
Examining Predictors of Different ABA Treatments: A Systematic Review

 , ,
, ,  and
and 
Abstract
1. Introduction
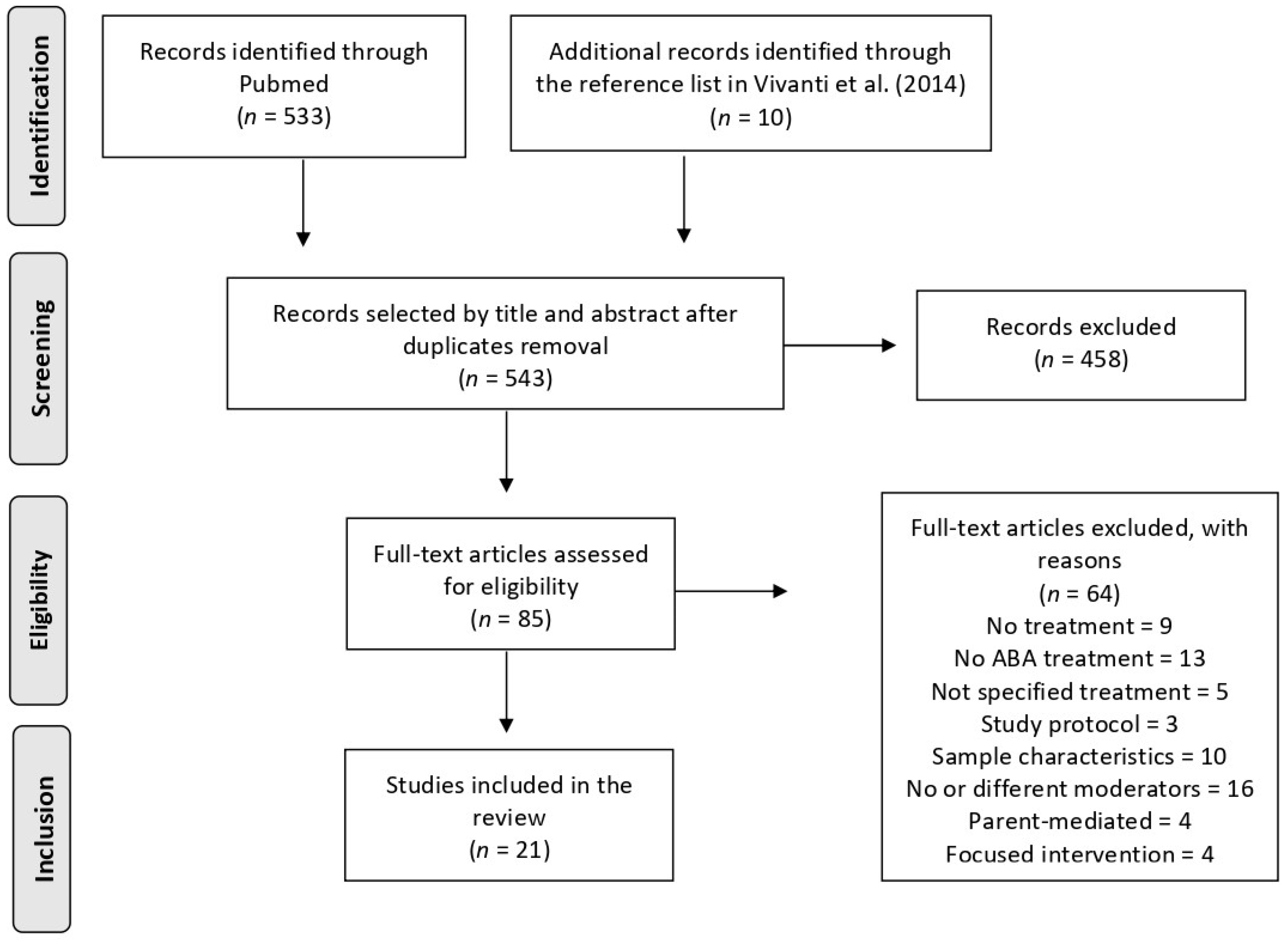
2. Methods: Data Sources and Study Selection
- (a)
- the sample included individuals with a clinical diagnosis of autism, infantile autism, ASD, PDD-NOS, or Asperger’s Syndrome (AS) in childhood (with and without an intellectual disability) and were younger than 13 years old
- (b)
- an ABA-based comprehensive behavioral treatment was administered
- (c)
- predictors and/or moderators were considered and referred to the patient’s individual characteristics
- (d)
- written in English.
