
Validation of the Cognitive Reserve Index Questionnaire (CRIq) in Arabic

Abstract
:1. Introduction
2. Materials and Methods
2.1. Sample
2.2. Procedure and Data Collection
2.3. Statistical Analysis
3. Results
3.1. Participants
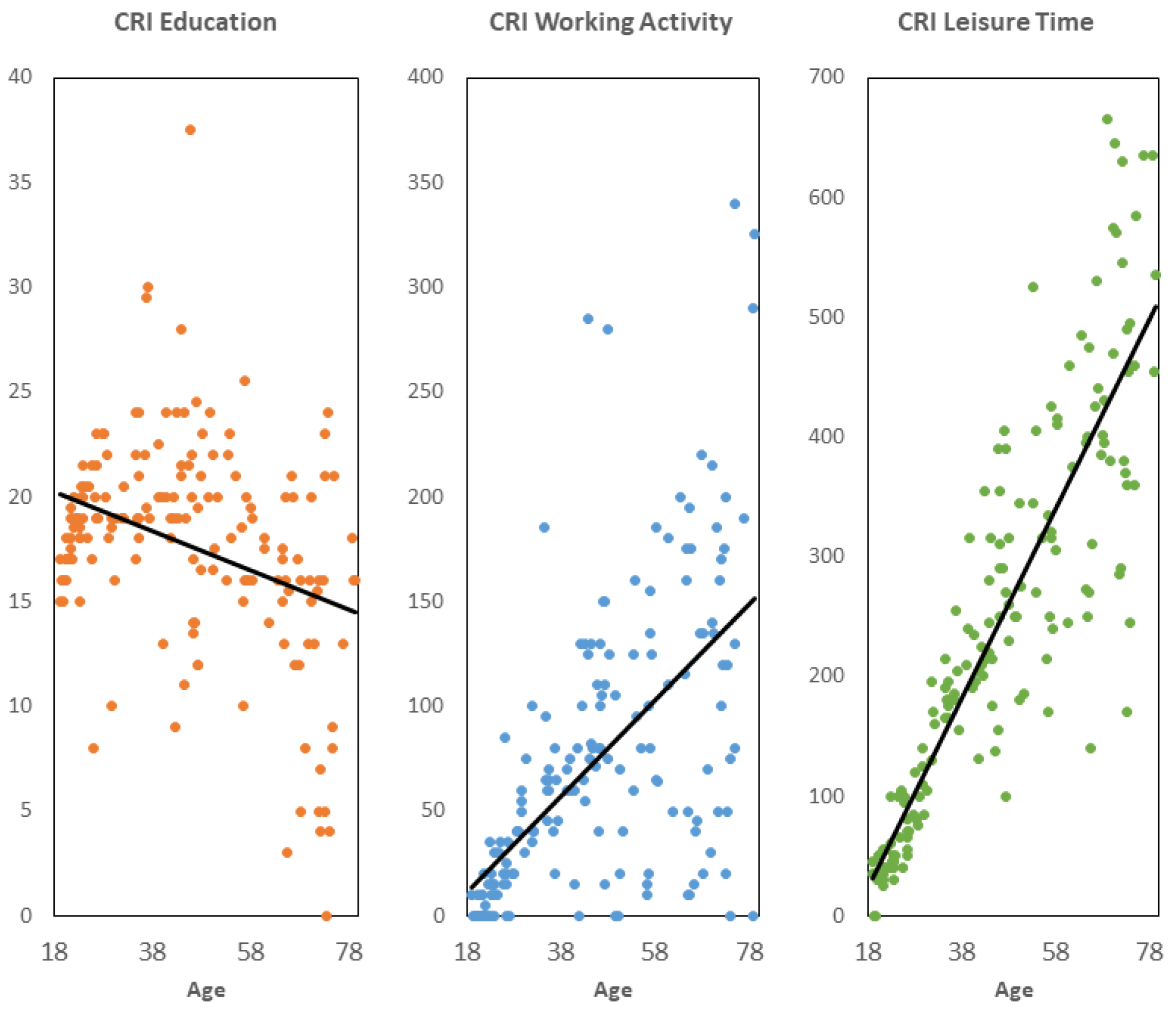
3.2. CRIq-Arabic Descriptions and Computations
3.3. Internal Consistency
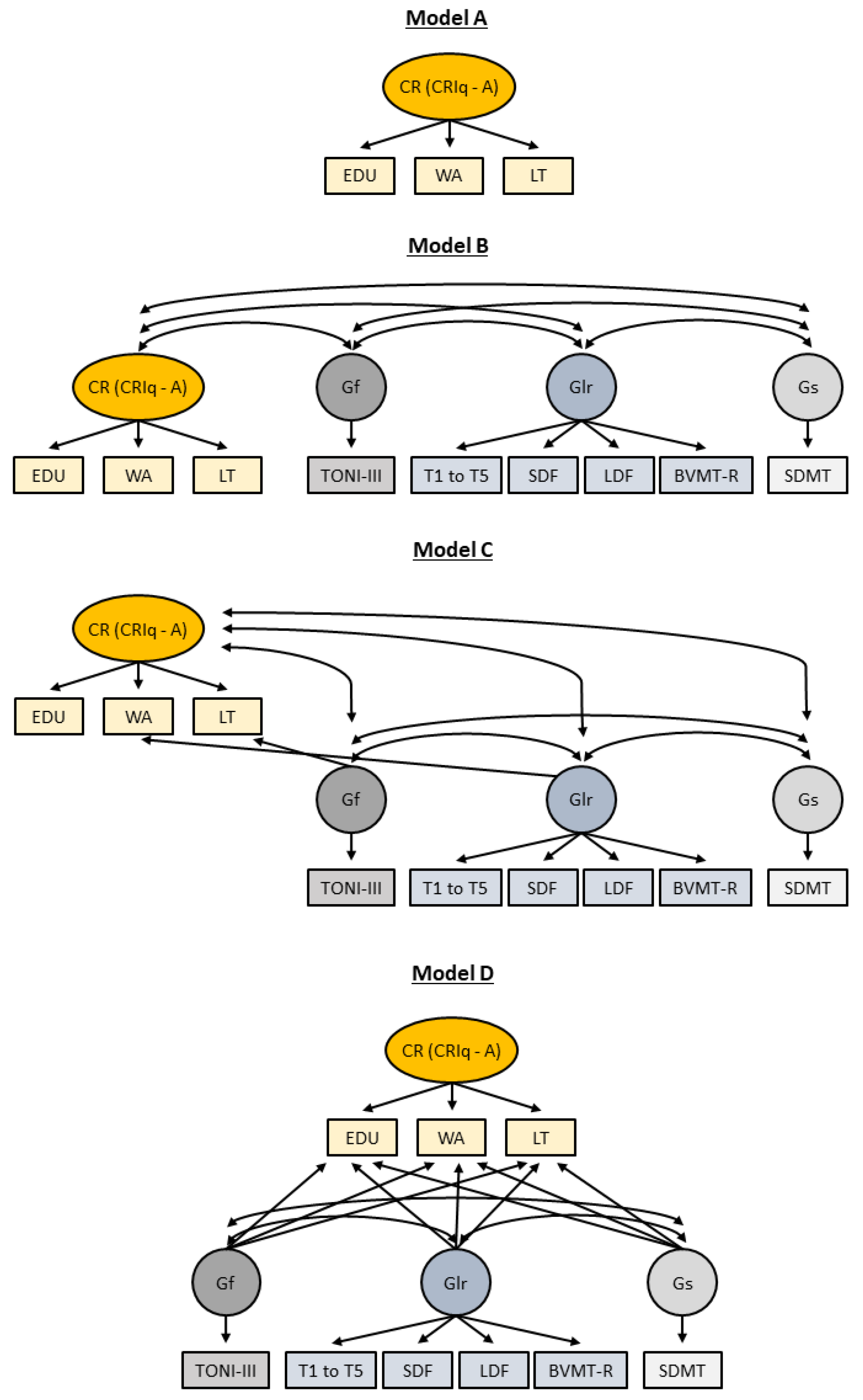
3.4. Construct Validity
4. Discussion
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Stern, Y. Cognitive reserve in ageing and Alzheimer’s disease. Lancet Neurol. 2012, 11, 1006–1012. [Google Scholar] [CrossRef] [PubMed]
- Cosentino, S.; Stern, Y. Consideration of cognitive reserve. In Handbook on the Neuropsychology of Aging and Dementia; Springer Nature: Cham, Switzerland, 2019; pp. 11–23. [Google Scholar]
- Stern, Y.; Arenaza-Urquijo, E.M.; Bartrés-Faz, D.; Belleville, S.; Cantilon, M.; Chetelat, G.; Ewers, M.; Franzmeier, N.; Kempermann, G.; Kremen, W.S.; et al. Whitepaper: Defining and investigating cognitive reserve, brain reserve, and brain maintenance. Alzheimer’s Dement. 2020, 16, 1305–1311. [Google Scholar] [CrossRef]
- Chapko, D.; McCormack, R.; Black, C.; Staff, R.; Murray, A. Life-course determinants of cognitive reserve (CR) in cognitive aging and dementia—A systematic literature review. Aging Ment. Health 2018, 22, 921–932. [Google Scholar] [CrossRef]
- Opdebeeck, C.; Martyr, A.; Clare, L. Cognitive reserve and cognitive function in healthy older people: A meta-analysis. Aging Neuropsychol. Cogn. 2016, 23, 40–60. [Google Scholar] [CrossRef] [PubMed]
- van Loenhoud, A.; Habeck, C.; van der Flier, W.; Ossenkoppele, R.; Stern, Y. Identifying a task-invariant cognitive reserve network using task potency. NeuroImage 2020, 210, 116593. [Google Scholar] [CrossRef] [PubMed]
- Menardi, A.; Pascual-Leone, A.; Fried, P.J.; Santarnecchi, E. The Role of Cognitive Reserve in Alzheimer’s Disease and Aging: A Multi-Modal Imaging Review. J. Alzheimer’s Dis. 2018, 66, 1341–1362. [Google Scholar] [CrossRef]
