 weeks (follow-up to week 20) | Supervised: Yes Familiarization: N/A ENEX: F: 3 sessions/week IL: 50–80% of HRmax Ti: 20–45 min Ty: progressive ET on a stationary bicycle ergometer. V: from 60 min to 135 min per week P: +5 min and +5% HRmax per week CTRL: 3 sessions/week Ty: stretching and toning exercise performed for the same amount of time as the AE program. Attrition of ENEX: 68.08% Attrition of CTRL: N/A Adherence of groups or study: N/A | Analysis within group ENEX: No significant difference after week 12 for MCCB composite scores CTRL: No significant difference after week 12 for MCCB composite scores Analysis between groups ENEX vs. CTRL ↑ENEX vs. ↓CTRL in MCCB composite score from week 12 to week 20 (p = 0.03) ↑ENEX vs. ↓CTRL in visual learning domain of MCCB composite score from week 12 to week 20 (p = 0.006) |
| Su et al. [55] | Sex: 45.5% male (ENEX)/45.5% male (CTRL) BMI (kg/m2): 30.72 (ENEX)/34.56 (CTRL) Race/ Ethnicity: N/A Other diseases: N/A Pharmacological treatment: were on stable antipsychotic medication with no major dose changes for at least 3 months before the study. Previous physical exercise experience: N/A Patients with a diagnosis of criteria for schizophrenia or schizoaffective disorder (DSM IV) with a stable medication. | Design: Single-blinded RCT ENEX CTRL (stretching and toning control group) Sample size: (n = 44) ENEX: n = 22/CTRL: n = 22 Intervention period: 12 weeks (follow-up to 6 months) | Supervised: Yes Familiarization: N/A ENEX: F: 4–5 sessions/week IL: 55–69% HRmax/13–16 RPE Ti: 30 min Ty: progressive ET on treadmill V: 120–150 min per week P: Not specified. CTRL: F: 4–5 sessions/week IE: 14 exercises, held for 10 s and repeated 10 times. Ti: 30 min Ty: stretching and toning control program. Attrition of groups or study: N/A Adherence of ENEX: 76.6% (45.95 of the 60 maximum scheduled sessions) Adherence of CTRL: 78.2% (46.91 of the 60 maximum scheduled sessions) | Analysis within group ENEX ↑ processing speed scores at posttest (p = 0.005) ↑ processing speed scores at follow-up (p = 0.009) ↑ attention scores at follow-up > posttest (p = 0.006) ↑ verbal learning scores at follow-up > posttest (p = 0.009) ↑ verbal learning scores at follow-up > pretest (p = 0.3001; ↑25.6%) CTRL: Processing speed scores at follow-up > posttest (p = 0.02) ↑ verbal learning scores at posttest (p = 0.02) Reasoning and problem solving at follow-up > posttest (p = 0.003) Analysis between groups ENEX vs. CTRL ENEX > CTRL In processing speed scores at posttest (p = 0.001) ENEX > CTRL in attention scores at posttest (p = 0.03) CTRL > ENEX in PANSS negative symptoms score at follow-up (p = 0.03) |
| Kimhy et al. [56] | Sex: 63% male (ENEX)/65% male (CTRL) BMI (kg/m2): 31.60 (ENEX)/30.75 (CTRL) Race/Ethnicity: 43% Hispanic (ENEX)/29% Hispanic (CTRL) Other diseases: 25% smokers (ENEX)/23% smokers (CTRL) Pharmacological treatment: 100% used antipsychotics, 44% used antidepressants and 31% used SSRIs in ENEX/100% used antipsychotics, 35% used antidepressants and 23% used SSRIs in CTRL. Previous physical exercise experience: N/A Outpatients with a diagnosis of schizophrenia or related disorders (DSM IV); age 18–55 years. | Design: Single-blind RCT ENEX CTRL (treatment as usual) Sample size: (n = 33) ENEX: n = 16/CTRL: n = 17 Intervention period: 12 weeks | Supervised: Yes Familiarization: N/A ENEX: F: 3 sessions/week IL: 60–75% of HRmax Ti: 45 min Ty: progressive ET with 2 active-play video game systems, 2 treadmill machines, a stationary bike and an elliptical machine. V: 135 min per week P: +5% of HRmax after week 1, +5% after week 2 and +5% after week 3. CTRL: Standard psychiatric care, regular meetings with a psychiatrist, psychologists, social workers or psychiatric nurses. Attrition of ENEX: 18.7% (dropped-out 3) Attrition of CTRL: 23.5% (dropped-out 4) Attrition of the study: 21% Adherence of ENEX: 79% (28.5 of 36 sessions) Adherence of study: N/A | Analysis within group ENEX: Not reported CTRL: Not reported Analysis between groups ENEX vs. CTRL ↑ENEX (+15%) > ↓CTRL (−2%) in MCCB composite scores after 12 weeks (p = 0.031) |
| Nygård et al., 2023 [57] | Sex: 58.33% male BMI (kg/m2): 27.98 ± 1.67 (CONCEX), 25.5 ± 5.0 (CTRL) Race/Ethnicity: N/A Other diseases: N/A Pharmacological treatment: First generation antipsychotics (n = 7), second generation antipsychotics (n = 42), clozapine (n = 18), 2 antipsychotics (n = 17) and without antipsychotics (n = 3) Previous physical exercise experience: N/A Outpatients with a schizophrenia spectrum disorders diagnosis (International Statistical Classification of Diseases (ICD)-10) between 18 and 65 years with clinically stable disease. | Design: RCT CONCEX CTRL Sample size: (n = 48) CONCEX: n = 25/CTRL: n = 23 Intervention period: 1 year | Supervised: Yes Familiarization: 1 session CONCEX: 2 sessions/week IL: RT: 90% 1RM/ET: 85–95% HRpeak Ti: RT: N/A/ET: 35 min Ty: leg press MST + interval ET. V: RT: 4 × 4 reps of leg press (r: 3–4 min), 32 reps per week/ET: 4 × 4 min treadmill walking/running (r: 3 min) P: RT: +5 kg if 5 reps in last set/ET: +1.75% per week CTRL: 2 introductory training sessions to inform them of the benefits of regular exercise and encourage them to train on their own. Attrition of CONCEX: 40% Attrition of CTRL: 21.74% Adherence of study: 64.58% (62 ± 16 attended sessions of 96) | Analysis within group CONCEX: = SF-36 score after 3 months (p = 0.720) = SF-36 score after 1 year (p = 0.336) CTRL: = SF-36 score after 3 months (p = 0.720) = SF-36 score after 1 year (p = 0.336) Analysis between groups CONCEX vs. CTRL No group × time significant differences in SF-36 scores after 3 months (p = 0.436) or 1 year (p = 0.304) |
RCT: randomized controlled trial; ENEX: endurance exercise; RESEX: resistance exercise; CONCEX: concurrent exercise; CTRL: control group; ET: endurance training; RT: resistance training; CT: concurrent training; HIIT: high-intensity interval training; FTP: functional threshold power; MST: maximal strength training; IL: intensity load; Ti: time; Ty: type; V: volume; P: progression; ns: not significant; DSM: diagnostic and statistical manual of mental disorders; PANSS: positive and negative syndrome scale; SF-36: short form-36 health survey; BPRS: brief psychiatric rating scale; BACS: brief assessment of cognition in schizophrenia; PSRS: positive self-relation scale; SANS: scale for the assessment of negative symptoms; SLOF: specific level of functioning; 6MWD: six minute walk distance; MHI: mental health inventory; BDI: Beck’s depression inventory; RSES: Rosenberg self-esteem scale; STAI: state-trait anxiety inventory; GAF: global assessment of functioning; QoL: quality of life; WCST-CC: Wisconsin card sorting test-categories complete; WCST-WR: Wisconsin card sorting test-correct rate; MCS-12: mental component summary; SF-12: short form-12 health survey; MCCB: MATRIC’s consensus cognitive battery; N/A: not applicable.
3. Results
3.1. Study Selection
The electronic search strategy retrieved 1210 articles, of which 480 papers stemmed from Web of Science, 442 from Scopus, 266 from PubMed, and 22 from SPORTDiscus with full text. After removing duplicates, 696 potentially relevant studies remained for screening. After analyzing the title and abstract, 655 studies were excluded and 41 full-text articles were reviewed (Supplementary Materials File S2). Finally, 13 of those papers were relevant to this review. The PRISMA flow diagram is shown in Figure 1.
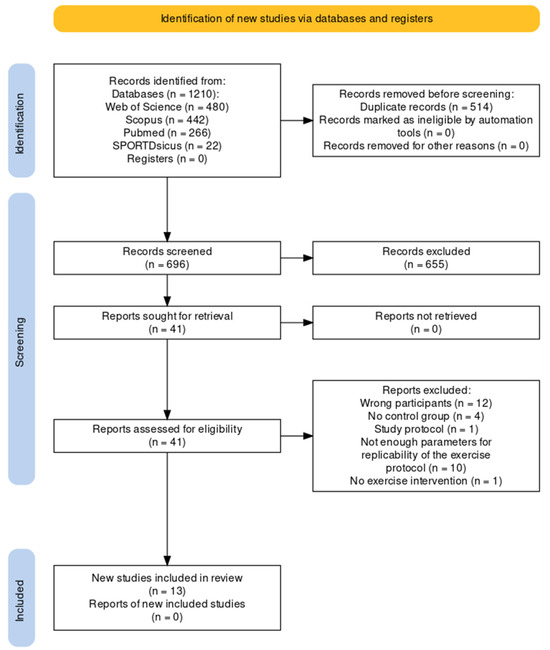
Figure 1.
