

The Association of Asthma with Anxiety, Depression, and Mild Cognitive Impairment among Middle-Aged and Elderly Individuals in Saudi Arabia
 , , ,
, , ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design and Setting
2.2. Population
2.3. Study Procedure
2.4. Study Instruments
2.4.1. Anxiety and Depression Assessment
2.4.2. Cognitive Function Assessment
2.4.3. Asthma Control Assessment
2.5. Statistical Analysis
3. Results
3.1. Descriptive Statistics
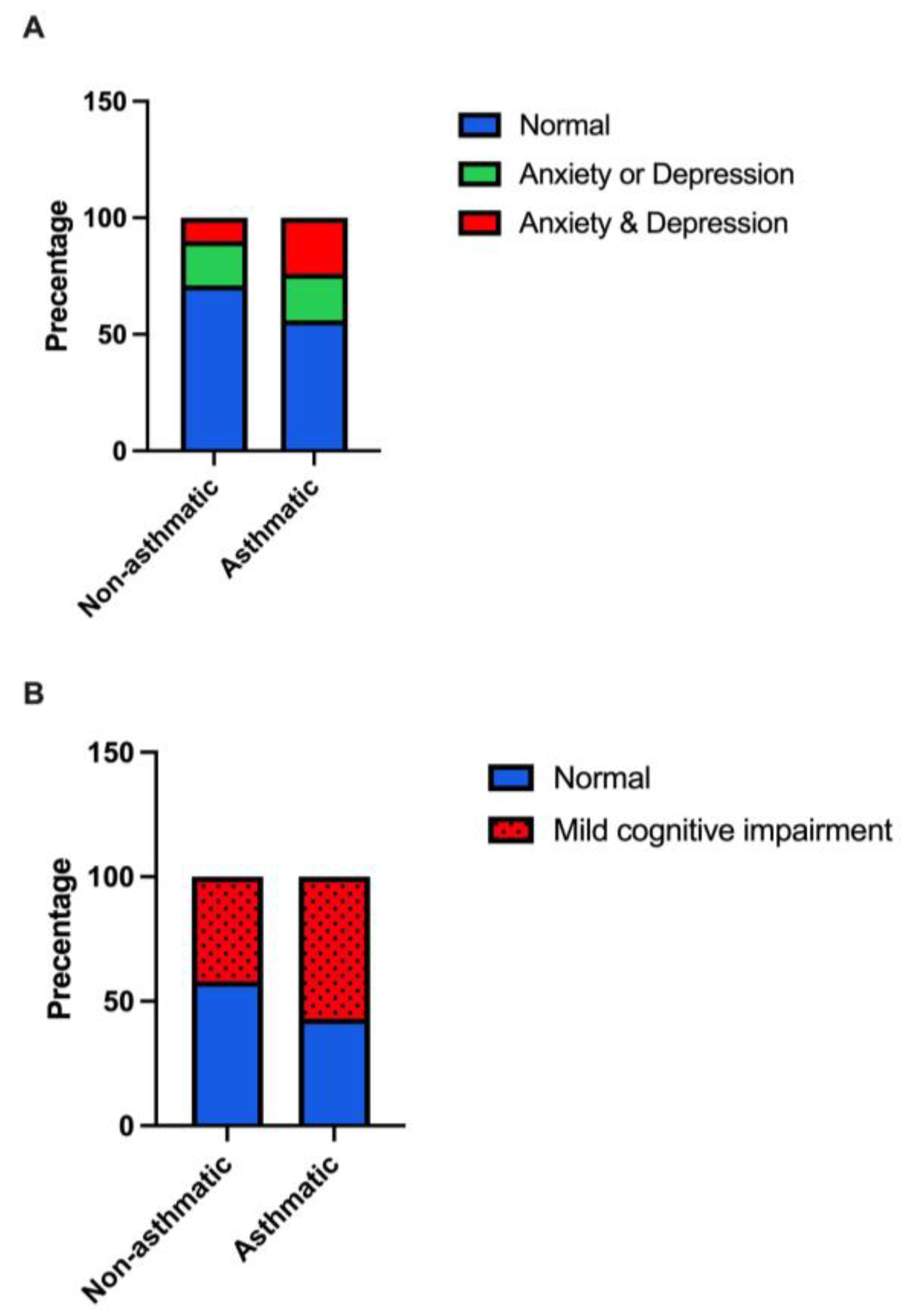
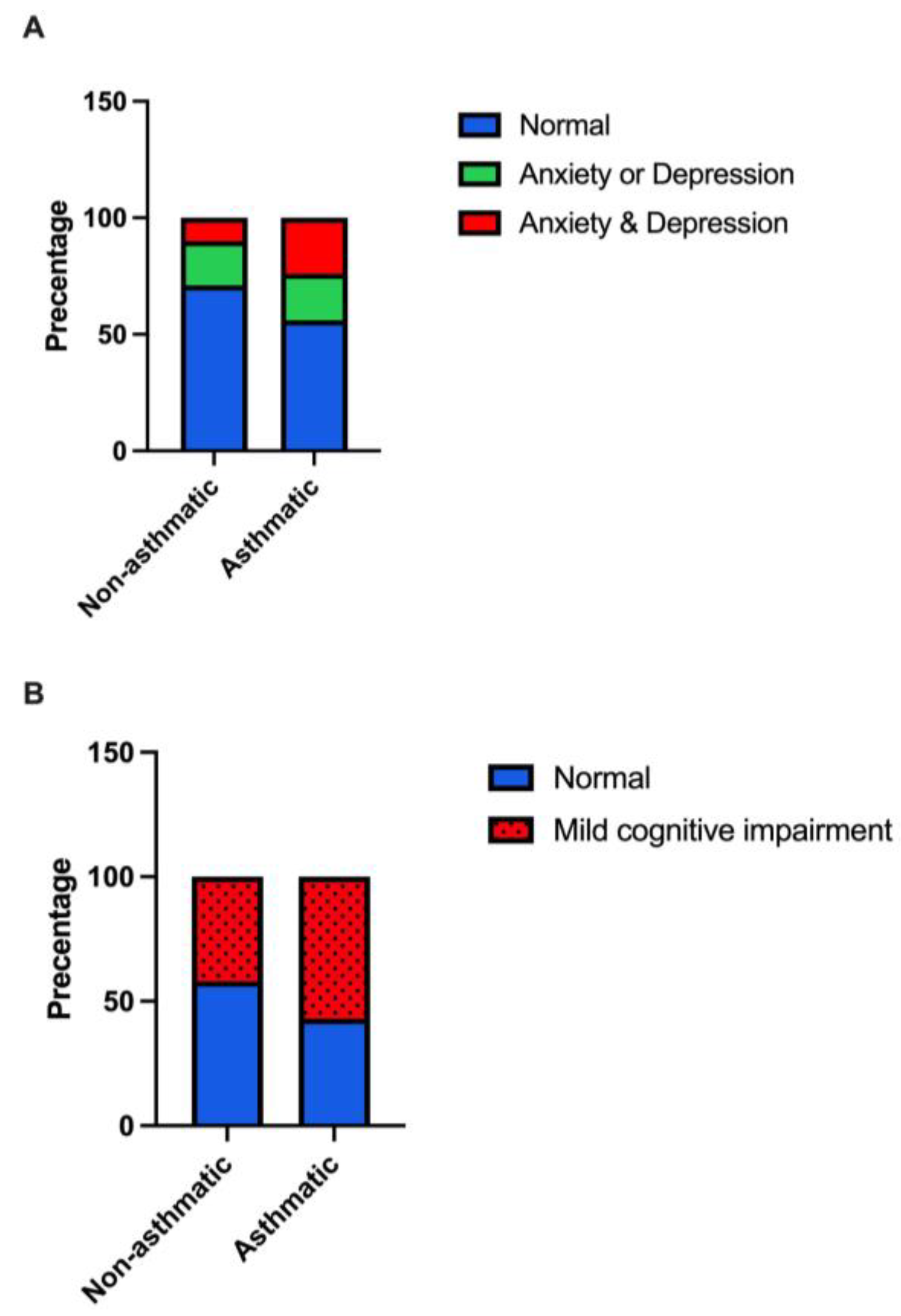
3.2. Asthma Association with Anxiety and Depression
3.3. Asthma Association with Cognition
3.4. Asthma Control Association with Anxiety
3.5. Participants’ Age Interval Moderating the Association between Asthma and Mood and Cognition
4. Discussion
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- The Global Asthma Report 2022. Int. J. Tuberc. Lung Dis. 2022, 26, 1–104. [CrossRef] [PubMed]
- Enilari, O.; Sinha, S. The Global Impact of Asthma in Adult Populations. Ann. Glob. Health 2019, 85, 2. [Google Scholar] [CrossRef] [PubMed]
- Moradi-Lakeh, M.; El Bcheraoui, C.; Daoud, F.; Tuffaha, M.; Kravitz, H.; Al Saeedi, M.; Basulaiman, M.; Memish, Z.A.; AlMazroa, M.A.; Al Rabeeah, A.A.; et al. Prevalence of asthma in Saudi adults: Findings from a national household survey, 2013. BMC Pulm. Med. 2015, 15, 77. [Google Scholar] [CrossRef] [PubMed]
- Al Ghobain, M.O.; Algazlan, S.S.; Oreibi, T.M. Asthma prevalence among adults in Saudi Arabia. Saudi Med. J. 2018, 39, 179–184. [Google Scholar] [CrossRef]
- Hosang, L.; Canals, R.C.; van der Flier, F.J.; Hollensteiner, J.; Daniel, R.; Flügel, A.; Odoardi, F. The lung microbiome regulates brain autoimmunity. Nature 2022, 603, 138–144. [Google Scholar] [CrossRef]
- Greve, H.J.; Dunbar, A.L.; Lombo, C.G.; Ahmed, C.; Thang, M.; Messenger, E.J.; Mumaw, C.L.; Johnson, J.A.; Kodavanti, U.P.; Oblak, A.L.; et al. The bidirectional lung brain-axis of amyloid-β pathology: Ozone dysregulates the peri-plaque microenvironment. Brain 2023, 146, 991–1005. [Google Scholar] [CrossRef]
- Rosenkranz, M.A.; Evans, M.D.; Mumford, J.A.; Esnault, S.; Davidson, R.J.; Busse, W.W. The Effect of Asthma on Activation of Brain Neurocircuits. J. Allergy Clin. Immunol. 2019, 143, AB7. [Google Scholar] [CrossRef]
- Rosenkranz, M.A.; Busse, W.W.; Sheridan, J.F.; Crisafi, G.M.; Davidson, R.J. Are There Neurophenotypes for Asthma? Functional Brain Imaging of the Interaction between Emotion and Inflammation in Asthma. PLoS ONE 2012, 7, e40921. [Google Scholar] [CrossRef]