3. Results
3.1. Demographics
3.2. Symptom Severity
3.3. Play Skills
3.4. Social Skills
3.5. Cognitive Functioning
3.6. Communication
3.7. Adaptive Behavior
3.8. Maladaptive Behavior
3.9. Developmental Quotient (DQ)
3.10. Emotional and Psychiatric Difficulties
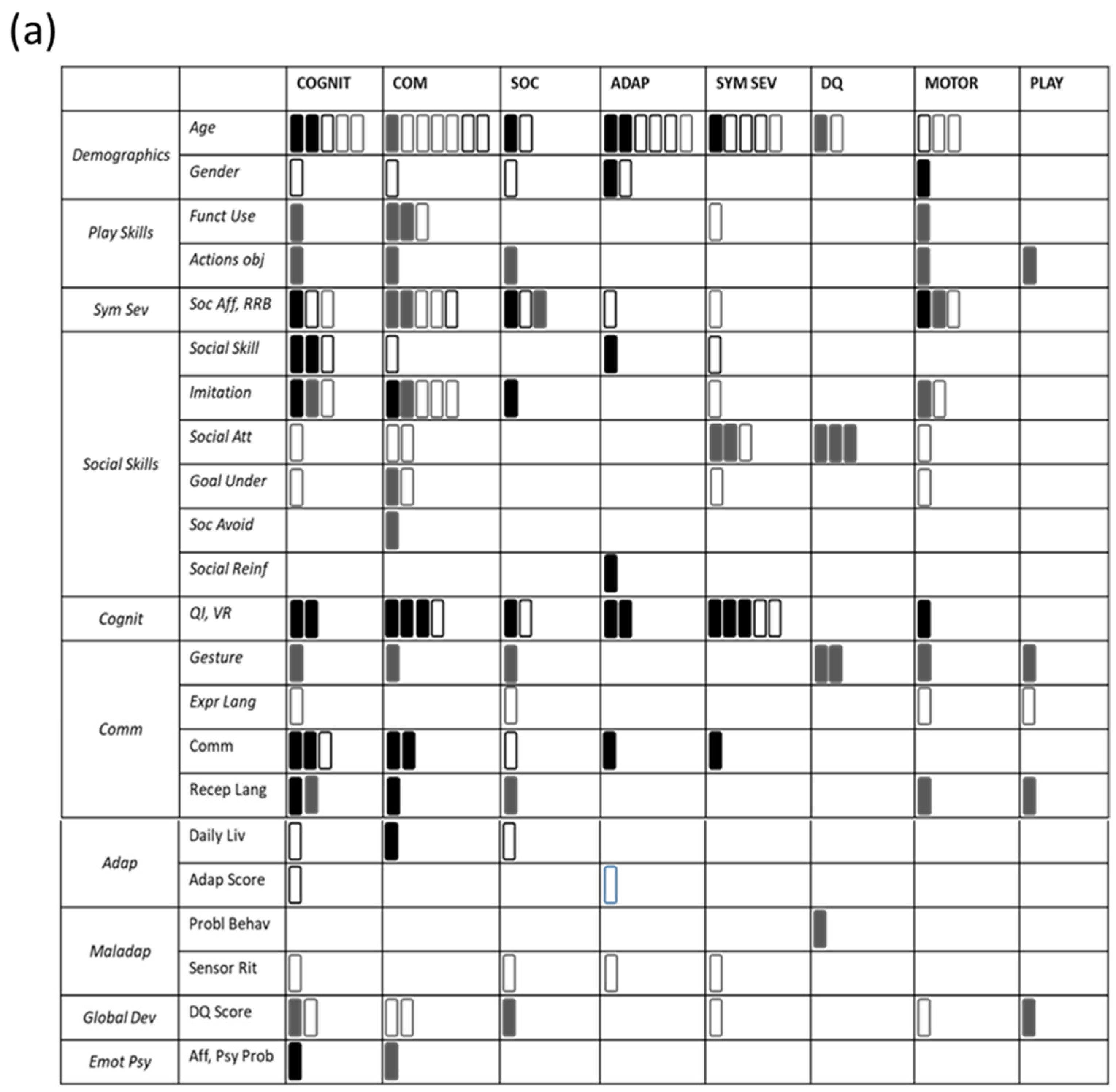
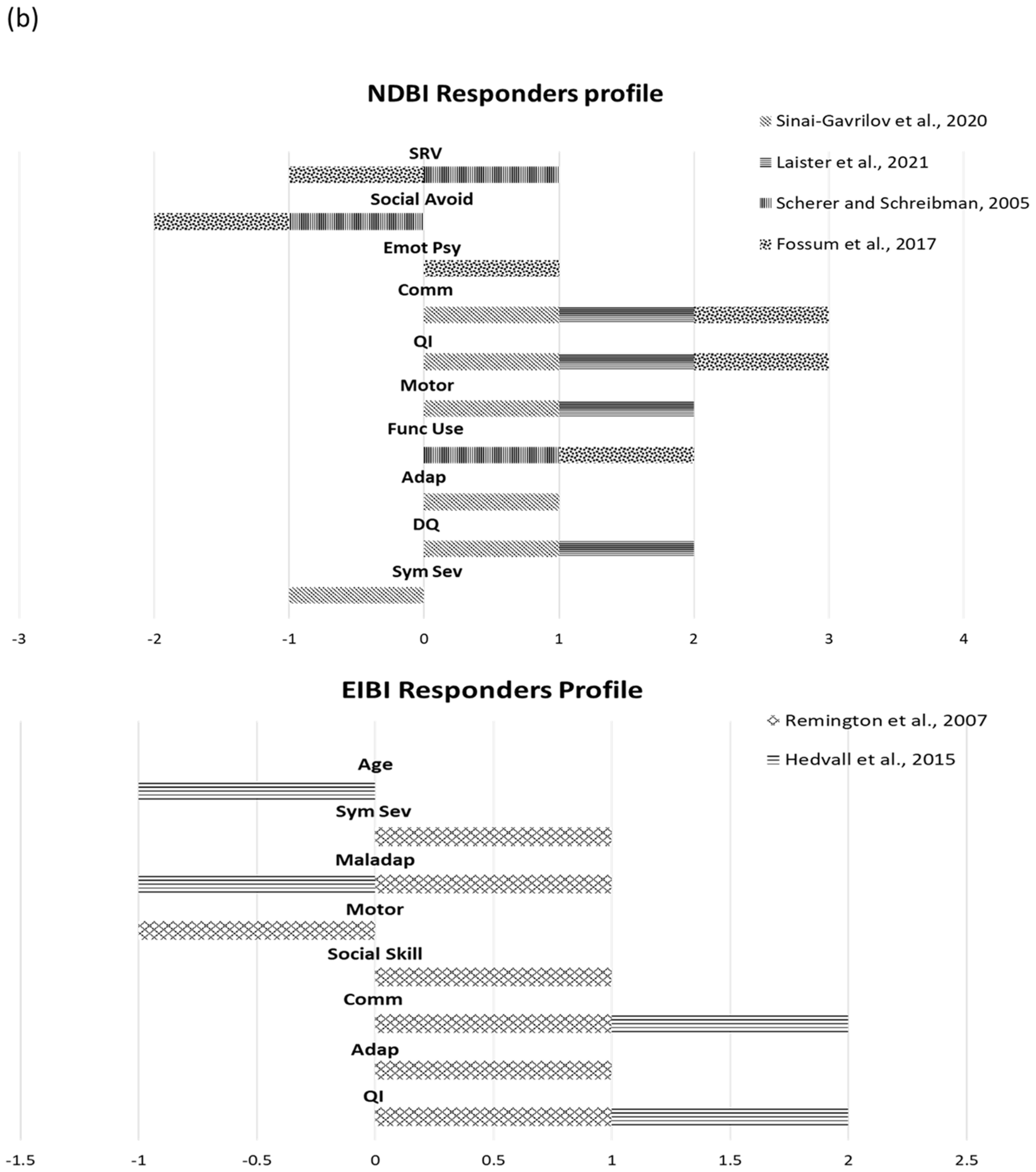
3.11. Responders
4. Discussion
5. Concluding Remarks and Future Directions for Research
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- American Psychiatry Association. Diagnostic and Statistical Manual of Mental Disorders (DSM-V-TR), 5th ed.; American Psychiatry Association: Washington, DC, USA, 2022. [Google Scholar]
- Rogers, S.J.; Vismara, L. Interventions for Infants and Toddlers at Risk for Autism Spectrum Disorder. In Handbook of Autism and Pervasive Developmental Disorders, 4th ed.; John Wiley & Sons, Ltd.: Hoboken, NJ, USA, 2014; ISBN 978-1-118-91138-9. [Google Scholar]
- Landa, R.J. Efficacy of Early Interventions for Infants and Young Children with, and at Risk for, Autism Spectrum Disorders. Int. Rev. Psychiatry 2018, 30, 25–39. [Google Scholar] [CrossRef] [PubMed]
- Smith, T. Discrete Trial Training in the Treatment of Autism. Focus Autism Other Dev. Disabl. 2001, 16, 86–92. [Google Scholar] [CrossRef]
- Schreibman, L.; Dawson, G.; Stahmer, A.C.; Landa, R.; Rogers, S.J.; McGee, G.G.; Kasari, C.; Ingersoll, B.; Kaiser, A.P.; Bruinsma, Y.; et al. Naturalistic Developmental Behavioral Interventions: Empirically Validated Treatments for Autism Spectrum Disorder. J. Autism Dev. Disord. 2015, 45, 2411–2428. [Google Scholar] [CrossRef] [PubMed]
- Vivanti, G.; Zhong, H. Naturalistic Developmental Behavioral Interventions for Children with Autism. In Clinical Guide for Early Interventions for Children with Autism. Best Practices in Child and Adolescence Behavioral Health Care; Vivanti, G., Bottema-Beutel, K., Turner-Brown, L., Eds.; Springer: Cham, Switzerland, 2020; pp. 93–130. ISBN 978-3-030-41159-6. [Google Scholar]
- Hart, B.; Risley, T.R. Incidental Teaching of Language in the Preschool. J. Appl. Behav. Anal. 1975, 8, 411–420. [Google Scholar] [CrossRef] [PubMed]
- McGee, G.G.; Morrier, M.J.; Daly, T. An Incidental Teaching Approach to Early Intervention for Toddlers with Autism. J. Assoc. Pers. Sev. Handicap. 1999, 24, 133–146. [Google Scholar] [CrossRef]
- Koegel, R.L.; Koegel, L.K. Pivotal Response Treatments for Autism: Communication, Social, & Academic Development; Paul H Brookes Publishing: Baltimore, MD, USA, 2006; ISBN 978-1-55766-819-6. [Google Scholar]
- Schreibman, L.; Koegel, R.L. Training for Parents of Children With Autism: Pivotal Responses, Generalization, and Individualization of Interventions. In Psychosocial Treatments for Child and Adolescent Disorders: Empirically Based Strategies for Clinical Practice, 2nd ed.; American Psychological Association: Washington, DC, USA, 2005; pp. 605–631. ISBN 978-1-59147-092-2. [Google Scholar]
- Dawson, G.; Rogers, S.; Munson, J.; Smith, M.; Winter, J.; Greenson, J.; Donaldson, A.; Varley, J. Randomized, Controlled Trial of an Intervention for Toddlers with Autism: The Early Start Denver Model. Pediatrics 2010, 125, e17–e23. [Google Scholar] [CrossRef] [PubMed]
- Rogers, S.J.; Dawson, G. Early Start Denver Model for Young Children with Autism: Promoting Language, Learning, and Engagement; Guilford Press: New York, NY, USA, 2010; ISBN 978-1-60623-632-1. [Google Scholar]
- Ingersoll, B. Pilot Randomized Controlled Trial of Reciprocal Imitation Training for Teaching Elicited and Spontaneous Imitation to Children with Autism. J. Autism Dev. Disord. 2010, 40, 1154–1160. [Google Scholar] [CrossRef]
- Ingersoll, B.; Schreibman, L. Teaching Reciprocal Imitation Skills to Young Children with Autism Using a Naturalistic Behavioral Approach: Effects on Language, Pretend Play, and Joint Attention. J. Autism Dev. Disord. 2006, 36, 487–505. [Google Scholar] [CrossRef]
- Kasari, C.; Freeman, S.; Paparella, T. Joint Attention and Symbolic Play in Young Children with Autism: A Randomized Controlled Intervention Study. J. Child Psychol. Psychiatry 2006, 47, 611–620. [Google Scholar] [CrossRef]
- Kasari, C.; Paparella, T.; Freeman, S.; Jahromi, L.B. Language Outcome in Autism: Randomized Comparison of Joint Attention and Play Interventions. J. Consult Clin. Psychol. 2008, 76, 125–137. [Google Scholar] [CrossRef]
- Vivanti, G.; Prior, M.; Williams, K.; Dissanayake, C. Predictors of Outcomes in Autism Early Intervention: Why Don’t We Know More? Front. Pediatr. 2014, 2, 58. [Google Scholar] [CrossRef]
- Stahmer, A.C.; Schreibman, L.; Cunningham, A.B. Toward a Technology of Treatment Individualization for Young Children with Autism Spectrum Disorders. Brain Res. 2011, 1380, 229–239. [Google Scholar] [CrossRef]
