
Deepening Depression in Women Balancing Work–Life Responsibilities and Caregiving during the COVID-19 Pandemic: Findings from Gender-Specific Face-to-Face Street Interviews Conducted in Italy

 , , ,
, , ,
Abstract
:1. Introduction
2. Methods
2.1. Study Design and Population
2.2. Context
2.3. Assessment Tools
- (a)
- Section 1 included information on the study, privacy protection, and informed consent.
- (b)
- Section 2 included the participants’ demographic backgrounds, including age, education, work, marital status, number of children, working activity, and socio-economic status. The history of life events included the impact of the COVID-19 pandemic, complex management of family life and work during the COVID-19 pandemic, and the impact produced by the 2009 L’Aquila earthquake measured on a 5-point Likert scale (0 = None; 1 = Only a little; 2 = To some extent; 3 = Considerably; 4 = Greatly). Previous contact with mental health services, mental health issues, and treatments were also assessed.
- (c)
- Section 3 included standardized questionnaires investigating quality of life, psychopathology, family functioning, and family burden.
2.4. Statistical Analyses
3. Results
3.1. Socio-Demographic and Characteristics of the Sample, Depression, Health-Related Quality of Life, and Family Functioning
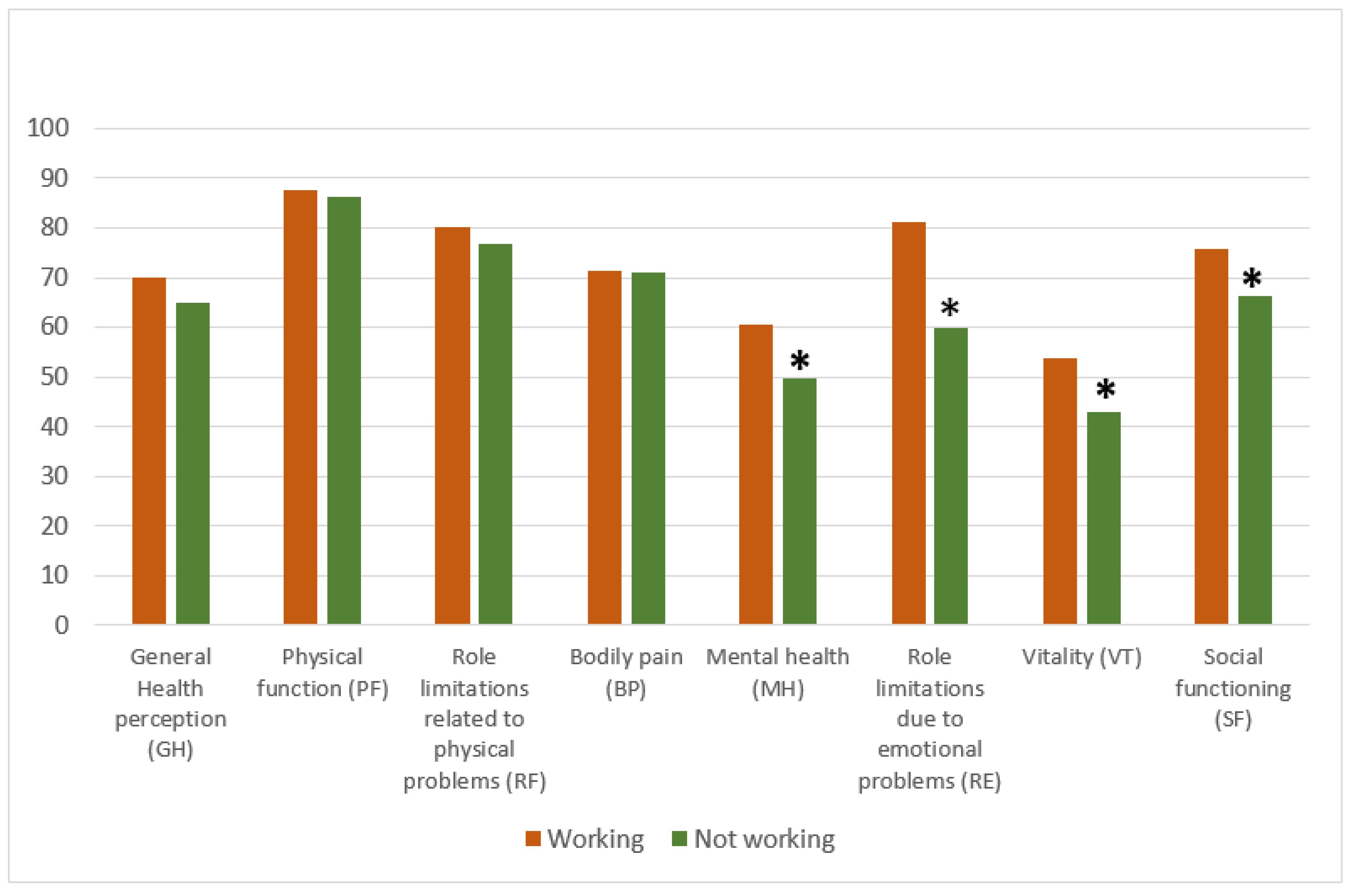
3.1.1. Comparison between Female Workers and Non-Workers
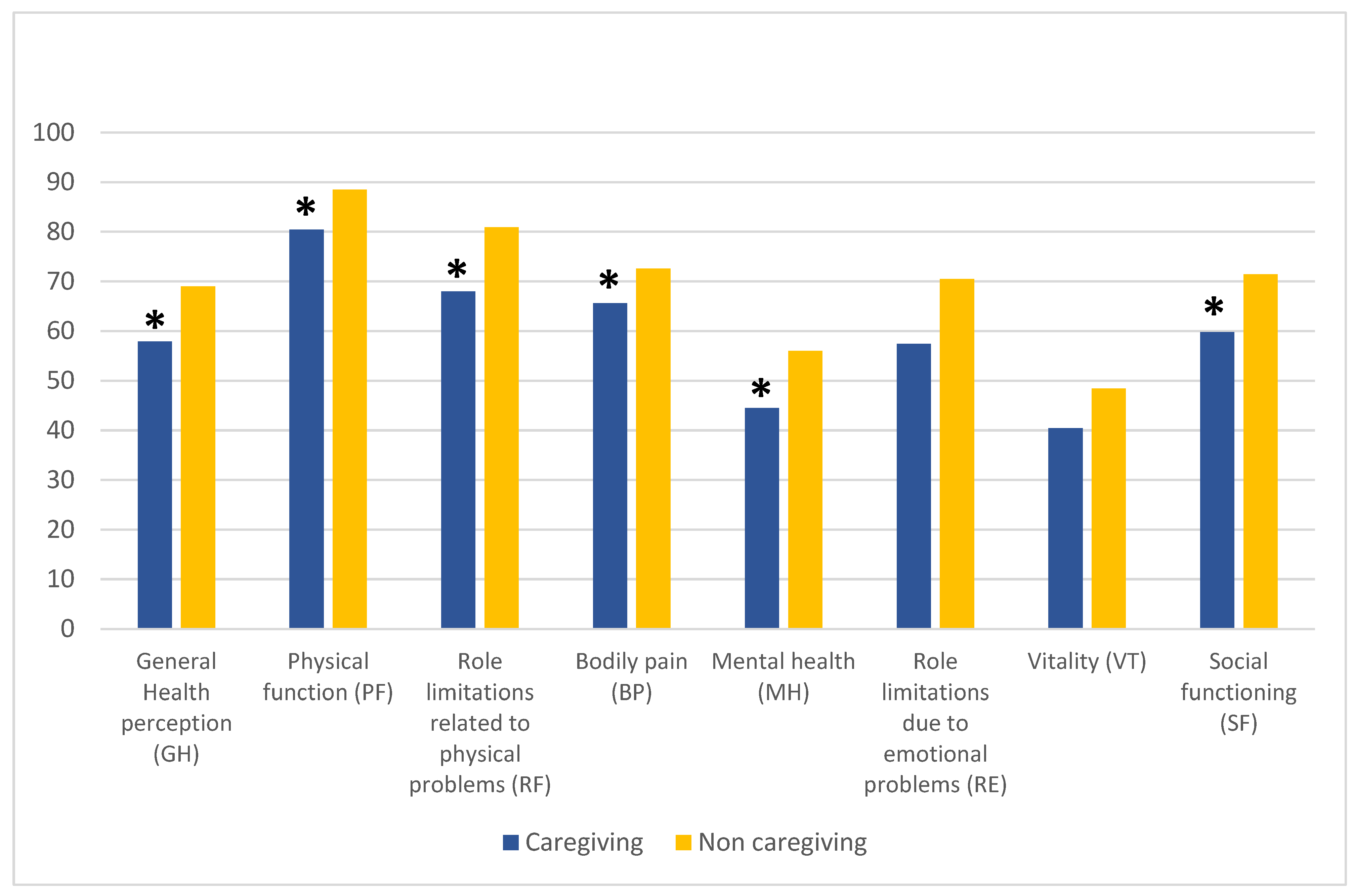
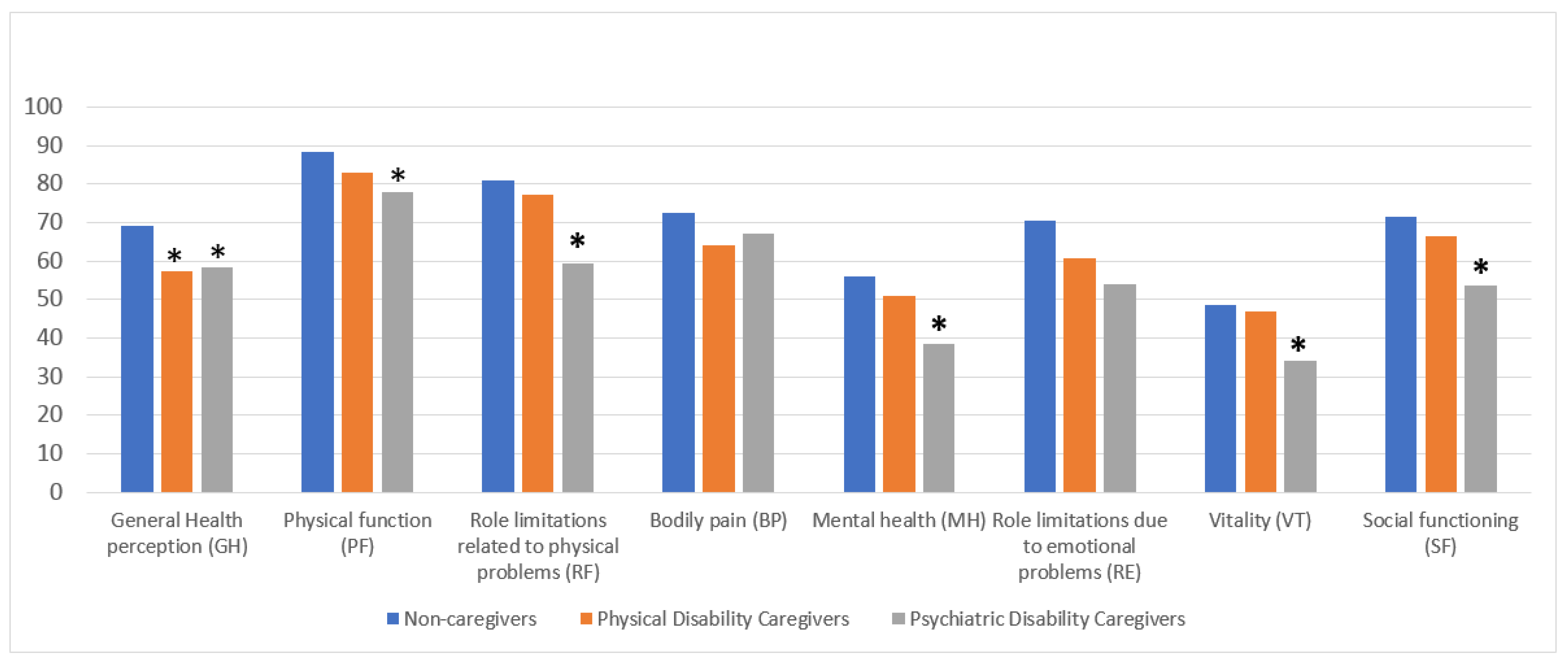
3.1.2. Comparison between Female Caregivers and Non-Caregivers
3.2. Correlations between Age, Years of Education, Health-Related Quality of Life, Family Functioning, and Burden of Care
3.3. Variables Impacting Severe Depressive Symptomatology
4. Discussion
Strengths and Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Shockley, K.M.; Clark, M.A.; Dodd, H.; King, E.B. Work-family strategies during COVID-19: Examining gender dynamics among dual-earner couples with young children. J. Appl. Psychol. 2021, 106, 15–28. [Google Scholar] [CrossRef]
- Wanberg, C.R.; Csillag, B.; Douglass, R.P.; Zhou, L.; Pollard, M.S. Socioeconomic status and well-being during COVID-19: A resource-based examination. J. Appl. Psychol. 2020, 105, 1382–1396. [Google Scholar] [CrossRef]
- Qiu, J.; Shen, B.; Zhao, M.; Wang, Z.; Xie, B.; Xu, Y. A nationwide survey of psychological distress among Chinese people in the COVID-19 epidemic: Implications and policy recommendations. Gen. Psychiatry 2020, 33, e100213. [Google Scholar] [CrossRef]
- Wang, C.; Pan, R.; Wan, X.; Tan, Y.; Xu, L.; Ho, C.S.; Ho, R.C. Immediate Psychological Responses and Associated Factors during the Initial Stage of the 2019 Coronavirus Disease (COVID-19) Epidemic among the General Population in China. Int. J. Environ. Res. Public Health 2020, 17, 1729. [Google Scholar] [CrossRef]
- Horesh, D.; Brown, A.D. Traumatic stress in the age of COVID-19: A call to close critical gaps and adapt to new realities. Psychol. Trauma 2020, 12, 331–335. [Google Scholar] [CrossRef]
- Lima, C.K.T.; Carvalho, P.M.M.; Lima, I.; Nunes, J.; Saraiva, J.S.; de Souza, R.I.; da Silva, C.G.L.; Neto, M.L.R. The emotional impact of Coronavirus 2019-nCoV (new Coronavirus disease). Psychiatry Res. 2020, 287, 112915. [Google Scholar] [CrossRef]
- Rajkumar, R.P. COVID-19 and mental health: A review of the existing literature. Asian J. Psychiatry 2020, 52, 102066. [Google Scholar] [CrossRef]
- Husky, M.M.; Kovess-Masfety, V.; Swendsen, J.D. Stress and anxiety among university students in France during COVID-19 mandatory confinement. Compr. Psychiatry 2020, 102, 152191. [Google Scholar] [CrossRef]
- Robinson, L.E.; Valido, A.; Drescher, A.; Woolweaver, A.B.; Espelage, D.L.; LoMurray, S.; Long, A.C.J.; Wright, A.A.; Dailey, M.M. Teachers, Stress, and the COVID-19 Pandemic: A Qualitative Analysis. Sch. Ment. Health 2023, 15, 78–89. [Google Scholar] [CrossRef]
- Giusti, L.; Salza, A.; Mammarella, S.; Bianco, D.; Ussorio, D.; Casacchia, M.; Roncone, R. #Everything Will Be Fine. Duration of Home Confinement and “All-or-Nothing” Cognitive Thinking Style as Predictors of Traumatic Distress in Young University Students on a Digital Platform During the COVID-19 Italian Lockdown. Front. Psychiatry 2020, 11, 574812. [Google Scholar] [CrossRef]
- Kar, N.; Kar, B.; Kar, S. Stress and coping during COVID-19 pandemic: Result of an online survey. Psychiatry Res. 2021, 295, 113598. [Google Scholar] [CrossRef]
- Phungsoonthorn, T.; Charoensukmongkol, P. How does mindfulness help university employees cope with emotional exhaustion during the COVID-19 crisis? The mediating role of psychological hardiness and the moderating effect of workload. Scand. J. Psychol. 2022, 63, 449–461. [Google Scholar] [CrossRef]