- Santangelo, G.; Altieri, M.; Enzinger, C.; Gallo, A.; Trojano, L. Cognitive reserve and neuropsychological performance in multiple sclerosis: A meta-analysis. Neuropsychology 2019, 33, 379–390. [Google Scholar] [CrossRef]
- Herrero, P.; Contador, I.; Stern, Y.; Fernandez-Calvo, B.; Sánchez, A.; Ramos, F. Influence of cognitive reserve in schizophrenia: A systematic review. Neurosci. Biobehav. Rev. 2020, 108, 149–159. [Google Scholar] [CrossRef]
- Hindle, J.V.; Martyr, A.; Clare, L. Cognitive reserve in Parkinson’s disease: A systematic review and meta-analysis. Park. Relat. Disord. 2014, 20, 1–7. [Google Scholar] [CrossRef]
- Migliore, S.; D’aurizio, G.; Scaricamazza, E.; Maffi, S.; Ceccarelli, C.; Ristori, G.; Romano, S.; Castaldo, A.; Fichera, M.; Curcio, G.; et al. Cognitive Reserve in Early Manifest Huntington Disease Patients: Leisure Time Is Associated with Lower Cognitive and Functional Impairment. J. Pers. Med. 2022, 12, 36. [Google Scholar] [CrossRef]
- Kaur, N.; Dendukuri, N.; Fellows, L.K.; Brouillette, M.-J.; Mayo, N. Association between cognitive reserve and cognitive performance in people with HIV: A systematic review and meta-analysis. AIDS Care 2019, 32, 1–11. [Google Scholar] [CrossRef]
- Lenehan, M.E.; Summers, M.J.; Saunders, N.L.; Summers, J.J.; Ward, D.D.; Ritchie, K.; Vickers, J.C. Sending your grandparents to university increases cognitive reserve: The Tasmanian Healthy Brain Project. Neuropsychology 2016, 30, 525–531. [Google Scholar] [CrossRef]
- Matyas, N.; Aschenberger, F.K.; Wagner, G.; Teufer, B.; Auer, S.; Gisinger, C.; Kil, M.; Klerings, I.; Gartlehner, G. Continuing education for the prevention of mild cognitive impairment and Alzheimer’s-type dementia: A systematic review and overview of systematic reviews. BMJ Open 2019, 9, e027719. [Google Scholar] [CrossRef]
- Mondini, S.; Madella, I.; Zangrossi, A.; Bigolin, A.; Tomasi, C.; Michieletto, M.; Villani, D.; Di Giovanni, G.; Mapelli, D. Cognitive Reserve in Dementia: Implications for Cognitive Training. Front. Aging Neurosci. 2016, 8, 84. [Google Scholar] [CrossRef]