- Chen, Y.-J.; Duku, E.; Georgiades, S. Rethinking Autism Intervention Science: A Dynamic Perspective. Front. Psychiatry 2022, 13, 827406. [Google Scholar] [CrossRef]
- Yoder, P.; Compton, D. Identifying Predictors of Treatment Response. Ment. Retard. Dev. Disabil. Res. Rev. 2004, 10, 162–168. [Google Scholar] [CrossRef]
- Kasari, C.; Sturm, A.; Shih, W. SMARTer Approach to Personalizing Intervention for Children With Autism Spectrum Disorder. J. Speech Lang. Hear. Res. 2018, 61, 2629–2640. [Google Scholar] [CrossRef]
- Klinger, L.G.; Cook, M.L.; Dudley, K.M. Predictors and Moderators of Treatment Efficacy in Children and Adolescents with Autism Spectrum Disorder. J. Clin. Child Adolesc. Psychol. 2021, 50, 517–524. [Google Scholar] [CrossRef]
- Siller, M. Editorial: Individualizing Interventions for Young Children With Autism: Embracing the Next Generation of Intervention Research. J. Am. Acad. Child Adolesc. Psychiatry 2021, 60, 680–682. [Google Scholar] [CrossRef]
- Moher, D.; Liberati, A.; Tetzlaff, J.; Altman, D.G. PRISMA Group Preferred Reporting Items for Systematic Reviews and Meta-Analyses: The PRISMA Statement. PLoS Med. 2009, 6, e1000097. [Google Scholar] [CrossRef]
- Vivanti, G.; Dissanayake, C.; Zierhut, C.; Rogers, S.J. Victorian ASELCC Team Brief Report: Predictors of Outcomes in the Early Start Denver Model Delivered in a Group Setting. J. Autism. Dev. Disord. 2013, 43, 1717–1724. [Google Scholar] [CrossRef]
- Vivanti, G.; Dissanayake, C. Victorian ASELCC Team Outcome for Children Receiving the Early Start Denver Model Before and After 48 Months. J. Autism Dev. Disord. 2016, 46, 2441–2449. [Google Scholar] [CrossRef]
- Sinai-Gavrilov, Y.; Gev, T.; Mor-Snir, I.; Vivanti, G.; Golan, O. Integrating the Early Start Denver Model into Israeli Community Autism Spectrum Disorder Preschools: Effectiveness and Treatment Response Predictors. Autism 2020, 24, 2081–2093. [Google Scholar] [CrossRef]
- Latrèche, K.; Kojovic, N.; Franchini, M.; Schaer, M. Attention to Face as a Predictor of Developmental Change and Treatment Outcome in Young Children with Autism Spectrum Disorder. Biomedicines 2021, 9, 942. [Google Scholar] [CrossRef]
- Robain, F.; Franchini, M.; Kojovic, N.; Wood de Wilde, H.; Schaer, M. Predictors of Treatment Outcome in Preschoolers with Autism Spectrum Disorder: An Observational Study in the Greater Geneva Area, Switzerland. J. Autism Dev. Disord. 2020, 50, 3815–3830. [Google Scholar] [CrossRef]
- Contaldo, A.; Colombi, C.; Pierotti, C.; Masoni, P.; Muratori, F. Outcomes and Moderators of Early Start Denver Model Intervention in Young Children with Autism Spectrum Disorder Delivered in a Mixed Individual and Group Setting. Autism 2020, 24, 718–729. [Google Scholar] [CrossRef]
- Fossum, K.-L.; Williams, L.; Garon, N.; Bryson, S.E.; Smith, I.M. Pivotal Response Treatment for Preschoolers with Autism Spectrum Disorder: Defining a Predictor Profile. Autism Res. 2018, 11, 153–165. [Google Scholar] [CrossRef]
- Schreibman, L.; Stahmer, A.C.; Barlett, V.C.; Dufek, S. Brief Report: Toward Refinement of a Predictive Behavioral Profile for Treatment Outcome in Children with Autism. Res. Autism Spectr. Disord. 2009, 3, 163–172. [Google Scholar] [CrossRef][Green Version]
- Tiura, M.; Kim, J.; Detmers, D.; Baldi, H. Predictors of Longitudinal ABA Treatment Outcomes for Children with Autism: A Growth Curve Analysis. Res. Dev. Disabil. 2017, 70, 185–197. [Google Scholar] [CrossRef]
- Magiati, I.; Moss, J.; Charman, T.; Howlin, P. Patterns of Change in Children with Autism Spectrum Disorders Who Received Community Based Comprehensive Interventions in Their Pre-School Years: A Seven Year Follow-up Study. Res. Autism Spectr. Disord. 2011, 5, 1016–1027. [Google Scholar] [CrossRef]
- Hedvall, Å.; Westerlund, J.; Fernell, E.; Norrelgen, F.; Kjellmer, L.; Olsson, M.B.; Carlsson, L.H.; Eriksson, M.A.; Billstedt, E.; Gillberg, C. Preschoolers with Autism Spectrum Disorder Followed for 2 Years: Those Who Gained and Those Who Lost the Most in Terms of Adaptive Functioning Outcome. J. Autism Dev. Disord. 2015, 45, 3624–3633. [Google Scholar] [CrossRef] [PubMed]
- Laister, D.; Stammler, M.; Vivanti, G.; Holzinger, D. Social-Communicative Gestures at Baseline Predict Verbal and Nonverbal Gains for Children with Autism Receiving the Early Start Denver Model. Autism 2021, 25, 1640–1652. [Google Scholar] [CrossRef] [PubMed]
- Sherer, M.R.; Schreibman, L. Individual Behavioral Profiles and Predictors of Treatment Effectiveness for Children with Autism. J. Consult. Clin. Psychol. 2005, 73, 525–538. [Google Scholar] [CrossRef]
- Smith, I.M.; Koegel, R.L.; Koegel, L.K.; Openden, D.A.; Fossum, K.L.; Bryson, S.E. Effectiveness of a Novel Community-Based Early Intervention Model for Children with Autistic Spectrum Disorder. Am. J. Intellect. Dev. Disabil. 2010, 115, 504–523. [Google Scholar] [CrossRef]
