
Randomized Trial on the Effects of a Mindfulness Intervention on Temperament, Anxiety, and Depression: A Multi-Arm Psychometric Study




Abstract
:1. Introduction
2. Materials and Methods
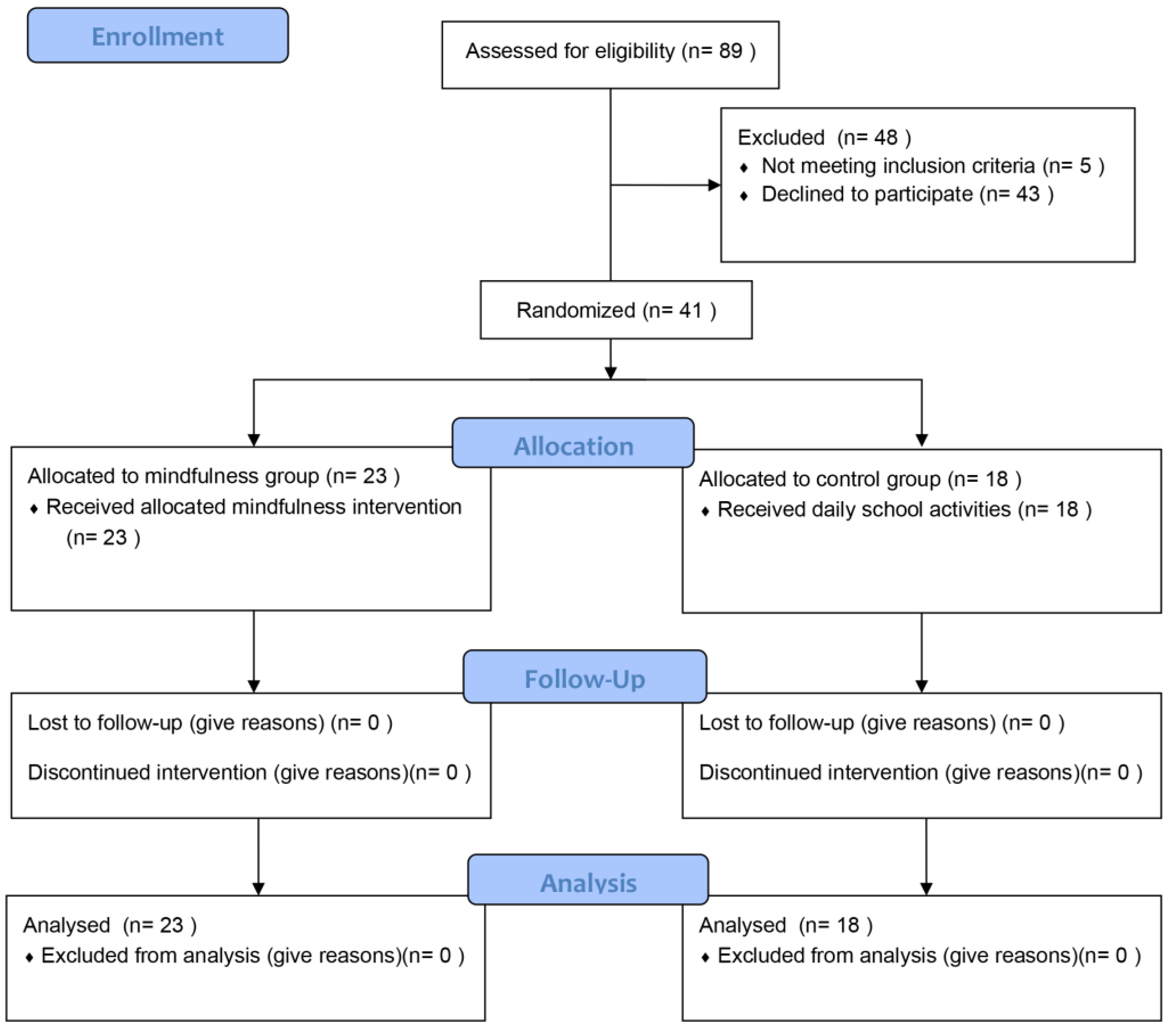
2.1. Trial Design
2.2. Participants
2.3. Interventions
2.4. Outcome Measures
2.4.1. Primary Outcome Measures
2.4.2. Secondary Outcome Measures
2.5. Sample Size
2.6. Randomization
2.7. Statistical Analysis
3. Results
3.1. Group Comparisons
3.2. GLM Regressions
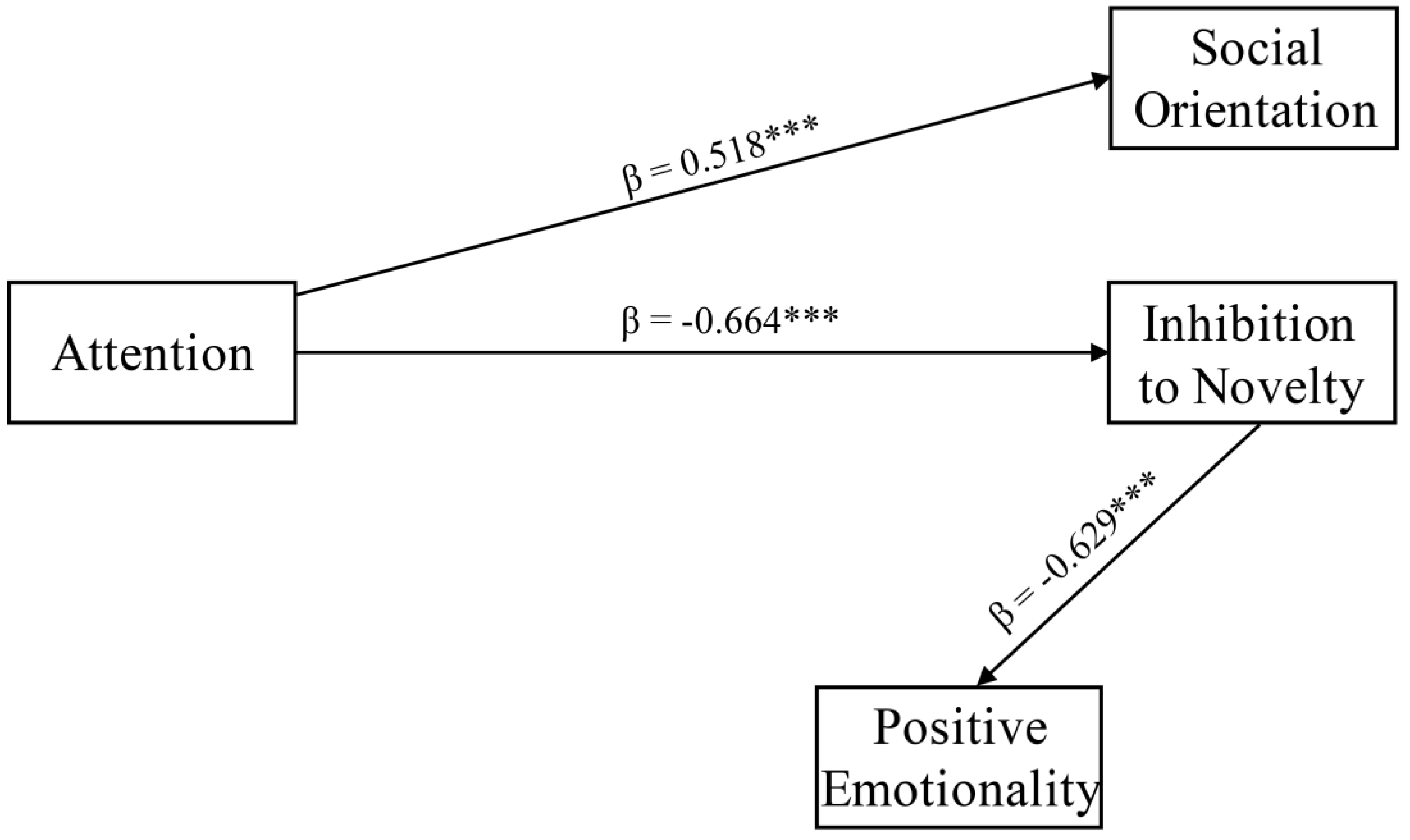
3.3. Path Analysis
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Kabat-Zinn, J. Wherever You Go, There You Are: Mindfulness Meditation in Everyday Life; Hyperion: New York, NY, USA, 1994; ISBN 978-0-7868-8070-6. [Google Scholar]
- Chiesa, A.; Malinowski, P. Mindfulness-Based Approaches: Are They All the Same? J. Clin. Psychol. 2011, 67, 404–424. [Google Scholar] [CrossRef] [PubMed]
- Kabat-Zinn, J. Full Catastrophe Living: Using the Wisdom of Your Body and Mind to Face Stress, Pain, and Illness; Bantam Dell: New York, NY, USA, 2013. [Google Scholar]
- Lutz, A.; Dunne, J.D.; Davidson, R.J. Meditation and the Neuroscience of Consciousness: An Introduction. In The Cambridge Handbook of Consciousness; Zelazo, P.D., Moscovitch, M., Thompson, E., Eds.; Cambridge University Press: Cambridge, UK, 2007; pp. 499–552. ISBN 978-0-511-81678-9. [Google Scholar]
- Segal, Z.V.; Williams, J.M.G.; Teasdale, J.D.; Kabat-Zinn, J. Mindfulness-Based Cognitive Therapy for Depression, 2nd ed.; paperback edition.; The Guilford Press: New York, NY, USA; London, UK, 2018; ISBN 978-1-4625-3703-7. [Google Scholar]
- Tang, Y.-Y.; Hölzel, B.K.; Posner, M.I. The Neuroscience of Mindfulness Meditation. Nat. Rev. Neurosci. 2015, 16, 213–225. [Google Scholar] [CrossRef] [PubMed]
- Conversano, C.; Ciacchini, R.; Orrù, G.; Di Giuseppe, M.; Gemignani, A.; Poli, A. Mindfulness, Compassion, and Self-Compassion Among Health Care Professionals: What’s New? A Systematic Review. Front. Psychol. 2020, 11, 1683. [Google Scholar] [CrossRef] [PubMed]
- Poli, A.; Gemignani, A.; Soldani, F.; Miccoli, M. A Systematic Review of a Polyvagal Perspective on Embodied Contemplative Practices as Promoters of Cardiorespiratory Coupling and Traumatic Stress Recovery for PTSD and OCD: Research Methodologies and State of the Art. Int. J. Environ. Res. Public Health 2021, 18, 11778. [Google Scholar] [CrossRef]
