
Public Health Safety in Community Living Circles Based on a Behavioral Motivation Perspective: Theoretical Framework and Evaluation System

Abstract
Highlights
- Building a “geographical environment–life activity–public health” model for evaluating health behavior.
- Building a public health safety evaluation system for community living circles.
- A new approach to the theory of “healthy communities” based on direct impact factors.
- The findings can be used in community living circles for “health checks”, and the planning of healthy and safe living circles.
Abstract
1. Introduction
2. Research Theory of Community Life Behavior Motivation and Public Health Safety
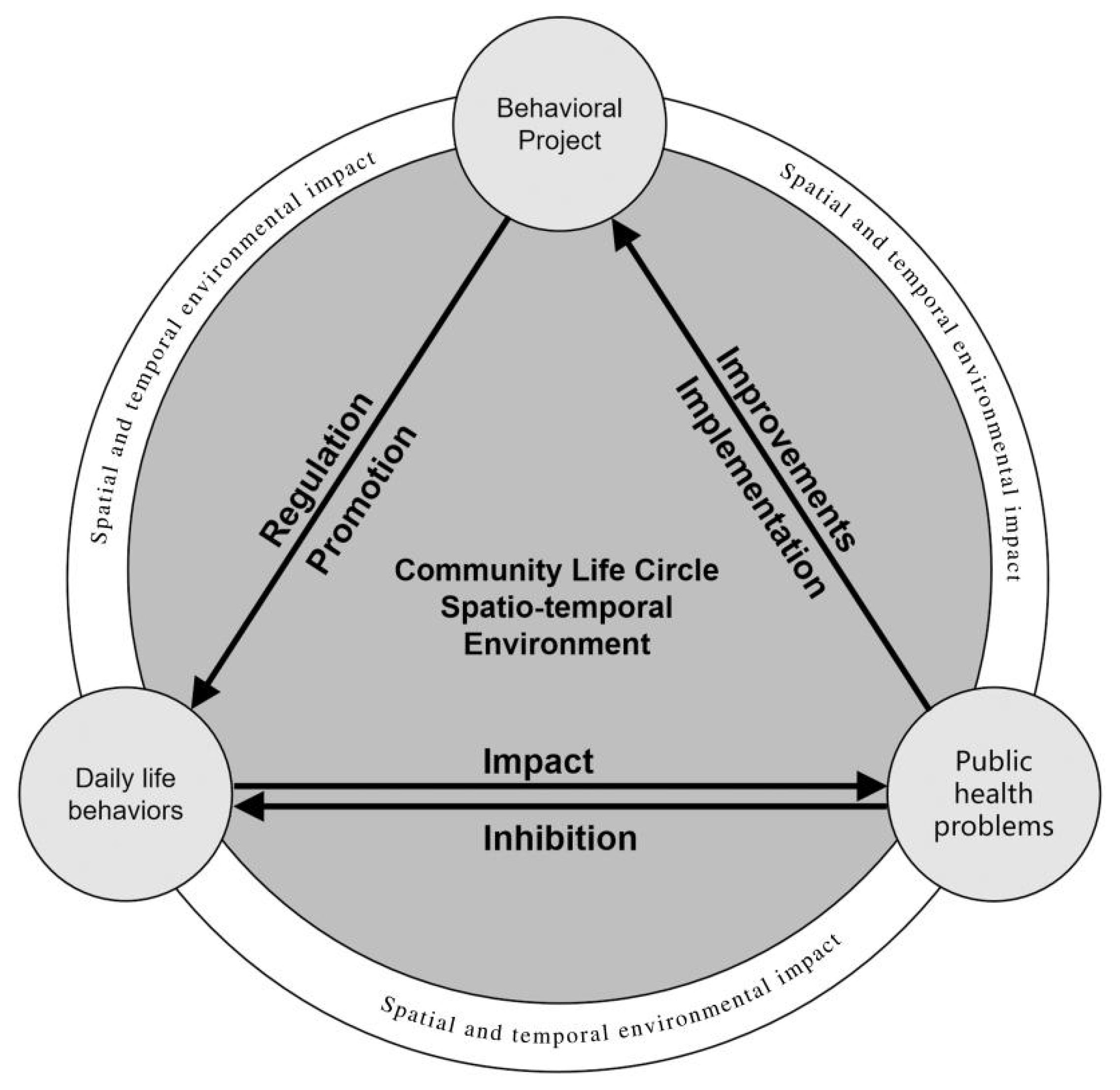
2.1. Behavioral Motivation Theory and CLC Public Health Safety
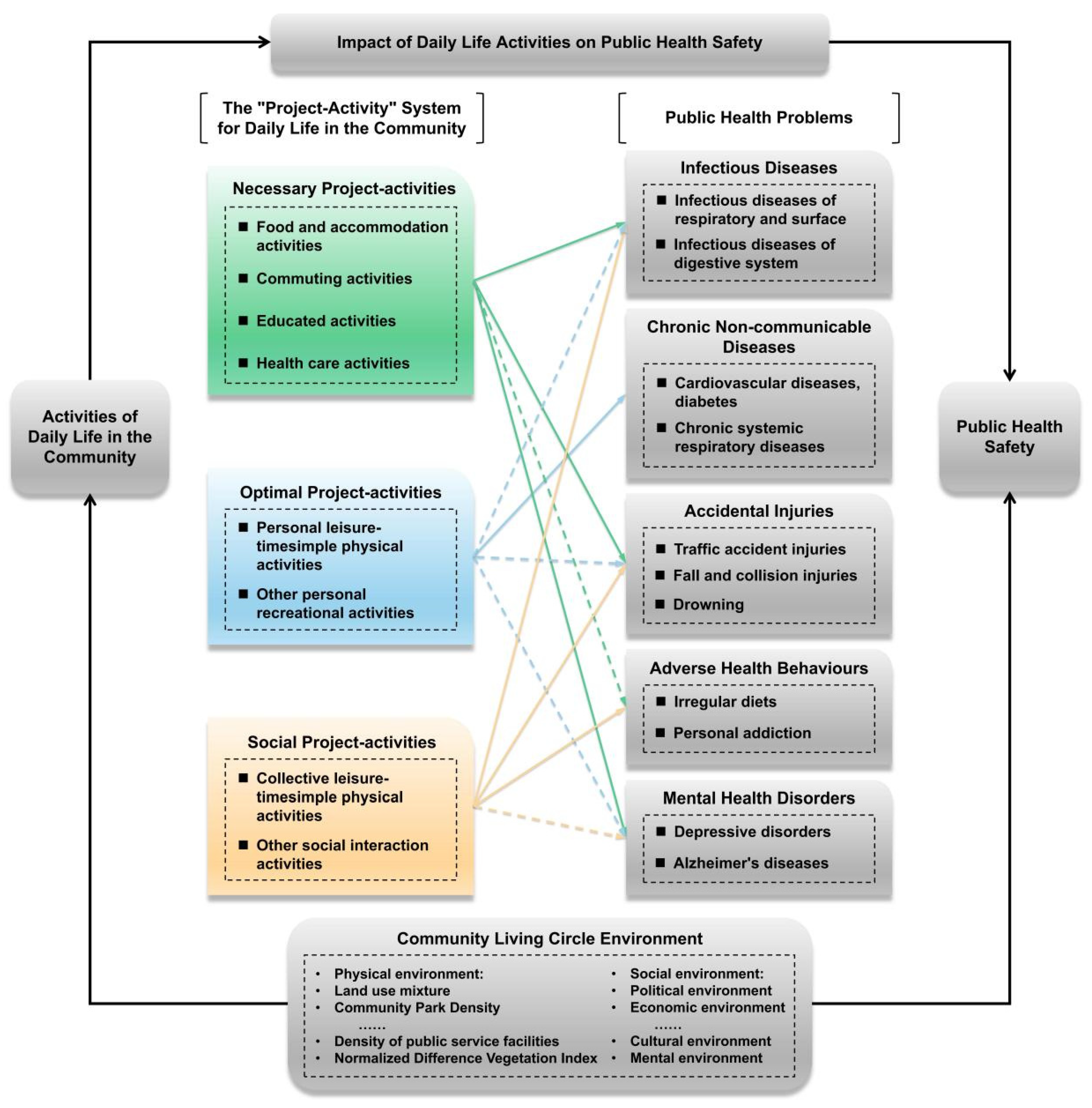
2.2. Types and Relationships between Community Daily Life Activities and Public Health Problems
2.3. Theoretical Framework of CLC Public Health Safety Research
3. CLC Health Behavior Evaluation Method
3.1. Evaluation Theory and Precondition
3.2. Health Behavior Evaluation Model of CLC
4. Construction of CLC Public Health Safety Evaluation System
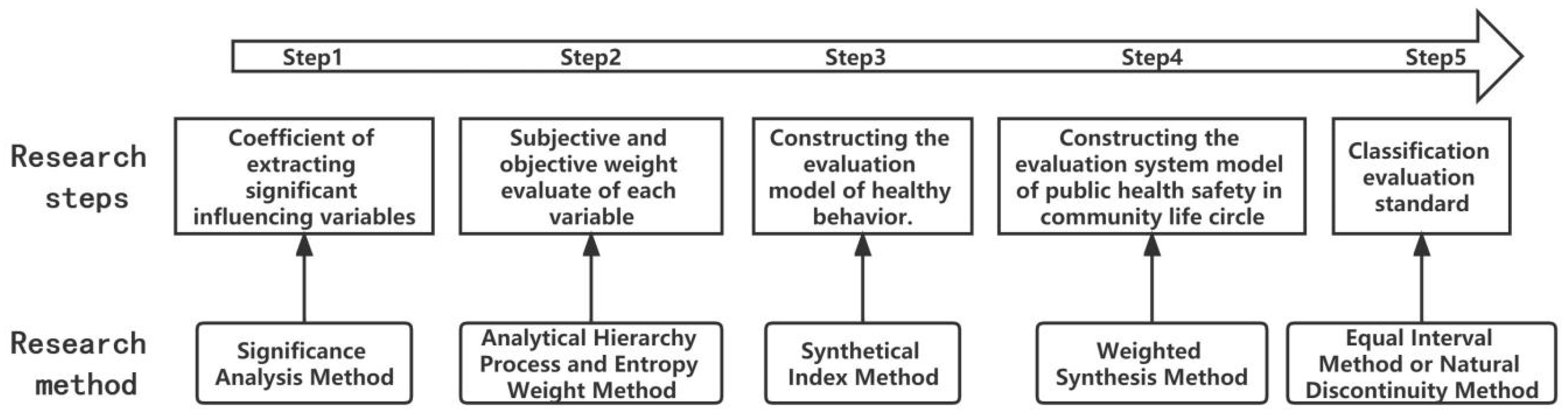
4.1. Public Health Safety Evaluation Steps of CLC
4.2. Public Health Safety Evaluation System of CLC
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Ford, E.S.; Li, C.Y.; Zhao, G.X.; Pearson, W.S.; Tsai, J.; Greenlund, K.J. Trends in low-risk lifestyle factors among adults in the United States: Findings from the Behavioral Risk Factor Surveillance System 1996–2007. Prev. Med. 2010, 51, 403–407. [Google Scholar] [CrossRef] [PubMed]
- Parsamehr, M.; Rasoulinejad, P. Investigating the relationship between health-based lifestyle and social health among people in Talesh. Q. J. Soc. Dev. 2015, 10, 35–66. [Google Scholar]
- Wang, W. Social significance of disease prevention and control. Chin. J. Public Health 2018, 34, 1–3. [Google Scholar]
- Wang, L.D. Healthy Lifestyles and Healthy China 2020. J. Peking Univ. Health Sci. 2010, 42, 245–246. [Google Scholar]
- Zhong, N.S. Health is determined by a healthy lifestyle: Zhong Nanshan on Health (II). China Model 2015, 2, 72–76. [Google Scholar]
- Chai, Y.W.; Shen, Y.; Chen, Z.F. Towards Smarter Cities: Human-oriented Urban Planning and Management Based on Space-Time Behavior Research. Urban Plan. Int. 2014, 6, 31–37+50. [Google Scholar]
- Chen, Z.F.; Chai, Y.W.; Zhou, S.H. A Comparative Studies of Susburban Residents’ Travel Behavior on Weekdays under Different Suburbanization Modes: A Case Analysis of Beijing and Guangzhou. Hum. Geogr. 2015, 2, 23–30. [Google Scholar]
- Zhang, G.Q.; Li, Y.; Lin, T.; Li, X.H.; Wang, L. The healthy community construction from a land senses ecology perspective. Acta Ecol. Sin. 2020, 40, 8130–8140. [Google Scholar]
- Chai, Y.W.; Wu, W.L.; Zhang, W.J.; Li, C.J.; Li, Y.X. A Research Framework of Precise Epidemic Prevention and Control from the Perspective of Space-time Behavioral Geography. Sci. Geogr. Sin. 2020, 40, 1585–1592. [Google Scholar]
- Li, Y.X.; Chai, Y.W.; Ta, N. From Disaster Precaution Life Circle to Safety Life Circle — Japanese Experience and Inspiration for China. Urban Plan. Int. 2022, 37, 113–120. [Google Scholar]
- Hu, H.; Xu, J.G. Progress in Urban Health Geography Using Complexity Theory. Hum. Geogr. 2018, 6, 1–8. [Google Scholar]
- Yu, Y.F.; Hu, Y.T. Progress of International Research on Health Impact of the Built Environment of Communities: Literature Review and Reflections from a Perspective of Physical Activities. Archit. J. 2017, 2, 33–38. [Google Scholar]