- Sallows, G.O.; Graupner, T.D. Intensive Behavioral Treatment for Children with Autism: Four-Year Outcome and Predictors. Am. J. Ment. Retard. 2005, 110, 417–438. [Google Scholar] [CrossRef]
- Smith, T.; Klorman, R.; Mruzek, D.W. Predicting Outcome of Community-Based Early Intensive Behavioral Intervention for Children with Autism. J. Abnorm. Child Psychol. 2015, 43, 1271–1282. [Google Scholar] [CrossRef]
- Klintwall, L.; Eikeseth, S. Number and Controllability of Reinforcers as Predictors of Individual Outcome for Children with Autism Receiving Early and Intensive Behavioral Intervention: A Preliminary Study. Res. Autism Spectr. Disord. 2012, 6, 493–499. [Google Scholar] [CrossRef]
- Pellecchia, M.; Connell, J.E.; Kerns, C.M.; Xie, M.; Marcus, S.C.; Mandell, D.S. Child Characteristics Associated with Outcome for Children with Autism in a School-Based Behavioral Intervention. Autism 2016, 20, 321–329. [Google Scholar] [CrossRef]
- Ben-Itzchak, E.; Watson, L.R.; Zachor, D.A. Cognitive Ability Is Associated with Different Outcome Trajectories in Autism Spectrum Disorders. J. Autism Dev. Disord. 2014, 44, 2221–2229. [Google Scholar] [CrossRef]
- Remington, B.; Hastings, R.P.; Kovshoff, H.; degli Espinosa, F.; Jahr, E.; Brown, T.; Alsford, P.; Lemaic, M.; Ward, N. Early Intensive Behavioral Intervention: Outcomes for Children with Autism and Their Parents after Two Years. Am. J. Ment. Retard 2007, 112, 418–438. [Google Scholar] [CrossRef]
- Eldevik, S.; Hastings, R.P.; Jahr, E.; Hughes, J.C. Outcomes of Behavioral Intervention for Children with Autism in Mainstream Pre-School Settings. J. Autism Dev. Disord. 2012, 42, 210–220. [Google Scholar] [CrossRef]
- Arick, J.; Loos, L.; Falco, R.; Krug, D. The STAR Program (Strategies for Teaching Based-on Autism Research); Pro-Ed, Inc.: Austin, TX, USA, 2015; ISBN 978-1-4164-0688-4. [Google Scholar]
- Mullen, E.M.; American Guidance Service. Mullen Scales of Early Learning; AGS: Circle Pines, MI, USA, 1995. [Google Scholar]
- Lord, C.; Luyster, R.J.; Gotham, K.; Guthrie, W. Autism Diagnostic Observation Schedule, Second Edition (ADOS-2) Manual (Part II): Toddler Module; Western Psychological Services: Torrance, CA, USA, 2012. [Google Scholar]
- Alpern, G.D. Developmental Profile III; Western Psychological Services: Los Angeles, CA, USA, 2007. [Google Scholar]
- Fenson, L.; Marchman, V.A.; Thal, D.J.; Dale, P.S.; Reznick, J.S. Macarthur-Bates Communicative Development Inventories: Users Guide and Technical Manual, 2nd ed.; Brookes Pub: Baltimore, MD, USA, 2006; ISBN 978-1-55766-884-4. [Google Scholar]
- Sparrow, S.S. Vineland Adaptive Behavior Scales. In Encyclopedia of Clinical Neuropsychology; Kreutzer, J.S., DeLuca, J., Caplan, B., Eds.; Springer: New York, NY, USA, 2011; pp. 2618–2621. ISBN 978-0-387-79948-3. [Google Scholar]
- Griffiths, R. The Abilities of Young Children: A Comprehensive System of Mental Measurement for the First Eight Years of Life; Revised edition; Test Agency Ltd.: London, UK, 1984. [Google Scholar]
- Roid, G.; Sampers, J. Merrill-Palmer-Revised Scales of Development—PsycNET; Stoelting: Wood Dale, IL, USA, 2004. [Google Scholar]
- Schopler, E.; Lansing, M.; Reichler, R.; Marcus, L. Psychoeducational Profile: Third Edition (PEP-3); Pro-Ed: Austin, TX, USA, 2005. [Google Scholar]
- Wechsler, D.; Psychological Corporation; PsychCorp (Firm). WAIS-IV Technical and Interpretive Manual; Pearson: San Antonio, TX, USA, 2008; ISBN 978-0-15-898084-3. [Google Scholar]
- Michalec, D. Bayley Scales of Infant Development: Third Edition. In Encyclopedia of Child Behavior and Development; Goldstein, S., Naglieri, J.A., Eds.; Springer: Boston, MA, USA, 2011; p. 215. ISBN 978-0-387-79061-9. [Google Scholar]
- Reynell, J.K.; Huntley, M. Reynell Developmental Language Scales; NFER-NELSON Publishing Co.: Windsor, PA, USA, 1985. [Google Scholar]
- Cohen, I.L.; Schmidt-Lackner, S.; Romanczyk, R.; Sudhalter, V. The PDD Behavior Inventory: A Rating Scale for Assessing Response to Intervention in Children with Pervasive Developmental Disorder. J. Autism Dev. Disord. 2003, 33, 31–45. [Google Scholar] [CrossRef]
- Harrison, P.; Oakland, T.T. Adaptive Behavior Assessment Syste; John, B., Ed.; Harcourt Assessment: San Antonio, TX, USA, 2000. [Google Scholar]
- Dunn, L.M.; Dunn, L.M.; Whetton, C.; Burley, J. British Picture Vocabulary Scale, 2nd ed.; NFER-Nelson: Windsor, PA, USA, 1997. [Google Scholar]
- Michalec, D.; Henninger, N. Expressive One-Word Picture Vocabulary Test. In Encyclopedia of Clinical Neuropsychology; Kreutzer, J.S., DeLuca, J., Caplan, B., Eds.; Springer: New York, NY, USA, 2011; pp. 1000–1002. ISBN 978-0-387-79948-3. [Google Scholar]
- Elliot, C.D. Differential Ability Scales, 2nd ed.; Harcourt Assessment: San Antonio, TX, USA, 2007. [Google Scholar]