- Keng, S.-L.; Smoski, M.J.; Robins, C.J. Effects of Mindfulness on Psychological Health: A Review of Empirical Studies. Clin. Psychol. Rev. 2011, 31, 1041–1056. [Google Scholar] [CrossRef] [Green Version]
- World Health Organization. The World Health Report 1998—Life in the 21st Century: A Vision for All; World Health Organization: Geneva, Switzerland, 1998. [Google Scholar]
- Parmentier, F.B.R.; García-Toro, M.; García-Campayo, J.; Yañez, A.M.; Andrés, P.; Gili, M. Mindfulness and Symptoms of Depression and Anxiety in the General Population: The Mediating Roles of Worry, Rumination, Reappraisal and Suppression. Front. Psychol. 2019, 10, 506. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hofmann, S.G.; Sawyer, A.T.; Witt, A.A.; Oh, D. The Effect of Mindfulness-Based Therapy on Anxiety and Depression: A Meta-Analytic Review. J. Consult. Clin. Psychol. 2010, 78, 169–183. [Google Scholar] [CrossRef]
- Siegel, D.J. Mindfulness Training and Neural Integration: Differentiation of Distinct Streams of Awareness and the Cultivation of Well-Being. Soc. Cogn. Affect Neurosci. 2007, 2, 259–263. [Google Scholar] [CrossRef]
- Kerr, C.E.; Sacchet, M.D.; Lazar, S.W.; Moore, C.I.; Jones, S.R. Mindfulness Starts with the Body: Somatosensory Attention and Top-down Modulation of Cortical Alpha Rhythms in Mindfulness Meditation. Front. Hum. Neurosci. 2013, 7, 12. [Google Scholar] [CrossRef] [Green Version]
- Bruno, R.M.; Stea, F.; Sicari, R.; Ghiadoni, L.; Taddei, S.; Ungar, A.; Bonuccelli, U.; Tognoni, G.; Cintoli, S.; Del Turco, S.; et al. Vascular Function Is Improved After an Environmental Enrichment Program: The Train the Brain–Mind the Vessel Study. Hypertension 2018, 71, 1218–1225. [Google Scholar] [CrossRef]
- Janz, P.; Dawe, S.; Wyllie, M. Mindfulness-Based Program Embedded Within the Existing Curriculum Improves Executive Functioning and Behavior in Young Children: A Waitlist Controlled Trial. Front. Psychol. 2019, 10, 2052. [Google Scholar] [CrossRef] [PubMed]
- Poli, A.; Maremmani, A.G.I.; Chiorri, C.; Mazzoni, G.-P.; Orrù, G.; Kolacz, J.; Porges, S.W.; Conversano, C.; Gemignani, A.; Miccoli, M. Item Reduction, Psychometric and Biometric Properties of the Italian Version of the Body Perception Questionnaire—Short Form (BPQ-SF): The BPQ-22. Int. J. Environ. Res. Public Health 2021, 18, 3835. [Google Scholar] [CrossRef] [PubMed]