- Alzueta, E.; Perrin, P.; Baker, F.C.; Caffarra, S.; Ramos-Usuga, D.; Yuksel, D.; Arango-Lasprilla, J.C. How the COVID-19 pandemic has changed our lives: A study of psychological correlates across 59 countries. J. Clin. Psychol. 2021, 77, 556–570. [Google Scholar] [CrossRef]
- Zhao, S.Z.; Wong, J.Y.H.; Luk, T.T.; Wai, A.K.C.; Lam, T.H.; Wang, M.P. Mental health crisis under COVID-19 pandemic in Hong Kong, China. Int. J. Infect. Dis. 2020, 100, 431–433. [Google Scholar] [CrossRef]
- Cecchini, J.A.; Carriedo, A.; Fernandez-Rio, J.; Mendez-Gimenez, A.; Gonzalez, C.; Sanchez-Martinez, B.; Rodriguez-Gonzalez, P. A longitudinal study on depressive symptoms and physical activity during the Spanish lockdown. Int. J. Clin. Health Psychol. 2021, 21, 100200. [Google Scholar] [CrossRef]
- Pai, N.; Vella, S.L. COVID-19 and loneliness: A rapid systematic review. Aust. N. Z. J. Psychiatry 2021, 55, 1144–1156. [Google Scholar] [CrossRef]
- Lampraki, C.; Hoffman, A.; Roquet, A.; Jopp, D.S. Loneliness during COVID-19: Development and influencing factors. PLoS ONE 2022, 17, e0265900. [Google Scholar] [CrossRef]
- Currin, J.M.; Evans, A.E.; Miller, B.M.; Owens, C.; Giano, Z.; Hubach, R.D. The impact of initial social distancing measures on individuals’ anxiety and loneliness depending on living with their romantic/sexual partners. Curr. Psychol. 2022, 42, 14953–14961. [Google Scholar] [CrossRef]
- Cacioppo, J.T.; Cacioppo, S. Loneliness in the modern age: An Evolutionary Theory of Loneliness (ETL). In Advances in Experimental Social Psychology; Olson, J.M., Ed.; Academic Press: London, UK, 2018; Volume 58, pp. 127–197. [Google Scholar]
- Keller, F.M.; Derksen, C.; Kotting, L.; Dahmen, A.; Lippke, S. Distress, loneliness, and mental health during the COVID-19 pandemic: Test of the extension of the Evolutionary Theory of Loneliness. Appl. Psychol. Health Well Being 2023, 15, 24–48. [Google Scholar] [CrossRef]
- Bianchini, V.; Giusti, L.; Salza, A.; Cofini, V.; Cifone, M.G.; Casacchia, M.; Fabiani, L.; Roncone, R. Moderate Depression Promotes Posttraumatic Growth (Ptg): A Young Population Survey 2 Years after the 2009 L’Aquila Earthquake. Clin. Pract. Epidemiol. Ment. Health 2017, 13, 10–19. [Google Scholar] [CrossRef]
- Gao, X.; Leng, Y.; Guo, Y.; Yang, J.; Cui, Q.; Geng, B.; Hu, H.; Zhou, Y. Association between earthquake experience and depression 37 years after the Tangshan earthquake: A cross-sectional study. BMJ Open 2019, 9, e026110. [Google Scholar] [CrossRef] [PubMed]
- Mazza, C.; Ricci, E.; Biondi, S.; Colasanti, M.; Ferracuti, S.; Napoli, C.; Roma, P. A Nationwide Survey of Psychological Distress among Italian People during the COVID-19 Pandemic: Immediate Psychological Responses and Associated Factors. Int. J. Environ. Res. Public Health 2020, 17, 3165. [Google Scholar] [CrossRef] [PubMed]
- Pancani, L.; Marinucci, M.; Aureli, N.; Riva, P. Forced Social Isolation and Mental Health: A Study on 1,006 Italians Under COVID-19 Lockdown. Front. Psychol. 2021, 12, 663799. [Google Scholar] [CrossRef] [PubMed]
- Carpiniello, B.; Tusconi, M.; Zanalda, E.; Di Sciascio, G.; Di Giannantonio, M.; Executive Committee of The Italian Society of Psychiatry. Psychiatry during the COVID-19 pandemic: A survey on mental health departments in Italy. BMC Psychiatry 2020, 20, 593. [Google Scholar] [CrossRef]
- Almeida, M.; Shrestha, A.D.; Stojanac, D.; Miller, L.J. The impact of the COVID-19 pandemic on women’s mental health. Arch. Women Ment. Health 2020, 23, 741–748. [Google Scholar] [CrossRef]
- Thibaut, F.; van Wijngaarden-Cremers, P.J.M. Women’s Mental Health in the Time of COVID-19 Pandemic. Front. Glob. Womens Health 2020, 1, 588372. [Google Scholar] [CrossRef]
- Liu, H.; Wang, L.L.; Zhao, S.J.; Kwak-Kim, J.; Mor, G.; Liao, A.H. Why are pregnant women susceptible to COVID-19? An immunological viewpoint. J. Reprod. Immunol. 2020, 139, 103122. [Google Scholar] [CrossRef]
- Santomauro, D.F.; Mantilla Herrera, A.M.; Shadid, J.; Zheng, P.; Ashbaugh, C.; Pigott, D.M.; Abbafati, C.; Adolph, C.; Amlag, J.O.; Aravkin, A.Y.; et al. Global prevalence and burden of depressive and anxiety disorders in 204 countries and territories in 2020 due to the COVID-19 pandemic. Lancet 2021, 398, 1700–1712. [Google Scholar] [CrossRef]
- Street, A.E.; Dardis, C.M. Using a social construction of gender lens to understand gender differences in posttraumatic stress disorder. Clin. Psychol. Rev. 2018, 66, 97–105. [Google Scholar] [CrossRef]
- Hao, F.; Tan, W.; Jiang, L.; Zhang, L.; Zhao, X.; Zou, Y.; Hu, Y.; Luo, X.; Jiang, X.; McIntyre, R.S.; et al. Do psychiatric patients experience more psychiatric symptoms during COVID-19 pandemic and lockdown? A case-control study with service and research implications for immunopsychiatry. Brain Behav. Immun. 2020, 87, 100–106. [Google Scholar] [CrossRef]
