

Combating Loneliness in Older Adults during the COVID-19 Pandemic: Findings from a Volunteer-Based Program in Greece

 ,
,  , ,
, ,  , and
, and {kind=link}
{kind=link}
Abstract
:1. Introduction
2. Materials and Methods
2.1. Design
2.2. Setting
2.3. The Two Main Pillars of the Friendship at Every Age Program
2.3.1. Loneliness Helpline
2.3.2. Interconnection Part of the Program (IC)
2.4. Measuring the Connection of Daily Loneliness Helpline Calls and Daily COVID-19 Cases
2.4.1. Number of Daily Loneliness Helpline Calls
2.4.2. Number of Daily COVID-19 Cases
2.5. Measurements during the IC Participation
2.5.1. Demographic Characteristics
2.5.2. UCLA Loneliness Scale
2.6. Bioethics
2.7. Statistical Analysis
2.7.1. Evaluation of the Impact on Loneliness
2.7.2. Time Series Models
3. Results
3.1. Number of Calls Received
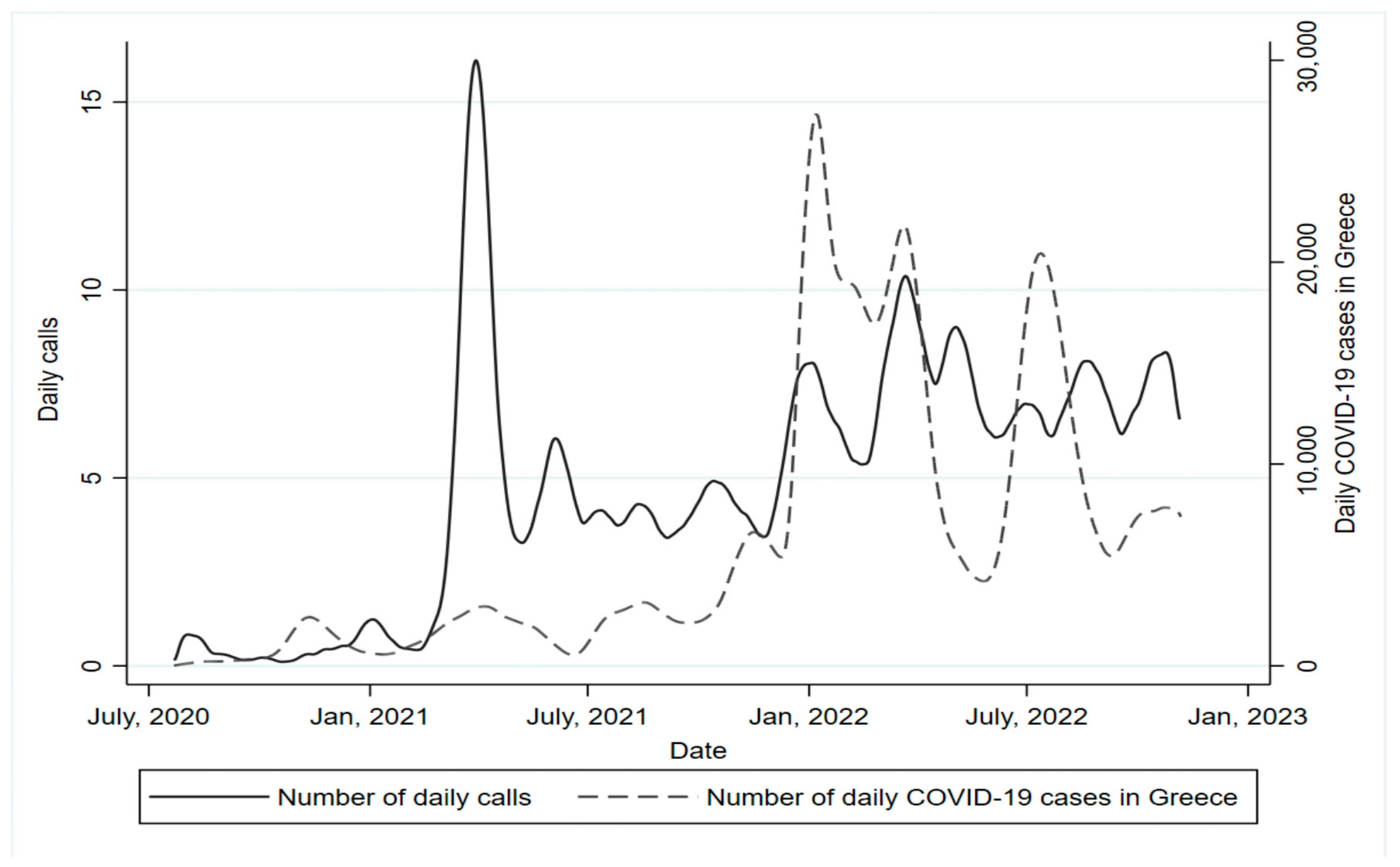
3.2. Calls Received by the Loneliness Helpline and COVID-19 Cases
3.3. Significant Reduction in Loneliness—Interconnection Part
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- CDC COVID-19 Provisional Counts—Weekly Updates by Select Demographic and Geographic Characteristics. Available online: https://www.cdc.gov/nchs/nvss/vsrr/covid_weekly/index.htm#AgeAndSex (accessed on 7 July 2023).
- WHO Older People and COVID-19. Available online: https://www.who.int/teams/social-determinants-of-health/demographic-change-and-healthy-ageing/covid-19 (accessed on 7 July 2023).
- WHO Ageing and Health. Available online: https://www.who.int/news-room/fact-sheets/detail/ageing-and-health (accessed on 7 July 2023).
