
Are You Happy? A Validation Study of a Tool Measuring Happiness

 ,
,  and
and 
Abstract
:1. Introduction
2. Materials and Methods
2.1. Participants
2.2. Measures
2.2.1. The Measure of Happiness (MH)
- Psychophysics Status:
- ○
- Come valuti il rapporto con il tuo corpo?
- ▪
- How do you evaluate your relationship with your body?
- ○
- Come valuti il tuo livello di equilibrio mentale e fisico?
- ▪
- How do you evaluate your level of mental and physical balance?
- ○
- Come valuti il tuo rapporto con te stesso?
- ▪
- How do you evaluate your relationship with yourself?
- Financial Status:
- ○
- Quanto ritieni di essere realizzato in questo momento?
- ▪
- How fulfilled do you feel with your life at this moment?
- ○
- Quanto sei soddisfatto della tua condizione finanziaria?
- ▪
- How satisfied are you with your financial situation?
- ○
- Quanto ti senti solido finanziariamente?
- ▪
- How financially sound do you feel?
- Relational Private Sphere:
- ○
- Come valuti la qualità dei tuoi rapporti con i tuoi affetti principali?
- ▪
- How do you evaluate the quality of your relationships with your dear ones?
- ○
- Quanto ti soddisfa l’atmosfera che si vive nella tua attuale casa?
- ▪
- At present, how satisfied are you with the atmosphere in your home?
- ○
- Secondo te, i membri della tua famiglia, quanto ti stimano?
- ▪
- In your opinion, how much do your family members appreciate you?
- Socio-Relational Sphere:
- ○
- Quanto pensi che le persone, in generale, siano felici di relazionarsi con te?
- ▪
- In general, how happy do you think people are to interact with you?
- ○
- Quanto ritieni apprezzati i tuoi comportamenti nella società?
- ▪
- How much do you think your behavior is appreciated in society?
- Life Perspective:
- ○
- Quanto ritieni importante porti degli obiettivi di lungo termine?
- ▪
- How important is it to you to set long-term goals?
- ○
- Quanto ti interessi al tuo miglioramento personale?
- ▪
- How much are you engaged in self-improvement?
- ○
- Quanto ti senti flessibile di fronte ai cambiamenti della vita?
- ▪
- How adaptable do you feel to major changes in your life?
2.2.2. Subjective Happiness Scale (SHS)
2.2.3. State–Trait Anxiety Inventory (STAI)—Anxiety
2.2.4. Beck Depression Inventory (BDI)
2.2.5. WHOQOL-BREF
2.3. Procedure
2.4. Data Analysis
3. Results
3.1. Happiness Scales: Descriptive Analysis and Internal Consistency
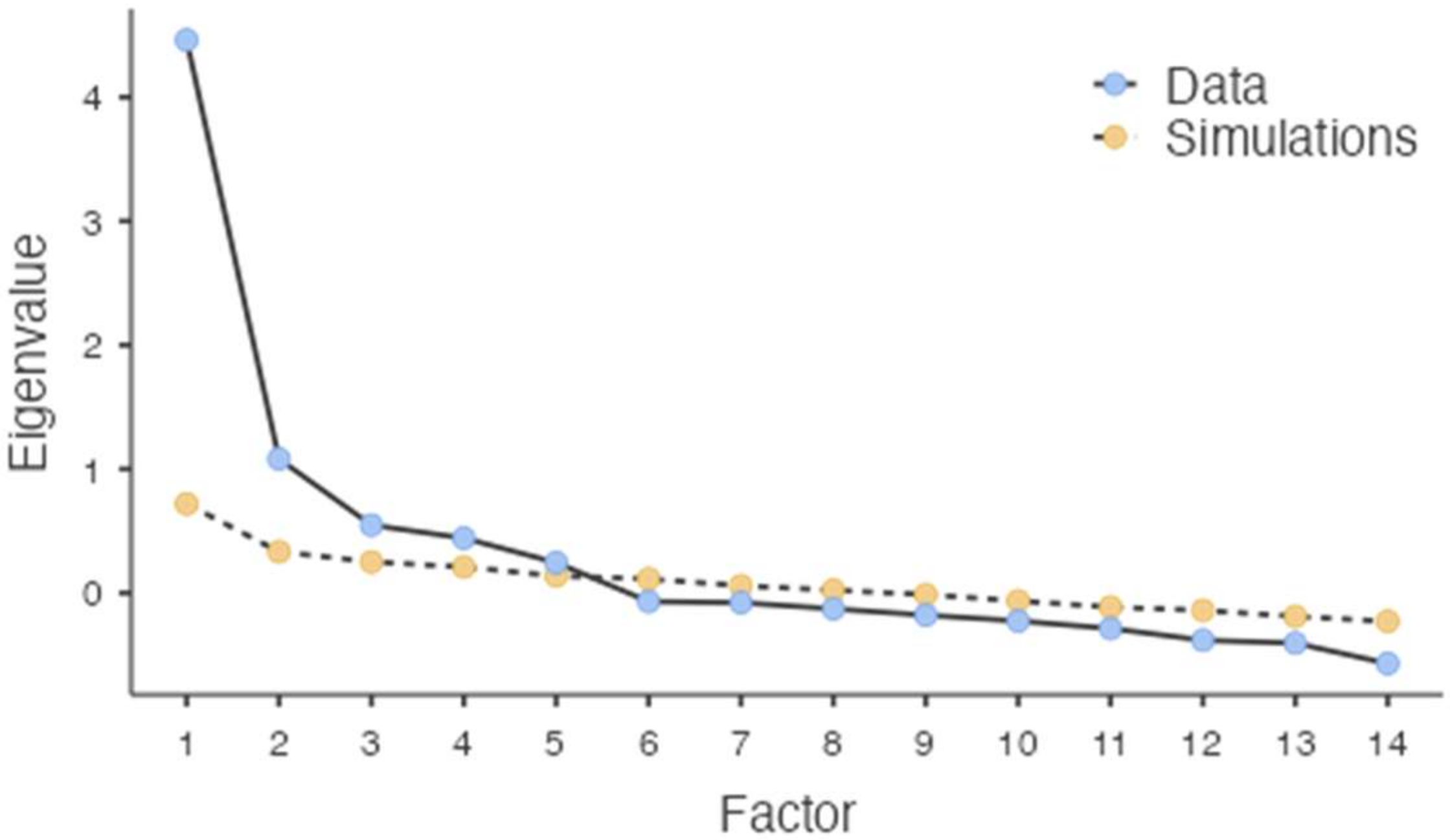
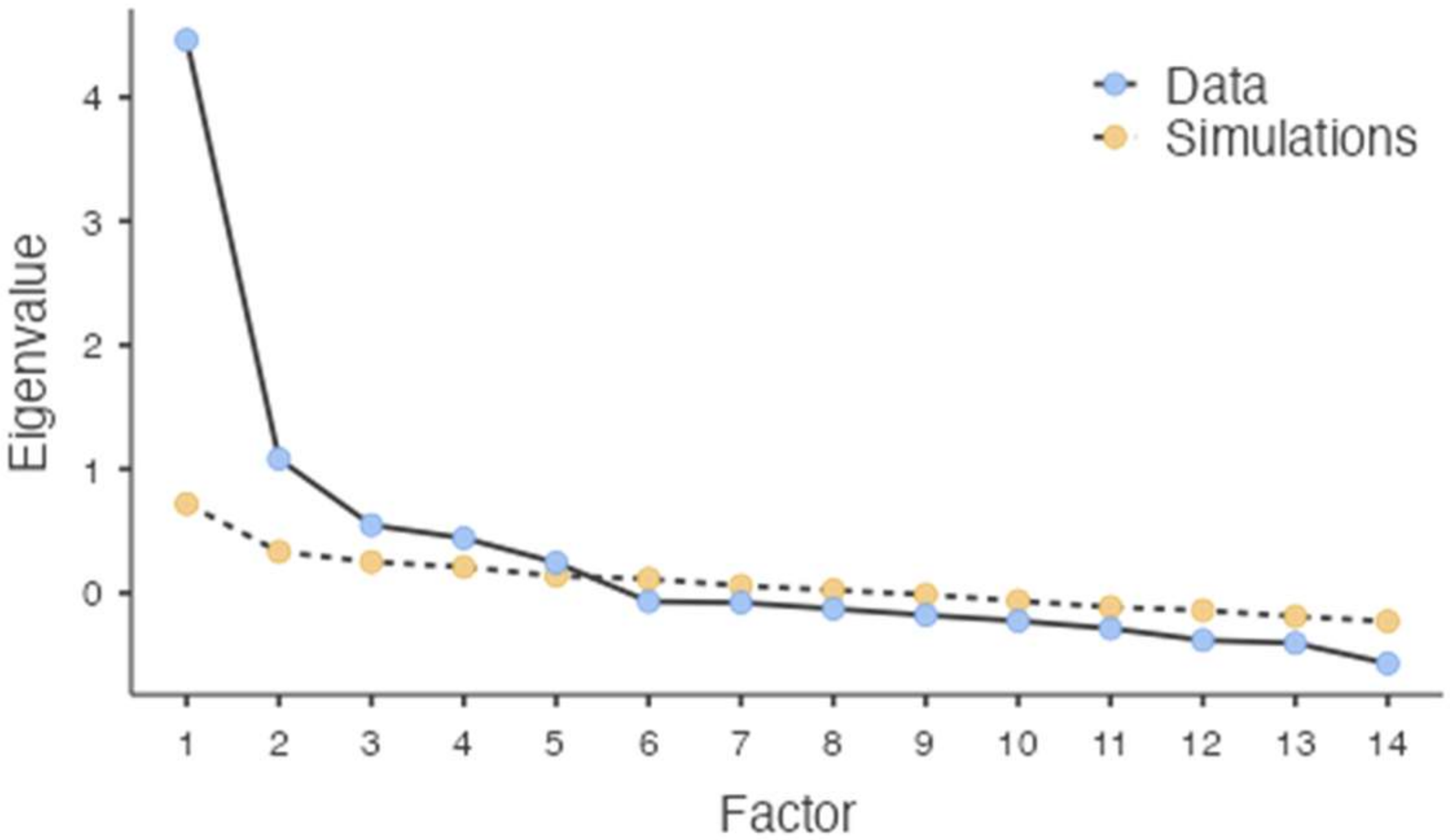