- Jones, R.N.; Manly, J.; Glymour, M.M.; Rentz, D.M.; Jefferson, A.L.; Stern, Y. Conceptual and Measurement Challenges in Research on Cognitive Reserve. J. Int. Neuropsychol. Soc. 2011, 17, 593–601. [Google Scholar] [CrossRef]
- Nucci, M.; Mapelli, D.; Mondini, S. Cognitive Reserve Index questionnaire (CRIq): A new instrument for measuring cognitive reserve. Aging Clin. Exp. Res. 2012, 24, 218–226. [Google Scholar] [CrossRef]
- Leon, I.; Garcia-Garcia, J.; Roldan-Tapia, L. Development of the scale of cognitive reserve in Spanish population: A pilot study. Rev. Neurol. 2011, 52, 653–660. [Google Scholar]
- Maiovis, P.; Ioannidis, P.; Nucci, M.; Gotzamani-Psarrakou, A.; Karacostas, D. Adaptation of the Cognitive Reserve Index Questionnaire (CRIq) for the Greek population. Neurol. Sci. 2016, 37, 633–636. [Google Scholar] [CrossRef]
- Valenzuela, M.J.; Sachdev, P. Assessment of complex mental activity across the lifespan: Development of the Lifetime of Experiences Questionnaire (LEQ). Psychol. Med. 2007, 37, 1015–1025. [Google Scholar] [CrossRef]
- Reed, B.R.; Mungas, D.; Farias, S.T.; Harvey, D.; Beckett, L.; Widaman, K.; Hinton, L.; DeCarli, C. Measuring cognitive reserve based on the decomposition of episodic memory variance. Brain 2010, 133, 2196–2209. [Google Scholar] [CrossRef]
- Kartschmit, N.; Mikolajczyk, R.; Schubert, T.; Lacruz, M.E. Measuring Cognitive Reserve (CR)—A systematic review of measurement properties of CR questionnaires for the adult population. PLoS ONE 2019, 14, e0219851. [Google Scholar] [CrossRef]
- Rami, L.; Valls-Pedret, C.; Bartres-Faz, D.; Caprile, C.; Sole-Padulles, C.; Castellvi, M.; Olives, J.; Bosch, B.; Molinuevo, J.L. Cognitive reserve questionnaire. Scores obtained in a healthy elderly population and in one with Alzheimer’s disease. Rev. Neurol. 2011, 52, 195–201. [Google Scholar]
- Minogue, C.; Delbaere, K.; Radford, K.; Broe, T.; Forder, W.S.; Lah, S. Development and initial validation of the Retrospective Indigenous Childhood Enrichment scale (RICE). Int. Psychogeriatr. 2018, 30, 519–526. [Google Scholar] [CrossRef]