- Stolz, E.; Mayerl, H.; Freidl, W. The Impact of COVID-19 Restriction Measures on Loneliness among Older Adults in Austria. Eur. J. Public Health 2021, 31, 44–49. [Google Scholar] [CrossRef] [PubMed]
- Triantafillou, E.; Tsellos, P.; Christodoulou, N.; Tzavara, C.; Mrvoljak-Theodoropoulou, I.; Christodoulou, G.N. The Effect of COVID-19 Pandemic on Mental Health and Quality of Life in the Athens Area—Greece. Psychiatriki 2022, 33, 271–282. [Google Scholar] [CrossRef] [PubMed]
- Cho, D.; Cheon, W. Older Adults’ Advance Aging and Life Satisfaction Levels: Effects of Lifestyles and Health Capabilities. Behav. Sci. 2023, 13, 293. [Google Scholar] [CrossRef] [PubMed]
- Donovan, N.J.; Blazer, D. Social Isolation and Loneliness in Older Adults: Review and Commentary of a National Academies Report. Am. J. Geriatr. Psychiatry 2020, 28, 1233–1244. [Google Scholar] [CrossRef]
- Bickerdike, L.; Wilson, P. Interventions for Loneliness and Social Isolation. Cent. Rev. Dissem. Natl. Inst. Health Res. 2014. [Google Scholar]
- Poscia, A.; Stojanovic, J.; La Milia, D.I.; Duplaga, M.; Grysztar, M.; Moscato, U.; Onder, G.; Collamati, A.; Ricciardi, W.; Magnavita, N. Interventions Targeting Loneliness and Social Isolation among the Older People: An Update Systematic Review. Exp. Gerontol. 2018, 102, 133–144. [Google Scholar] [CrossRef]
- Steptoe, A.; Shankar, A.; Demakakos, P.; Wardle, J. Social Isolation, Loneliness, and All-Cause Mortality in Older Men and Women. Proc. Natl. Acad. Sci. USA 2013, 110, 5797–5801. [Google Scholar] [CrossRef]
- Social Isolation and Loneliness in Older Adults: Opportunities for the Health Care System; National Academies Press: Washington, DC, USA, 2020; ISBN 978-0-309-67100-2.