3.2. MH Structure: Exploratory Factor Analysis
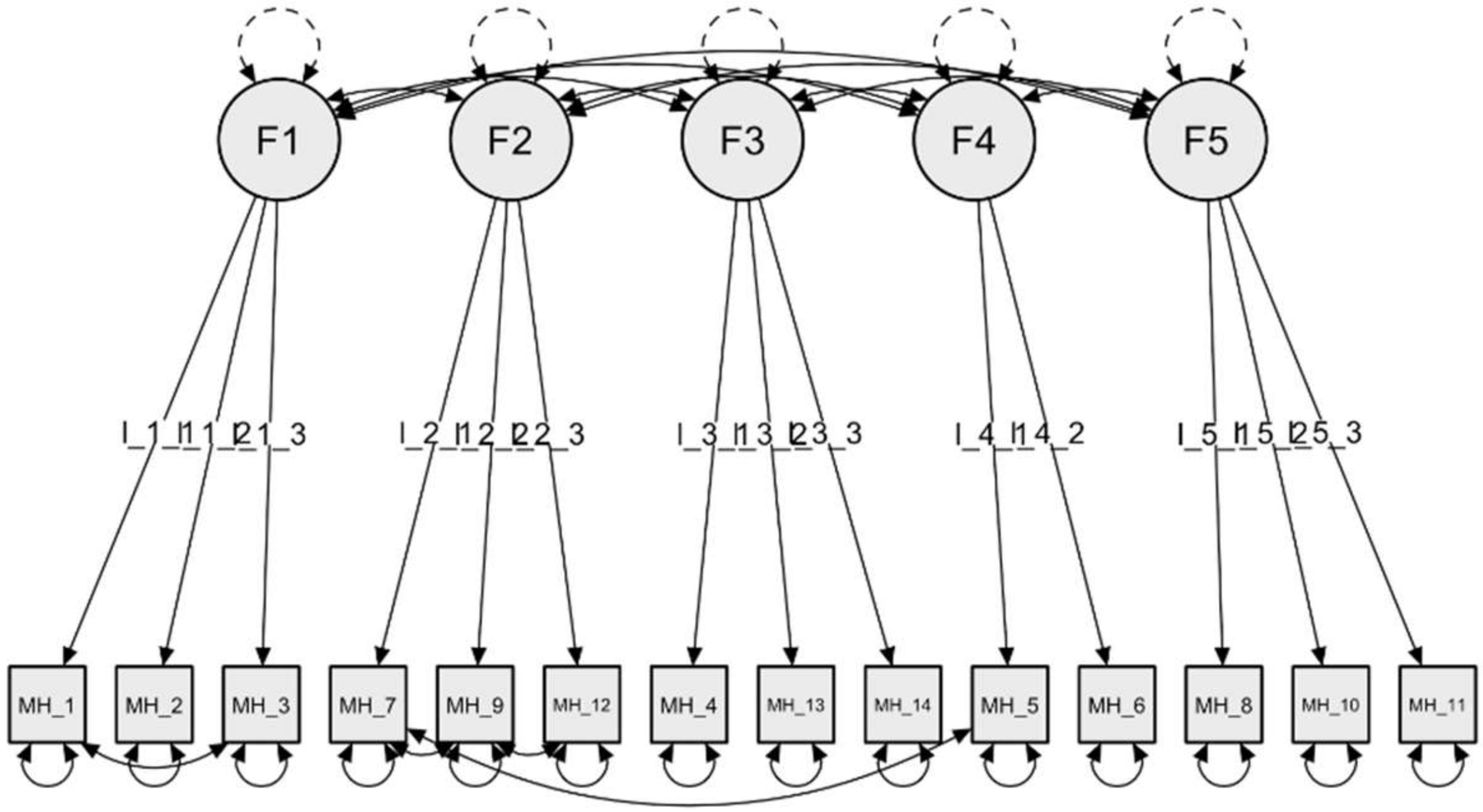
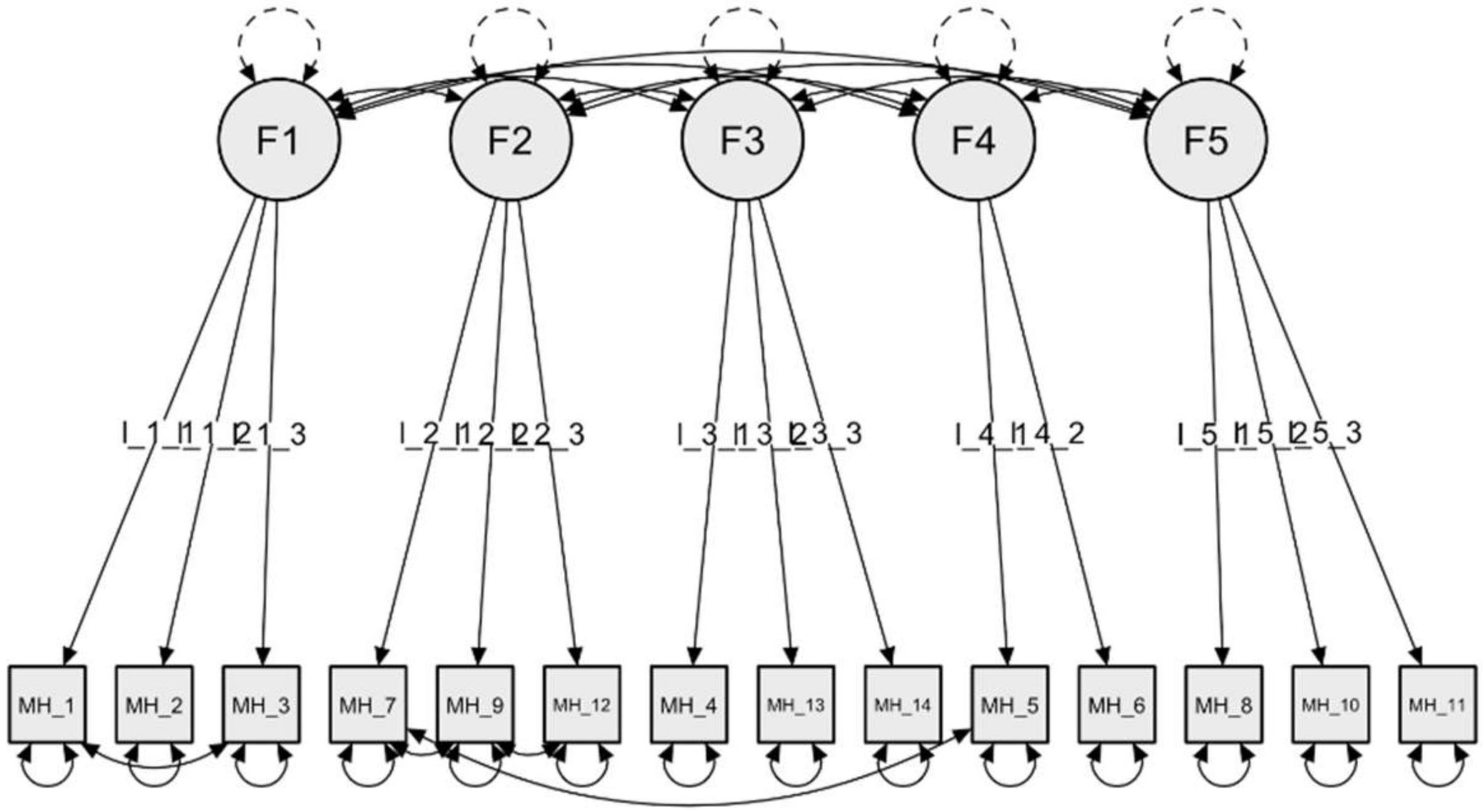
3.3. CFA of the Five-Factor Solution and Structural Invariance
3.4. Convergent and Discriminant Validity
4. Discussion
Study Limitations
5. Concluding Remarks
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Freedman, J.L. Happy People: What Happiness Is, Who Has It, and Why; Harcourt Brace Jovanovich: New York, NY, USA, 1978. [Google Scholar]
- Juster, F.T.; Stafford, F.P. Time, Goods, and Well-Being; Survey Research Center, Institute for Social Research, University of Michigan: Ann Arbor, MI, USA, 1985. [Google Scholar]
- Lemon, B.W.; Bengtson, V.L.; Peterson, J.A. An exploration of the activity theory of aging: Activity types and life satisfaction among in-movers to a retirement community. J. Gerontol. 1972, 27, 511–523. [Google Scholar] [CrossRef] [PubMed]
- Eysenck, H.J.; Eysenck, M.W. Happiness: Facts and Myths; Lawrence Erlbaum: London, UK, 1994. [Google Scholar]
- Myers, D.G.; Diener, E. Who is happy? Psychol. Sci. 1995, 6, 10–19. [Google Scholar] [CrossRef]
- Diener, E. Subjective well-being: The science of happiness, and a proposal for a national index. Am. Psychol. 2000, 55, 34–43. [Google Scholar] [CrossRef] [PubMed]
- Csikszentmihalyi, M.; Hunter, J. Happiness in everyday life: The uses of experience sampling. J. Happiness Study 2003, 4, 185–199. [Google Scholar] [CrossRef]
- Lyubomirsky, S.; Sheldon, K.M.; Schkade, D. Pursuing happiness: The architecture of sustainable change. Rev. Gen. Psychol. 2005, 9, 111–131. [Google Scholar] [CrossRef]
- Bradburn, N.M. The Structure of Psychological Well-Being; Alpine: Chicago, IL, USA, 1969. [Google Scholar]
- Watson, D.; Clark, L.A.; Tellegen, A. Development and validation of brief measures of positive and negative affect: The PANAS scales. J. Personal. Soc. Psychol. 1988, 54, 1063–1070. [Google Scholar] [CrossRef]
- Diener, E.; Emmons, R.A.; Larsen, R.J.; Griffin, S. The satisfaction with life scale. J. Pers. Assess. 1985, 49, 71–75. [Google Scholar] [CrossRef]
- Andrews, F.M.; Withey, S.B. Measuring global well-being. In Social Indicators of Well-Being; Springer: Boston, MA, USA, 1976; pp. 63–106. [Google Scholar]
- Omodei, M.M.; Wearing, A.J. Need satisfaction and involvement in personal projects: Toward an integrative model of subjective well-being. J. Personal. Soc. Psychol. 1990, 59, 762. [Google Scholar] [CrossRef]