- Apolinario, D.; Brucki, S.M.D.; Ferretti, R.E.d.L.; Farfel, J.M.; Magaldi, R.M.; Busse, A.L.; Jacob-Filho, W. Estimating Premorbid Cognitive Abilities in Low-Educated Populations. PLoS ONE 2013, 8, e60084. [Google Scholar] [CrossRef]
- Amoretti, S.; Cabrera, B.; Torrent, C.; Bonnín, C.d.M.; Mezquida, G.; Garriga, M.; Jiménez, E.; Martínez-Arán, A.; Solé, B.; Reinares, M.; et al. Cognitive Reserve Assessment Scale in Health (CRASH): Its Validity and Reliability. J. Clin. Med. 2019, 8, 586. [Google Scholar] [CrossRef]
- Darwish, H.; Farran, N.; Assaad, S.; Chaaya, M. Cognitive Reserve Factors in a Developing Country: Education and Occupational Attainment Lower the Risk of Dementia in a Sample of Lebanese Older Adults. Front. Aging Neurosci. 2018, 10, 277. [Google Scholar] [CrossRef]
- Salthouse, T.A.; Atkinson, T.M.; Berish, D.E. Executive Functioning as a Potential Mediator of Age-Related Cognitive Decline in Normal Adults. J. Exp. Psychol. Gen. 2003, 132, 566–594. [Google Scholar] [CrossRef]
- Ikanga, J.; Hill, E.M.; MacDonald, D.A. The conceptualization and measurement of cognitive reserve using common proxy indicators: Testing some tenable reflective and formative models. J. Clin. Exp. Neuropsychol. 2017, 39, 72–83. [Google Scholar] [CrossRef] [PubMed]
- Siedlecki, K.L.; Stern, Y.; Reuben, A.; Sacco, R.L.; Elkind, M.S.; Wright, C.B. Construct validity of cognitive reserve in a multiethnic cohort: The Northern Manhattan Study. J. Int. Neuropsychol. Soc. 2009, 15, 558–569. [Google Scholar] [CrossRef]
- Darwish, H.; Zeinoun, P.; Farran, N.; Ghusn, H.; Yamout, B.; Khoury, S.J. The Brief International Cognitive Assessment in Multiple Sclerosis (BICAMS): Validation in Arabic and Lebanese Normative Values. J. Int. Neuropsychol. Soc. 2022, 28, 94–103. [Google Scholar] [CrossRef] [PubMed]
- CIA. The World Fact Book: Lebanon; Central Intelligence Agency: Washington, DC, USA, 2020; Volume 2020. Available online: https://www.cia.gov/the-world-factbook/countries/lebanon/ (accessed on 28 November 2023).