- Lord, C.; Rutter, M.; Le Couteur, A. Autism Diagnostic Interview-Revised: A Revised Version of a Diagnostic Interview for Caregivers of Individuals with Possible Pervasive Developmental Disorders. J. Autism Dev. Disord. 1994, 24, 659–685. [Google Scholar] [CrossRef]
- Bodfish, J.W.; Symons, F.J.; Parker, D.E.; Lewis, M.H. Varieties of Repetitive Behavior in Autism: Comparisons to Mental Retardation. J. Autism Dev. Disord. 2000, 30, 237–243. [Google Scholar] [CrossRef]
- Gadow, K.D.; Sprafkin, J.N. Child Symptom Inventory 4: Screening and Norms Manual; Checkmate Plus: Stony Brook, NY, USA, 2002. [Google Scholar]
- Berument, S.K.; Rutter, M.; Lord, C.; Pickles, A.; Bailey, A. Autism Screening Questionnaire: Diagnostic Validity. Br. J. Psychiatry 1999, 175, 444–451. [Google Scholar] [CrossRef]
- Krug, D.A.; Arick, J.; Almond, P. Behavior Checklist for Identifying Severely Handicapped Individuals with High Levels of Autistic Behavior. J. Child Psychol. Psychiatry 1980, 21, 221–229. [Google Scholar] [CrossRef]
- Iovino, L.; Canniello, F.; Simeoli, R.; Gallucci, M.; Benincasa, R.; D’Elia, D.; Hanley, G.P.; Cammilieri, A.P. A New Adaptation of the Interview-Informed Synthesized Contingency Analyses (IISCA): The Performance-Based IISCA. Eur. J. Behav. Anal. 2022, 1–12. [Google Scholar] [CrossRef]
- Tiger, J.H.; Hanley, G.P.; Bruzek, J. Functional Communication Training: A Review and Practical Guide. Behav. Anal. Pract. 2008, 1, 16–23. [Google Scholar] [CrossRef]
- Rogers, S.J.; Yoder, P.; Estes, A.; Warren, Z.; McEachin, J.; Munson, J.; Rocha, M.; Greenson, J.; Wallace, L.; Gardner, E.; et al. A Multisite Randomized Controlled Trial Comparing the Effects of Intervention Intensity and Intervention Style on Outcomes for Young Children With Autism. J. Am. Acad. Child. Adolesc. Psychiatry 2021, 60, 710–722. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| Study | Study Design and Participants | Treatment Features | Dependent Variables | Moderators | Main Findings |
|---|---|---|---|---|---|
| Vivanti et al., 2013 [25] | Interventional single group Total sample: n = 21 Mage = 38 ± 11.5 months | Group-based ESDM Intensity: 15–25 h/week Duration: 1 year | Visual Reception; Fine Motor; Receptive Language; Expressive Language; Symptoms severity | Functional use of objects; Imitation; Goal Understanding; Symptom severity; Social Attention; Chronological age; DQ | Functional use of objects was positively associated with Visual Reception, Fine Motor and Expressive Language domains gains and alone explained 70% of the variance of the Visual Reception domains; Imitation was positively associated with Visual Reception, Fine Motor and Receptive Language domains gains; Goal Understanding was positively associated with Receptive Language gains and explained alone 30% of the variance of Receptive Language; Symptom severity was negatively associated with Receptive and Expressive Language gains and alone explained 40% of the variance of Expressive Language; Chronological age was negatively associated with Expressive Language; Functional use of objects was not associated with Receptive Language, Symptoms severity Social attention was not associated with Visual Reception, Fine Motor, Receptive and Expressive Language, Symptoms severity; Goal Understanding was not associated with Visual Reception, Fine Motor, Expressive Language, Symptoms severity; Imitation was not associated with Expressive Language, Symptoms severity; Chronological Age was not associated with Visual Reception, Fine Motor, Receptive Language, Symptoms severity; DQ was not associated with Visual Reception, Fine Motor, Receptive and Expressive Language, Symptoms severity; Symptom severity was not associated with Visual Reception, Fine Motor, Symptoms severity |
| Vivanti et al., 2016 [26] | Observational case control study Total sample: n = 60 Younger group (18–48 months): n = 32 Mage = 33.25 ± 7.2 years Older group (48–62 months): n = 28 Mage = 49.54 ± 5.36 years | Group-based ESDM Intensity: 15–25 h/week | Verbal DQ; NonVerbal DQ; Adaptive behavior; Symptom severity | Chronological age | Chronological age was inversely associated with Verbal DQ gains; Changes in NonVerbal DQ, Adaptive behavior, Symptom severity were not associated with Chronological age |
| Sinai-Gavrilov et al., 2020 [27] * | Repeated measures factorial design Total sample: n = 51 PB-ESDM: n = 26 Mage = 43.65 ± 7.37 years MDI group: n = 25 Mage = 45.12 ± 4.8 years | preschool-based ESDM Intensity: 44 h/week Duration: 8 weeks | DQ; Communication; Daily living skills; Socialization; Motor skills; Adaptive behavior | Symptom severity; Fine Motor Skills; Visual Reception; Receptive Language; Expressive Language; DQ; Adaptive behavior; Chronological Age; Gender | High responders had lower Symptom severity, higher DQ and higher Adaptive behavior compared to low responders; No between-group changes emerged for Gender and Chronological age |