- Costa, P.T.; McCrae, R.R. Personality as a Lifelong Determinant of Well-Being; Emotion in Adult Development; SAGE Publications: Beverly Hills, CA, USA, 1984; pp. 141–157. [Google Scholar]
- Dambrun, M.; Ricard, M.; Després, G.; Drelon, E.; Gibelin, E.; Gibelin, M.; Loubeyre, M.; Py, D.; Delpy, A.; Garibbo, C.; et al. Measuring happiness: From fluctuating happiness to authentic durable happiness. Front. Psychol. 2012, 3, 16. [Google Scholar] [CrossRef]
- Lyubomirsky, S.; Lepper, H.S. A measure of subjective happiness: Preliminary reliability and construct validation. Soc. Indic. Res. 1999, 46, 137–155. [Google Scholar] [CrossRef]
- Mauss, I.B.; Tamir, M.; Anderson, C.L.; Savino, N.S. Can seeking happiness make people unhappy? Paradoxical effects of valuing happiness. Emotion 2011, 11, 807–815. [Google Scholar] [CrossRef]
- Joshanloo, M. The influence of fear of happiness beliefs on responses to the satisfaction with life scale. Personal. Individ. Differ. 2013, 54, 647–651. [Google Scholar] [CrossRef]
- Yildirim, M.; Maltby, J. Irrational Happiness Beliefs Scale: Development and Initial Validation. Int. J. Ment. Health Addict. 2021, 20, 2277–2290. [Google Scholar] [CrossRef]
- De Girolamo, G.; Rucci, P.; Scocco, P.; Becchi, A.; Coppa, F.; Addario, A.; Daru, E.; De Leo, D.; Galassi, L.; Mangelli, L.; et al. Quality of Life assessment validation of the Italian version of WHOQOL-Bref. Epidemiol. Psichiatr. Soc. 2000, 9, 45–55. [Google Scholar] [CrossRef]
- Spielberger, C.D.; Gorsuch, R.L.; Lushene, R.; Vagg, P.R.; Jacobs, G.A. Manual for the State-Trait Anxiety Inventory; Consulting Psychologists Press: Palo Alto, CA, USA, 1983. [Google Scholar]
- Spielberger, C.D. State-Trait Anxiety Inventory: Bibliography, 2nd ed.; Consulting Psychologists Press: Palo Alto, CA, USA, 1989. [Google Scholar]
- Spielberger, C.D.; Sydeman, S.J. State-Trait Anxiety Inventory and State-Trait Anger Expression Inventory. In The Use of Psychological Testing for Treatment Planning and Outcome Assessment; Maruish, M.E., Ed.; Lawrence Erlbaum Associates: Hillsdale, NJ, USA, 1994; pp. 292–321. [Google Scholar]
- Beck, A.T.; Steer, R.A.; Garbin, M.G. Psychometric properties of the Beck Depression Inventory: Twenty-five years of evaluation. Clin. Psychol. Rev. 1988, 8, 77–100. [Google Scholar] [CrossRef]
- Stewart, A.; Ware, J.E.; Sherbourne, C.D.; Wells, K.B. Psychological distress/well-being and cognitive functioning measures. In Measuring Functioning and Well-Being; Stewart, A.L., Ware, J.E., Eds.; Duke University Press: Durham, UK, 1992; pp. 102–142. [Google Scholar]