Flowchart of study following the PRISMA (Preferred Reporting Items for Systematic Meta-Analyses) guidelines.
3.2. Study Characteristics
The main characteristics and findings of interest are shown in Table 2. The twelve eligible articles included a total sample of 553 participants over 18 years old [45,46,47,48,49,50,51,52,53,54,55,56,57]. All of these studies were randomized controlled trials, of which only seven were blinded [49,51,52,54,55,56,57]. According to the type of training, most articles evaluated interventions with endurance training (ET) (70%) [46,47,48,49,51,52,54,55,56]. The other studies used concurrent or combined training (CT) programs as exercise intervention [45,50,53,57], and one of them additionally implemented an isolated resistance exercise training (RT) intervention [45]. Most of these protocols lasted 12 weeks [46,47,48,49,50,52,53,54,55,56] with the exception of three studies that used 20 weeks [45], 16 weeks [51], and 1 year [57], respectively.
3.3. Critical Appraisal
3.3.1. Risk of Bias
The risk of bias reported by the Rob 2 tool is shown in Figure 2 and Figure 3. Nine (70%) of the included articles were considered at high risk of bias in the overall score [45,46,47,49,51,52,53,54,55]. Concerning the different domains, eleven studies (84.6%) were assessed as being at low risk regarding bias arising from the randomization process [45,46,48,50,51,52,53,54,55,56,57]. Only four randomized controlled trials (30.77%) were judged as being at low risk considering bias due to deviations from intended interventions [48,49,56,57]. Seven studies (53.84%) reported a low risk of bias due to missing outcome data [46,47,48,49,50,56,57]. All studies except one [53] were classified as low risk in the fourth domain (bias in the outcome measurement). Finally, five studies (30.77%) were assessed as being at low risk regarding bias in the selection of the reported results [45,48,53,56,57].
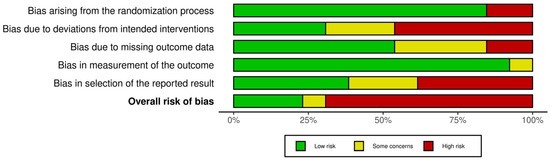
Figure 2.
Risk of bias graph: judgment regarding each risk-of-bias item, presented as percentages across all included studies.
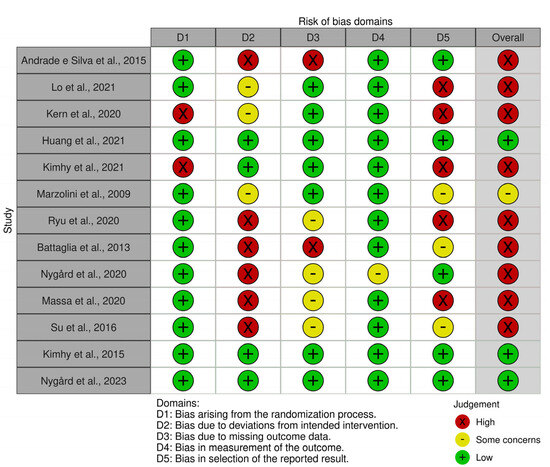
Figure 3.
Ratings considering risk-of-bias items for each study. The references of the cited articles [45,46,47,48,49,50,51,52,53,54,55,56,57] can be found in the reference list.
3.3.2. Quality Reporting of Exercise Intervention in the Training Programs
The rigor of the intervention protocols regarding the total sample (TS), ET, CT, and RT is shown in Table 3 after the evaluation of the CERT items in the included articles. The reviewers evaluated item 13, which refers to the description of the exercise, with a specific emphasis on whether the exercise fulfilled the F.I.T.T.−V.P. parameters. However, the articles did not provide a complete account of all the parameters of F.I.T.T.−V.P. The aforementioned item 13 was the most commonly reported in exercise interventions (100%). The second most frequently reported item was whether the exercises were generic or tailored to the individual, with 76.9%, 66.7%, 100%, and 100% reporting for TS, ET, CT, and RT, respectively. The third most commonly reported item was the degree to which the intervention was executed according to plan, with 76.9%, 77.7%, and 66.7% reporting for TS, ET, and CT, respectively; however, this item was not reported in the resistance training protocol. On the other hand, adherence, replication, and home components were not reported by any of the included articles, while motivation strategies were reported in less than 10% of the selected studies. Further, only Kimhy et al. [49] reported more than 50% of CERT items when describing their exercise intervention.
Table 3.
Exercise intervention quality report of the included studies according to the CERT.
3.4. Summary of Evidence
3.4.1. Psychopathology
Eight articles among the eligible studies evaluated the effects of physical exercise on the psychopathology of individuals diagnosed with schizophrenia [45,46,47,49,50,51,52,55]. The measuring instruments used to evaluate the results were the positive and negative symptoms scale (PANSS) [45,46,49,55], the mental health inventory (MHI) [50], the brief psychiatric rating scale (BPRS) [47,51], Beck’s depression inventory (BDI) [51], the state and trait anxiety inventory (STAI) [51], the Rosenberg self-esteem scale (RSES) [51], and the mental component summary (MCS-12) of self-reported QoL short form (SF-12) [52].
Taking all these results together, most of the reviewed studies showed benefits in some psychopathological variables after exercise independently of the training protocol [45,50,51,52,55]. Only one of the studies used two training protocols with different types of exercise (i.e., ET and RT), demonstrating a decrease in negative symptoms only after RT [45]. Three of the included studies [46,47,49] found no significant differences in positive or negative symptoms of schizophrenia following an ET program with comparable characteristics (i.e., three sessions per week over 12 weeks, with a duration of 20 to 60 min per session).
3.4.2. Cognition
Eight of the eligible articles assessed cognitive variables using different measuring instruments. In this regard, Kimhy et al. [56], Su et al. [55], and Massa et al. [54] revealed improvements in MATRICS Consensus Cognitive Battery (MCCB) scores in patients with diagnosis of schizophrenia. Specifically, these studies found improvements in processing speed, attention, verbal learning domains [55], and visual learning [54] following a regular ET program. Huang et al. [48] found no significant improvements in cognitive function as assessed using the Brief Assessment of Cognition in Schizophrenia (BACS) instrument when comparing the exercise group and control group (maintenance of original lifestyle and psychotropic treatment) following a 12 week walking exercise program (i.e., ET). Ryu et al. [51] reported an increase in executive function scores as measured by the Wisconsin Card Sorting Test (WCST) in individuals diagnosed with schizophrenia after following an outdoor cycling training. In the same line, Lo et al. [46] evaluated sleep-dependent procedural memory consolidation performance as measured by the finger-tapping motor sequence task (MST). These authors showed that both high-intensity interval training (HIIT) and moderate-to-vigorous (91–105% of the functional threshold power, FTP) ET had a positive impact on memory consolidation. Moreover, HIIT was found to be more effective than moderate-to-vigorous (91–105% FTP) continuous ET.
3.4.3. Quality of Life
A number of recent studies [45,51,52,53,57] have used different instruments to assess patients’ QoL (e.g., the Short Form (SF)-36 Health Survey, World Health Organization Quality of Life Scale Abbreviated Version (WHOQOL-BREF), SF-12 Health Survey, Patient Activation Measure-13). However, the impact of exercise programs on the QoL of individuals with schizophrenia remains inconclusive. Silva et al. [45] and Battaglia et al. [52] reported positive effects of physical exercise, whereas other studies [51,53,57] did not obtain significant changes. Conversely, with regard to the social domain, Kern et al. [47] and Kimhy et al. [49] demonstrated that physical exercise could benefit social functioning.
4. Discussion
The main findings of this scoping review were: (1) supervised regular physical exercise of various modalities improves the psychopathology of schizophrenia; (2) regular ET seems to be an effective strategy to enhance cognitive function in patients with schizophrenia, while evidence regarding other training modalities is limited; and (3) while regular exercise may promote both social functioning and social cognition, thereby positively affecting the QoL of patients diagnosed with schizophrenia, the results are currently inconclusive.
To the best of our knowledge, this is the first scoping review to include studies that meet strict selection criteria for ensuring replicability regarding exercise training protocol characteristics. Further, a special focus was placed on the effects of those training protocols on the three main non-physical health-related areas affected by schizophrenia (i.e., psychopathology, cognition, and QoL). Considering the limited availability of randomized controlled trials satisfying the predetermined selection criteria, conducting a meta-analysis of the data was unfeasible.