- Campbell, A.M. An increasing risk of family violence during the COVID-19 pandemic: Strengthening community collaborations to save lives. Forensic Sci. Int. Rep. 2020, 2, 100089. [Google Scholar] [CrossRef]
- Romito, P.; Pellegrini, M.; Saurel-Cubizolles, M.J. Intimate Partner Violence Against Women During the COVID-19 Lockdown in Italy: A Multicenter Survey Involving Anti-Violence Centers. Violence Against Women 2022, 28, 2186–2203. [Google Scholar] [CrossRef] [PubMed]
- Piquero, A.R.; Jennings, W.G.; Jemison, E.; Kaukinen, C.; Knaul, F.M. Domestic violence during the COVID-19 pandemic—Evidence from a systematic review and meta-analysis. J. Crim. Justice 2021, 74, 101806. [Google Scholar] [CrossRef] [PubMed]
- Leroy, S.; Schmidt, A.M.; Madjar, N. Working from home during COVID-19: A study of the interruption landscape. J. Appl. Psychol. 2021, 106, 1448–1465. [Google Scholar] [CrossRef]
- Loezar-Hernandez, M.; Briones-Vozmediano, E.; Ronda-Perez, E.; Otero-Garcia, L. Juggling during Lockdown: Balancing Telework and Family Life in Pandemic Times and Its Perceived Consequences for the Health and Wellbeing of Working Women. Int. J. Environ. Res. Public Health 2023, 20, 4781. [Google Scholar] [CrossRef]
- Matthews, T.A.; Chen, L.; Omidakhsh, N.; Zhang, D.; Han, X.; Chen, Z.; Shi, L.; Li, Y.; Wen, M.; Li, H.; et al. Gender difference in working from home and psychological distress—A national survey of U.S. employees during the COVID-19 pandemic. Ind. Health 2022, 60, 334–344. [Google Scholar] [CrossRef]
- Xiao, Y.; Becerik-Gerber, B.; Lucas, G.; Roll, S.C. Impacts of Working from Home During COVID-19 Pandemic on Physical and Mental Well-Being of Office Workstation Users. J. Occup. Environ. Med. 2021, 63, 181–190. [Google Scholar] [CrossRef]
- Möhring, K.; Naumann, E.; Reifenscheid, M.; Wenz, A.; Rettig, T.; Krieger, U.; Friedel, S.; Finkel, M.; Cornesse, C.; Blom, A.G. The COVID-19 pandemic and subjective well-being: Longitudinal evidence on satisfaction with work and family. Eur. Soc. 2020, 23, S601–S617. [Google Scholar] [CrossRef]
- Burn, E.; Tattarini, G.; Williams, I.; Lombi, L.; Gale, N.K. Women’s Experience of Depressive Symptoms While Working from Home During the COVID-19 Pandemic: Evidence from an International Web Survey. Front. Sociol. 2022, 7, 763088. [Google Scholar] [CrossRef]
- Damian, A.C.; Ciobanu, A.M.; Anghele, C.; Papacocea, I.R.; Manea, M.C.; Iliuta, F.P.; Ciobanu, C.A.; Papacocea, S. Caregiving for Dementia Patients during the Coronavirus Pandemic. J. Clin. Med. 2023, 12, 2616. [Google Scholar] [CrossRef]
- Zwar, L.; Konig, H.H.; Hajek, A. Gender Differences in Mental Health, Quality of Life, and Caregiver Burden among Informal Caregivers during the Second Wave of the COVID-19 Pandemic in Germany: A Representative, Population-Based Study. Gerontology 2022, 69, 149–162. [Google Scholar] [CrossRef] [PubMed]
- Maggio, M.G.; La Rosa, G.; Calatozzo, P.; Andaloro, A.; Foti Cuzzola, M.; Cannavo, A.; Militi, D.; Manuli, A.; Oddo, V.; Pioggia, G.; et al. How COVID-19 Has Affected Caregivers’ Burden of Patients with Dementia: An Exploratory Study Focusing on Coping Strategies and Quality of Life during the Lockdown. J. Clin. Med. 2021, 10, 5953. [Google Scholar] [CrossRef] [PubMed]
- Dhiman, S.; Sahu, P.K.; Reed, W.R.; Ganesh, G.S.; Goyal, R.K.; Jain, S. Impact of COVID-19 outbreak on mental health and perceived strain among caregivers tending children with special needs. Res. Dev. Disabil. 2020, 107, 103790. [Google Scholar] [CrossRef] [PubMed]
- Busse, C.; Barnini, T.; Zucca, M.; Rainero, I.; Mozzetta, S.; Zangrossi, A.; Cagnin, A. Depression, Anxiety and Sleep Alterations in Caregivers of Persons With Dementia After 1-Year of COVID-19 Pandemic. Front. Psychiatry 2022, 13, 826371. [Google Scholar] [CrossRef] [PubMed]
- Eckardt, J.P. Caregivers of people with severe mental illness in the COVID-19 pandemic. Lancet Psychiatry 2020, 7, E53. [Google Scholar] [CrossRef] [PubMed]
- Fusar-Poli, L.; Surace, T.; Meo, V.; Patania, F.; Avanzato, C.; Pulvirenti, A.; Aguglia, E.; Signorelli, M.S. Psychological well-being and family distress of Italian caregivers during the COVID-19 outbreak. J. Community Psychol. 2022, 50, 2243–2259. [Google Scholar] [CrossRef]
- Stanley, S.; Balakrishnan, S.; Ilangovan, S. Psychological distress, perceived burden and quality of life in caregivers of persons with schizophrenia. J. Ment. Health 2017, 26, 134–141. [Google Scholar] [CrossRef]
- Yasuma, N.; Yamaguchi, S.; Ogawa, M.; Shiozawa, T.; Abe, M.; Igarashi, M.; Kawaguchi, T.; Sato, S.; Nishi, D.; Kawakami, N.; et al. Care difficulties and burden during COVID-19 pandemic lockdowns among caregivers of people with schizophrenia: A cross-sectional study. Neuropsychopharmacol. Rep. 2021, 41, 242–247. [Google Scholar] [CrossRef]