- Nair, A.K.; Van Hulle, C.A.; Bendlin, B.B.; Zetterberg, H.; Blennow, K.; Wild, N.; Kollmorgen, G.; Suridjan, I.; Busse, W.W.; Dean, D.C.; et al. Impact of asthma on the brain: Evidence from diffusion MRI, CSF biomarkers and cognitive decline. Brain Commun. 2023, 5, fcad180. [Google Scholar] [CrossRef]
- Wang, T.; Huang, X.; Wang, J. Asthma’s effect on brain connectivity and cognitive decline. Front. Neurol. 2023, 13, 1065942. [Google Scholar] [CrossRef]
- Ye, G.; Baldwin, D.S.; Hou, R. Anxiety in asthma: A systematic review and meta-analysis. Psychol. Med. 2021, 51, 11–20. [Google Scholar] [CrossRef] [PubMed]
- Gao, Y.; Zhao, H.; Zhang, F.; Gao, Y.; Shen, P.; Chen, R.; Zhang, G. The Relationship between Depression and Asthma: A Meta-Analysis of Prospective Studies. PLoS ONE 2015, 10, e0132424. [Google Scholar] [CrossRef] [PubMed]
- Simões Cunha, M.; Amaral, R.; Pereira, A.M.; Almeida, R.; Alves-Correia, M.; Loureiro, C.C.; Lopes, C.; Carvalho, J.; Ribeiro, C.; Vidal, C.; et al. Symptoms of anxiety and depression in patients with persistent asthma: A cross-sectional analysis of the INSPIRERS studies. BMJ Open 2023, 13, e068725. [Google Scholar] [CrossRef] [PubMed]
- Strine, T.W.; Mokdad, A.H.; Balluz, L.S.; Berry, J.T.; Gonzalez, O. Impact of Depression and Anxiety on Quality of Life, Health Behaviors, and Asthma Control Among Adults in the United States with Asthma, 2006. J. Asthma 2008, 45, 123–133. [Google Scholar] [CrossRef]
- Deshmukh, V.M.; Toelle, B.G.; Usherwood, T.; O’grady, B.; Jenkins, C.R. The association of comorbid anxiety and depression with asthma-related quality of life and symptom perception in adults. Respirology 2008, 13, 695–702. [Google Scholar] [CrossRef]
- Yohannes, A.M.; Hanania, N.A. Depression and Anxiety in Adult Patients with Asthma. In Depression and Anxiety in Patients with Chronic Respiratory Diseases; Springer: New York, NY, USA, 2017; pp. 73–84. [Google Scholar]
- Irani, F.; Barbone, J.M.; Beausoleil, J.; Gerald, L. Is asthma associated with cognitive impairments? A meta-analytic review. J. Clin. Exp. Neuropsychol. 2017, 39, 965–978. [Google Scholar] [CrossRef]
- Ren, M.; Feng, M.; Long, Z.; Ma, J.; Peng, X.; He, G. Allergic Asthma-Induced Cognitive Impairment is Alleviated by Dexamethasone. Front. Pharmacol. 2021, 12, 680815. [Google Scholar] [CrossRef]