- Cattell, R.B.; Scheier, I.H. The Meaning and Measurement of Neuroticism and Anxiety; Ronald Press: New York, NY, USA, 1961. [Google Scholar]
- WHOQOL Group. Development of the World Health Organization WHOQOL-BREF quality of life assessment. Psychol Med. 1998, 28, 551–558. [Google Scholar] [CrossRef]
- Boateng, G.O.; Neilands, T.B.; Frongillo, E.A.; Melgar-Quiñonez, H.R.; Young, S.L. Best practices for developing and validating scales for health, social, and behavioral research: A primer. Front. Public Health 2018, 6, 149. [Google Scholar] [CrossRef]
- Chesney, M.A.; Neilands, T.B.; Chambers, D.B.; Taylor, J.M.; Folkman, S. A validity and reliability study of the coping self-efficacy scale. Br. J. Health Psychol. 2006, 11, 421–437. [Google Scholar] [CrossRef]
- Cattell, R.B. The scree test for the number of factors. Multivar. Behav. Res. 1966, 1, 245–276. [Google Scholar] [CrossRef]
- Horn, J.L. A rationale and test for the number of factors in factor analysis. Psychometrika 1965, 30, 179–185. [Google Scholar] [CrossRef]
- Hu, L.; Bentler, P.M. Cutoff criteria for fit indexes in covariance structure analysis: Conventional criteria versus new alternatives. Struct. Equ. Modeling Multidiscip. J. 1999, 6, 1–55. [Google Scholar] [CrossRef]
- Bentler, P.M. Comparative fit indexes in structural models. Psychol. Bull. 1990, 107, 238–246. [Google Scholar] [CrossRef]
- Fan, X.; Thompson, B.; Wang, L. Effects of sample size, estimation methods, and model specification on structural equation modeling fit indexes. Struct. Equ. Modeling Multidiscip. J. 1999, 6, 56–83. [Google Scholar] [CrossRef]
- Hox, J.J. Multilevel Analysis: Techniques and Applications, 2nd ed.; Routledge/Taylor & Francis Group: London, UK, 2010. [Google Scholar]
- Lai, K.; Green, S.B. The Problem with Having Two Watches: Assessment of Fit When RMSEA and CFI Disagree. Multivar. Behav. Res. 2016, 51, 220–239. [Google Scholar] [CrossRef]
- Browne, M.W.; Cudeck, R. Alternative Ways of Assessing Model Fit. Sociol. Methods Res. 1992, 21, 230–258. [Google Scholar] [CrossRef]
- Byrne, B.M. Structural Equation Modeling with Lisrel, Prelis, and Simplis: Basic Concepts, Applications, and Programming; Lawrence Erlbaum Associates Publishers: Mahwah, NJ, USA, 1998. [Google Scholar]
- Schermelleh-Engel, K.; Moosbrugger, H.; Müller, H. Evaluating the Fit of Structural Equation Models: Tests of Significance and Descriptive Goodness-of-Fit Measures. Methods Psychol. Res. 2003, 8, 23–74. [Google Scholar]