4.1. Training Characteristics of the Included Studies
Concerning the training protocol duration, most of the works reported an intervention period of 12 weeks [46,47,48,49,50,52,53,54,55,56]. However, three studies deviated from this standard duration, with intervention periods of 16 weeks [51], 20 weeks [45], and 1 year [57]. Furthermore, other reviews found a similar mean duration [58,59], while certain authors [31,32] presented heterogeneous durations in their included studies. In this context, extended intervention durations exhibited a correlation with reduced rates of adherence to training programs. This implies that briefer intervention periods may be better tolerated by individuals diagnosed with schizophrenia. Additional research is needed to explore strategies aimed at improving adherence to exercise interventions in individuals with schizophrenia. It is worth noting that, concerning the form of physical exercise utilized, the prevailing mode of physical training in this review was ET [46,47,48,49,51,52,54,55,56]. Only one of the selected studies included RT for one of its groups of participants [45]. Our results are in accordance with most previous reviews, as the majority of their articles reported ET interventions [32,58,59,60]. In line with this, in a recent review by Bredin et al. [33], the above authors refer to three studies reporting RT interventions. However, when analyzing this more deeply, one of the studies is already included in our review, while the others are a pilot study [61] and a study with an intervention protocol that was not described in sufficient detail to ensure replication [62]. Although scientific evidence has widely demonstrated that RT has important health-related benefits on the regulation of diabetes, weight loss, and improvements in cardiovascular health [63,64], as well as in cognitive abilities and self-esteem [63], RT interventions among patients with schizophrenia are scarce.
Regarding the quality of the analyzed training protocols, it was observed that many of the CERT tool items were not reported. It is striking that less than 10% of the studies reported the motivational strategies implemented in their training interventions. In this regard, it has been previously suggested that patients suffering from schizophrenia present different barriers that prevent them from reaching the minimum exercise recommendations, with lack of motivation being one of the most important [65,66,67]. Hence, it is of paramount importance to describe in detail those motivational strategies that optimize adherence to physical exercise in patients with schizophrenia [66,67]. While recent systematic reviews have neglected to incorporate the CERT checklist for the reviewed articles, and have further failed to report data pertaining to motivation strategies and adherence to the exercise sessions [36,37,39,40], Gallardo et al. [37] and Cella et al. [36] have underscored the pivotal role of motivation in ameliorating adherence to interventions and optimizing the positive effects of exercise programs among this population.
In the reviewed body of literature, it is noteworthy that only approximately 50% of the studies reported on the inclusion of non-exercise components. The non-exercise component encompasses social interactions and interpersonal relationships, both of which constitute integral elements of supervised training and group-based interventions. It is imperative to acknowledge that these facets may exert an influence on the outcomes observed after physical exercise interventions [66].
4.2. Effects of Regular Exercise on Psychopathology, Cognition, and Quality of Life of Patients with Schizophrenia
4.2.1. Psychopathology
Concerning the effects of overall physical exercise on patients with schizophrenia, the results of the included studies reported important health-related benefits. Silva et al. [45], Marzolini et al. [50], and Ryu et al. [51] showed improvements in psychiatric symptoms of the disease. These findings align with previous reviews [30,37,58] that reported positive outcomes of ET and other training modalities on both the positive and negative symptoms of schizophrenia, validating the beneficial effects of these interventions. In this regard, another recent review by Bredin et al. [33] showed improved PANSS scale scores following walking training. Further, the authors of a study that implemented an aerobic exercise program for 12 weeks demonstrated that exercise both improved patients’ symptoms and prevented up to a 7% increase in negative symptoms observed in the subsequent follow-up of patients in the control group [68]. Similar results have been reported by several studies [30,31,35,60,69,70], whereas other authors [46,47,49] did not show significant changes in psychiatric symptoms after prescribing ET. In this regard, a minimum physical exercise intensity threshold seems to be necessary for obtaining health benefits, as when the data related to low-intensity interventions (e.g., yoga and stretching) were removed from the meta-analysis these authors obtained significant improvements in psychiatric symptoms [32]. Additionally, interventions involving moderate-to-vigorous exercise accumulating approximately 90 min per week produced significant reductions in psychiatric symptoms and improved the cognitive function, co-morbid disorders, and functioning of individuals with schizophrenia [32]. It is difficult to analyze what the causes of these discrepancies in these results might be. On the one hand, there is some difficulty in carrying out the methodology of studies with physical exercise in patients with schizophrenia. We can see this reflected when looking at the dropout rates of the included studies. Despite the strictness of the inclusion criteria in terms of methodology, most studies exceeded a 10% dropout rate [45,46,47,48,49,51,52,53,54,55,56]. Specifically, one exceeded a 50% dropout rate without specifying any medical or personal cause that prevented the patients from carrying out exercise [54]. The differences between patients and the wide variety of physical, psychological, and social factors that impact their lives may be among the reasons that hinder the generalization of results [69]. Along with this, the methodological shortcomings of the included studies and their exercise interventions, which we have previously analyzed, make it difficult to compare results [28].
Focusing attention on affective symptoms reported in the included articles, Marzolini et al. demonstrated improvements in depressive symptoms by enhancing functional capacities after 12 weeks of CT [50]. Similarly, Ryu et al. [51] showed improved depressive symptoms and levels of anxiety after 16 weeks of outdoor cycling in patients with schizophrenia. This association between aerobic exercise and depressive symptoms in patients with schizophrenia was already demonstrated in 1993 by Pelham et al. [71], who concluded that this type of exercise decreased depressive symptoms. Furthermore, more recent studies support these positive effects after 12 weeks of CT [72], while other authors have reported positive effects on anxiety [73].
4.2.2. Cognition
Regarding the cognitive effects of physical exercise on schizophrenia, our results are in accordance with previous reviews [59,74]. Firth et al. [59] additionally differentiated those domains that independently reflect a significant improvement after the exercise intervention (i.e., working memory, social cognition, and attention/vigilance). In these domains, we found specific improvements in three of the clinical trials selected in our review [47,48,55]. In this regard, a recent systematic review and meta-analysis performed with older adults suggested a nonlinear dose-response relationship between overall exercise and cognition [75]. The authors estimated a minimal threshold of 724 METs a minute per week for obtaining relevant changes in cognition. Moreover, although lower doses of different exercise types could already produce benefits, it seems that RT leads to greater positive effects on cognition in older adults than other training modalities [75]. Certain authors have mentioned the relationship between training intensity and the magnitude of effects on cognition in patients with schizophrenia [48]. These researchers found study greater benefits in attention, processing speed, and verbal fluency with high ET intensity [48]. Nevertheless, further investigation is warranted in order to assess the potential of resistance training (RT) as a cognitive enhancement intervention in individuals diagnosed with schizophrenia.
4.2.3. Quality of Life and Functioning
The majority of research included in the present scoping review supports the implementation of physical exercise as a tool to improve the QoL and functioning of individuals with schizophrenia [45,49,52]. Nevertheless, further studies are warranted to meticulously address potential biases and provide comprehensive descriptions of the independent variable, that is, exercise, in order to enhance the quality of evidence in this field. In this regard, three studies that investigated QoL and functioning did not find significant improvements in the different scales used [47,53,57].
Ryu et al. [51] showed improvements in global functioning index as measured by the GAF scale after 16 weeks of ET; however, they did not report changes in QoL. These results are in line with a pilot study by Loh and colleagues [70], who showed improvements in QoL, the social functioning component, and the global functioning index as assessed through the personal social performance scale (PSP) after 12 weeks of structured walking training. According to this, Acil et al. [24] observed improvements after an ET program in the scores related to QoL in participants with schizophrenia. Although there is some controversy surrounding this topic, and the results obtained from various studies remain inconclusive and subject to methodological limitations, the available evidence suggests that regular exercise has the potential to enhance both social and global functioning, exerting a positive impact on the QoL of individuals diagnosed with schizophrenia.
Considering all the evidence, the regular engagement in diverse forms of physical exercise exhibited potential in yielding health benefits in the mental and social domains in patients diagnosed with schizophrenia. Nevertheless, there is a lack of knowledge on the optimal dose–response relationship and the types of exercise that produces the greatest health benefits and optimizes QoL.
5. Future Perspectives
Due to the nature of this scoping review, the possibility of conducting a meta-analysis was impeded by the inclusion of multiple outcomes and the limited number of articles per outcome. One of the challenges encountered during the review process was the insufficient availability of detailed information regarding exercise characteristics in the reviewed studies, which restricts the transferability of the results to clinical practice and the replicability of future studies.
While recent investigations suggest that multimodal or concurrent training (CT) programs are more effective than isolated exercise training for patients diagnosed with schizophrenia [33,34], further research is needed to establish optimal dose–response relationships and exercise types, particularly in relation to non-physical health-related components such as psychopathology, cognition, and quality of life. Future interventions targeting individuals diagnosed with schizophrenia should adhere to the CERT criteria, which consider factors such as motivation, exercise supervision, adherence, adverse event reporting, and non-exercise components. On the other hand, it could be interesting for future research to consider the influence of hormones on this disease and on the effects of its treatment [76]. In light of the limitations imposed by the challenges of daily life associated with this condition, considering these aspects could improve both the methodological approach and the training protocol itself, leading to overall enhancements in patients diagnosed with schizophrenia.