- Bernhoff, C.; Jespersen, A.E.; Dyhre-Petersen, N.; Klein, D.K.; Miskowiak, K.W.; Porsbjerg, C.M. Cognitive impairment is common in patients with severe astma that are commenced on a biological treatment. Eur. Respir. J. 2022, 60, 4644. [Google Scholar]
- Ray, M.; Sano, M.; Wisnivesky, J.P.; Wolf, M.S.; Federman, A.D. Asthma Control and Cognitive Function in a Cohort of Elderly Adults. J. Am. Geriatr. Soc. 2015, 63, 684–691. [Google Scholar] [CrossRef]
- Rhyou, H.-I.; Nam, Y.-H. Association between cognitive function and asthma in adults. Ann. Allergy Asthma Immunol. 2021, 126, 69–74. [Google Scholar] [CrossRef]
- Carlson, S.M.; Kim, J.; Khan, D.A.; King, K.; Lucarelli, R.T.; McColl, R.; Peshock, R.; Brown, E.S. Hippocampal volume in patients with asthma: Results from the Dallas Heart Study. J. Asthma 2017, 54, 9–16. [Google Scholar] [CrossRef] [PubMed]
- Terkawi, A.; Tsang, S.; AlKahtani, G.; Al-Mousa, S.; Al Musaed, S.; AlZoraigi, U.; Alasfar, E.; Doais, K.; Abdulrahman, A.; Altirkawi, K. Development and validation of Arabic version of the Hospital Anxiety and Depression Scale. Saudi J. Anaesth. 2017, 11, 11. [Google Scholar] [CrossRef] [PubMed]
- Snaith, R.P. The Hospital Anxiety And Depression Scale. Health Qual. Life Outcomes 2003, 1, 29. [Google Scholar] [CrossRef] [PubMed]
- Rahman, T.T.A.; El Gaafary, M.M. Montreal Cognitive Assessment Arabic version: Reliability and validity prevalence of mild cognitive impairment among elderly attending geriatric clubs in Cairo. Geriatr. Gerontol. Int. 2009, 9, 54–61. [Google Scholar] [CrossRef] [PubMed]
- Nasreddine, Z.S.; Phillips, N.A.; Bédirian, V.; Charbonneau, S.; Whitehead, V.; Collin, I.; Cummings, J.L.; Chertkow, H. The Montreal Cognitive Assessment, MoCA: A Brief Screening Tool for Mild Cognitive Impairment. J. Am. Geriatr. Soc. 2005, 53, 695–699. [Google Scholar] [CrossRef] [PubMed]
- Lababidi, H.; Hijaoui, A.; Zarzour, M. Validation of the Arabic version of the asthma control test. Ann. Thorac. Med. 2008, 3, 44. [Google Scholar] [CrossRef] [PubMed]
- Nathan, R.A.; Sorkness, C.A.; Kosinski, M.; Schatz, M.; Li, J.T.; Marcus, P.; Murray, J.J.; Pendergraft, T.B. Development of the asthma control test: A survey for assessing asthma control. J. Allergy Clin. Immunol. 2004, 113, 59–65. [Google Scholar] [CrossRef]
- Soler, X.; Holbrook, J.T.; Gerald, L.B.; Berry, C.E.; Saams, J.; Henderson, R.J.; Sugar, E.; Wise, R.A.; Ramsdell, J.W. Validity of the Asthma Control Test Questionnaire Among Smoking Asthmatics. J. Allergy Clin. Immunol. Pract. 2018, 6, 151–158. [Google Scholar] [CrossRef]