- Li, Y.T.; Huang, J.W.; Li, B.X. Built Community Environment Governance with Healthy City Concept: Planning Thinking of Public Health Event in a Vegetable Market. Planners 2020, 36, 107–111. [Google Scholar]
- Yang, Y.; Lin, L.; Zhong, Z.; Ou, Y.; Hao, S. Comprehensive Evaluation and Spatial Differentiation of Community Resilience in Guangzhou Based on Response of the City to Public Health Hazards. Acta Geogr. Sin. 2019, 74, 266–284. [Google Scholar]
- Huang, L.; Luo, J.H.; Song, C.P.; Zhao, C.; Li, Q.; Zhou, M. Community Home System Planning Based on the Concept of Community Life Circle: A Case Study of Cuiyun Area, Liangjiang New District in Chongqing. Urban Plan. Forum 2021, 2, 102–109. [Google Scholar]
- Li, S.Y.; Cai, Z.C.; Tang, J.W. Analysis of the Spatial Layout of Community Medical Facilities from the Perspective of Health Resilience: A Case Study of Nanjing’s Downtown Area. Mod. Urban Res. 2021, 7, 45–52+59. [Google Scholar]
- Yang, S.; Li, H.R.; Li, Y.H.; Wang, W.Y.; Tan, J.A. Progress of Medical Geography and Environmental Health Studies. Prog. Geogr. 2010, 29, 31–44. [Google Scholar]
- Xu, Y.S.; Zhou, D.; Liu, K.J. Research on The Elderly Space–Time Behavior Visualization and Community Healthy Livable Environment. Archit. J. 2019, S1, 90–95. [Google Scholar]
- Tesson, S.; Richards, I.; Porter, D.; Phillips, K.A.; Rankin, N.; Musiello, T.; Marven, M.; Butow, P. Women’s preferences for contralateral prophylactic mastectomy: An investigation using protection motivation theory. Patient Educ. Couns. 2016, 99, 814–822. [Google Scholar] [CrossRef]
- Feng, L.S.; Zhang, L.; Gao, B.H.; Xu, J.F.; Lu, Y.L.; Gao, H.; Ma, F.H.; Fan, R.Y.; Chen, W.H. Effects of Aerobic Exercise in Different Environments on Body Weight and Body Fat Mass of Obese and Overweight Adolescents. China Sport Sci. 2013, 33, 58–65. [Google Scholar]
- Li, B.; Liu, Q.H.; Wang, T.; He, H.; Peng, Y.; Feng, T. Analysis of Urban Built Environment Impacts on Outdoor Physical Activities—A Case Study in China. Front. Public Health 2022, 10, 861456. [Google Scholar] [CrossRef] [PubMed]
- Chen, C.; Chen, Y.; Yu, L.; Zhou, W. Planning for Healthy City: The Influence of the Built Environment on the Body Mass Index of the Elderly. Urban Dev. Stud. 2017, 24, 7–13. [Google Scholar]
- Al-Qahtani, A.M.; Shaikh, M.A.K.; Shaikh, I.A. Exercise as a treatment modality for depression: A narrative review. Alex. J. Med. 2018, 54, 429–435. [Google Scholar] [CrossRef]
- Duan, M.X.; Mo, M.L.; Wang, T.W.; Xiong, H.Y. Compliance and influencing factors of health behavior intervention among community people with prediabetes. J. Army Med. Univ. 2017, 13, 1404–1409. [Google Scholar]
- Bi, N.; Ding, H.; Su, T.J.; Yang, X. Dietary behavior in osteoporosis patients and community health management strategy. Chin. J. Osteoporos. 2017, 4, 452–455+472. [Google Scholar]
- Cao, C.; Zhen, F.; Wang, X.; Jiang, Y.P. Study on the influence of commuting behavior characteristics of urban residents on health in Nanjing City based on structural equation model. Prog. Geogr. 2020, 12, 2043–2053. [Google Scholar] [CrossRef]
- Xu, A.H. Effect of Protective Motivation Theory-based Nursing Intervention on Self-care Ability of Elderly Patients with Chronic Diseases. J. Nurs. 2021, 28, 47–51. [Google Scholar]
- Zohreh, R.; Mohammad, A.M.; Eesa, M. Determinants of cancer early detection behaviors: Application of protection motivation theory. Health Promot. Perspect. 2015, 5, 138–146. [Google Scholar]