- Mork, E.; Aminoff, S.R.; Barrett, E.A.; Simonsen, C.; Hegelstad, W.T.V.; Lagerberg, T.V.; Melle, I.; Romm, K.L. COVID-19 lockdown—Who cares? The first lockdown from the perspective of relatives of people with severe mental illness. BMC Public Health 2022, 22, 1104. [Google Scholar] [CrossRef]
- Jesus, T.S.; Bhattacharjya, S.; Papadimitriou, C.; Bogdanova, Y.; Bentley, J.; Arango-Lasprilla, J.C.; Kamalakannan, S.; The Refugee Empowerment Task Force International Networking Group of The American Congress of Rehabilitation Medicine. Lockdown-Related Disparities Experienced by People with Disabilities during the First Wave of the COVID-19 Pandemic: Scoping Review with Thematic Analysis. Int. J. Environ. Res. Public Health 2021, 18, 6178. [Google Scholar] [CrossRef]
- Kinser, P.A.; Lyon, D.E. A conceptual framework of stress vulnerability, depression, and health outcomes in women: Potential uses in research on complementary therapies for depression. Brain Behav. 2014, 4, 665–674. [Google Scholar] [CrossRef]
- Roncone, R.; Giusti, L.; Mazza, M.; Bianchini, V.; Ussorio, D.; Pollice, R.; Casacchia, M. Persistent fear of aftershocks, impairment of working memory, and acute stress disorder predict post-traumatic stress disorder: 6-month follow-up of help seekers following the L’Aquila earthquake. Springerplus 2013, 2, 636. [Google Scholar] [CrossRef]
- Casacchia, M.; Bianchini, V.; Mazza, M.; Pollice, R.; Roncone, R. Acute stress reactions and associated factors in the help-seekers after the L’Aquila earthquake. Psychopathology 2013, 46, 120–130. [Google Scholar] [CrossRef]
- Casacchia, M.; Pollice, R.; Roncone, R. The narrative epidemiology of L’Aquila 2009 earthquake. Epidemiol. Psychiatr. Sci. 2012, 21, 13–21. [Google Scholar] [CrossRef] [PubMed]
- Cofini, V.; Carbonelli, A.; Cecilia, M.R.; di Orio, F. Quality of life, psychological wellbeing and resilience: A survey on the Italian population living in a new lodging after the earthquake of April 2009. Ann. Ig. 2014, 26, 46–51. [Google Scholar] [CrossRef]
- Gigantesco, A.; Mirante, N.; Granchelli, C.; Diodati, G.; Cofini, V.; Mancini, C.; Carbonelli, A.; Tarolla, E.; Minardi, V.; Salmaso, S.; et al. Psychopathological chronic sequelae of the 2009 earthquake in L’Aquila, Italy. J. Affect. Disord. 2013, 148, 265–271. [Google Scholar] [CrossRef] [PubMed]
- Imperiale, A.J.; Vanclay, F. The mechanism of disaster capitalism and the failure to build community resilience: Learning from the 2009 earthquake in L’Aquila, Italy. Disasters 2021, 45, 555–576. [Google Scholar] [CrossRef] [PubMed]
- Spitzer, R.L.; Kroenke, K.; Williams, J.B. Validation and utility of a self-report version of PRIME-MD: The PHQ primary care study. Primary Care Evaluation of Mental Disorders. Patient Health Questionnaire. JAMA 1999, 282, 1737–1744. [Google Scholar] [CrossRef] [PubMed]
- Kroenke, K.; Spitzer, R.L.; Williams, J.B. The PHQ-9: Validity of a brief depression severity measure. J. Gen. Intern. Med. 2001, 16, 606–613. [Google Scholar] [CrossRef]
- Ware, J.E.J.; Sherbourne, C.D. The MOS 36-item short-form health survey (SF-36). I. Conceptual framework and item selection. Med. Care 1992, 30, 473–483. [Google Scholar] [CrossRef]
- Apolone, G.; Mosconi, P. The Italian SF-36 Health Survey. J. Clin. Epidemiol. 1998, 51, 1025–1036. [Google Scholar] [CrossRef] [PubMed]
- Roncone, R.; Mazza, M.; Ussorio, D.; Pollice, R.; Falloon, I.R.; Morosini, P.; Casacchia, M. The questionnaire of family functioning: A preliminary validation of a standardized instrument to evaluate psychoeducational family treatments. Community Ment. Health J. 2007, 43, 591–607. [Google Scholar] [CrossRef] [PubMed]
- Morosini, P.; Roncone, R.; Veltro, F.; Palomba, U.; Casacchia, M. Routine assessment tool in psychiatry: The case of questionnaire of family attitude and burden. Ital. J. Psychiatry Behav. Sci. 1991, 1, 95–101. [Google Scholar]
- Andrews, G.; Hunt, C.; Jarry, M.; Morosini, P.; Roncone, R.; Tibaldi, G. Disturbi Mentali. Competenze di Base, Strumenti e Tecniche per Tutti gli Operatori; Centro Scientifico Editore: Torino, Italy, 2004. [Google Scholar]
- Roncone, R.; Giusti, L.; Bianchini, V.; Casacchia, M.; Carpiniello, B.; Aguglia, E.; Altamura, M.; Barlati, S.; Bellomo, A.; Bucci, P.; et al. Family functioning and personal growth in Italian caregivers living with a family member affected by schizophrenia: Results of an add-on study of the Italian network for research on psychoses. Front. Psychiatry 2022, 13, 1042657. [Google Scholar] [CrossRef] [PubMed]