- Tragantzopoulou, P.; Giannouli, V. Social Isolation and Loneliness in Old Age: Exploring Their Role in Mental and Physical Health. Psychiatr. Psychiatr. 2021, 32, 59–66. [Google Scholar] [CrossRef]
- MacLeod, S.; Tkatch, R.; Kraemer, S.; Fellows, A.; McGinn, M.; Schaeffer, J.; Yeh, C.S. COVID-19 Era Social Isolation among Older Adults. Geriatrics 2021, 6, 52. [Google Scholar] [CrossRef]
- Harden, K.; Price, D.M.; Mason, H.; Bigelow, A. COVID-19 Shines a Spotlight on the Age-Old Problem of Social Isolation. J. Hosp. Palliat. Nurs. JHPN Off. J. Hosp. Palliat. Nurses Assoc. 2020, 22, 435–441. [Google Scholar] [CrossRef]
- Smith, M.L.; Steinman, L.E.; Casey, E.A. Combatting Social Isolation Among Older Adults in a Time of Physical Distancing: The COVID-19 Social Connectivity Paradox. Front. Public Health 2020, 8, 403. [Google Scholar] [CrossRef] [PubMed]
- Barbieri, V.; Wiedermann, C.J.; Lombardo, S.; Plagg, B.; Piccoliori, G.; Gärtner, T.; Engl, A. Age-Related Associations of Altruism with Attitudes towards COVID-19 and Vaccination: A Representative Survey in the North of Italy. Behav. Sci. 2023, 13, 188. [Google Scholar] [CrossRef] [PubMed]
- Shah, S.G.S.; Nogueras, D.; van Woerden, H.C.; Kiparoglou, V. The COVID-19 Pandemic: A Pandemic of Lockdown Loneliness and the Role of Digital Technology. J. Med. Internet Res. 2020, 22, e22287. [Google Scholar] [CrossRef] [PubMed]
- Gerst-Emerson, K.; Jayawardhana, J. Loneliness as a Public Health Issue: The Impact of Loneliness on Health Care Utilization among Older Adults. Am. J. Public Health 2015, 105, 1013–1019. [Google Scholar] [CrossRef] [PubMed]
- WHO Greece: WHO Coronavirus Disease (COVID-19) Dashboard with Vaccination Data. Available online: https://covid19.who.int (accessed on 19 August 2023).
- Atzendorf, J.; Gruber, S. Depression and Loneliness of Older Adults in Europe and Israel after the First Wave of COVID-19. Eur. J. Ageing 2022, 19, 849–861. [Google Scholar] [CrossRef]
- Moustakopoulou, L.; Adamakidou, T.; Plakas, S.; Drakopoulou, M.; Apostolara, P.; Mantoudi, A.; Mastrogiannis, D.; Zartaloudi, A.; Parissopoulos, S.; Koreli, A.; et al. Exploring Loneliness, Fear and Depression among Older Adults during the COVID-19 Era: A Cross-Sectional Study in Greek Provincial Towns. Healthcare 2023, 11, 1234. [Google Scholar] [CrossRef]
- Peppou, L.E.; Economou, M.; Skali, T.; Papageorgiou, C. From Economic Crisis to the COVID-19 Pandemic Crisis: Evidence from a Mental Health Helpline in Greece. Eur. Arch. Psychiatry Clin. Neurosci. 2021, 271, 407–409. [Google Scholar] [CrossRef]
- Joosten-Hagye, D.; Katz, A.; Sivers-Teixeira, T.; Yonshiro-Cho, J. Age-Friendly Student Senior Connection: Students’ Experience in an Interprofessional Pilot Program to Combat Loneliness and Isolation among Older Adults during the COVID-19 Pandemic. J. Interprof. Care 2020, 34, 668–671. [Google Scholar] [CrossRef]
- Office, E.E.; Rodenstein, M.S.; Merchant, T.S.; Pendergrast, T.R.; Lindquist, L.A. Reducing Social Isolation of Seniors during COVID-19 through Medical Student Telephone Contact. J. Am. Med. Dir. Assoc. 2020, 21, 948–950. [Google Scholar] [CrossRef]
- Kadowaki, L.; Wister, A. Older Adults and Social Isolation and Loneliness During the COVID-19 Pandemic: An Integrated Review of Patterns, Effects, and Interventions. Can. J. Aging Rev. Can. Vieil. 2023, 42, 199–216. [Google Scholar] [CrossRef]
- Petits Frères des Pauvres La Solitude chez nos aînés est un Véritable Fléau. Available online: https://www.petitsfreresdespauvres.fr/ete (accessed on 7 July 2023).