- Wu, A.D.; Li, Z.; Zumbo, B.D. Decoding the Meaning of Factorial Invariance and Updating the Practice of Multi-group Confirmatory Factor Analysis: A Demonstration With TIMSS Data. Pract. Assess. Res. Eval. 2007, 12, 3. [Google Scholar] [CrossRef]
- Chen, F.F. Sensitivity of Goodness of Fit Indexes to Lack of Measurement Invariance. Struct. Equ. Modeling Multidiscip. J. 2007, 14, 464–504. [Google Scholar] [CrossRef]
- Cheung, G.W.; Rensvold, R.B. Evaluating goodness-of-fit indexes for testing measurement invariance. Struct. Equ. Modeling Multidiscip. J. 2002, 9, 233–255. [Google Scholar] [CrossRef]
- Kaiser, H.F. The application of electronic computers to factor analysis. Educ. Psychol. Meas. 1960, 20, 141–151. [Google Scholar] [CrossRef]
- Hubbard, R.; Allen, S.J. A Cautionary Note on the Use of Principal Components Analysis: Supportive Empirical Evidence. Sociol. Methods Res. 1987, 16, 301–308. [Google Scholar] [CrossRef]
- Zwick, W.R.; Velicer, W.F. Comparison of five rules for determining the number of components to retain. Psychol. Bull. 1986, 99, 432–442. [Google Scholar] [CrossRef]
- Hair, J.F., Jr.; Anderson, R.E.; Tatham, R.L.; Black, W.C. Multivariate Data Analysis, 5th ed.; Macmillan: New York, NY, USA, 1998. [Google Scholar]
- Cantril, H. Pattern of Human Concerns; Rutgers University Press: New Brunswick, NJ, USA, 1965. [Google Scholar]
- Helm, D.T. The measurement of happiness. Am. J. Ment. Retard. 2000, 105, 326–335. [Google Scholar] [CrossRef]
- Siegrist, J.; Wahrendorf, M. Work Stress and Health in a Globalized Economy; Springer: Berlin/Heidelberg, Germany, 2016. [Google Scholar]
- Rugulies, R.; Aust, B.; Madsen, I.E. Effort–reward imbalance at work and risk of depressive disorders. A systematic review and meta-analysis of prospective cohort studies. Scand. J. Work. Environ. Health 2017, 43, 294–306. [Google Scholar] [CrossRef]
- Du Prel, J.B.; Siegrist, J.; Borchart, D. The role of leisure-time physical activity in the change of work-related stress (eri) over time. Int. J. Environ. Res. Public Health 2019, 16, 4839. [Google Scholar] [CrossRef]
- Hamer, M. Psychosocial stress and cardiovascular disease risk: The role of physical activity. Psychosom. Med. 2012, 74, 896–903. [Google Scholar] [CrossRef]
- Jonsdottir, I.H.; Rödjer, L.; Hadzibajramovic, E.; Börjesson, M.; Ahlborg, G., Jr. A prospective study of leisure-time physical activity and mental health in Swedish health care workers and social insurance officers. Prev. Med. 2010, 51, 373–377. [Google Scholar] [CrossRef]