- UNESCO. Education and Literacy: Lebanon; United Nations Educational, Scientific and Cultural Organization, Institute for Statistics, Sustainable Development Goals: Montreal, QC, Canada, 2017; Volume 2020, Available online: http://uis.unesco.org/en/country/lb (accessed on 28 November 2023).
- Fares, S.; Dirani, J.; Darwish, H. Arabic validation of the hopkins symptom checklist-25 (HSCL) in a Lebanese sample of adults and older adults. Curr. Psychol. 2021, 40, 2980–2987. [Google Scholar] [CrossRef]
- Mahfoud, Z.; Kobeissi, L.; Peters, T.J.; Araya, R.; Ghantous ZKhoury, B. The Arabic Validation of the Hopkins Symptoms Checklist-25 against MINI in a Disadvantaged Suburb of Beirut, Lebanon. Int. J. Educ. Psychol. Assess. 2013, 13, 17–33. [Google Scholar]
- Winokur, A.; Winokur, D.F.; Rickels, K.; Cox, D.S. Symptoms of Emotional Distress in a Family Planning Service: Stability over a Four-Week Period. Br. J. Psychiatry 1984, 144, 395–399. [Google Scholar] [CrossRef] [PubMed]
- Rahman, T.T.A.; El Gaafary, M.M. Montreal Cognitive Assessment Arabic version: Reliability and validity prevalence of mild cognitive impairment among elderly attending geriatric clubs in Cairo. Geriatr. Gerontol. Int. 2009, 9, 54–61. [Google Scholar] [CrossRef] [PubMed]
- Nasreddine, Z.S.; Phillips, N.A.; Bédirian, V.; Charbonneau, S.; Whitehead, V.; Collin, I.; Cummings, J.L.; Chertkow, H. The Montreal Cognitive Assessment, MoCA: A Brief Screening Tool for Mild Cognitive Impairment. J. Am. Geriatr. Soc. 2005, 53, 695–699. [Google Scholar] [CrossRef]
- Carson, N.; Leach, L.; Murphy, K.J. A re-examination of Montreal Cognitive Assessment (MoCA) cutoff scores. Int. J. Geriatr. Psychiatry 2018, 33, 379–388. [Google Scholar] [CrossRef]
- WHO. WHODAS Version 2.0 Translation Package (Version 1). World Health Organization. 2012. Available online: https://terrance.who.int/mediacentre/data/WHODAS/Guidelines/WHODAS%202.0%20Translation%20guidelines.pdf (accessed on 28 November 2023).