- National Public Health Organazation Epidemiological Surveillance Reports of SARS-CoV-2; Εθνικός Oργανισμός Δημόσιας Υγείας: 2022. Available online: https://eody.gov.gr/epidimiologika-statistika-dedomena/ektheseis-epidimiologikis-epitirisis-loimoxis-apo-ton-sars-cov-2/imerisies-ektheseis-covid-19-2022/ (accessed on 7 July 2023).
- Russell, D.W. UCLA Loneliness Scale (Version 3): Reliability, Validity, and Factor Structure. J. Pers. Assess. 1996, 66, 20–40. [Google Scholar] [CrossRef] [PubMed]
- Hughes, M.E.; Waite, L.J.; Hawkley, L.C.; Cacioppo, J.T. A Short Scale for Measuring Loneliness in Large Surveys: Results From Two Population-Based Studies. Res. Aging 2004, 26, 655–672. [Google Scholar] [CrossRef] [PubMed]
- Scerri, J.; Sammut, A.; Cilia Vincenti, S.; Grech, P.; Galea, M.; Scerri, C.; Calleja Bitar, D.; Dimech Sant, S. Reaching out for Help: Calls to a Mental Health Helpline Prior to and during the COVID-19 Pandemic. Int. J. Environ. Res. Public. Health 2021, 18, 4505. [Google Scholar] [CrossRef]
- Müller, F.; Röhr, S.; Reininghaus, U.; Riedel-Heller, S.G. Social Isolation and Loneliness during COVID-19 Lockdown: Associations with Depressive Symptoms in the German Old-Age Population. Int. J. Environ. Res. Public. Health 2021, 18, 3615. [Google Scholar] [CrossRef] [PubMed]
- Armitage, R.; Nellums, L.B. COVID-19 and the Consequences of Isolating the Elderly. Lancet Public Health 2020, 5, e256. [Google Scholar] [CrossRef]
- Yoon, H.; Jang, Y.; Vaughan, P.W.; Garcia, M. Older Adults’ Internet Use for Health Information: Digital Divide by Race/Ethnicity and Socioeconomic Status. J. Appl. Gerontol. Off. J. South. Gerontol. Soc. 2020, 39, 105–110. [Google Scholar] [CrossRef]
- Sayin Kasar, K.; Karaman, E. Life in Lockdown: Social Isolation, Loneliness and Quality of Life in the Elderly during the COVID-19 Pandemic: A Scoping Review. Geriatr. Nurs. 2021, 42, 1222–1229. [Google Scholar] [CrossRef]
- Pancani, L.; Marinucci, M.; Aureli, N.; Riva, P. Forced Social Isolation and Mental Health: A Study on 1006 Italians under COVID-19 Lockdown. Front. Psychol. 2021, 12, 663799. [Google Scholar] [CrossRef]
- Humphrey, A.; March, E.; Lavender, A.P.; Miller, K.J.; Alvarenga, M.; Mesagno, C. Buffering the Fear of COVID-19: Social Connectedness Mediates the Relationship between Fear of COVID-19 and Psychological Wellbeing. Behav. Sci. 2022, 12, 86. [Google Scholar] [CrossRef]
- Whatley, M.C.; Siegel, A.L.M.; Schwartz, S.T.; Silaj, K.M.; Castel, A.D. Younger and Older Adults’ Mood and Expectations Regarding Aging During COVID-19. Gerontol. Geriatr. Med. 2020, 6, 2333721420960259. [Google Scholar] [CrossRef]
- Wong, S.Y.S.; Zhang, D.; Sit, R.W.S.; Yip, B.H.K.; Chung, R.Y.-N.; Wong, C.K.M.; Chan, D.C.C.; Sun, W.; Kwok, K.O.; Mercer, S.W. Impact of COVID-19 on Loneliness, Mental Health, and Health Service Utilisation: A Prospective Cohort Study of Older Adults with Multimorbidity in Primary Care. Br. J. Gen. Pract. J. R. Coll. Gen. Pract. 2020, 70, e817–e824. [Google Scholar] [CrossRef] [PubMed]