- Yazawa, A.; Aida, J.; Kondo, K.; Kawachi, I. Gender differences in risk of posttraumatic stress symptoms after disaster among older people: Differential exposure or differential vulnerability? J. Affect. Disord. 2022, 297, 447–454. [Google Scholar] [CrossRef]
- Ribe, J.M.; Salamero, M.; Perez-Testor, C.; Mercadal, J.; Aguilera, C.; Cleris, M. Quality of life in family caregivers of schizophrenia patients in Spain: Caregiver characteristics, caregiving burden, family functioning, and social and professional support. Int. J. Psychiatry Clin. Pract. 2018, 22, 25–33. [Google Scholar] [CrossRef]
- Barrowclough, C.; Gooding, P.; Hartley, S.; Lee, G.; Lobban, F. Factors associated with distress in relatives of a family member experiencing recent-onset psychosis. J. Nerv. Ment. Dis. 2014, 202, 40–46. [Google Scholar] [CrossRef]
- Ilhan, B.; Berikol, G.B.; Eroglu, O.; Deniz, T. Prevalence and associated risk factors of post-traumatic stress disorder among survivors of the 2023 Turkey earthquake. Am. J. Emerg. Med. 2023, 72, 39–43. [Google Scholar] [CrossRef]
- Pazderka, H.; Shalaby, R.; Eboreime, E.; Mao, W.; Obuobi-Donkor, G.; Agyapong, B.; Oluwasina, F.; Adu, M.K.; Owusu, E.; Sapara, A.; et al. Isolation, Economic Precarity, and Previous Mental Health Issues as Predictors of PTSD Status in Females Living in Fort McMurray During COVID-19. Front. Psychiatry 2022, 13, 837713. [Google Scholar] [CrossRef]
- Wenham, C.; Smith, J.; Davies, S.E.; Feng, H.; Grepin, K.A.; Harman, S.; Herten-Crabb, A.; Morgan, R. Women are most affected by pandemics—Lessons from past outbreaks. Nature 2020, 583, 194–198. [Google Scholar] [CrossRef]
- Wenham, C.; Smith, J.; Morgan, R.; on behalf of the Gender and COVID-19 Working Group. COVID-19: The gendered impacts of the outbreak. Lancet 2020, 395, 846–848. [Google Scholar] [CrossRef] [PubMed]
- Bu, F.; Steptoe, A.; Fancourt, D. Loneliness during a strict lockdown: Trajectories and predictors during the COVID-19 pandemic in 38,217 United Kingdom adults. Soc. Sci. Med. 2020, 265, 113521. [Google Scholar] [CrossRef] [PubMed]
- Purvis, R.S.; Ayers, B.L.; Rowland, B.; Moore, R.; Hallgren, E.; McElfish, P.A. “Life is hard”: How the COVID-19 pandemic affected daily stressors of women. Dialogues Health 2022, 1, 100018. [Google Scholar] [CrossRef] [PubMed]
- Keitner, G.I.; Miller, I.W. Family functioning and major depression: An overview. Am. J. Psychiatry 1990, 147, 1128–1137. [Google Scholar] [CrossRef]
- Herr, N.R.; Hammen, C.; Brennan, P.A. Current and past depression as predictors of family functioning: A comparison of men and women in a community sample. J. Fam. Psychol. 2007, 21, 694–702. [Google Scholar] [CrossRef]
- Febres, J.; Rossi, R.; Gaudiano, B.A.; Miller, I.W. Differential relationship between depression severity and patients’ perceived family functioning in women versus in men. J. Nerv. Ment. Dis. 2011, 199, 449–453. [Google Scholar] [CrossRef]
- Fondazione ONDA Osservatorio Nazionale Sulla Salute della Donna e di Genere. COVID-19 e Salute di Genere: Da Pandemia a Sindemia. Esperienze, Nuove Consapevolezze, Sfide Future; Libro bianco 2021; Franco Angeli: Milano, Italy, 2021. [Google Scholar]
- Arpino, B.; Pasqualini, M. Effects of Pandemic on Feelings of Depression in Italy: The Role of Age, Gender, and Individual Experiences During the First Lockdown. Front. Psychol. 2021, 12, 660628. [Google Scholar] [CrossRef]
- Wormald, A.; McGlinchey, E.; D’Eath, M.; Leroi, I.; Lawlor, B.; McCallion, P.; McCarron, M.; O’Sullivan, R.; Chen, Y. Impact of COVID-19 Pandemic on Caregivers of People with an Intellectual Disability, in Comparison to Carers of Those with Other Disabilities and with Mental Health Issues: A Multicountry Study. Int. J. Environ. Res. Public Health 2023, 20, 3256. [Google Scholar] [CrossRef]
- Rainero, I.; Bruni, A.C.; Marra, C.; Cagnin, A.; Bonanni, L.; Cupidi, C.; Lagana, V.; Rubino, E.; Vacca, A.; Di Lorenzo, R.; et al. The Impact of COVID-19 Quarantine on Patients With Dementia and Family Caregivers: A Nation-Wide Survey. Front. Aging Neurosci. 2020, 12, 625781. [Google Scholar] [CrossRef]
- Boyd, K.; Winslow, V.; Borson, S.; Lindau, S.T.; Makelarski, J.A. Caregiving in a Pandemic: Health-Related Socioeconomic Vulnerabilities Among Women Caregivers Early in the COVID-19 Pandemic. Ann. Fam. Med. 2022, 20, 406–413. [Google Scholar] [CrossRef]
- Sharma, N.; Chakrabarti, S.; Grover, S. Gender differences in caregiving among family—Caregivers of people with mental illnesses. World J. Psychiatry 2016, 6, 7–17. [Google Scholar] [CrossRef] [PubMed]
- Fancourt, D.; Steptoe, A.; Bu, F. Trajectories of anxiety and depressive symptoms during enforced isolation due to COVID-19 in England: A longitudinal observational study. Lancet Psychiatry 2021, 8, 141–149. [Google Scholar] [CrossRef] [PubMed]