- Kim, H.-Y. Statistical notes for clinical researchers: Assessing normal distribution using skewness and kurtosis. Restor. Dent. Endod. 2013, 38, 52. [Google Scholar] [CrossRef] [PubMed]
- Ghasemi, A.; Zahediasl, S. Normality tests for statistical analysis: A guide for non-statisticians. Int. J. Endocrinol. Metab. 2012, 10, 486–489. [Google Scholar] [CrossRef]
- Pavlidi, P.; Kokras, N.; Dalla, C. Sex Differences in Depression and Anxiety. In Sex Differences in Brain Function and Dysfunction; Springer: Berlin/Heidelberg, Germany, 2022; pp. 103–132. [Google Scholar]
- Lin, K.A.; Choudhury, K.R.; Rathakrishnan, B.G.; Marks, D.M.; Petrella, J.R.; Doraiswamy, P.M. Marked gender differences in progression of mild cognitive impairment over 8 years. Alzheimer’s Dement. Transl. Res. Clin. Interv. 2015, 1, 103–110. [Google Scholar] [CrossRef]
- Sears, M.R.; Greene, J.M.; Willan, A.R.; Wiecek, E.M.; Taylor, D.R.; Flannery, E.M.; Cowan, J.O.; Herbison, G.P.; Silva, P.A.; Poulton, R. A Longitudinal, Population-Based, Cohort Study of Childhood Asthma Followed to Adulthood. N. Engl. J. Med. 2003, 349, 1414–1422. [Google Scholar] [CrossRef] [PubMed]
- Baghdadi, L.R.; Alhassan, M.K.; Alotaibi, F.H.; AlSelaim, K.B.; Alzahrani, A.A.; AlMusaeed, F.F. Anxiety, Depression, and Common Chronic Diseases, and Their Association with Social Determinants in Saudi Primary Care. J. Prim. Care Community Health 2021, 12, 215013272110549. [Google Scholar] [CrossRef] [PubMed]
- Wong, K.O.; Hunter Rowe, B.; Douwes, J.; Senthilselvan, A. Asthma and Wheezing Are Associated with Depression and Anxiety in Adults: An Analysis from 54 Countries. Pulm. Med. 2013, 2013, 929028. [Google Scholar] [CrossRef] [PubMed]
- Stubbs, M.A.; Clark, V.L.; Gibson, P.G.; Yorke, J.; McDonald, V.M. Associations of symptoms of anxiety and depression with health-status, asthma control, dyspnoea, dysfunction breathing and obesity in people with severe asthma. Respir. Res. 2022, 23, 341. [Google Scholar] [CrossRef]
- Del Giacco, S.R.; Cappai, A.; Gambula, L.; Cabras, S.; Perra, S.; Manconi, P.E.; Carpiniello, B.; Pinna, F. The asthma-anxiety connection. Respir. Med. 2016, 120, 44–53. [Google Scholar] [CrossRef]
- Al-Zalabani, A.H.; Almotairy, M.M. Asthma control and its association with knowledge of caregivers among children with asthma. Saudi Med. J. 2020, 41, 733–739. [Google Scholar] [CrossRef]