- Whitehead, B.R.; Torossian, E. Older Adults’ Experience of the COVID-19 Pandemic: A Mixed-Methods Analysis of Stresses and Joys. Gerontologist 2021, 61, 36–47. [Google Scholar] [CrossRef] [PubMed]
- Dykstra, P.A.; van Tilburg, T.G.; Gierveld, J.D.J. Changes in Older Adult Loneliness: Results From a Seven-Year Longitudinal Study. Res. Aging 2005, 27, 725–747. [Google Scholar] [CrossRef]
- Rijken, A.J.; Liefbroer, A.C. Differences in Family Norms for Men and Women Across Europe. J. Marriage Fam. 2016, 78, 1097–1113. [Google Scholar] [CrossRef]
- Krumm, S.; Checchia, C.; Koesters, M.; Kilian, R.; Becker, T. Men’s Views on Depression: A Systematic Review and Metasynthesis of Qualitative Research. Psychopathology 2017, 50, 107–124. [Google Scholar] [CrossRef]
- Seidler, Z.E.; Dawes, A.J.; Rice, S.M.; Oliffe, J.L.; Dhillon, H.M. The Role of Masculinity in Men’s Help-Seeking for Depression: A Systematic Review. Clin. Psychol. Rev. 2016, 49, 106–118. [Google Scholar] [CrossRef]
- Weiss, R. Loneliness: The Experience of Emotional and Social Isolation; MIT Press: Cambridge, MA, USA, 1973; Volume 22. [Google Scholar]
- Savage, R.D.; Wu, W.; Li, J.; Lawson, A.; Bronskill, S.E.; Chamberlain, S.A.; Grieve, J.; Gruneir, A.; Reppas-Rindlisbacher, C.; Stall, N.M.; et al. Loneliness among Older Adults in the Community during COVID-19: A Cross-Sectional Survey in Canada. BMJ Open 2021, 11, e044517. [Google Scholar] [CrossRef]

Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Balta, M.; Katsas, K.; Grigoropoulou, C.; Diamantis, D.V.; Kalogiannis, D.; Drougos, N.; Fagogeni, E.; Veloudaki, A.; Panagiotakos, D.; Linos, A. Combating Loneliness in Older Adults during the COVID-19 Pandemic: Findings from a Volunteer-Based Program in Greece. Behav. Sci. 2023, 13, 804. https://doi.org/10.3390/bs13100804
Balta M, Katsas K, Grigoropoulou C, Diamantis DV, Kalogiannis D, Drougos N, Fagogeni E, Veloudaki A, Panagiotakos D, Linos A. Combating Loneliness in Older Adults during the COVID-19 Pandemic: Findings from a Volunteer-Based Program in Greece. Behavioral Sciences. 2023; 13(10):804. https://doi.org/10.3390/bs13100804
Chicago/Turabian StyleBalta, Marianna, Konstantinos Katsas, Chrysoula Grigoropoulou, Dimitrios V. Diamantis, Dimitrios Kalogiannis, Nikolaos Drougos, Eleni Fagogeni, Afroditi Veloudaki, Demosthenes Panagiotakos, and Athena Linos. 2023. "Combating Loneliness in Older Adults during the COVID-19 Pandemic: Findings from a Volunteer-Based Program in Greece" Behavioral Sciences 13, no. 10: 804. https://doi.org/10.3390/bs13100804
APA StyleBalta, M., Katsas, K., Grigoropoulou, C., Diamantis, D. V., Kalogiannis, D., Drougos, N., Fagogeni, E., Veloudaki, A., Panagiotakos, D., & Linos, A. (2023). Combating Loneliness in Older Adults during the COVID-19 Pandemic: Findings from a Volunteer-Based Program in Greece. Behavioral Sciences, 13(10), 804. https://doi.org/10.3390/bs13100804