- Holz, N.E.; Berhe, O.; Sacu, S.; Schwarz, E.; Tesarz, J.; Heim, C.M.; Tost, H. Early Social Adversity, Altered Brain Functional Connectivity, and Mental Health. Biol. Psychiatry 2023, 93, 430–441. [Google Scholar] [CrossRef] [PubMed]
- Kourti, A.; Stavridou, A.; Panagouli, E.; Psaltopoulou, T.; Spiliopoulou, C.; Tsolia, M.; Sergentanis, T.N.; Tsitsika, A. Domestic Violence During the COVID-19 Pandemic: A Systematic Review. Trauma Violence Abus. 2023, 24, 719–745. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| Variables Included | Workers (n = 73) | Non-Workers (n = 138) |
|---|---|---|
| Age, mean (SD) * | 41.8 (13.2) | 32.4 (20.1) |
| Working conditions (%) | ||
| Self-employed/freelancers | 23 (31.5) | |
| Full-time work | 35 (47.9) | |
| Part-time work | 15 (20.5) | |
| Student | - | 91 (65.9) |
| Housewife | - | 13 (9.4) |
| Unemployed | - | 12 (8.7) |
| Retired | - | 22 (15.9) |
| Nationality (%) | ||
| Non-EU citizens | 4 (5.5) | 4 (2.9) |
| Marital status (%) * | ||
| Single | 16 (21.9) | 77 (55.8) |
| Married/partnership | 49 (67.1) | 50 (36.2) |
| Separated/divorced | 7 (9.6) | 4 (2.9) |
| Widowed | 1 (1.4) | 7 (5.1) |
| Parents of children (%) * | 33 (45.2) | 32 (23.2) |
| Level of education (%) * | ||
| >13 years (graduated) | 24 (32.9) | 96 (69.6) |
| Socio-economic status (%) | ||
| High–upper middle income | 39 (53.4) | 56 (40.6) |
| Middle–low income | 27 (40.2) | 57 (41.3) |
| Struggling financially | 7 (9.6) | 25 (18.1) |
| Variables | Workers (n = 73) | Non-Workers (n = 138) |
|---|---|---|
| Complex management of family life and work during COVID-19 pandemic (%) | 31 (42.5) | 77 (55.8) |
| Infection with COVID-19 (%) | 9 (12.3) | 12 (8.7) |
| Refusal of COVID-19 vaccination (%) | 6 (8.2) | 10 (7.2) |
| Loss of someone close due to COVID-19 (%) * | 7 (9.6) | 21 (15.2) |
| Subjected to the 2009 L’Aquila earthquake (%) (n = 100) * | 45 (61.6) | 55 (39.9) |
| Loss of someone close during the 2009 L’Aquila earthquake (%) (n = 100) | 5 (11.1) | 10 (18.2) |
| Severe impact of 2009 L’Aquila earthquake (%) (n = 100 women exposed) (intensity: severe; very severe) | ||
| Family life | 21 (46.7) | 27 (49.1) |
| Work | 18 (40) | 13 (23.6) |
| Social life | 21 (46.7) | 22 (40) |
| Severe impairment due to the L’Aquila 2009 earthquake in two out of the three domains investigated (%) (n = 43) * | 22 (30.1) | 21 (15.2) |
| Previous contact with services due to mental health problems (%) (n = 94) | 38 (52.1) | 56 (40.6) |
| Mental health problems reported (%) | ||
| Anxiety | 20 (27.4) | 40 (29) |
| Family and interpersonal problems | 13 (17.8) | 26 (18.8) |
| Depression | 14 (19.2) | 23 (16.7) |
| Sleep disorders | 9 (12.3) | 15 (10.9) |
| Eating disorders | 10 (13.7) | 12 (8.7) |
| Substance abuse | -- | 3 (2.2) |
| Other problems | 5 (6.8) | 14 (10.1) |
| Treatments | ||
| Admission to a psychiatric ward | -- | 2 (3.5) |
| Psychopharmacological treatment (n = 39) | 11 | 28 |
| Type of drug | ||
| Anxiolytic drugs | 4 (36.4) | 8 (28.6) |
| Antidepressant drugs | 6 (54.5) | 14 (50) |
| Antipsychotic drugs | 1 (9.1) | 6 (21.4) |
| Variables | Total Sample (n = 211) | Workers (n = 73) | Non-Workers (n = 138) |
|---|---|---|---|
| PHQ-9 total mean score (SD) * | 9.5 (6.17) | 7.82 (5.7) | 10.30 (6.2) |
| PHQ-9 total score > 10 (%) * | 82 (40.2) | 19 (26) | 63 (45.7) |
| PHQ-9 score 1–5—absent–mild depression (%) | 64 (30.3) | 28 (38.4) | 36 (26.1) |
| PHQ-9 score 6–10—moderate depression (%) | 65 (30.8) | 26 (35.6) | 39 (28.3) |
| PHQ-9 score 11–15—moderately severe depression (%) | 44 (20.9) | 9 (20.5) | 35 (25.4) |
| PHQ-9 score > 15—severe depression (%) | 38 (18) | 10 (26.3) | 28 (20.3) |
| Family Functioning Questionnaire (SD) | |||
| Communication * | 23.3 (4.8) | 24.9 (4.7) | 22.5 (4.6) |
| Problem solving * | 21.0 (6.7) | 23.6 (6.0) | 19.7 (6.7) |
| Personal goals * | 23.8 (3.9) | 22.3 (3.8) | 24.5 (3.8) |
| Variables Included | Non-Caregivers (n = 164) | Caregivers (n = 47) |
|---|---|---|
| Age, mean (SD) | 35.3 (18.5) | 37.0 (18.8) |
| Range age | ||
| Young adults (18–35 years) (%) | 100 (61) | 26 (55.3) |
| Adults (%) | 51 (31.1) | 18 (38.3) |
| Over 65 (%) | 13 (7.9) | 3 (6.4) |
| Nationality (%) | ||
| Non-EU citizens | 7 (4.3) | 1 (2.1) |
| Marital status (%) | ||
| Single | 72 (43.9) | 21 (44.7) |
| Married/partnership | 76 (46.3) | 23 (48.9) |
| Separated/ divorced | 8 (4.9) | 3 (6.4) |
| Widowed | 8 (4.9) | -- |
| Parents of children (%) | ||
| No children | 118 (71.3) | 29 (61.7) |
| 1 child | 15 (9.2) | 8 (17.0) |
| 2 children | 23 (14.1) | 6 (12.7) |
| 3 children | 8 (4.2) | 4 (10.6) |
| Level of education (%) | ||
| >13 years (graduated) | 70 (42.3) | 21 (44.7) |
| Working conditions (%) | ||
| Self-employed/freelancers | 15 (9.1) | 8 (17.0) |