- Zhang, Y.J.; Qin, B.; Tang, J. The impact of urban built environment on residential physical health: Based on propensity score matching. Acta Geogr. Sin. 2018, 73, 333–345. [Google Scholar]
- Lu, C.X.; Chen, W.S. Healthy Communities and the Conceptual Framework of Their Indicators. J. Beijing Univ. Aeronaut. Astronaut. Soc. Sci. Ed. 2011, 24, 1–7. [Google Scholar]
- Zhang, Q.F. The Construction of Healthy Communities in China from the Perspective of Ecosystem. Ningxia Soc. Sci. 2021, 6, 162–168. [Google Scholar]
- De Castella, K.; Goldin, P.; Jazaieri, H.; Heimberg, R.G.; Dweck, C.S.; Gross, J.J. Emotion Beliefs and Cognitive Behavioural Therapy for Social Anxiety Disorder. Cogn. Behav. Therary 2015, 44, 128–141. [Google Scholar] [CrossRef] [PubMed]
- Carrera, P.; Caballero, A.; Munoz, D.; Gonzalez-Iraizoz, M.; Fernandez, I. Construal level as a moderator of the role of affective and cognitive attitudes in the prediction of health-risk behavioural intentions. Br. J. Soc. Psychol. 2014, 53, 773–791. [Google Scholar] [CrossRef] [PubMed][Green Version]
- Sun, X.Y.; Guo, Y.; Sun, J. Verification of the Integration of Health Belief Model and Planned Behavior Theory. J. Peking Univ. Health Sci. 2009, 41, 129–134. [Google Scholar]
- Dryhurst, S.; Schneider, C.R.; Kerr, J.; Freeman, A.L.J.; Recchia, G.; van der Bles, A.M.; Spiegelhalter, D.; van der Linden, S. Risk perceptions of COVID-19 around the world. J. Risk Res. 2020, 23, 994–1006. [Google Scholar] [CrossRef]
- Kenny, R.; Dooley, B.; Fitzgerald, A. Interpersonal relationships and emotional distress in adolescence. J. Adolesc. 2013, 36, 351–360. [Google Scholar] [CrossRef]
- Zhou, S.K. On the Basic Theoretical Questions in Moral Assessment. Stud. Ethics 2006, 6, 47–51. [Google Scholar]
- Fang, J.L.; Chen, W.L.; Wang, J.Y.; Zhao, J.; Wang, J.W.; Shao, C.H. Factors associated with medication adherence in community patients with coronary artery disease based on health belief model (HBM): A cross-sectional study. Fudan Univ. J. Med. Sci. 2020, 3, 378–384+391. [Google Scholar]
- Pachankis, J.M.; Eldahan, A.I.; Golub, S.A. New to New York: Ecological and psychological predictors of health among recently arrived young adult gay and bisexual urban migrants. Ann. Behav. Med. 2016, 50, 692–703. [Google Scholar] [CrossRef]
- Salerno, J.P.; Devadas, J.; Pease, M.; Nketia, B.; Fish, J.N. Sexual and gender minority stress amid the COVID-19 pandemic: Implications for LGBTQ young persons’ mental health and well-being. Public Health Rep. 2020, 135, 721–727. [Google Scholar] [CrossRef]
- Hu, X.Y.; Yang, S.L.; Zhong, Q.; Yu, F.; Chen, H. The relationship between social class and health: Their “social-psychological-physiological” mechanism. Chin. Sci. Bull. 2019, 2, 194–205. [Google Scholar] [CrossRef]
- Kajsa, E.; Liu, B.C.; Zhang, Y.; Chai, Y.W. Concept of Project in Time-Geography and Its Empirical Case Studies. Hum. Geogr. 2016, 5, 32–38. [Google Scholar]
- Zhang, Y.; Chai, Y.W. “New” Time-Geography: A Review of Recent Progresses of Time-Geography Researches from KAJSA Ellegard in Sweden. Hum. Geogr. 2016, 5, 19–24+46. [Google Scholar]
- Zhang, Y.; Cai, Y.W. Development of time geography based on the project-activity system. Prog. Geogr. 2022, 41, 53–63. [Google Scholar] [CrossRef]
- Liu, L.; Wu, L.L.; Song, G.W.; Zhou, S.H.; Kwan, M.P. An innovation research framework of crime geography based on spatio-temporal behavior perspective. Geogr. Res. 2022, 41, 1748–1764. [Google Scholar]