| Latrèche et al., 2021 [28] | Longitudinal cohort study Total sample: n = 95 Mage = 2.81 ± 0.65 years ESDM-AF+ group: n = 25 Mage = 2.83 ± 0.48 years ESDM-AF- group: n = 26 Mage = 2.68 ± 0.68 years CT-AF+ group: n = 16 Mage = 3.04 ± 0.55 years CT-AF- group: n = 14 Mage = 2.62 ± 0.67 years | ESDM Intensity: 20 h/week | DQ | Attention to face | Children with more Attention to face at baseline (ASD-AF + ) demonstrated statistically significantly higher DQ scores over time, especially in the verbal domain |
| Robain et al., 2020 [29] | Observational case-control study Total sample: n = 60 Mage = 3.0 ± 0.8 years ESDM-GR group: n = 9 Mage = 2.61 ± 0.39 years ESDM-SR group: n = 13 Mage = 2.57 ± 0.37 years CT-GR group: n = 23 Mage = 3.36 ± 0.72 years CT-SM group: n = 15 Mage = 3.20 ± 1.10 years | ESDM Duration: 1 year | RRB; Social Affect; Symptom severity; DQ | Social orienting; Maladaptive behavior | Social orienting predicted changes in Social Affect, Symptom severity and DQ changes after ESDM treatment, in that ESDM-SR group reported lower Symptom severity and higher DQ over time; Higher Maladaptive behavior were associated with lower DQ after treatment but not with DQ changes over time Social orienting was not predictive of RRB mean change over time |
| Contaldo et al., 2020 [30] | Pre-post single-group design Total sample: n = 32 Mage = 28.8 ± 6.5 months | Community-based ESDM Intensity: 4 h/week Duration: 1 year | Communication; Socialization; Cognition and Play; Motor skills; Number of learning objective acquired by each child in a month; Adaptive functioning; First Communicative Gestures; Actions with objects; Imitation; Receptive Lexical Quotient; DQ | First Communicative Gestures; Actions with objects; Receptive Lexical Quotient; Word Production; Imitation; DQ; Symptom severity; Chronological age | Number of First Communicative Gestures were positively associated with gains in Communication, Socialization, Cognition and Play, and Motor skills and with the number of learning objective acquired by each child in a month; Actions with objects were positively associated with gains in Socialization, Cognition and Play, and Motor skills and with the number of learning objective acquired by each child in a month; Receptive Lexical Quotient was positively associated with gains in Socialization, Cognition and Play, and Motor skills and with the number of learning objective acquired by each child in a month; DQ was positively associated with gains in Socialization, Cognition and Play, and with the number of learning objective acquired by each child in a month Symptom severity was negatively associated with gains in Socialization and Motor skills and with the number of learning objective acquired by each child in a month; Actions with objects and Receptive Lexical Quotient were not associated with the Communication domain; Symptom severity was not associated with Communication and Cognition and Play domains; DQ was not associated with Communication and Motor skills domains; Chronological age, Word Production, and Imitation were not associated with any changes neither with the rate of learning objectives acquisition |
| Fossum et al., 2018 [31] * | Prospective single-subject design Total sample: n = 57 Mage = 47.84 ± 8.86 years | PRT; Duration: 1 year | Communication | Toy contact; Social avoidance; Verbal self-stimulatory behavior; Positive affect; Cognitive abilities; Expressive language; Chronological age; Symptoms severity | Higher levels of Expressive Language, Cognitive ability, Toy contact, Positive affect, lower Social avoidance and Verbal self-stimulatory behavior at baseline appeared to predict treatment outcome in Expressive language; Chronological age and Symptom severity were not predictive of Communication outcome |
| Schreibman et al., 2009 [32] * | Single-subject multiple baseline design across participants Total sample: n = 6 Rage = 2–4 years Nonresponders with high toy contact: n = 3 Mage = 26 month Nonresponders with low avoidance: n = 3 Mage = 34.67 months | PRT + DTT Intensity: 18 h/week | Communication | Toy contact; low avoidance | Higher Toy contact is a key characteristic of PRT treatment responders, whereas low avoidance is not associated with a better response to PRT |
| Tiura et al., 2017 [33] | Longitudinal study Total sample: n = 35 Mage = 2.10 years | EIBI Intensity: 9–30 h/week | Communication; Social–emotional; Adaptive behavior; Physical development | Cognitive functioning; Speaking English as the primary language; Gender; Symptom severity; Chronological age | Children with higher Cognitive functioning predicted rapid growth across the four dependent variables; Participants who spoke English as a primary language had faster growth rates in the social–emotional and physical development domains; Male participants tended to improve more quickly in the areas of Adaptive behavior and Physical development; Children with higher Symptom severity tended to improve at a slower pace in the Physical development domain; Speaking English as the primary language was not associated with Adaptive behavior and Communication; Gender was not associated with Social–emotional and Communication; Symptom severity was not associated with Adaptive, Social–emotional and Communication; Chronological age did not predict growth rate |