| Full-time work | 32 (19.5) | 3 (6.4) |
| Part-time work | 11 (6.7) | 4 (8.5) |
| Student | 72 (43.9) | 19 (40.4) |
| Housewife | 9 (5.5) | 4 (8.5) |
| Unemployed | 9 (5.5) | 3 (6.4) |
| Retired | 16 (9.8) | 6 (12.8) |
| Socio-economic status (%) | ||
| High–upper middle income | 75 (45.7) | 20 (42.6) |
| Middle–low income | 66 (40.2) | 18 (38.3) |
| Struggling financially | 23 (14.0) | 9 (19.1) |
| Variables | Non-Caregivers (n = 164) | Caregivers (n = 47) |
|---|---|---|
| Complex management of family life and work during COVID-19 pandemic (%) | 86 (52.4) | 22 (46.8) |
| COVID-19 infection (%) | 16 (9.8) | 5 (10.6) |
| Refusal of COVID-19 vaccination (%) | 11 (6.7) | 5 (10.6) |
| Loss of someone close due to COVID-19 (%) * | 17 (10.4) | 11 (23.4) |
| Subjected to 2009 L’Aquila earthquake (%) (n = 100) | 77 (47) | 23 (48.9) |
| Loss of someone close during the 2009 L’Aquila earthquake (%) | 12 (15.5) | 3 (13) |
| Severe impact of 2009 L’Aquila earthquake (%) (n = 100 women exposed) (intensity: severe; very severe) | ||
| Family life | 37 (48) | 11 (47.8) |
| Work | 25 (32.4) | 6 (26.1) |
| Social life | 32 (41.5) | 11 (47.8) |
| Severe impairment due to the 2009 L’Aquila earthquake in two out of the three domains investigated (%) (n = 43) | 33 (42.9) | 10 (43.5) |
| Previous contact with services due to mental health problems (%) (n = 94) | 71 (43.3) | 23 (48.9) |
| Mental health problems reported (%) | ||
| Anxiety | 42 (25.6) | 18 (38.3) |
| Family and interpersonal problems | 28 (17.1) | 11 (23.4) |
| Depression | 27 (16.5) | 10 (21.3) |
| Sleep disorders | 16 (9.8) | 8 (17) |
| Eating disorders | 17 (10.4) | 5 (10.6) |
| Substance abuse | 1 (0.6) | 2 (4.3) |
| Other problems | 16 (9.8) | 3 (6.4) |
| Treatments | ||
| Admission to a psychiatric ward | 1 | 1 |
| Integrated treatment (drug prescription + psychotherapy) | 14 (8.5) | 7 (14.8) |
| Psychopharmacological treatment (n = 39) | 29 | 10 |
| Type of drug | ||
| Anxiolytic drugs | 10 (34.5) | 2 (20) |
| Antidepressant drugs | 16 (55.2) | 4 (40) |
| Antipsychotic drugs | 3 (10.3) | 4 (40) |
| Variables | Non-Caregivers (n = 164) | Caregivers (n = 47) |
|---|---|---|
| PHQ-9 total mean score (SD) | 9.07 (5.8) | 11 (7.1) |
| PHQ-9 total score > 10 (%) | 59 (37.1) | 23 (51.1) |
| PHQ-9 score 1–5—absent–mild depression (%) | 51 (31.1) | 13 (27.7) |
| PHQ-9 score 6–10—moderate depression (%) | 54 (32.9) | 11 (23.4) |
| PHQ-9 score 11–15—moderately severe depression | 35 (21.3) | 9 (19.1) |
| PHQ-9 score > 15—severe depression (%) | 24 (14.6) | 14 (29.8) |
| Family Functioning Questionnaire (SD) | ||
| Communication | 23.5 (4.4) | 22.7 (5.7) |
| Problem solving | 21.4 (6.6) | 19.8 (7.1) |
| Personal goals | 24.0 (3.8) | 23.0 (4.3) |
| Physical Disability Caregivers (n = 23) | Mental Disability Caregivers (n = 24) | |
|---|---|---|
| Family Functioning | ||
| Communication | 22.6 (6.5) | 22.8 (5.1) |
| Problem solving | 20.6 (4.3) | 19.0 (6.5) |
| Personal goals | 22.9 (4.6) | 23.0 (4.1) |
| Burden of care | ||
| Objective burden | 1.79 (0.50) | 1.86 (0.41) |
| Subjective burden * | 2.00 (0.54) | 2.64 (0.70) |
| Support received from professionals | 2.43 (0.92) | 2.51 (0.68) |
| Support received from relatives and friends * | 2.24 (0.98) | 2.80 (0.69) |
| Measures | Age | 1 | 2 | 3 | 4 | 5 | 6 | 7 | 8 | 9 | 10 | 11 | 12 | 13 |
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| 1. Education, years | 0.304 ** | -- | ||||||||||||
| 2. SF-36 GH | 0.245 ** | 0.143 * | -- | |||||||||||
| 3. SF-36 MH | 0.413 ** | 0.202 ** | 0.512 ** | -- | ||||||||||
| 4. SF-36 RE | 0.380 ** | 0.322 ** | 0.451 ** | 0.628 ** | -- | |||||||||
| 5. SF-36 VT | 0.419 ** | 0.204 ** | 0.590 ** | 0.835 ** | 0.646 ** | -- | ||||||||
| 6. SF-36 SF | 0.412 ** | 0.214 ** | 0.542 ** | 0.755 ** | 0.611 ** | 0.697 ** | -- | |||||||
| 7. PHQ9 total score | 0.452 ** | −0.310 ** | −0.560 ** | −0.836 ** | −0.681 ** | −0.799 ** | −0.738 ** | -- | ||||||
| 8. FPQ, objective burden of care | −0.171 | −0.0151 | −0.384 ** | −0.207 | −0.354 * | −0.337 * | −0.300 * | 0.332 * | -- | |||||
| 9. FPQ, subjective burden of care | −0.076 | −0.011 | −0.292 * | −0.545 ** | −0.391 ** | −0.631 ** | −0.550 ** | 0.501 ** | 0.563 ** | -- | ||||
| 10. FPQ, (lack of) support from relatives and friends | 0.020 | −0.179 | −0.207 | −0.342 * | −0.155 | −0.412 ** | −0.231 | 0.303 * | 0.232 | 0.304 * | -- | |||
| 11. FPQ, (lack of) professional support | −0.031 | −0.186 | −0.236 | −0.200 | −0.139 | −0.336 * | −0.199 | 0.301 * | 0.007 | 0.155 | 0.580 ** | -- | ||
| 12. FFQ, problem solving | 0.434 ** | 0.291 ** | 0.422 ** | 0.519 ** | 0.399 * | 0.556 ** | 0.529 ** | −0.569 ** | −0.130 | −0.110 | −0.465 ** | −0.453 ** | -- | |