Supplementary Materials
The following supporting information can be downloaded at: https://www.mdpi.com/article/10.3390/bs13120959/s1, File S1: Electronic search strategy; File S2: Excluded studies and reasons for exclusion. References [24,61,62,68,77,78,79,80,81,82,83,84,85,86,87,88,89,90,91,92,93,94,95,96,97,98,99,100] are cited in the Supplementary Materials.
Author Contributions
Conceptualization, L.V.-B., E.C. and X.D.-C.; methodology, E.C. and X.D.-C.; screening process, L.V.-B., A.V.-S. and X.D.-C.; data extraction, L.V.-B., A.V.-S. and E.I.-S.; data curation, L.V.-B. and E.C.; writing—original draft preparation, L.V.-B., E.C. and A.V.-S.; writing—review and editing, L.V.-B., E.C., A.V.-S., E.I.-S. and X.D.-C.; visualization, L.V.-B. and E.I.-S.; supervision, E.C. and X.D.-C. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Conflicts of Interest
The authors declare no conflict of interest.
References
- ICD-11 for Mortality and Morbidity Statistics [Internet]. Available online: https://icd.who.int/browse11/l-m/en#/http%3a%2f%2fid.who.int%2ficd%2fentity%2f1683919430 (accessed on 26 November 2022).
- American Psychiatric Association. Guía de Consulta de los Criterios Diagnósticos del DSM-5; American Psychiatric Publishing: Arlington, VA, USA, 2014. [Google Scholar]
- GBD Results [Internet]. Institute for Health Metrics and Evaluation. Available online: https://vizhub.healthdata.org/gbd-results (accessed on 28 November 2022).
- Jin, H.; Mosweu, I. The Societal Cost of Schizophrenia: A Systematic Review. PharmacoEconomics 2017, 35, 25–42. [Google Scholar] [CrossRef]
- Keepers, G.A.; Fochtmann, L.J.; Anzia, J.M.; Benjamin, S.; Lyness, J.M.; Mojtabai, R.; Servis, M.; Walaszek, A.; Buckley, P.; Lenzenweger, M.F.; et al. The American Psychiatric Association Practice Guideline for the Treatment of Patients with Schizophrenia. Am. J. Psychiatry 2020, 177, 868–872. [Google Scholar] [CrossRef]
- Pennington, M.; McCrone, P. The Cost of Relapse in Schizophrenia. PharmacoEconomics 2017, 35, 921–936. [Google Scholar] [CrossRef]
- Correll, C.U.; Ng-Mak, D.S.; Stafkey-Mailey, D.; Farrelly, E.; Rajagopalan, K.; Loebel, A. Cardiometabolic comorbidities, readmission, and costs in schizophrenia and bipolar disorder: A real-world analysis. Ann. Gen. Psychiatry 2017, 16, 9. [Google Scholar] [CrossRef]
- Ride, J.; Kasteridis, P.; Gutacker, N.; Aragon, M.J.A.; Jacobs, R. Healthcare Costs for People with Serious Mental Illness in England: An Analysis of Costs Across Primary Care, Hospital Care, and Specialist Mental Healthcare. Appl. Health Econ. Health Policy 2020, 18, 177–188. [Google Scholar] [CrossRef]
- Auquier, P.; Lançon, C.; Rouillon, F.; Lader, M. Mortality in schizophrenia. Pharmacoepidemiol. Drug Safe 2007, 16, 1308–1312. [Google Scholar] [CrossRef]
- Connolly, M.; Kelly, C. Lifestyle and physical health in schizophrenia. Adv. Psychiatr. Treat. 2005, 11, 125–132. [Google Scholar] [CrossRef]
- Hennekens, C.H.; Hennekens, A.R.; Hollar, D.; Casey, D.E. Schizophrenia and increased risks of cardiovascular disease. Am. Heart J. 2005, 150, 1115–1121. [Google Scholar] [CrossRef]
- Lee, S.-H.; Kim, G.; Kim, C.-E.; Ryu, S. Physical Activity of Patients with Chronic Schizophrenia and Related Clinical Factors. Psychiatry Investig. 2018, 15, 811–817. [Google Scholar] [CrossRef]
- Vancampfort, D.; Firth, J.; Schuch, F.B.; Rosenbaum, S.; Mugisha, J.; Hallgren, M.; Probst, M.; Ward, P.B.; Gaughran, F.; De Hert, M.; et al. Sedentary behavior and physical activity levels in people with schizophrenia, bipolar disorder and major depressive disorder: A global systematic review and meta-analysis. World Psychiatry 2017, 16, 308–315. [Google Scholar] [CrossRef]
- Vancampfort, D.; Probst, M.; Knapen, J.; Carraro, A.; De Hert, M. Associations between sedentary behaviour and metabolic parameters in patients with schizophrenia. Psychiatry Res. 2012, 200, 73–78. [Google Scholar] [CrossRef]
- Soundy, A.; Wampers, M.; Probst, M.; De Hert, M.; Stubbs, B.; Vancampfort, D.; Attux, C.; Leutwyler, H.; Ströhle, A. Physical activity and sedentary behaviour in outpatients with schizophrenia: A systematic review and meta-analysis. Int. J. Ther. Rehabil. 2013, 20, 588–595. [Google Scholar] [CrossRef]
- Lebiecka, Z.; Łopuszko, A.; Rudkowski, K.; Dańczura, E. Effects of physical activity on treatmentof schizophrenia. Arch. Psychiatry Psychother. 2019, 21, 28–35. [Google Scholar] [CrossRef]
- Shimada, T.; Ito, S.; Makabe, A.; Yamanushi, A.; Takenaka, A.; Kawano, K.; Kobayashi, M. Aerobic exercise and cognitive functioning in schizophrenia: An updated systematic review and meta-analysis. Psychiatry Res. 2022, 314, 114656. [Google Scholar] [CrossRef]
- Girdler, S.J.; Confino, J.E.; Woesner, M.E. Exercise as a Treatment for Schizophrenia: A Review. Psychopharmacol. Bull. 2019, 49, 56–69. [Google Scholar]
- Laursen, T.M.; Nordentoft, M.; Mortensen, P.B. Excess Early Mortality in Schizophrenia. Annu. Rev. Clin. Psychol. 2014, 10, 425–448. [Google Scholar] [CrossRef]
- Hjorthøj, C.; Stürup, A.E.; McGrath, J.J.; Nordentoft, M. Years of potential life lost and life expectancy in schizophrenia: A systematic review and meta-analysis. Lancet Psychiatry 2017, 4, 295–301. [Google Scholar] [CrossRef]
- Laursen, T.M. Life expectancy among persons with schizophrenia or bipolar affective disorder. Schizophr. Res. 2011, 131, 101–104. [Google Scholar] [CrossRef]
- World Health Organization. Programme on Mental Health: WHOQOL User Manual; World Health Organization: Geneva, Switzerland, 2023; Available online: https://apps.who.int/iris/handle/10665/77932 (accessed on 16 May 2023).