- Brown, L.; RJSherbenou, R.J.; Johnsen, S.K. Test of Nonverbal Intelligence, 3rd ed.; Examiner’s Manual; Pro-Ed: Austin, TX, USA, 1997. [Google Scholar]
- Smith, A. Symbol Digit Modalities Test; Western Psychological Services: Los Angeles, CA, USA, 1973. [Google Scholar]
- Benedict, R.H.B. Brief Visuospatial Memory Test—Revised; PAR: Lutz, FL, USA, 1997. [Google Scholar]
- Zeinoun, P.; Farran, N.; Khoury, S.J.; Darwish, H. Development, psychometric properties, and pilot norms of the first Arabic indigenous memory test: The Verbal Memory Arabic Test (VMAT). J. Clin. Exp. Neuropsychol. 2020, 42, 505–515. [Google Scholar] [CrossRef]
- Jewsbury, P.A.; Bowden, S.C.; Duff, K. The Cattell–Horn–Carroll model of cognition for clinical assessment. J. Psychoeduc. Assess. 2017, 35, 547–567. [Google Scholar] [CrossRef]
- McGrew, K.S. CHC theory and the human cognitive abilities project: Standing on the shoulders of the giants of psychometric intelligence research. Intelligence 2009, 37, 1–10. [Google Scholar] [CrossRef]
- Bell, N.L.; McConnell, J.E.; Lassiter, K.S.; Darin Matthews, T. The Validity of the Universal Nonverbal Intelligence Test with the Woodcock-Johnson III Tests of Achievement. N. Am. J. Psychol. 2013, 15, 243–256. [Google Scholar]
- Hu, L.T.; Bentler, P.M. Cutoff criteria for fit indexes in covariance structure analysis: Conventional criteria versus new alternatives. Struct. Equ. Model. Multidiscip. J. 1999, 6, 1–55. [Google Scholar] [CrossRef]
- Lewis, M.P.; Simons, G.F.; Fennig, C.D. Ethnologue: Languages of Ecuador; SIL International: Dallas, TX, USA, 2015. [Google Scholar]
- Stern, Y. Cognitive Reserve: Theory and Applications; Taylor and Francis: New York, NY, USA, 2007. [Google Scholar]
- Satz, P.; Cole, M.A.; Hardy, D.J.; Rassovsky, Y. Brain and cognitive reserve: Mediator(s) and construct validity, a critique. J. Clin. Exp. Neuropsychol. 2011, 33, 121–130. [Google Scholar] [CrossRef] [PubMed]
- Mitchell, M.B.; Shaughnessy, L.W.; Shirk, S.D.; Yang, F.M.; Atri, A. Neuropsychological Test Performance and Cognitive Reserve in Healthy Aging and the Alzheimer’s Disease Spectrum: A Theoretically Driven Factor Analysis. J. Int. Neuropsychol. Soc. 2012, 18, 1071–1080. [Google Scholar] [CrossRef] [PubMed]
- Manly, J.J.; Schupf, N.; Tang, M.-X.; Stern, Y. Cognitive Decline and Literacy Among Ethnically Diverse Elders. J. Geriatr. Psychiatry Neurol. 2005, 18, 213–217. [Google Scholar] [CrossRef]
- Manly, J.J.; Touradji, P.; Tang, M.-X.; Stern, Y. Literacy and Memory Decline Among Ethnically Diverse Elders. J. Clin. Exp. Neuropsychol. 2003, 25, 680–690. [Google Scholar] [CrossRef]
- Chan, R.C.K.; Shum, D.; Toulopoulou, T.; Chen, E.Y. Assessment of executive functions: Review of instruments and identification of critical issues. Arch. Clin. Neuropsychol. 2008, 23, 201–216. [Google Scholar] [CrossRef]