- Harvey, S.B.; Øverland, S.; Hatch, S.L.; Wessely, S.; Mykletun, A.; Hotopf, M. Exercise and the prevention of depression: Results of the HUNT cohort study. Am. J. Psychiatry 2018, 175, 28–36. [Google Scholar] [CrossRef]
- Gerrans, P.; Speelman, C.; Campitelli, G. The relationship between personal financial wellness and financial wellbeing: A structural equation modelling approach. J. Fam. Econ. Issues 2014, 35, 145–160. [Google Scholar] [CrossRef]
- Zemtsov, A.A.; Osipova, T.Y. Financial wellbeing as a type of human wellbeing: Theoretical review. Eur. Proc. Soc. Behav. Sci. EpSBS 2016, 7, 385–392. [Google Scholar]
- Diener, E.; Seligman, M.E. Very Happy People. Psychol. Sci. 2002, 13, 81–84. [Google Scholar] [CrossRef]
- Gable, S.L.; Gosnell, C.L. The positive side of close relationships. In Designing Positive Psychology: Taking Stock and Moving Forward; Sheldon, K.M., Kashdan, T.B., Steger, M.F., Eds.; Oxford University Press: Oxford, UK, 2011; pp. 265–279. [Google Scholar] [CrossRef]
- Heaphy, E.D.; Dutton, J.E. Positive social interactions and the human body at work: Linking organizations and physiology. Acad. Manag. Rev. 2008, 33, 137–162. [Google Scholar] [CrossRef]
- Cacioppo, J.T.; Hawkley, L.C.; Norman, G.J.; Berntson, G.G. Social isolation. Ann. N. Y. Acad. Sci. 2011, 1231, 17–22. [Google Scholar] [CrossRef]
- Bruner, J. Narrative, Culture, and Psychology. In Reflective Thinking in Educational Settings: A Cultural Framework; Antonietti, A., Confalonieri, E., Marchetti, A., Eds.; Cambridge University Press: Cambridge, UK, 2014; pp. 221–227. [Google Scholar]
- Fonagy, P.; Target, M.; Steele, H.; Steele, M. Reflective-Functioning Manual, Version 5.0, for Application to Adult Attachment Interviews; University College London: London, UK, 1998. [Google Scholar]
- Fonagy, P.; Target, M. Psychoanalytic Theories: Perspectives from Developmental Psychopathology; Whurr Publishers: London, UK, 2003. [Google Scholar]
- Van IJzendoorn, M.H.; Bakermans-Kranenburg, M.J. The distribution of adult attachment representations in clinical groups: A meta-analytic search for patterns of attachment in 105 AAI studies. Attach. Hum. Dev. 2008, 11, 223–263. [Google Scholar]
- George, C.; West, M.L. The Adult Attachment Projective Picture System: Attachment Theory and Assessment in Adults; Guilford Press: New York, NY, USA, 2012. [Google Scholar]