- Zou, S.C.; Zhang, S.Q.; Zhen, F. Measurement of community daily activity space and influencing factors of vitality based onresidents’ spatiotemporal behavior: Taking Shazhou and Nanyuan streets in Nanjing as examples. Prog. Geogr. 2021, 40, 580–596. [Google Scholar] [CrossRef]
- Huang, H.M.; Zhou, D.L.; Wang, Y. An Analysis of the Spatial Organization of Community Life-cycle under Residential Morphological Categories. Urban Plan. Forum 2021, 2, 94–101. [Google Scholar]
- Xie, B.; Zheng, Y.L.; Li, Z.G.; An, Z.H. Planning Model for the Elderly Outdoor Space from the Perspective of Behavior Activities: A Case in Wuhan. Mod. Urban Res. 2019, 2, 30–37. [Google Scholar]
- Rogers, R.W. A protection motivation theory of fear appeals and attitude change. J. Psychol. 1975, 91, 93–114. [Google Scholar] [CrossRef]
- Maddux, J.E.; Rogers, R.W. Protection motivation and selfefficacy: A revised theory of fear appeals and attitude change. J. Exp. Soc. Psychol. 1983, 19, 469–479. [Google Scholar] [CrossRef]
- Seow, A.N.; Choong, Y.O.; Moorthy, K.; Choong, C.K. Predicting medical tourism behavioural intention using social cognition models. Tour. Rev. 2020, 76, 374–391. [Google Scholar] [CrossRef]
- Farooq, A.; Laato, S.; Islam, A.K.M.N. Impact of Online Information on Self-Isolation Intention During the COVID-19 Pandemic: Cross-Sectional Study. J. Med. Internet Res. 2020, 22, e19128. [Google Scholar] [CrossRef] [PubMed]
- Rad, R.E.; Mohseni, S.; Takhti, H.K. Azad, M.H.; Shahabi, N.; Aghamolaei, T.; Norozian, F. Application of the protection motivation theory for predicting COVID-19 preventive behaviors in Hormozgan, Iran: A cross-sectional study. BMC Public Health 2021, 21, 466. [Google Scholar]
- Roozbahani, N.; Kaviani, A.H.; Khorsandi, M. Path analysis of skin cancer preventive behavior among the rural women based on protection motivation theory. BMC Women’s Health 2020, 20, 121. [Google Scholar] [CrossRef] [PubMed]
- Tian, Y. Application progress on protection motivation theory in health behavior promotion and disease management. Chin. Nurs. Res. 2018, 32, 3845–3847. [Google Scholar]
- Becker, G.; Murphy, K. A Theory of Rational Addiction. J. Political Econ. 1988, 96, 675–700. [Google Scholar] [CrossRef]
- Liu, Y.W.; Lu, S.R. A Preliminary Study on Main Theories of Individual Health Behavior Change and Intergration. Chin. J. Health Educ. 2018, 34, 284–287. [Google Scholar]
- Tang, M.M.; Wang, D.H.; Wang, Y.; Guerrien, A. Motivation Characteristic of Daily Activity Participation among Urban Elderly in China et in France and lts Relationship with Subjective Health. Chin. J. Clin. Psychol. 2019, 3, 555–560. [Google Scholar]
- Mao, Y.Q.; Li, J.Q. Context in Daily Life Circle of the Elderly Based on Family Life Cycle Theory: A Case Study of Xi’an City. Areal Res. Dev. 2020, 39, 169–175. [Google Scholar]
- Jiang, X.; Zhang, W.H.; Li, X.; Li, L.; Lin, Q. Fragmentation and Integration: Research on the Alienation and Fusion Renewal of Public Space in the Old City of Jinan Based on Crowd Activities from the Perspective of Daily Life. Chin. Landsc. Archit. 2022, 38, 93–98. [Google Scholar]
- Gehl, J. Life between Buildings: Using Public Space (transl. by Koch, J.); Van Nostrand Reinhold: New York, NY, USA, 1987. [Google Scholar]
- Jin, F.J. Essential classification and its effects of spatial profiting of human activity. Geogr. Res. 2014, 1, 191–198. [Google Scholar]
- World Health Organization. International Classification of Functioning, Disability and Health: ICF: Short Version; World Health Organization: Geneva, Switzerland, 2001. [Google Scholar]