{kind=link}
{kind=link}
| Age Group | F | % |
|---|---|---|
| Young adults (18–35 years) | 69 | 39.66 |
| Middle-aged adults (36–55 years) | 50 | 28.74 |
| Older adults (56–80 years) | 55 | 31.61 |
| Sex | ||
| Male | 68 | 39.08 |
| Female | 106 | 60.92 |
| Education * | ||
| Literate with no schooling | 2 | 1.15 |
| Young adults | 0 | 0 |
| Middle-aged adults | 0 | 0 |
| Older adults | 2 | 1.15 |
| Elementary to Intermediate | 15 | 8.62 |
| Young adults | 0 | 0 |
| Middle-aged adults | 2 | 1.15 |
| Older adults | 3 | 7.47% |
| Some high school | 7 | 4.02 |
| Young adults | 0 | 0 |
| Middle-aged adults | 4 | 2.30 |
| Older adults | 3 | 1.72 |
| Completed high school | 24 | 13.79 |
| Young adults | 12 | 6.90 |
| Middle-aged adults | 4 | 2.30 |
| Older adults | 8 | 4.60 |
| Vocational education | 12 | 6.90 |
| Young adults | 1 | 0.57 |
| Middle-aged adults | 3 | 1.72 |
| Older adults | 8 | 4.60 |
| University | 114 | 65.52 |
| Young adults | 56 | 32.18 |
| Middle-aged adults | 37 | 21.26 |
| Older adults | 21 | 12.07 |
| Current employment status | ||
| Employed | 100 | 57.47 |
| Unemployed | 74 | 42.53 |
| Marital status | ||
| Married | 75 | 43.10 |
| In a relationship | 12 | 6.90 |
| Divorced, separated, or widowed | 21 | 12.07 |
| Single | 66 | 37.93 |
| General health | ||
| Illness present (apart from the health-related exclusion criteria) ** | 46 | 26.44 |
| Illness absent | 128 | 73.56 |
| Smoking | ||
| Yes | 50 | 28.74 |
| No | 124 | 71.26 |
| Physical activity | ||
| Yes | 125 | 71.84 |
| Frequency | ||
| 1–2 times per week | 38 | 21.84 |
| 3–4 times per week | 32 | 18.39 |
| 5 or more times per week | 47 | 27.01 |
| 1–5 times per month | 8 | 4.60 |
| No | 49 | 28.16 |
| Gf | M | SD |
|---|---|---|
| Test of Nonverbal Intelligence, 3rd Edition | 103.02 | 16.82 |
| Glr | ||
| Verbal Memory Arabic Test: Trials 1 to 5 | 50.90 | 9.19 |
| Verbal Memory Arabic Test: Short Delay-Free | 10.27 | 2.76 |
| Verbal Memory Arabic Test: Long Delay-Free | 10.72 | 2.60 |
| Brief Visuospatial Memory Test—Revised | 22.25 | 6.95 |
| Gs | ||
| Symbol Digit Modalities Test | 55.38 | 13.28 |
| Cognitive Reserve Domain | Total Sample | Young Adults | Middle-Aged Adults | Older Adults |
|---|---|---|---|---|
| Education * | ||||
| Years of education (including postgraduate/ specializations) | 17.09 ± 4.83 | 18.36 ± 2.75 | 18.93 ± 4.83 | 13.82 ± 5.28 |
| Years of vocational training | 10.66 ± 1.31 | 0.26 ± 0.52 | 1.07 ± 1.78 | 0.79 ± 1.39 |
| Working activity ** | ||||
| Never employed | 0.71 | 1.69 | 0.09 | 0.59 |
| Level 1: low-skilled manual work | 4.01 | 3.55 | 2.38 | 8.89 |
| Level 2: skilled manual work | 21.84 | 30.51 | 14.53 | 27.17 |