| Magiati et al., 2011 [34] | Longitudinal study Total sample: n = 36 Mage = 3.4 ± 0.6 years | EIBI Intensity: 15–40 h/week; Duration: 22–90 months | Cognitive functioning; Language skills; Adaptive behavior; Symptom severity | Cognitive functioning; Language skills; Adaptive behavior; Symptom severity; Chronological age | Cognitive functioning, Language and Adaptive behavior skills were predictive of outcomes after 4–5 years of intervention; Chronological age was not associated with treatment outcomes; Symptom severity was not predictive of outcomes |
| Hedvall et al., 2015 [35] | Observational Case Crossover Initial group: n = 198 Mage 39 ± 8.5 months GM group: n = 30 Mage = 41 ± 8.7 months LM group: n = 23 Mage = 33 ± 7.9 months | EIBI Intensity: 15–40 h/week Duration: 2 years | Adaptive behavior | Cognitive functioning; Chronological age; Developmental milestones at 18 months; Regression; Symptom severity; Gender | Children in the LM group had been referred at significantly lower ages; Symptom severity was significantly higher in the LM group as compared to the GM group; Most of the children in the GM group significantly had passed the expected developmental milestones at the 18-month check-up; The GM group had a significantly higher cognitive level |
| Laister et al., 2021 [36] * | Longitudinal pre-post design Total sample: n = 56 Mage = 41.96 ± 7.5 years | ESDM Duration: 12 months | Social skills; Language skills | Verbal DQ; Nonverbal DQ; Fine Motor skills; Gross Motor skills; Visual Reception; Receptive Language; Expressive Language; Gestural approach behavior; Social approach behaviors; Problem behavior; Chronological Age | Verbal and Nonverbal DQ, Fine Motor skills, Visual Reception, and Gestural Approach Behavior were significantly higher for the High responder group who gains the most in social and language skills; Receptive Language, Expressive Language, Problem Behavior, Chronological Age, and Social approach behaviors were not significantly different for the two groups; Gestural approach behaviors were found to significantly predict Verbal and Nonverbal DQ; |
| Sherer and Schreibman, 2005 [37] * | Multiple baseline design across participants Total sample: n = 6 Responders: n = 3 Mage = 3:3 years; Nonresponders: n = 3 Mage = 4:2 years | PRT Intensity: 10 h/week | Language Skills; Adaptive Behavior; IQ; Symptom severity; Play skills | Toy Contact/Object Manipulation; Approach behaviors; Avoidant behaviors; Verbal Self-Stimulatory behaviors; Nonverbal Self-Stimulatory Behaviors | Children with higher Toy contact/Object Manipulation, Approach behavior and Verbal Self-Stimulatory behaviors but lower Avoidant behaviors responded better to treatment than children in the nonresponder group |
| Smith et al., 2010 [38] | Observational case control study Total sample: n = 45 Mage = 50 ± 10 months | EIBI Intensity: 14 h/week Duration: 12 months | Expressive Language; Receptive Language Adaptive behavior; Symptoms severity; Problem behavior | IQ | Significant main effects of IQ on Expressive and Receptive Language, Communication, Adaptive behavior and Symptom severity were found; Non-significant effects of IQ on Problem Behavior emerged |
| Sallows and Graupner, 2005 [39] | Interventional Parallel Group Study Total sample: n = 23 UCLA group: n = 13 Mage = 33.2 ± 3.89 months Parent group: n = 10 Mage = 34.2 ± 5.06 months | UCLA EIBI Intensity: 40 h/week Duration: 2 years | IQ; Language skills; Social skills; Early Learning Measure | IQ; Daily Living skills; Social skills; Communication; Symptoms severity; Early Learning Measure | IQ was best predicted by Early Learning Measure, IQ, Social skills, lower Symptom severity; Daily Living skills and Communication did not predict changes in IQ; Language skills was predicted by the ability to imitate, Daily Living skills and Communication; IQ, Social skills and Symptom severity did not predict changes in Language skills; Social skills was predicted by the ability to imitate, Early Learning Measure, Symptom severity; Daily Living skills, IQ and Communication did not predict Social skills |