- BinSaeed, A.A. Asthma control among adults in Saudi Arabia. Saudi Med. J. 2015, 36, 599–604. [Google Scholar] [CrossRef]
- AL-Jahdali, H.; Wali, S.; Salem, G.; Al-Hameed, F.; Almotair, A.; Zeitouni, M.; Aref, H.; Nadama, R.; Algethami, M.; Al Ghamdy, A.; et al. Asthma control and predictive factors among adults in Saudi Arabia: Results from the Epidemiological Study on the Management of Asthma in Asthmatic Middle East Adult Population study. Ann. Thorac. Med. 2019, 14, 148. [Google Scholar] [CrossRef]
- Ritz, T.; Kroll, J.L.; Aslan, S.; Janssens, T.; Khan, D.A.; Pinkham, A.E.; Brown, E.S. Subcortical gray matter volumes in asthma: Associations with asthma duration, control, and anxiety. Brain Imaging Behav. 2020, 14, 2341–2350. [Google Scholar] [CrossRef]
- Janssens, T.; Verleden, G.; De Peuter, S.; Van Diest, I.; Van den Bergh, O. Inaccurate perception of asthma symptoms: A cognitive–affective framework and implications for asthma treatment. Clin. Psychol. Rev. 2009, 29, 317–327. [Google Scholar] [CrossRef] [PubMed]
- Favreau, H.; Bacon, S.L.; Labrecque, M.; Lavoie, K.L. Prospective Impact of Panic Disorder and Panic-Anxiety on Asthma Control, Health Service Use, and Quality of Life in Adult Patients with Asthma Over a 4-Year Follow-Up. Psychosom. Med. 2014, 76, 147–155. [Google Scholar] [CrossRef] [PubMed]
- Sastre, J.; Crespo, A.; Fernandez-Sanchez, A.; Rial, M.; Plaza, V.; González, F.C.; López, J.J.; Riaza, M.M.; Orenes, M.M.; Montaño, P.P.; et al. Anxiety, Depression, and Asthma Control: Changes After Standardized Treatment. J. Allergy Clin. Immunol. Pract. 2018, 6, 1953–1959. [Google Scholar] [CrossRef]
- Cooley, C.; Park, Y.; Ajilore, O.; Leow, A.; Nyenhuis, S.M. Impact of interventions targeting anxiety and depression in adults with asthma. J. Asthma 2022, 59, 273–287. [Google Scholar] [CrossRef] [PubMed]
- Bonnert, M.; Andersson, E.; Serlachius, E.; Manninen, I.; Bergström, S.; Almqvist, C. Exposure-based cognitive behavior therapy for anxiety related to asthma: A feasibility study with multivariate baseline design. Scand. J. Psychol. 2020, 61, 827–834. [Google Scholar] [CrossRef] [PubMed]
- Engelkes, M.; Janssens, H.M.; de Jongste, J.C.; Sturkenboom, M.C.J.M.; Verhamme, K.M.C. Medication adherence and the risk of severe asthma exacerbations: A systematic review. Eur. Respir. J. 2015, 45, 396–407. [Google Scholar] [CrossRef]