- Wang, H.; Zhou, Y.J.; Liu, J.; Li, X.; Yang, W.; Qi, J.H.; He, S.P.; Tian, Y.; Liu, J.R. Health Related Risky Behaviors in Adolescents with Schizophrenia. Chin. Ment. Health J. 2016, 5, 363–368. [Google Scholar]
- Xu, Y.F.; Huang, X.J. Progress and prospects of geography in public health: A review of literature abroad. Geogr. Res. 2021, 9, 2638–2656. [Google Scholar]
- Yao, X.Y.; Zhang, Y. Understanding the Changing Household Project and the Pocket of Local Orders of Home under the COVID-19: Case Studies from Residents of Shuangjing Subdistrict in Beijing. Urban Dev. Stud. 2021, 28, 10–17+2. [Google Scholar]
- Ludwig, D.; Peterson, K.; Gortmaker, S. Relation between Consumption of Sugar-sweetened Drinks and Childhood 0besity: A Prospective, Observational Analysis. Lancet 2001, 357, 505–509. [Google Scholar] [CrossRef] [PubMed]
- Zhao, J.; Zhao, Q.L.; Wang, L.M.; Hou, S.N.; Liang, Y. A Qualitative Study on Characteristics of Eating Behavior Change in Patients with Type 2 Diabetes. Chin. J. Nurs. 2018, 2, 139–143. [Google Scholar]
- Mitchell, N.S.; Scialla, J.J.; Yancy, W.S. Are low-carbohydrate diets safe in diabetic and nondiabetic chronic kidney disease? Ann. N. Y. Acad. Sci. 2020, 1461, 25–36. [Google Scholar] [CrossRef]
- He, W.; Geng, G.L.; Qian, X.Y. Application of Protective Motivation Theory in Lifestyle Analysis of Hypertensive Patients. J. Qilu Nurs. 2011, 17, 29–30. [Google Scholar]
- Ralph, A.F.; Ager, B.; Bell, M.L.; Collins, I.M.; Andrews, L.; Tucker, K.; Phillips, K.A.; Butow, P. Women’s preferences for selective estrogen reuptake modulators: An investigation using protection motivation theory. Patient Educ. Couns. 2014, 96, 106–112. [Google Scholar] [CrossRef]
- Moghadam, M.H.; Andi, S.J.; Shirvani, J.S.; Khafri, S.; Ghadimi, R.; Parsian, H. Efficiency of two constructs called “fear of disease” and “perceived severityof disease” on the prevention of gastric cancer: Application of protecion motivation theory. Casp. J. Intern. Med. 2015, 6, 201–208. [Google Scholar]
- Plotnikoff, R.C.; Trinh, L.; Courneya, K.S.; Karunamuni, N.; Sigal, R.J. Predictors of aerobic physical activity and resistance training among Canadian adults with type 2diabetes:an application of the protection motivation theory. Psychol. Sport Exerc. 2009, 10, 320–328. [Google Scholar] [CrossRef]
- Hua, Y. Analysis of the effect of protection motivation on the prevention of falls in elderly inhospitalized patients. J. Qiqihar Med. Univ. 2013, 34, 1030–1031. [Google Scholar]
- Yan, Q.Y.; Jacques-Tiura, A.J.; Chen, X.G.; Xie, N.H.; Chen, J.; Yang, N.N.; Gong, J.; MacDonell, K.K. Application of the Protection Motivation Theory in predicting cigarette smoking among adolescents in China. Addict. Behav. 2014, 39, 181–188. [Google Scholar] [CrossRef] [PubMed]
- Wu, C.S.T.; Wong, H.T.; Chou, L.Y.; To, B.P.W.; Lee, W.L.; Loke, A.Y. Correlates of protective motivation theory (PMT) to adolescents drug use intention. Int. J. Environ. Res. Public Health 2014, 11, 671–684. [Google Scholar] [CrossRef] [PubMed]
- Xiao, Y.; Chen, S.J.; Miao, S.Y.; Yu, Y.F. Exploring the Mediating Effect of Physical Activities on Built Environment and Obesity for Elderly People: Evidence from Shanghai, China. Front. Public Health 2022, 10, 853292. [Google Scholar] [CrossRef] [PubMed]
- Edwards, N.M.; Myer, G.D.; Kalkwarf, H.J.; Woo, J.G.; Khoury, P.R.; Hewett, T.E.; Daniels, S.R. Outdoor Temperature, Precipitation, and Wind Speed Affect Physical Activity Levels in Children: A Longitudinal Cohort Study. J. Phys. Act. Health 2015, 12, 1074–1081. [Google Scholar] [CrossRef] [PubMed]