- Galuppi, A.; Turola, M.C.; Nanni, M.G.; Mazzoni, P.; Grassi, L. Schizophrenia and quality of life: How important are symptoms and functioning? Int. J. Ment. Health Syst. 2010, 4, 31. [Google Scholar] [CrossRef]
- Acil, A.A.; Dogan, S.; Dogan, O. The effects of physical exercises to mental state and quality of life in patients with schizophrenia. J. Psychiatr. Ment. Health Nurs. 2008, 15, 808–815. [Google Scholar] [CrossRef]
- Stępnicki, P.; Kondej, M.; Kaczor, A.A. Current Concepts and Treatments of Schizophrenia. Molecules 2018, 23, 2087. [Google Scholar] [CrossRef]
- Patel, K.R.; Cherian, J.; Gohil, K.; Atkinson, D. Schizophrenia: Overview and treatment options. Pharm. Ther. 2014, 39, 638–645. [Google Scholar]
- Tandon, R.; Lenderking, W.R.; Weiss, C.; Shalhoub, H.; Barbosa, C.D.; Chen, J.; Greene, M.; Meehan, S.R.; Duvold, L.B.; Arango, C.; et al. The impact on functioning of second-generation antipsychotic medication side effects for patients with schizophrenia: A worldwide, cross-sectional, web-based survey. Ann. Gen. Psychiatry 2020, 19, 42. [Google Scholar] [CrossRef]
- Hansford, H.J.; A Wewege, M.; Cashin, A.G.; Hagstrom, A.D.; Clifford, B.K.; McAuley, J.H.; Jones, M.D. If exercise is medicine, why don’t we know the dose? An overview of systematic reviews assessing reporting quality of exercise interventions in health and disease. Br. J. Sports Med. 2022, 56, 692–700. [Google Scholar] [CrossRef]
- Bayles, M.P.; Swank, A.M. General Principles of Exercise Prescription. In ACSM’s Exercise Testing and Prescription; American College of Sports Medicine; Wolters Kluwer: Philadelphia, PA, USA, 2018; pp. 126–141. [Google Scholar]
- Sabe, M.; Kaiser, S.; Sentissi, O. Physical exercise for negative symptoms of schizophrenia: Systematic review of randomized controlled trials and meta-analysis. Gen. Hosp. Psychiatry 2020, 62, 13–20. [Google Scholar] [CrossRef]
- Martin, H.; Beard, S.; Clissold, N.; Andraos, K.; Currey, L. Combined aerobic and resistance exercise interventions for individuals with schizophrenia: A systematic review. Ment. Health Phys. Act. 2017, 12, 147–155. [Google Scholar] [CrossRef]
- Firth, J.; Cotter, J.; Elliott, R.; French, P.; Yung, A.R. A systematic review and meta-analysis of exercise interventions in schizophrenia patients. Psychol. Med. 2015, 45, 1343–1361. [Google Scholar] [CrossRef]
- Bredin, S.S.D.; Kaufman, K.L.; Chow, M.I.; Lang, D.J.; Wu, N.; Kim, D.D.; Warburton, D.E.R. Effects of Aerobic, Resistance, and Combined Exercise Training on Psychiatric Symptom Severity and Related Health Measures in Adults Living with Schizophrenia: A Systematic Review and Meta-Analysis. Front. Cardiovasc. Med. 2022, 8, 753117. [Google Scholar] [CrossRef]
- Yu, Q.; Wong, K.-K.; Lei, O.-K.; Nie, J.; Shi, Q.; Zou, L.; Kong, Z. Comparative Effectiveness of Multiple Exercise Interventions in the Treatment of Mental Health Disorders: A Systematic Review and Network Meta-Analysis. Sports Med. Open 2022, 8, 135. [Google Scholar] [CrossRef]
- Dauwan, M.; Begemann, M.J.H.; Heringa, S.M.; Sommer, I.E. Exercise Improves Clinical Symptoms, Quality of Life, Global Functioning, and Depression in Schizophrenia: A Systematic Review and Meta-analysis. Schizophr. Bull. 2016, 42, 588–599. [Google Scholar] [CrossRef]
- Cella, M.; Roberts, S.; Pillny, M.; Riehle, M.; O’Donoghue, B.; Lyne, J.; Tomlin, P.; Valmaggia, L.; Preti, A. Psychosocial and behavioural interventions for the negative symptoms of schizophrenia: A systematic review of efficacy meta-analyses. Br. J. Psychiatry 2023, 223, 321–331. [Google Scholar] [CrossRef]
- Gallardo-Gómez, D.; Noetel, M.; Álvarez-Barbosa, F.; Alfonso-Rosa, R.M.; Ramos-Munell, J.; Cruz, B.d.P.; del Pozo-Cruz, J. Exercise to treat psychopathology and other clinical outcomes in schizophrenia: A systematic review and meta-analysis. Eur. Psychiatry 2023, 66, e40. [Google Scholar] [CrossRef]
- Korman, N.; Stanton, R.; Vecchio, A.; Chapman, J.; Parker, S.; Martland, R.; Siskind, D.; Firth, J. The effect of exercise on global, social, daily living and occupational functioning in people living with schizophrenia: A systematic review and meta-analysis. Schizophr. Res. 2023, 256, 98–111. [Google Scholar] [CrossRef]
- Oliva, H.N.; Monteiro-Junior, R.S.; Oliva, I.O.; Powers, A.R. Effects of exercise intervention on psychotic symptoms: A meta-analysis and hypothetical model of neurobiological mechanisms. Prog. Neuro-Psychopharmacol. Biol. Psychiatry 2023, 125, 110771. [Google Scholar] [CrossRef]
- Tavares, V.D.d.O.; Rossell, S.L.; Schuch, F.B.; Herring, M.; de Sousa, G.M.; Galvão-Coelho, N.L.; Hallgren, M. Effects of exercise on cognitive functioning in adults with serious mental illness: A meta analytic review. Psychiatry Res. 2023, 321, 115081. [Google Scholar] [CrossRef]
- Tricco, A.C.; Lillie, E.; Zarin, W.; O’brien, K.; Colquhoun, H.; Kastner, M.; Levac, D.; Ng, C.; Sharpe, J.P.; Wilson, K.; et al. A scoping review on the conduct and reporting of scoping reviews. BMC Med. Res Methodol. 2016, 16, 15. [Google Scholar] [CrossRef]
- Zotero [Software], Version 6.0.26; Corporation for Digital Scholarship: Vienna, VA, USA, 2023. Available online: https://www.zotero.org/(accessed on 5 April 2022).
- Ouzzani, M.; Hammady, H.; Fedorowicz, Z.; Elmagarmid, A. Rayyan—A web and mobile app for systematic reviews. Syst. Rev. 2016, 5, 210. [Google Scholar] [CrossRef]