- Bond, L.A.; Hauf, A.M.H. Taking Stock and Putting Stock in Primary Prevention: Characteristics of Effective Programs. J. Prim. Prev. 2004, 24, 199–221. [Google Scholar] [CrossRef]
- Orri, M.; Côté, S.M.; Tremblay, R.E.; Doyle, O. Impact of an Early Childhood Intervention on the Home Environment, and Subsequent Effects on Child Cognitive and Emotional Development: A Secondary Analysis. PLoS ONE 2019, 14, e0219133. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Balasundaram, P.; Avulakunta, I.D. Human Growth and Development. In StatPearls; StatPearls Publishing: Treasure Island, FL, USA, 2021. [Google Scholar]
- Melli, G.; Moulding, R.; Poli, A. Is It More Disgusting If I Think about It? Examining the Interaction of Obsessive Beliefs and Disgust Propensity in Clinical Obsessive-Compulsive Disorder. J. Obs. Compuls. Relat. Disord. 2016, 11, 74–81. [Google Scholar] [CrossRef]
- Melli, G.; Poli, A.; Chiorri, C.; Olatunji, B.O. Is Heightened Disgust Propensity Truly a Risk Factor for Contamination-Related Obsessive-Compulsive Disorder? Behav. Ther. 2019, 50, 621–629. [Google Scholar] [CrossRef] [Green Version]
- Melli, G.; Bulli, F.; Carraresi, C.; Tarantino, F.; Gelli, S.; Poli, A. The Differential Relationship between Mental Contamination and the Core Dimensions of Contact Contamination Fear. J. Anxiety Disord. 2017, 45, 9–16. [Google Scholar] [CrossRef]
- Poli, A.; Melli, G.; Radomsky, A.S. Different Disgust Domains Specifically Relate to Mental and Contact Contamination Fear in Obsessive-Compulsive Disorder: Evidence From a Path Analytic Model in an Italian Clinical Sample. Behav. Ther. 2019, 50, 380–394. [Google Scholar] [CrossRef]
- Conversano, C.; Poli, A.; Ciacchini, R.; Hitchcott, P.; Bazzichi, L.; Gemignani, A. A Psychoeducational Intervention Is a Treatment for Fibromyalgia Syndrome. Clin. Exp. Rheumatol. 2019, 37 (Suppl. S116), 98–104. [Google Scholar]
- Poli, A.; Melli, G.; Ghisi, M.; Bottesi, G.; Sica, C. Anxiety Sensitivity and Obsessive-Compulsive Symptom Dimensions: Further Evidence of Specific Relationships in a Clinical Sample. Pers. Individ. Differ. 2017, 109, 130–136. [Google Scholar] [CrossRef]