- Chen, D.R.; Lin, Y.C. Social identity, perceived urban neighborhood quality, and physical inactivity: A comparison study of China, Taiwan, and South Korea. Health Place 2016, 41, 1–10. [Google Scholar] [CrossRef]
- Sato, H.; Inoue, S.; Fukushima, N.; Kikuchi, H.; Takamiya, T.; Tudor-Locke, C.; Hikihara, Y.; Tanaka, S. Lower youth steps/day values observed at both high and low population density areas: A cross-sectional study in metropolitan Tokyo. BMC Public Health 2018, 18, 1132. [Google Scholar] [CrossRef]
- Kabisch, N.; Kraemer, R. Physical activity patterns in two differently characterised urban parks under conditions of summer heat. Environ. Sci. Policy 2020, 107, 56–65. [Google Scholar] [CrossRef]
- Wang, X.W.; Niu, J.; Zhou, H. Analysis of Protection Motive Theory on Young People Smoking Behavior. Mod. Prev. Med. 2009, 36, 1704–1707. [Google Scholar]
- Menard, P.; Bott, G.J.; Crossler, R.E. User Motivations in Protecting Information Security: Protection Motivation Theory Versus Self-Determination Theory. J. Manag. Inf. Syst. 2017, 34, 1203–1230. [Google Scholar] [CrossRef]
- Zhang, J.; Li, S.P.; Guo, Y.N. Study on the influencing factors of farmers’ environmental behavior based on the protection motivation theory. J. Arid Land Resour. Environ. 2019, 33, 8–13. [Google Scholar]
- Hanus, B.; Wu, Y. Impact of Users’ Security Awareness on Desktop Security Behavior: A Protection Motivation Theory Perspective. Inf. Syst. Manag. 2016, 33, 2–16. [Google Scholar] [CrossRef]
- Kothe, E.J.; Ling, M.; North, M.; Klas, A.; Mullan, B.A.; Novoradovskaya, L. Protection motivation theory and pro-environmental behaviour: A systematic mapping review. Aust. J. Psychol. 2019, 71, 411–432. [Google Scholar] [CrossRef]
- Xing, X.; Xiu, C.B.; Yan, Y. Influencing factors on agricultural water saving technology adoption behavior:Based on the protection motivation theory and transtheoretical model. J. China Agric. Univ. 2022, 27, 274–286. [Google Scholar]
- Li, M. The Planning Strategies of a 15-minute Community Life Circle Based on Behaviors of Residents. Urban Plan. Forum 2017, 1, 111–118. [Google Scholar]
- Chai, Y.W.; Li, C.J.; Xia, W.Q.; Wang, J.; Zhang, X.; Sun, D.S. Study on the Delineation Model of Urban Community Life Circle:Based on Qinghe District in Haidian District, Beijing. Urban Dev. Stud. 2019, 26, 1–8+68. [Google Scholar]
- Huang, J.Z.; Zhang, R.Q.; Hu, G.Y. A research on the daily life circle of the participants based on spatio-temporal behaviour:spatial cognizance and feature analysis. Urban Plan. Forum 2019, 3, 87–95. [Google Scholar]
- Liu, Y.; Xiao, T.; Liu, Y.; Qiu, Y.; Liu, Y.; Li, Z. Impact of urban built envionments on residents’ subjective well-being:An analysis based on 15-minute walking distance. Prog. Geogr. 2020, 39, 1270–1282. [Google Scholar] [CrossRef]
- Zhou, X. Assessing the Distribution of Public Service Facilities in Unit Planning Based on the Perspective of the 15-minute Community-life Circle: Evidence from Huangpu District of Shanghai. Urban Plan. Forum 2020, 1, 57–64. [Google Scholar]









{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Project Activities Categories | Categories of Activity Motivations and Objectives | Major Life Activities | Major Activity Motivations and Objectives |
|---|---|---|---|
| necessary activities | Activities that are less influenced by the external environment and are necessary to maintain one’s own survival or are required to be completed by the regulations. | Food and accommodation activities | Based on basic survival activities of feeding and housework |
| Commuting activities | Daily commuting activities to and from work, or to and from the community | ||