- Toelle, B.G.; Marks, G.B.; Dunn, S.M. Psychological and Medical Characteristics Associated with Non-Adherence to Prescribed Daily Inhaled Corticosteroid. J. Pers. Med. 2020, 10, 126. [Google Scholar] [CrossRef]
- Bosley, C.; Fosbury, J.; Cochrane, G. The psychological factors associated with poor compliance with treatment in asthma. Eur. Respir. J. 1995, 8, 899–904. [Google Scholar] [CrossRef]
- DiMatteo, M.R.; Lepper, H.S.; Croghan, T.W. Depression Is a Risk Factor for Noncompliance with Medical Treatment. Arch. Intern. Med. 2000, 160, 2101. [Google Scholar] [CrossRef]
- Thoren, C.; Petermann, F. Reviewing asthma and anxiety. Respir. Med. 2000, 94, 409–415. [Google Scholar] [CrossRef]
- Alkhunizan, M.; Alkhenizan, A.; Basudan, L. Prevalence of Mild Cognitive Impairment and Dementia in Saudi Arabia: A Community-Based Study. Dement. Geriatr. Cogn. Dis. Extra 2018, 8, 98–103. [Google Scholar] [CrossRef] [PubMed]
- Battaglia, S.; Sandrini, M.C.; Catalano, F.; Arcoleo, G.; Giardini, G.; Vergani, C.; Bellia, V. Effects of aging on sensation of dyspnea and health-related quality of life in elderly asthmatics. Aging Clin. Exp. Res. 2005, 17, 287–292. [Google Scholar] [CrossRef] [PubMed]
- Kroll, J.L.; Steele, A.M.; Pinkham, A.E.; Choi, C.; Khan, D.A.; Patel, S.V.; Chen, J.R.; Aslan, S.; Sherwood Brown, E.; Ritz, T. Hippocampal metabolites in asthma and their implications for cognitive function. NeuroImage Clin. 2018, 19, 213–221. [Google Scholar] [CrossRef] [PubMed]
- Frieri, M.; O’Connor, M.; Nassef, M. Asthma, stress, and depression in women. Allergy Asthma Proc. 2015, 36, 256–261. [Google Scholar] [CrossRef]
- Jorm, A.F. Does old age reduce the risk of anxiety and depression? A review of epidemiological studies across the adult life span. Psychol. Med. 2000, 30, 11–22. [Google Scholar] [CrossRef]
- Potvin, O.; Forget, H.; Grenier, S.; Préville, M.; Hudon, C. Anxiety, Depression, and 1-Year Incident Cognitive Impairment in Community-Dwelling Older Adults. J. Am. Geriatr. Soc. 2011, 59, 1421–1428. [Google Scholar] [CrossRef]
- Ahn, S.; Mathiason, M.A.; Yu, F. Longitudinal Cognitive Profiles by Anxiety and Depressive Symptoms in American Older Adults with Subjective Cognitive Decline. J. Nurs. Scholarsh. 2021, 53, 698–708. [Google Scholar] [CrossRef]
- Gulpers, B.J.A.; Oude Voshaar, R.C.; van Boxtel, M.P.J.; Verhey, F.R.J.; Köhler, S. Anxiety as a Risk Factor for Cognitive Decline: A 12-Year Follow-Up Cohort Study. Am. J. Geriatr. Psychiatry 2019, 27, 42–52. [Google Scholar] [CrossRef]

{kind=link}