- Melli, G.; Carraresi, C.; Poli, A.; Bailey, R. The Role of Metacognitive Beliefs in Health Anxiety. Pers. Individ. Differ. 2016, 89, 80–85. [Google Scholar] [CrossRef]
- Melli, G.; Bailey, R.; Carraresi, C.; Poli, A. Metacognitive Beliefs as a Predictor of Health Anxiety in a Self-Reporting Italian Clinical Sample. Clin. Psychol. Psychother. 2018, 25, 263–271. [Google Scholar] [CrossRef] [PubMed]
- Melli, G.; Carraresi, C.; Poli, A.; Marazziti, D.; Pinto, A. The Role of Guilt Sensitivity in OCD Symptom Dimensions. Clin. Psychol. Psychother. 2017, 24, 1079–1089. [Google Scholar] [CrossRef] [PubMed]
- Flook, L.; Goldberg, S.B.; Pinger, L.; Bonus, K.; Davidson, R.J. Mindfulness for Teachers: A Pilot Study to Assess Effects on Stress, Burnout, and Teaching Efficacy: Mindfulness for Teachers. Mind Brain Educ. 2013, 7, 182–195. [Google Scholar] [CrossRef] [Green Version]
- Kuyken, W.; Weare, K.; Ukoumunne, O.C.; Vicary, R.; Motton, N.; Burnett, R.; Cullen, C.; Hennelly, S.; Huppert, F. Effectiveness of the Mindfulness in Schools Programme: Non-Randomised Controlled Feasibility Study. Br. J Psychiatry 2013, 203, 126–131. [Google Scholar] [CrossRef] [Green Version]
- Bostic, J.Q.; Nevarez, M.D.; Potter, M.P.; Prince, J.B.; Benningfield, M.M.; Aguirre, B.A. Being Present at School. Child Adolesc. Psychiatr. Clin. N. Am. 2015, 24, 245–259. [Google Scholar] [CrossRef]
- Schonert-Reichl, K.A.; Oberle, E.; Lawlor, M.S.; Abbott, D.; Thomson, K.; Oberlander, T.F.; Diamond, A. Enhancing Cognitive and Social–Emotional Development through a Simple-to-Administer Mindfulness-Based School Program for Elementary School Children: A Randomized Controlled Trial. Dev. Psychol. 2015, 51, 52–66. [Google Scholar] [CrossRef] [Green Version]
- Semple, R.J.; Lee, J.; Rosa, D.; Miller, L.F. A Randomized Trial of Mindfulness-Based Cognitive Therapy for Children: Promoting Mindful Attention to Enhance Social-Emotional Resiliency in Children. J Child Fam. Stud. 2010, 19, 218–229. [Google Scholar] [CrossRef]
- van den Heuvel, M.I.; Johannes, M.A.; Henrichs, J.; Van den Bergh, B.R.H. Maternal Mindfulness during Pregnancy and Infant Socio-Emotional Development and Temperament: The Mediating Role of Maternal Anxiety. Early Hum. Dev. 2015, 91, 103–108. [Google Scholar] [CrossRef]