| Educated activities | Activities for groups of students going to and from school and receiving education | ||
| Health care activities | Health and medical activities for middle-aged and elderly groups and the sick and infirm | ||
| spontaneous activities | Activities that are greatly influenced by the external environment and are undertaken spontaneously depending on one’s own will for the purpose of fitness, leisure and entertainment. | Personal leisure physical activity | Personal physical activity for the purpose of recreation and fitness |
| Other personal recreational activities | The activities in which individuals pay more attention to the needs of their own spirit or enjoyment after meeting the needs of their basic physiological and security. | ||
| social activities | Social activities that are influenced by the external environment, for the purpose of fitness and recreation, and which are dependent on the participation of others and cannot be performed independently. | Group leisure and physical activity | Group physical activity for the purpose of recreation and fitness |
| Other social interaction activities | Through various social activities, people can meet more different people to relieve the monotony and tedium of their life, exercise for their bodies and brains better, maintain vitality, delay senescence, and reduce the infestation of psychological diseases and senile diseases. |
| Variables | Definition | Assignment | ||
|---|---|---|---|---|
| Dependent Variables | Behavioral Intention | The extent to which daily life activities affect their associated public health issues. | No impact = 1; Less impact = 2; General = 3; More impact = 4; Extraordinary impact = 5 | |
| Independent Variables | Density | Refers to the number of residents, housing units or employment in the unit area. | ||
| Diversity | Refers to the degree of land mix, i.e., different land use types and degree of complementarity in some area. | |||
| Destination Accessibility | Refers to the degree of proximity of non-residential land use (e.g., shops, parks, bus stops, etc.), mainly measuring the accessibility from one destination to another. | |||
| Design | Refers to the number of choices of directions and routes to destinations, which is often used to measure the difficulty of traveling between one place to another, and is usually shown by the street network pattern; The main measurements include block size, length, intersection density, complex network variables, etc. | |||
| Bus Stop Distance | Refers to the average value of the shortest route from the residence or workplace to the nearest bus stop, or uses bus route density, distance between bus stops, and the number of stops per unit area to quantify this indicator. | |||
| Mediator Variables | Daily Life Activity | Frequency of daily life activity | ||
| Intensity of daily life activity. | ||||
| Moderator Variables | Threat assessment | Severity (Ser) | daily life activities may lead to public health diseases (Sev1). | Strongly disagree = 1; Disagree = 2; General = 3; Agree = 4; Strongly agree = 5 |
| Public health diseases increase the burden on families (Sev2). | ||||
| Vulnerability (Vul) | daily life activities may cause diseases to spread to others (Vul1). | |||
| The possibility that daily life activities will cause public health diseases to disable oneself (Vul2). | ||||
| Internal reward (Int) | Performing daily life activities makes residents feel very happy (Int1). | |||