- Boud, D.; Keogh, R.; Walker, D. Reflection: Turning Experience into Learning; Routledge: London, UK, 2013. [Google Scholar]
- Ghanizadeh, A. The interplay between reflective thinking, critical thinking, self-monitoring, and academic achievement in higher education. High. Educ. 2017, 74, 101–114. [Google Scholar] [CrossRef]
- Paulhus, D.L.; Vazire, S. The Self-Report Method. In Handbook of Research Methods in Personality Psychology; Robins, R., Fraley, R.W., Krueger, R.C., Eds.; Guilford: New York, NY, USA, 2009; pp. 224–239. [Google Scholar]

{kind=link}
{kind=link}
| Sociodemographic Characteristics | Sample 1 N = 366 | Sample 2 N = 421 |
|---|---|---|
| Age, mean ± SD | 49.28 ± 16.93 | 43.48 ± 10.61 |
| Gender | N (%) | N (%) |
| Male | 182 (49.7%) | 195 (46.3%) |
| Female | 184 (50.3%) | 226 (53.7%) |
| Residence | N (%) | N (%) |
| North Italy | 299 (81.7%) | 255 (60.6%) |
| Centre Italy | 27 (7.4%) | 78 (18.5%) |
| South Italy | 32 (8.7%) | 56 (13.3%) |
| Sicily and Sardinia | 8 (2.2%) | 32 (7.6%) |
| Educational level | N (%) | N (%) |
| Middle school or below | Nd | 11 (2,6%) |
| High school | Nd | 252 (59,9%) |
| Graduate school | Nd | 158 (37,5%) |
| Mean annual income (euros) | N (%) | N (%) |
| <21,000 | Nd | 166 (39,4%) |
| 21,000–60,000 | Nd | 214 (50,8%) |
| >60,000 | Nd | 41 (9,7%) |
| Drugs | N (%) | N (%) |
| Yes | 2 (0.5%) | 13 (3.1%) |
| No | 364 (99.5%) | 408 (96.9%) |
| Psychotropic drugs | N (%) | N (%) |
| Yes | 11 (3.0%) | 4 (1.0%) |
| No | 355 (97.0%) | 417 (99.0%) |
| Descriptive Statistics | Max. | Mean | SD | Skewness | Kurtosis | |
|---|---|---|---|---|---|---|
| Scale | Min. | |||||
| MH_F1 | 3 | 30 | 22.14 | 4.9 | −0.84 | 0.84 |
| MH_F2 | 3 | 30 | 19.21 | 5.55 | −0.52 | −0.12 |
| MH_F3 | 11 | 30 | 24.64 | 4.06 | −0.93 | 0.74 |
| MH_F4 | 8 | 20 | 15.14 | 2.28 | −0.08 | −0.01 |
| MH_F5 | 7 | 30 | 23.70 | 4.093 | −1.01 | 1.45 |
| MH_TOT | 53 | 140 | 104.84 | 14.87 | −0.39 | 0.11 |
| MH Items | Factor 1 Psychophysics Status | Factor 2 Financial Status | Factor 3 Relational Private Sphere | Factor 4 Socio-Relational Sphere | Factor 5 Life Perspective |
|---|---|---|---|---|---|
| 1. Come valuti il rapporto con il tuo corpo? | 0.869 | ||||
| 2. Come valuti il tuo livello di equilibrio mentale e fisico? | 0.781 | ||||
| 3. Come valuti il tuo rapporto con te stesso? | 0.883 | ||||
| 4. Quanto ritieni di essere realizzato in questo momento? | 0.538 | ||||
| 5. Quanto sei soddisfatto della tua condizione finanziaria? | 0.929 | ||||