| Smith et al., 2015 [40] | Interventional Single Group Study Total sample: n = 71 Mage = 3.27 ± 0.65 years | EIBI Intensity: ≥15 h/week Duration: 24 months | IQ; Adaptive behavior; Symptom severity; Social skills; Communication; RRB | Chronological age; IQ; Social Engagement; Social approach; Joint attention; Imitation; Sensorimotor rituals | Higher values of outcome variables at intake predicted better outcome in IQ, Adaptive behavior, Symptom severity; Lower Chronological age predicted better outcome for IQ, Adaptive behavior, and Communication; Higher IQ predicted IQ level, Adaptive behavior and lower Symptom severity; Higher Social Engagement scores at intake predicted higher IQ and Adaptive behavior; Sensorimotor rituals did not predict any outcome; Social engagement did not predict Symptom severity outcome; Chronological age did not predict Social Interaction deficit and Symptom severity; IQ did not predict Social Interaction and RRB |
| Klintwall and Eikeseth, 2012 [41] | Interventional Single Group Study Total sample: n = 21 Mage = 3.7 Rge = 2.3–4.11 years | EIBI Intensity: 20 h/week | Learning rate of Adaptive behavior | Automatic reinforcers; Socially-mediated reinforcers; Chronological age; Adaptive behavior | The number of Socially-mediated reinforcers was found to be a significant predictor of increase in the learning rate, vice-versa for the number of automatic reinforcers; Chronological age was also found to be a significant predictor of learning rate: older children exhibited larger treatment gains; Adaptive behavior did not predict learning rate |
| Pellecchia et al., 2016 [42] | Interventional Single group Study Total sample: n = 152 Mage = 6 ± 0.9 years | STAR Duration: 3 years | IQ | Language and Communication; Adaptive behavior; Challenging behavior; Symptom severity; Social skills; Chronological age; Symptoms associated with co-occurring psychiatric difficulties | Social anxiety symptoms significantly predicted IQ outcome, in that increased social phobia was associated with a decrease in cognitive functioning; Chronological age significantly predicted IQ changes, in that lower age was associated with a decrease in cognitive functioning;Language and Communication, Adaptive skills, Challenging behaviors, Symptom severity, Social skills and other co-occuring psychiatric difficulties did not predict any change in IQ |
| Ben-Itzchak et al., 2014 [43] | Interventional Parallel Study Total sample: n = 46 Mage = 25.5 ± 3.95 months | ABA-based treatment Intensity: 20 h/week | Communication; Daily Living skills; Socialization; Motor skills; Fine Motor; Visual Reception; Receptive Language; Expressive Language; Symptoms severity | IQ | Higher IQ was associated with increases in Communication, Daily Living skills, Socialization; A lower IQ was associated with an increase in Fine Motor and Receptive Language; IQ did not predict Symptom severity |
| Remington et al., 2007 [44] * | Interventional Parallel Group Study Total sample: n = 44 Range = 30–40 months EIBI group n = 23 Mage = 35.7 ± 4.0 months Control group n = 21 Mage = 38.4 ± 4.4 months | EIBI Intensity: 25.6 h/week Duration: 2 years | IQ; Language skills | IQ; Adaptive behavior; Communication; Socialization; Daily Living skills; Motor skills; Problems behavior; Symptoms severity | Children who responded better to intervention had higher IQ, higher Adaptive behavior, Communication and Social Skills scores, lower Motor skills scores, more Problems behaviors and higher Symptoms severity; No between-group differences were found for Daily living skills |
| Eldevik et al., 2012 [45] | Interventional Parallel Group Study Total sample: n = 43 EIBI group: n = 31 Mage = 42.2 ± 9 months TAU group: n = 12 Mage = 46.2 ± 12.4 months | EIBI Intensity: 10–20 h/week Duration: 2 years | Communication; Socialization; Daily Living skills; Adaptive behavior; IQ | Chronological age; IQ; Adaptive behavior; Gender; Diagnosis | Chronological age positively correlated with gains in Adaptive behavior scores; IQ positively correlated with changes in the Socialization domain;Gender was not associated with any of the dependent variables |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Cerasuolo, M.; Simeoli, R.; Nappo, R.; Gallucci, M.; Iovino, L.; Frolli, A.; Rega, A. Examining Predictors of Different ABA Treatments: A Systematic Review. Behav. Sci. 2022, 12, 267. https://doi.org/10.3390/bs12080267
Cerasuolo M, Simeoli R, Nappo R, Gallucci M, Iovino L, Frolli A, Rega A. Examining Predictors of Different ABA Treatments: A Systematic Review. Behavioral Sciences. 2022; 12(8):267. https://doi.org/10.3390/bs12080267
Chicago/Turabian StyleCerasuolo, Mariangela, Roberta Simeoli, Raffaele Nappo, Maria Gallucci, Luigi Iovino, Alessandro Frolli, and Angelo Rega. 2022. "Examining Predictors of Different ABA Treatments: A Systematic Review" Behavioral Sciences 12, no. 8: 267. https://doi.org/10.3390/bs12080267
APA StyleCerasuolo, M., Simeoli, R., Nappo, R., Gallucci, M., Iovino, L., Frolli, A., & Rega, A. (2022). Examining Predictors of Different ABA Treatments: A Systematic Review. Behavioral Sciences, 12(8), 267. https://doi.org/10.3390/bs12080267