| Level 3: skilled non-manual work | 25.63 | 30.67 | 23.40 | 23.72 |
| Level 4: professional occupation | 39.77 | 27.31 | 49.20 | 34.80 |
| Level 5: highly responsible or intellectual occupation | 8.04 | 6.27 | 10.40 | 4.83 |
| Leisure time ** | ||||
| Reading newspapers and magazines | 7.26 | 7.42 | 6.70 | 8.26 |
| Domestic chores | 7.94 | 5.38 | 9.76 | 8.62 |
| Driving | 8.68 | 8.17 | 9.31 | 8.20 |
| Leisure activities | 7.68 | 6.26 | 8.36 | 8.85 |
| Using new technologies | 10.18 | 12.46 | 10.06 | 5.95 |
| Social activities | 7.99 | 11.44 | 6.30 | 5.27 |
| Cinema, theater | 2.96 | 3.65 | 2.56 | 2.59 |
| Small-scale operations | 5.15 | 2.35 | 5.76 | 9.19 |
| Looking after others | 2.75 | 2.46 | 2.85 | 3.11 |
| Voluntary work | 3.34 | 3.74 | 2.93 | 3.56 |
| Artistic activities | 3.89 | 5.76 | 2.61 | 3.28 |
| Exhibitions, concerts, conferences | 5.60 | 6.28 | 5.21 | 5.17 |
| Holidays | 3.54 | 2.16 | 3.94 | 5.36 |
| Reading books | 7.52 | 8.17 | 6.68 | 8.28 |
| Pet care | 2.94 | 3.87 | 2.63 | 1.79 |
| Managing one’s bank account(s) | 7.99 | 9.24 | 7.65 | 6.34 |
| Model | ||||
|---|---|---|---|---|
| Variable | A | B | C | D |
| Fit statistics | ||||
| X2 | 0 | 45.37 | 41.48 | 39.52 |
| df | 0 | 23.00 | 21.00 | 17.00 |
| X2/df | 1.97 | 1.98 | 2.33 | |
| CFI | 1 | 0.96 | 0.97 | 0.96 |
| RMSEA | 0.08 | 0.08 | 0.09 | |
| Loadings on cognitive reserve construct | ||||
| CR-->education | 0.42 ** | 0.46 ** | 0.44 * | 0.35 * |
| CR-->working activity | 0.66 * | 0.63 ** | 0.64 * | 0.59 * |
| CR-->leisure time | 0.56 NA | 0.55 NA | 0.74 NA | 0.55 NA |
| Correlations with other constructs | ||||
| CR<->Gf | 0.38 * | 0.54 * | ||
| CR<->Glr | 0.24 * | 0.39 * | ||
| CR<->Gs | 0.37 * | 0.48 * | ||
| Gf | Glr | Gs | ||
| Loadings on other constructs | ||||
| Model C | ||||
| Education | ||||
| Working activity | −0.14 | |||
| Leisure time | −0.25 | |||
| Model D | ||||
| Education | 0.27 * | −0.03 | 0.05 | |
| Working activity | 0.22 | −0.08 | 0.12 | |
| Leisure time | −0.02 | 0.03 | 0.24 | |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Farran, N.; Darwish, H. Validation of the Cognitive Reserve Index Questionnaire (CRIq) in Arabic. Behav. Sci. 2023, 13, 1006. https://doi.org/10.3390/bs13121006
Farran N, Darwish H. Validation of the Cognitive Reserve Index Questionnaire (CRIq) in Arabic. Behavioral Sciences. 2023; 13(12):1006. https://doi.org/10.3390/bs13121006
Chicago/Turabian StyleFarran, Natali, and Hala Darwish. 2023. "Validation of the Cognitive Reserve Index Questionnaire (CRIq) in Arabic" Behavioral Sciences 13, no. 12: 1006. https://doi.org/10.3390/bs13121006
APA StyleFarran, N., & Darwish, H. (2023). Validation of the Cognitive Reserve Index Questionnaire (CRIq) in Arabic. Behavioral Sciences, 13(12), 1006. https://doi.org/10.3390/bs13121006