| 6. Quanto ti senti solido finanziariamente? | 0.959 | ||||
| 7. Come valuti la qualità dei tuoi rapporti con i tuoi affetti principali? | −0.829 | ||||
| 8. Quanto ti soddisfa l’atmosfera che si vive nella tua attuale casa? | −0.781 | ||||
| 9. Secondo te, i membri della tua famiglia, quanto ti stimano? | −0.718 | ||||
| 10. Quanto pensi che le persone, in generale, siano felici di relazionarsi con te? | 0.869 | ||||
| 11. Quanto ritieni apprezzati i tuoi comportamenti nella società? | 0.903 | ||||
| 12. Quanto ritieni importante porti degli obiettivi di lungo termine? | 0.877 | ||||
| 13. Quanto ti interessi al tuo miglioramento personale? | 0.725 | ||||
| 14. Quanto ti senti flessibile di fronte ai cambiamenti della vita? | 0.389 | ||||
| % of explained variance | 36.48% | 12.77% | 9.19% | 7.52% | 7.09% |
| Cronbach’s alpha | 0.85 | 0.82 | 0.75 | 0.81 | 0.61 |
| Psychophysics Status | Financial Status | Relational Private Sphere | Socio-Relational Sphere | Life Perspective | |
|---|---|---|---|---|---|
| SHS | 0.46 ** | 0.43 ** | 0.30 ** | 0.35 ** | 0.34 ** |
| WHO-F1 | 0.21 * | 0.12 | 0.14 | 0.15 | −0.03 |
| WHO-F2 | 0.26 ** | 0.14 | 0.04 | 0.11 | 0.02 |
| WHO-F3 | 0.20 * | 0.15 | 0.10 | 0.17 | −0.004 |
| WHO-F4 | 0.11 | 0.13 | 0.03 | 0.18 | 0.05 |
| STAI-1 | −0.51 ** | −0.44 ** | −0.39 ** | −0.35 ** | −0.28 ** |
| STAI-2 | −0.44 ** | −0.31 ** | −0.33 ** | −0.27 ** | −0.28 ** |
| BDI | −0.55 ** | −0.31 ** | −0.37 ** | −0.22 ** | −0.25 ** |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Rizzato, M.; Di Dio, C.; Miraglia, L.; Sam, C.; D’Anzi, S.; Antonelli, M.; Donelli, D. Are You Happy? A Validation Study of a Tool Measuring Happiness. Behav. Sci. 2022, 12, 295. https://doi.org/10.3390/bs12080295
Rizzato M, Di Dio C, Miraglia L, Sam C, D’Anzi S, Antonelli M, Donelli D. Are You Happy? A Validation Study of a Tool Measuring Happiness. Behavioral Sciences. 2022; 12(8):295. https://doi.org/10.3390/bs12080295
Chicago/Turabian StyleRizzato, Matteo, Cinzia Di Dio, Laura Miraglia, Carlo Sam, Sharon D’Anzi, Michele Antonelli, and Davide Donelli. 2022. "Are You Happy? A Validation Study of a Tool Measuring Happiness" Behavioral Sciences 12, no. 8: 295. https://doi.org/10.3390/bs12080295
APA StyleRizzato, M., Di Dio, C., Miraglia, L., Sam, C., D’Anzi, S., Antonelli, M., & Donelli, D. (2022). Are You Happy? A Validation Study of a Tool Measuring Happiness. Behavioral Sciences, 12(8), 295. https://doi.org/10.3390/bs12080295