| Variables | Mean (Range) | Frequency | Percent (%) | |
|---|---|---|---|---|
| Age | 52.3 (40–81) | |||
| Middle age (40–59) | 148 | 75.7 | ||
| Elderly (≥60) | 59 | 24.3 | ||
| BMI | 31 (16.6–50.9) | |||
| Sex | ||||
| Male | 55 | 22.6 | ||
| Female | 188 | 77.4 | ||
| Social status | ||||
| Single | 8 | 3.3 | ||
| Married | 211 | 86.8 | ||
| Divorced | 15 | 6.2 | ||
| Widow | 9 | 3.7 | ||
| Education | ||||
| None | 21 | 8.6 | ||
| Elementary | 19 | 7.8 | ||
| Middle | 15 | 6.2 | ||
| Secondary | 40 | 16.5 | ||
| University | 92 | 37.9 | ||
| Postgraduate | 56 | 23.0 | ||
| Occupation | ||||
| Unemployed | 60 | 24.7 | ||
| Employed | 146 | 60.1 | ||
| Retired | 37 | 15.2 | ||
| Asthmatic | ||||
| Yes | 84 | 34.6 | ||
| No | 159 | 65.4 | ||
| Onset of Asthma | ||||
| <12 years old | 10 | 11.9 | ||
| 12–18 years old | 10 | 11.9 | ||
| >18 years old | 64 | 76.2 | ||
| Asthma Severity | ||||
| Mild | 25 | 29.8 | ||
| Moderate | 43 | 51.2 | ||
| Sever | 16 | 19.0 | ||
| Asthma Control | ||||
| Well-controlled | 40 | 47.6 | ||
| Partially controlled | 15 | 17.9 | ||
| Poorly controlled | 29 | 34.5 | ||
| Chronic health conditions | ||||
| Heart disease | 17 | 7 | ||
| Hypertension | 91 | 37 | ||
| Diabetes | 78 | 32 |
| Variables | Asthmatic (n = 84) | Non-Asthmatic (n = 159) | Total (n = 243) | p-Value b |
|---|---|---|---|---|
| Anxiety | 6.2 ± 4.7 | 4.7 ± 3.5 | 5.2 ± 4.0 | 0.04 |
| Depression | 5.2± 3.9 | 4.1 ± 3.3 | 4.5 ± 3.6 | 0.08 |
| MoCA Test a | 23.7 ± 5.0 | 25.5 ± 3.7 | 24.9 ± 4.2 | 0.06 |
| Variables | Anxiety/Depression | Cognition | ||||
|---|---|---|---|---|---|---|
| Anxiety or Depression | Anxiety and Depression | Mild Cognitive Impairment | ||||
| OR (CI 95%) | p-Value | OR (CI 95%) | p-Value | OR (CI 95%) | p-Value | |
| Age | 0.99 (0.95–1.03) | 0.8 | 0.98 (0.94–1.02) | 0.3 | 1.03 (1.00–1.06) | 0.06 |
| Gender (Female) | 1.33 (0.57–3.10) | 0.5 | 1.80 (0.57- 5.70) | 0.3 | 0.80 (0.41–1.56) | 0.5 |
| BMI | 0.99 (0.93–1.06) | 0.8 | 1.06 (0.99–1.13) | 0.08 | 1.03 (0.98–1.08) | 0.2 |
| Asthma | 1.33 (0.62–2.77) | 0.4 | 2.40 (1.07–5.35) | 0.03 | 1.80 (1.00–3.24) | 0.05 |
| Variables | Anxiety | |||
|---|---|---|---|---|
| Borderline | Case | |||
| OR (CI 95%) | p-Value | OR (CI 95%) | p-Value | |
| Age | 0.95 (0.88–1.02) | 0.1 | 0.96 (0.90–1.03) | 0.2 |
| Gender (Female) | 1.20 (0.21–6.82) | 0.8 | 1.86 (0.19–18.3) | 0.6 |
| BMI | 0.98 (0.89–1.09) | 0.7 | 1.05 (0.96–1.16) | 0.3 |
| Asthma control (Well controlled) | ||||