| 13. FFQ, communication | 0.382 ** | 0.214 ** | 0.404 ** | 0.442 ** | 0.324 ** | 0.460 ** | 0.433 ** | −0.472 ** | −0.290 * | −0.291 * | −0.373 ** | −0.309 * | 0.733 ** | -- |
| 14. FFQ, personal Goals | −0.147 * | −0.167 * | 0.350 ** | 0.208 ** | 0.131 | 0.233 ** | 0.277 ** | −0.209 ** | −0.261 | −0.300 * | −0.403 ** | −0.315 * | 0.171 * | 0.165 * |
| Variables | Categories | B | p | Exp(B) | 95% Confidence Interval for Exp(B) | |
|---|---|---|---|---|---|---|
| Lower Bound | Upper Bound | |||||
| Age | Moderate depression | −0.036 | 0.010 | 0.964 | 0.938 | 0.991 |
| Moderately severe depression | −0.095 | 0.000 | 0.909 | 0.868 | 0.952 | |
| Severe depression | −0.068 | 0.008 | 0.934 | 0.888 | 0.983 | |
| Lack of a stable romantic partnership | Moderate depression | 0.124 | 0.784 | 1132 | 0.465 | 2.756 |
| Moderately severe depression | 1.101 | 0.053 | 3.006 | 0.988 | 9.148 | |
| Severe depression | 1.113 | 0.098 | 3.044 | 0.813 | 11.399 | |
| Less than 13 years of education | Moderate depression | 0.0362 | 0.411 | 1.436 | 0.605 | 3.408 |
| Moderately severe depression | 0.306 | 0.591 | 1.358 | 0.444 | 4.152 | |
| Severe depression | 1.688 | 0.021 | 5.410 | 1.288 | 22.714 | |
| Struggling financially | Moderate depression | −0.427 | 0.579 | 0.652 | 0.144 | 2.952 |
| Moderately severe depression | 0.870 | 0.260 | 2.387 | 0.525 | 10.852 | |
| Severe depression | 1.224 | 0.145 | 3.402 | 0.654 | 17.687 | |
| Previous access to mental health services | Moderate depression | 0.634 | 0.155 | 1.885 | 0.787 | 4.514 |
| Moderately severe depression | 1.956 | 0.001 | 7.070 | 2.288 | 21.842 | |
| Severe depression | 2.391 | 0.000 | 10.923 | 2.908 | 41.020 | |
| Traumatic experience with the 2009 L’Aquila earthquake | Moderate depression | 1.369 | 0.013 | 3.932 | 1.332 | 11.612 |
| Moderately severe depression | 2.242 | 0.004 | 9.416 | 2.077 | 42.691 | |
| Severe depression | 1.705 | 0.077 | 5.502 | 0.829 | 36.527 | |
| COVID-19 infection | Moderate depression | 0.239 | 0.742 | 1.270 | 0.307 | 5.248 |
| Moderately severe depression | −0.073 | 0.939 | 0.930 | 0.143 | 6.039 | |
| Severe depression | −0.483 | 0.651 | 0.617 | 0.076 | 5.008 | |
| Complex life management during the COVID-19 pandemic | Moderate depression | 0.533 | 0.221 | 1.705 | 0.726 | 4.003 |
| Moderately severe depression | 1.086 | 0.046 | 2.964 | 1.018 | 8.628 | |
| Severe depression | 1.280 | 0.045 | 3.598 | 1.026 | 12.616 | |
| Caregiving for a loved one | Moderate depression | −0.129 | 0.821 | 0.879 | 0.287 | 2.693 |
| Moderately severe depression | 0.304 | 0.652 | 1.355 | 0.362 | 5.075 | |
| Severe depression | 1.058 | 0.150 | 2.880 | 0.683 | 12.147 | |
| Problem solving | Moderate depression | −0.093 | 0.096 | 0.912 | 0.817 | 1.017 |
| Moderately severe depression | −0.164 | 0.010 | 0.849 | 0.750 | 0.961 | |
| Severe depression | −0.234 | 0.001 | 0.791 | 0.686 | 0.912 | |
| Communication | Moderate depression | −0.095 | 0.192 | 0.909 | 0.788 | 1.049 |
| Moderately severe depression | −0.029 | 0.726 | 0.971 | 0.824 | 1.145 | |
| Severe depression | −0.124 | 0.189 | 0.883 | 0.734 | 1.063 | |
| Personal goals | Moderate depression | −0.100 | 0.100. | 0.905 | 0.803 | 1.019 |
| Moderately severe depression | −0.127 | 0.105 | 0.881 | 0.756 | 1.027 | |
| Severe depression | −0.222 | 0.012 | 0.801 | 0.674 | 0.952 | |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Giusti, L.; Mammarella, S.; Del Vecchio, S.; Salza, A.; Casacchia, M.; Roncone, R. Deepening Depression in Women Balancing Work–Life Responsibilities and Caregiving during the COVID-19 Pandemic: Findings from Gender-Specific Face-to-Face Street Interviews Conducted in Italy. Behav. Sci. 2023, 13, 892. https://doi.org/10.3390/bs13110892
Giusti L, Mammarella S, Del Vecchio S, Salza A, Casacchia M, Roncone R. Deepening Depression in Women Balancing Work–Life Responsibilities and Caregiving during the COVID-19 Pandemic: Findings from Gender-Specific Face-to-Face Street Interviews Conducted in Italy. Behavioral Sciences. 2023; 13(11):892. https://doi.org/10.3390/bs13110892
Chicago/Turabian StyleGiusti, Laura, Silvia Mammarella, Sasha Del Vecchio, Anna Salza, Massimo Casacchia, and Rita Roncone. 2023. "Deepening Depression in Women Balancing Work–Life Responsibilities and Caregiving during the COVID-19 Pandemic: Findings from Gender-Specific Face-to-Face Street Interviews Conducted in Italy" Behavioral Sciences 13, no. 11: 892. https://doi.org/10.3390/bs13110892
APA StyleGiusti, L., Mammarella, S., Del Vecchio, S., Salza, A., Casacchia, M., & Roncone, R. (2023). Deepening Depression in Women Balancing Work–Life Responsibilities and Caregiving during the COVID-19 Pandemic: Findings from Gender-Specific Face-to-Face Street Interviews Conducted in Italy. Behavioral Sciences, 13(11), 892. https://doi.org/10.3390/bs13110892