| Performing daily life activities makes residents feel satisfied (Int2). | ||||
| External reward (Ext) | daily life activities can attract the attention of the opposite sex (Ext1). | |||
| Performing daily life activities can be identified by others (Ext2). | ||||
| Response assessment | Self-efficacy (Sel) | Residents are full of confidence that performing daily life activities can enhance their health (Sel1). | ||
| Residents are full of confidence in their self-restraint ability to inhint their daily life activities (Sel2). | ||||
| Response efficiency (Res) | daily life activities can improve residents’ awareness of the benefits of disease prevention (Res1). | |||
| Controlling health risk behaviors can lead a comfortable life. Keeping healthy behaviors can improve the healthy level (Res2). | ||||
| Cost of response (Cos) | Restraining daily life activities needs to bear additional burdens (Cos1). | |||
| Other obstacles or inconveniences may be encountered in the process of inhibiting daily life activities (Cos2). | ||||
| Controlled Variables for Demographic Characteristics | Gender (X1) | Male = 1; Female = 0 | ||
| Age (X2) | Actual Age | |||
| Educational Level (X3) | Never been to school = 1; Primary school = 2; Junior high school = 3; High school = 4; College degree or above = 5 | |||
| Marital Status (X4) | Unmarried = 1; Married = 0 | |||
| Career Information (X5) | ||||
| Income (X6) | ||||
| Controlled Variables for Social Environment | Political Environment | Liberty of Speech (%) | No liberty = 1; Less liberty = 2; General = 3; More liberty = 4; Quite a lot of liberty = 5 | |
| Citizens’ participation in politics (%) | Non-participation in politics = 1; Less political participation = 2; General = 3; More political participation = 4; Participation in politics very often = 5 | |||
| Policy Transparency (%) | Very opaque = 1; Opacity = 2; General = 3; Transparency = 4; Very transparent = 5 | |||
| Economic Circumstances | Net Income Per Capita | |||
| R&D Internal Appropriation Expenditure | ||||
| Proportion of Secondary and Tertiary Industries in GDP | ||||
| Regional GDP | ||||
| Cultural and Educational Environment | Percentage of Cultural and Educational Activities of Community (%) | |||
| Average Annual Education and Publicity Expenses of Community | ||||
| Per Capita Expenditure on Education | ||||
| Psychological Environment | Community Identification | |||
| Community Satisfaction | ||||
| Community Security | ||||
| Community Participation | ||||
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Zhong, Q.; Li, B.; Chen, Y.; Zhu, J. Public Health Safety in Community Living Circles Based on a Behavioral Motivation Perspective: Theoretical Framework and Evaluation System. Behav. Sci. 2023, 13, 26. https://doi.org/10.3390/bs13010026
Zhong Q, Li B, Chen Y, Zhu J. Public Health Safety in Community Living Circles Based on a Behavioral Motivation Perspective: Theoretical Framework and Evaluation System. Behavioral Sciences. 2023; 13(1):26. https://doi.org/10.3390/bs13010026
Chicago/Turabian StyleZhong, Qikang, Bo Li, Yue Chen, and Jiawei Zhu. 2023. "Public Health Safety in Community Living Circles Based on a Behavioral Motivation Perspective: Theoretical Framework and Evaluation System" Behavioral Sciences 13, no. 1: 26. https://doi.org/10.3390/bs13010026
APA StyleZhong, Q., Li, B., Chen, Y., & Zhu, J. (2023). Public Health Safety in Community Living Circles Based on a Behavioral Motivation Perspective: Theoretical Framework and Evaluation System. Behavioral Sciences, 13(1), 26. https://doi.org/10.3390/bs13010026