- Sterne, J.A.C.; Savović, J.; Page, M.J.; Elbers, R.G.; Blencowe, N.S.; Boutron, I.; Cates, C.J.; Cheng, H.Y.; Corbett, M.S.; Eldridge, S.M.; et al. RoB 2: A revised tool for assessing risk of bias in randomised trials. BMJ 2019, 366, l4898. [Google Scholar] [CrossRef]
- Silva, B.A.; Cassilhas, R.C.; Attux, C.; Cordeiro, Q.; Gadelha, A.L.; Telles, B.A.; Bressan, R.A.; Ferreira, F.N.; Rodstein, P.H.; Daltio, C.S.; et al. A 20-week program of resistance or concurrent exercise improves symptoms of schizophrenia: Results of a blind, randomized controlled trial. Rev. Bras. Psiquiatr. 2015, 37, 271–279. [Google Scholar] [CrossRef]
- Lo, L.L.H.; Lee, E.H.M.; Hui, C.L.M.; Chong, C.S.Y.; Chang, W.C.; Chan, S.K.W.; Lin, J.J.; Lo, W.T.L.; Chen, E.Y.H. Effect of high-endurance exercise intervention on sleep-dependent procedural memory consolidation in individuals with schizophrenia: A randomized controlled trial. Psychol. Med. 2021, 53, 1708–1720. [Google Scholar] [CrossRef]
- Kern, R.S.; Reddy, L.F.; Cohen, A.N.; Young, A.S.; Green, M.F. Effects of aerobic exercise on cardiorespiratory fitness and social functioning in veterans 40 to 65 years old with schizophrenia. Psychiatry Res. 2020, 291, 113258. [Google Scholar] [CrossRef]
- Huang, Y.-C.; Hung, C.-F.; Hsu, S.-T.; Lin, P.-Y.; Lee, Y.; Chong, M.-Y.; Chen, C.-C.; Kuo, Y.-H.; Wang, L.-J. Effects of aerobic walking on cognitive function in patients with schizophrenia: A randomized controlled trial. J. Psychiatr. Res. 2021, 134, 173–180. [Google Scholar] [CrossRef]
- Kimhy, D.; Tay, C.; Vakhrusheva, J.; Beck-Felts, K.; Ospina, L.H.; Ifrah, C.; Parvaz, M.; Gross, J.J.; Bartels, M.N. Enhancement of aerobic fitness improves social functioning in individuals with schizophrenia. Eur. Arch. Psychiatry Clin. Neurosci. 2021, 271, 367–376. [Google Scholar] [CrossRef]
- Marzolini, S.; Jensen, B.; Melville, P. Feasibility and effects of a group-based resistance and aerobic exercise program for individuals with severe schizophrenia: A multidisciplinary approach. Ment. Health Phys. Act. 2009, 2, 29–36. [Google Scholar] [CrossRef]
- Ryu, J.; Jung, J.H.; Kim, J.; Kim, C.-H.; Lee, H.-B.; Kim, D.-H.; Lee, S.-K.; Shin, J.-H.; Roh, D. Outdoor cycling improves clinical symptoms, cognition and objectively measured physical activity in patients with schizophrenia: A randomized controlled trial. J. Psychiatr. Res. 2020, 120, 144–153. [Google Scholar] [CrossRef]
- Battaglia, G.; Alesi, M.; Inguglia, M.; Roccella, M.; Caramazza, G.; Bellafiore, M.; Palma, A. Soccer practice as an add-on treatment in the management of individuals with a diagnosis of schizophrenia. Neuropsychiatr. Dis. Treat. 2013, 9, 595–603. [Google Scholar] [CrossRef]
- Nygård, M.; Brobakken, M.F.; Taylor, J.L.; Reitan, S.K.; Güzey, I.C.; Morken, G.; Lydersen, S.; Vedul-Kjelsås, E.; Wang, E.; Heggelund, J. Strength training restores force-generating capacity in patients with schizophrenia. Scand. J. Med. Sci. Sports 2021, 31, 665–678. [Google Scholar] [CrossRef]
- Massa, N.; Alrohaibani, A.; Mammino, K.; Bello, M.; Taylor, N.; Cuthbert, B.; Fargotstein, M.; Coulter, M.M.; Boatright, J.H.; Nocera, J.; et al. The Effect of Aerobic Exercise on Physical and Cognitive Outcomes in a Small Cohort of Outpatients with Schizophrenia. Brain Plast. 2020, 5, 161–174. [Google Scholar] [CrossRef]
- Su, C.-Y.; Wang, P.-W.; Lin, Y.-J.; Tang, T.-C.; Liu, M.-F.; Chen, M.-D. The effects of aerobic exercise on cognition in schizophrenia: A 3-month follow-up study. Psychiatry Res. 2016, 244, 394–402. [Google Scholar] [CrossRef]
- Kimhy, D.; Vakhrusheva, J.; Bartels, M.N.; Armstrong, H.F.; Ballon, J.S.; Khan, S.; Chang, R.W.; Hansen, M.C.; Ayanruoh, L.; Lister, A.; et al. The Impact of Aerobic Exercise on Brain-Derived Neurotrophic Factor and Neurocognition in Individuals With Schizophrenia: A Single-Blind, Randomized Clinical Trial. Schizophr. Bull. 2015, 41, 859–868. [Google Scholar] [CrossRef]
- Nygård, M.; Brobakken, M.F.; Lydersen, S.; Güzey, I.C.; Morken, G.; Heggelund, J.; Wang, E. Strength training integrated in long term collaborative care of patients with schizophrenia. Schizophr. Res. 2023, 260, 67–75. [Google Scholar] [CrossRef]
- Kim, M.; Jeon, J. The effect of exercise on physical and mental health for adults with schizophrenia: A review of clinical aerobic exercise. Ethiop. J. Health Dev. 2020, 34, 35–43. [Google Scholar]
- Firth, J.; Stubbs, B.; Rosenbaum, S.; Vancampfort, D.; Malchow, B.; Schuch, F.; Elliott, R.; Nuechterlein, K.H.; Yung, A.R. Aerobic Exercise Improves Cognitive Functioning in People with Schizophrenia: A Systematic Review and Meta-Analysis. Schizophr. Bull. 2016, 43, 546–556. [Google Scholar] [CrossRef]
- Stanton, R.; Happell, B. A systematic review of the aerobic exercise program variables for people with schizophrenia. Curr. Sports Med. Rep. 2014, 13, 260–266. [Google Scholar] [CrossRef]
- Heggelund, J.; Morken, G.; Helgerud, J.; E Nilsberg, G.; Hoff, J. Therapeutic effects of maximal strength training on walking efficiency in patients with schizophrenia—A pilot study. BMC Res. Notes 2012, 5, 344. [Google Scholar] [CrossRef]
- Maurus, I.; Mantel, C.; Keller-Varady, K.; Schmitt, A.; Lembeck, M.; Röh, A.; Papazova, I.; Falkai, P.; Schneider-Axmann, T.; Hasan, A.; et al. Resistance training in patients with schizophrenia: Concept and proof of principle trial. J. Psychiatr. Res. 2020, 120, 72–82. [Google Scholar] [CrossRef]
- Westcott, W.L. Resistance Training is Medicine: Effects of Strength Training on Health. Curr. Sports Med. Rep. 2012, 11, 209–216. [Google Scholar] [CrossRef]