- Hoffmann, T.C.; Glasziou, P.P.; Boutron, I.; Milne, R.; Perera, R.; Moher, D.; Altman, D.G.; Barbour, V.; Macdonald, H.; Johnston, M.; et al. Better Reporting of Interventions: Template for Intervention Description and Replication (TIDieR) Checklist and Guide. BMJ 2014, 348, g1687. [Google Scholar] [CrossRef] [Green Version]
- Saltzman, A. Mindfulness: A Guide For Teachers. 2012. Available online: https://www.contemplativemind.org/Mindfulness-A_Teachers_Guide.pdf (accessed on 2 March 2022).
- Emerson, L.-M.; Leyland, A.; Hudson, K.; Rowse, G.; Hanley, P.; Hugh-Jones, S. Teaching Mindfulness to Teachers: A Systematic Review and Narrative Synthesis. Mindfulness 2017, 8, 1136–1149. [Google Scholar] [CrossRef] [Green Version]
- Miller, C.J.; Brooker, B. Mindfulness Programming for Parents and Teachers of Children with ADHD. Complementary Ther. Clin. Pract. 2017, 28, 108–115. [Google Scholar] [CrossRef] [PubMed]
- Axia, G. QUIT: Questionari Italiani del Temperamento; Erickson: Trento, Italy, 2002; ISBN 978-88-7946-430-7. [Google Scholar]
- Newcomer, P.L.; Barenbaum, E.M.; Bryant, B.R. Depression and Anxiety in Youth Scale; PRO-ED: Austin, TX, USA, 1994. [Google Scholar]
- Newcomer, P.L.; Barenbaum, E.M.; Bryant, B.R. Test TAD: Test Dell’ansia e Depressione Nell’infanzia e Adolescenza; Erickson: Trento, Italy, 1997; ISBN 978-88-7946-164-1. [Google Scholar]
- Julious, S.A. Sample Size of 12 per Group Rule of Thumb for a Pilot Study. Pharmaceut. Statist. 2005, 4, 287–291. [Google Scholar] [CrossRef]
- Bell, M.L.; Whitehead, A.L.; Julious, S.A. Guidance for Using Pilot Studies to Inform the Design of Intervention Trials with Continuous Outcomes. CLEP 2018, 10, 153–157. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Feeley, N.; Cossette, S.; Côté, J.; Héon, M.; Stremler, R.; Martorella, G.; Purden, M. The Importance of Piloting an RCT Intervention. Can. J. Nurs Res. 2009, 41, 85–99. [Google Scholar] [PubMed]
- Menard, S. Applied Logistic Regression Analysis; SAGE Publications, Inc.: Newbury Park, CA, USA, 2002; ISBN 978-0-7619-2208-7. [Google Scholar]
- Park, E.-Y. Path Analysis of Strength, Spasticity, Gross Motor Function, and Health-Related Quality of Life in Children with Spastic Cerebral Palsy. Health Qual. Life Outcomes 2018, 16, 70. [Google Scholar] [CrossRef] [Green Version]