| Poorly controlled | 0.92 (0.19–4.33) | 0.9 | 4.33 (1.09–17.2) | 0.04 |
| Not well controlled | 1.46 (0.30–7.10) | 0.6 | 1.89 (0.28–12.5) | 0.5 |
| Variables | Anxiety/Depression | Cognition | ||||
|---|---|---|---|---|---|---|
| Anxiety or Depression | Anxiety and Depression | Mild Cognitive Impairment | ||||
| OR (CI 95%) | p-Value | OR (CI 95%) | p-Value | OR (CI 95%) | p-Value | |
| Gender (Female) | 1.33 (0.57–3.08) | 0.5 | 1.80 (0.57–5.70) | 0.3 | 0.80 (0.41–1.56) | 0.5 |
| BMI | 0.99 (0.93–1.05) | 0.8 | 1.06 (0.99–1.13) | 0.08 | 1.03 (0.98–1.08) | 0.2 |
| Asthma age interval (Middle age Non-asthmatic) | ||||||
| Middle age asthmatic | 1.83 (0.80–4.18) | 0.1 | 2.48 (1.00–6.08) | 0.05 | 1.44 (0.74–2.81) | 0.3 |
| Elderly non-asthmatic | 1.61 (0.59–4.37) | 0.3 | 0.73 (0.15–3.53) | 0.7 | 2.07 (0.88–4.82) | 0.09 |
| Elderly asthmatic | 0.77 (0.20–2.96) | 0.7 | 1.60 (0.48–5.36) | 0.4 | 7.39 (2.34–23.31) | 0.001 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Abuaish, S.; Eltayeb, H.; Bepari, A.; Hussain, S.A.; Alqahtani, R.S.; Alshahrani, W.S.; Alqahtani, A.H.; Almegbil, N.S.; Alzahrani, W.N. The Association of Asthma with Anxiety, Depression, and Mild Cognitive Impairment among Middle-Aged and Elderly Individuals in Saudi Arabia. Behav. Sci. 2023, 13, 842. https://doi.org/10.3390/bs13100842
Abuaish S, Eltayeb H, Bepari A, Hussain SA, Alqahtani RS, Alshahrani WS, Alqahtani AH, Almegbil NS, Alzahrani WN. The Association of Asthma with Anxiety, Depression, and Mild Cognitive Impairment among Middle-Aged and Elderly Individuals in Saudi Arabia. Behavioral Sciences. 2023; 13(10):842. https://doi.org/10.3390/bs13100842
Chicago/Turabian StyleAbuaish, Sameera, Huda Eltayeb, Asmatanzeem Bepari, Syed Arif Hussain, Raneem Saad Alqahtani, Waad Saeed Alshahrani, Amjad Hayf Alqahtani, Nada Saad Almegbil, and Wafa Nedal Alzahrani. 2023. "The Association of Asthma with Anxiety, Depression, and Mild Cognitive Impairment among Middle-Aged and Elderly Individuals in Saudi Arabia" Behavioral Sciences 13, no. 10: 842. https://doi.org/10.3390/bs13100842
APA StyleAbuaish, S., Eltayeb, H., Bepari, A., Hussain, S. A., Alqahtani, R. S., Alshahrani, W. S., Alqahtani, A. H., Almegbil, N. S., & Alzahrani, W. N. (2023). The Association of Asthma with Anxiety, Depression, and Mild Cognitive Impairment among Middle-Aged and Elderly Individuals in Saudi Arabia. Behavioral Sciences, 13(10), 842. https://doi.org/10.3390/bs13100842