- Maestroni, L.; Read, P.; Bishop, C.; Papadopoulos, K.; Suchomel, T.J.; Comfort, P.; Turner, A. The Benefits of Strength Training on Musculoskeletal System Health: Practical Applications for Interdisciplinary Care. Sports Med. 2020, 50, 1431–1450. [Google Scholar] [CrossRef]
- Rastad, C.; Martin, C.; Åsenlöf, P. Barriers, Benefits, and Strategies for Physical Activity in Patients with Schizophrenia. Phys. Ther. 2014, 94, 1467–1479. [Google Scholar] [CrossRef]
- Gross, J.; Vancampfort, D.; Stubbs, B.; Gorczynski, P.; Soundy, A. A narrative synthesis investigating the use and value of social support to promote physical activity among individuals with schizophrenia. Disabil. Rehabil. 2016, 38, 123–150. [Google Scholar] [CrossRef]
- Arnautovska, U.; Kesby, J.P.; Korman, N.; Rebar, A.L.; Chapman, J.; Warren, N.; Rossell, S.L.; Dark, F.L.; Siskind, D. Biopsychology of Physical Activity in People with Schizophrenia: An Integrative Perspective on Barriers and Intervention Strategies. Neuropsychiatr. Dis. Treat. 2022, 18, 2917–2926. [Google Scholar] [CrossRef]
- Wang, P.-W.; Lin, H.-C.; Su, C.-Y.; Chen, M.-D.; Lin, K.C.; Ko, C.-H.; Yen, C.-F. Effect of Aerobic Exercise on Improving Symptoms of Individuals with Schizophrenia: A Single Blinded Randomized Control Study. Front. Psychiatry 2018, 9, 167. [Google Scholar] [CrossRef]
- Curcic, D.; Lazarevic, B.C.; Stojmenovic, T.; Djukic-Dejanovic, S.; Dikic, N.; Vesic-Vukasinovic, M.; Radivojevic, N.; Andjelkovic, M.; Borovcanin, M.; Djokic, G. Positive impact of prescribed physical activity on symptoms of schizophrenia: Randomized clinical trial. Psychiatr. Danub. 2017, 29, 459–465. [Google Scholar] [CrossRef]
- Loh, S.Y.; Abdullah, A.; Abu Bakar, A.K.; Thambu, M.; Jaafar, N.R.N. Structured Walking and Chronic Institutionalized Schizophrenia Inmates: A pilot RCT Study on Quality of Life. Glob. J. Health Sci. 2015, 8, p238–p248. [Google Scholar] [CrossRef]
- Pelham, T.W.; Campagna, P.D.; Ritvo, P.G.; Birnie, W.A. The effects of exercise therapy on clients in a psychiatric rehabilitation program. Psychosoc. Rehabil. J. 1993, 16, 75–84. [Google Scholar] [CrossRef]
- Ho, R.T.; Fong, T.C.; Wan, A.H.; Au-Yeung, F.S.; Wong, C.P.; Ng, W.Y.; Cheung, I.K.; Lo, P.H.; Ng, S.; Chan, C.L.; et al. A randomized controlled trial on the psychophysiological effects of physical exercise and Tai-chi in patients with chronic schizophrenia. Schizophr. Res. 2016, 171, 42–49. [Google Scholar] [CrossRef]
- Schmitt, A.; Maurus, I.; Rossner, M.J.; Röh, A.; Lembeck, M.; von Wilmsdorff, M.; Takahashi, S.; Rauchmann, B.; Keeser, D.; Hasan, A.; et al. Effects of Aerobic Exercise on Metabolic Syndrome, Cardiorespiratory Fitness, and Symptoms in Schizophrenia Include Decreased Mortality. Front. Psychiatry 2018, 9, 690. [Google Scholar] [CrossRef]
- Ashdown-Franks, G.; Firth, J.; Carney, R.; Carvalho, A.F.; Hallgren, M.; Koyanagi, A.; Rosenbaum, S.; Schuch, F.B.; Smith, L.; Solmi, M.; et al. Exercise as Medicine for Mental and Substance Use Disorders: A Meta-review of the Benefits for Neuropsychiatric and Cognitive Outcomes. Sports Med. 2020, 50, 151–170. [Google Scholar] [CrossRef]
- Gallardo-Gómez, D.; del Pozo-Cruz, J.; Noetel, M.; Álvarez-Barbosa, F.; Alfonso-Rosa, R.M.; Cruz, B.d.P. Optimal dose and type of exercise to improve cognitive function in older adults: A systematic review and bayesian model-based network meta-analysis of RCTs. Ageing Res. Rev. 2022, 76, 101591. [Google Scholar] [CrossRef]
- Papadea, D.; Dalla, C.; Tata, D.A. Exploring a Possible Interplay between Schizophrenia, Oxytocin, and Estrogens: A Narrative Review. Brain Sci. 2023, 13, 461. [Google Scholar] [CrossRef]
- Bhatia, T.; Mazumdar, S.; Wood, J.; He, F.; Gur, R.E.; Gur, R.C.; Nimgaonkar, V.L.; Deshpande, S.N. A randomised controlled trial of adjunctive yoga and adjunctive physical exercise training for cognitive dysfunction in schizophrenia. Acta Neuropsychiatr. 2016, 29, 102–114. [Google Scholar] [CrossRef]
- Nasution, N.M.; Effendy, E.; Amin, M.M.; Siregar, I.R. Effect of Aerobic Exercise in Positive and Negative Symptoms in Schizophrenia. Open Access Maced. J. Med. Sci. 2021, 9, 178–181. [Google Scholar] [CrossRef]
- Malchow, B.; Keeser, D.; Keller, K.; Hasan, A.; Rauchmann, B.-S.; Kimura, H.; Schneider-Axmann, T.; Dechent, P.; Gruber, O.; Ertl-Wagner, B.; et al. Effects of endurance training on brain structures in chronic schizophrenia patients and healthy controls. Schizophr. Res. 2016, 173, 182–191. [Google Scholar] [CrossRef]
- Chen, M.-D.; Kuo, Y.-H.; Chang, Y.-C.; Hsu, S.-T.; Kuo, C.-C.; Chang, J.-J. Influences of Aerobic Dance on Cognitive Performance in Adults with Schizophrenia. Occup. Ther. Int. 2016, 23, 346–356. [Google Scholar] [CrossRef]
- Sisman, F.N.; Büber, B.; Taş, F.; Turan, H. Randomized Controlled Trial for the Effects of an Exercise Program for Functional Remission and Weight Control in Schizophrenia: A Community Mental Health Study. Issues Ment. Health Nurs. 2022, 43, 603–612. [Google Scholar] [CrossRef]
- Le, T.P.; Ventura, J.; Ruiz-Yu, B.; McEwen, S.C.; Subotnik, K.L.; Nuechterlein, K.H. Treatment engagement in first-episode schizophrenia: Associations between intrinsic motivation and attendance during cognitive training and an aerobic exercise program. Schizophr. Res. 2023, 251, 59–65. [Google Scholar] [CrossRef]
- Nuechterlein, K.H.; McEwen, S.C.; Ventura, J.; Subotnik, K.L.; Turner, L.R.; Boucher, M.; Casaus, L.R.; Distler, M.G.; Hayata, J.N. Aerobic exercise enhances cognitive training effects in first-episode schizophrenia: Randomized clinical trial demonstrates cognitive and functional gains. Psychol. Med. 2022, 53, 4751–4761. [Google Scholar] [CrossRef]
- Ventura, J.; McEwen, S.; Subotnik, K.L.; Hellemann, G.S.; Ghadiali, M.; Rahimdel, A.; Seo, M.J.; Irwin, M.R.; Nuechterlein, K.H. Changes in inflammation are related to depression and amount of aerobic exercise in first episode schizophrenia. Early Interv. Psychiatry 2021, 15, 213–216. [Google Scholar] [CrossRef]
- Nuechterlein, K.H.; Ventura, J.; McEwen, S.C.; Gretchen-Doorly, D.; Vinogradov, S.; Subotnik, K.L. Enhancing Cognitive Training Through Aerobic Exercise After a First Schizophrenia Episode: Theoretical Conception and Pilot Study. Schizophr. Bull. 2016, 42 (Suppl. S1), S44–S52. [Google Scholar] [CrossRef]
- Bang-Kittilsen, G.; Egeland, J.; Holmen, T.L.; Bigseth, T.T.; Andersen, E.; Mordal, J.; Ulleberg, P.; Engh, J.A. High-intensity interval training and active video gaming improve neurocognition in schizophrenia: A randomized controlled trial. Eur. Arch. Psychiatry Clin. Neurosci. 2020, 271, 339–353. [Google Scholar] [CrossRef]
- Cristiano, V.B.; Szortyka, M.F.; Belmonte-De-Abreu, P. A controlled open clinical trial of the positive effect of a physical intervention on quality of life in schizophrenia. Front. Psychiatry 2023, 14, 1066541. [Google Scholar] [CrossRef]
- Arietaleanizbeaskoa, M.S.; on behalf of the EfiKroniK group; Sancho, A.; Olazabal, I.; Moreno, C.; Gil, E.; Garcia-Alvarez, A.; Mendizabal, N.; de la Fuente, I.; Dominguez, S.; et al. Effectiveness of physical exercise for people with chronic diseases: The EFIKRONIK study protocol for a hybrid, clinical and implementation randomized trial. BMC Fam. Pract. 2020, 21, 227. [Google Scholar] [CrossRef]
- Nyboe, L.; Moeller, M.K.; Vestergaard, C.H.; Lund, H.; Videbech, P. Physical activity and anomalous bodily experiences in patients with first-episode schizophrenia. Nord. J. Psychiatry 2016, 70, 514–520. [Google Scholar] [CrossRef]
- Shimada, T.; Ito, S.; Makabe, A.; Yamanushi, A.; Takenaka, A.; Kobayashi, M. Aerobic exercise and cognitive functioning in schizophrenia: A pilot randomized controlled trial. Psychiatry Res. 2019, 282, 112638. [Google Scholar] [CrossRef]
- Shimada, T.; Ito, S.; Makabe, A.; Yamanushi, A.; Takenaka, A.; Kawano, K.; Kobayashi, M. Aerobic exercise and cognitive functioning in schizophrenia: Results of a 1-year follow-up from a randomized controlled trial. Psychiatry Res. 2020, 286, 112854. [Google Scholar] [CrossRef]
- Khonsari, N.M.; Badrfam, R.; Mohammdi, M.R.; Rastad, H.; Etemadi, F.; Vafaei, Z.; Zandifar, A. Effect of Aerobic Exercise as Adjunct Therapy on the Improvement of Negative Symptoms and Cognitive Impairment in Patients with Schizophrenia: A Randomized, Case-Control Clinical Trial. J. Psychosoc. Nurs. Ment. Health Serv. 2022, 60, 38–43. [Google Scholar] [CrossRef]
- Şenormancı, G.; Korkmaz, N.; Şenormancı, Ö.; Uğur, S.; Topsaç, M.; Gültekin, O. Effects of Exercise on Resilience, Insight and Functionality in Patients with Chronic Schizophrenia in a Psychiatric Nursing Home Setting: A Randomized Controlled Trial. Issues Ment. Health Nurs. 2021, 42, 690–698. [Google Scholar] [CrossRef]
- Heggelund, J.; Nilsberg, G.E.; Hoff, J.; Morken, G.; Helgerud, J. Effects of high aerobic intensity training in patients with schizophrenia—A controlled trial. Nord. J. Psychiatry 2011, 65, 269–275. [Google Scholar] [CrossRef]
- Maggouritsa, G.; Kokaridas, D.; Theodorakis, I.; Patsiaouras, A.; Mouzas, O.; Dimitrakopoulos, S.; Diggelidis, N. The effect of a physical activity programme on improving mood profile of patients with schizophrenia. Int. J. Sport Exerc. Psychol. 2014, 12, 273–284. [Google Scholar] [CrossRef]
- Areshtanab, H.N.; Ebrahimi, H.; Abdi, M.; Mohammadian, R.; Asl, A.M.; Piri, S. The Effect of Aerobic Exercise on the Quality of Life of Male Patients Who Suffer from Chronic Schizophrenia: Double-Blind, Randomized Control Trial. Iran. J. Psychiatry Behav. Sci. 2020, 14, 529–535. [Google Scholar] [CrossRef]
- Areshtanab, H.; Ebrahimi, H.; Farnam, A.; Mohammadpoorasl, A.; Jamali, B.; Piri, S. The effect of regular aerobic exercise on both positive and negative symptoms of male patients with chronic Schizophrenia: A double blinded study. Int. J. Med. Res. Health Sci. 2016, 5, 529–535. [Google Scholar]
- Ho, R.T.H.; Wan, A.H.Y.; Au-Yeung, F.S.W.; Lo, P.H.Y.; Siu, P.J.C.Y.; Wong, C.P.K.; Ng, W.Y.H.; Cheung, I.K.M.; Ng, S.M.; Chan, C.L.W.; et al. The psychophysiological effects of Tai-chi and exercise in residential schizophrenic patients: A 3-arm randomized controlled trial. BMC Complement. Altern. Med. 2014, 14, 364. [Google Scholar] [CrossRef]
- Mullor, D.; Gallego, J.; Cangas, A.; Aguilar-Parra, J.; Trigueros, R.; Lopez-Pardo, A. Psychological and social impact of an inclusive sports program among students and people with severe mental disorder. Rev. Psicol. Deporte 2020, 29, 8–15. [Google Scholar]
- Hasson-Ohayon, I.; Kravetz, S.; Roe, D.; Rozencwaig, S.; Weiser, M. Qualitative assessment of verbal and non-verbal psychosocial interventions for people with severe mental illness. J. Ment. Health 2006, 15, 343–353. [Google Scholar] [CrossRef]
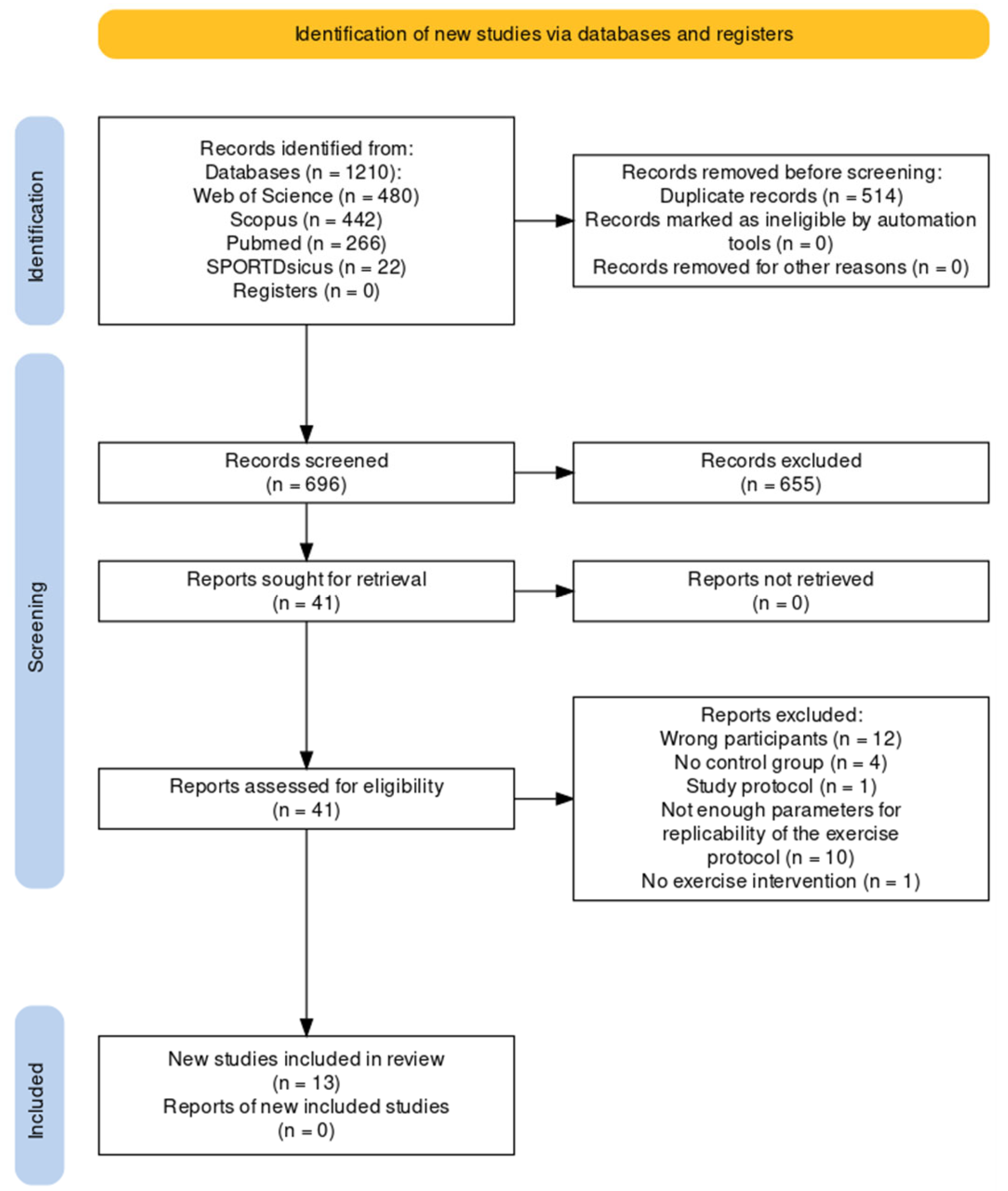
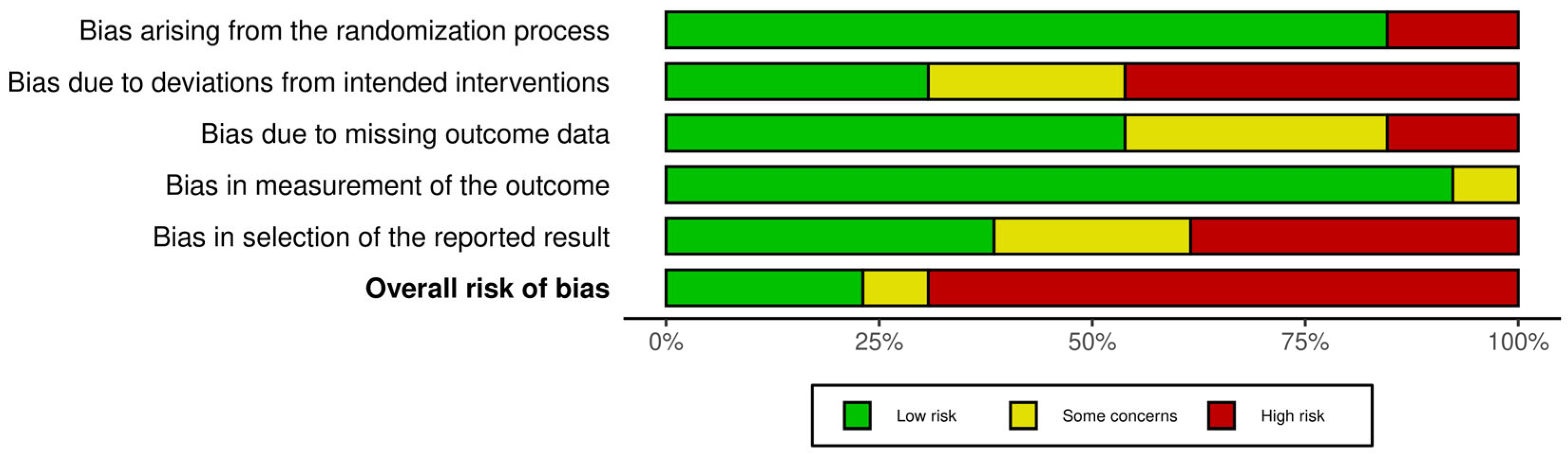
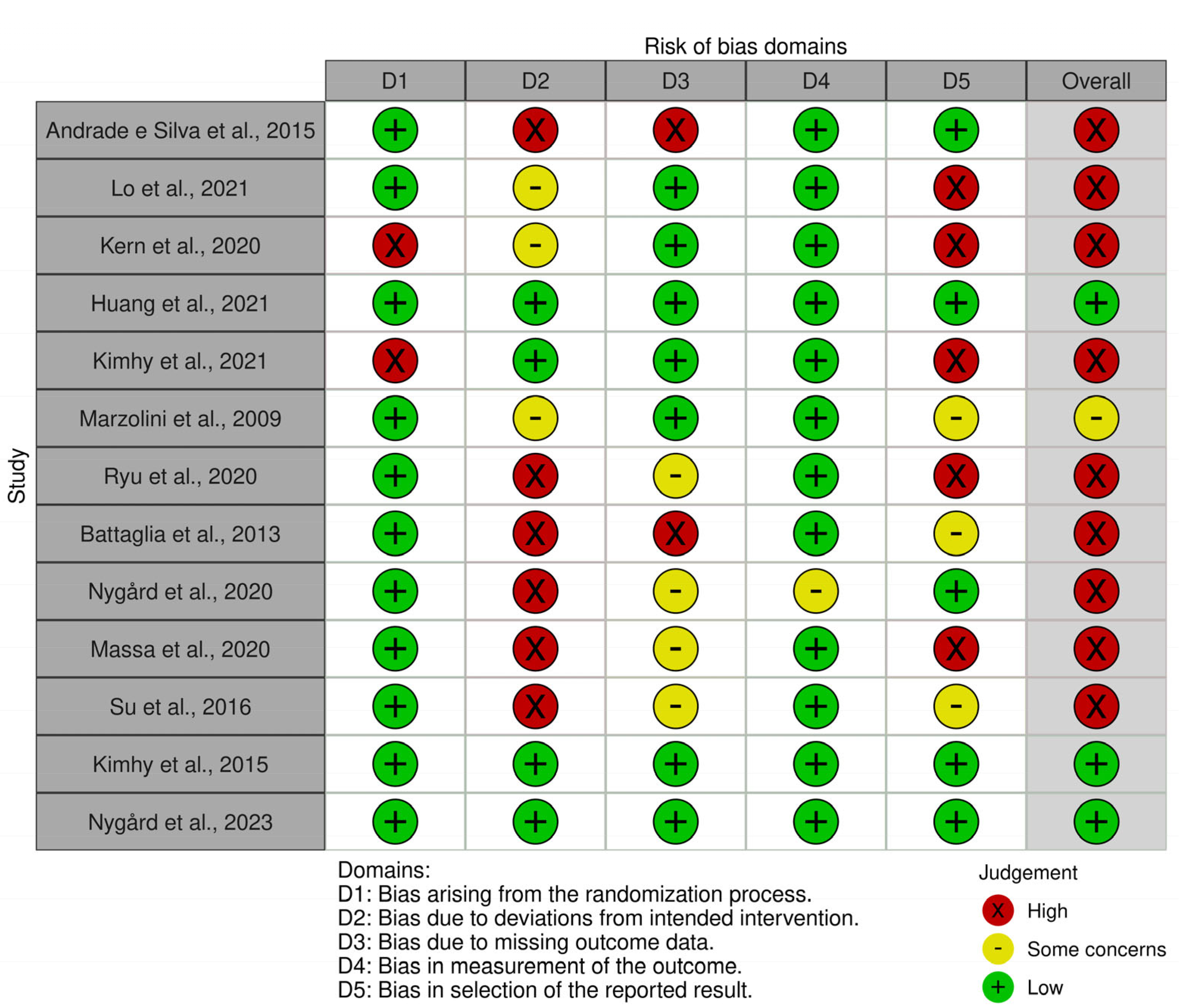
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).