- Marsh, H.W.; Hau, K.-T.; Wen, Z. In Search of Golden Rules: Comment on Hypothesis-Testing Approaches to Setting Cutoff Values for Fit Indexes and Dangers in Overgeneralizing Hu and Bentler’s (1999) Findings. Struct. Equ. Model. A Multidiscip. J. 2004, 11, 320–341. [Google Scholar] [CrossRef]
- Schulz, K.F.; Altman, D.G.; Moher, D. CONSORT 2010 Statement: Updated Guidelines for Reporting Parallel Group Randomised Trials. PLoS Med. 2010, 7, e1000251. [Google Scholar] [CrossRef]
- Brown, T.A. Methodology in the social sciences. In Confirmatory Factor Analysis for Applied Research, 2nd ed.; The Guilford Press: New York, NY, USA; London, UK, 2015; ISBN 978-1-4625-1536-3. [Google Scholar]
- Griffin, M.M.; Steinbrecher, T.D. Large-Scale Datasets in Special Education Research. In International Review of Research in Developmental Disabilities; Elsevier: Amsterdam, The Netherlands, 2013; Volume 45, pp. 155–183. ISBN 978-0-12-407760-7. [Google Scholar]
- Zenner, C.; Herrnleben-Kurz, S.; Walach, H. Mindfulness-Based Interventions in Schools—a Systematic Review and Meta-Analysis. Front. Psychol. 2014, 5, 603. [Google Scholar] [CrossRef] [Green Version]
- Tymofiyeva, O.; Henje, E.; Yuan, J.P.; Huang, C.-Y.; Connolly, C.G.; Ho, T.C.; Bhandari, S.; Parks, K.C.; Sipes, B.S.; Yang, T.T.; et al. Reduced Anxiety and Changes in Amygdala Network Properties in Adolescents with Training for Awareness, Resilience, and Action (TARA). Neuro. Clin. 2021, 29, 102521. [Google Scholar] [CrossRef]
- Braschi, C.; Capsoni, S.; Narducci, R.; Poli, A.; Sansevero, G.; Brandi, R.; Maffei, L.; Cattaneo, A.; Berardi, N. Intranasal Delivery of BDNF Rescues Memory Deficits in AD11 Mice and Reduces Brain Microgliosis. Aging Clin. Exp. Res. 2021, 33, 1223–1238. [Google Scholar] [CrossRef] [PubMed]
- Kallapiran, K.; Koo, S.; Kirubakaran, R.; Hancock, K. Review: Effectiveness of Mindfulness in Improving Mental Health Symptoms of Children and Adolescents: A Meta-Analysis. Child. Adolesc. Ment. Health 2015, 20, 182–194. [Google Scholar] [CrossRef] [PubMed]
- Crescentini, C.; Capurso, V.; Furlan, S.; Fabbro, F. Mindfulness-Oriented Meditation for Primary School Children: Effects on Attention and Psychological Well-Being. Front. Psychol. 2016, 7, 805. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Luby, J.; Belden, A.; Sullivan, J.; Hayen, R.; McCadney, A.; Spitznagel, E. Shame and Guilt in Preschool Depression: Evidence for Elevations in Self-Conscious Emotions in Depression as Early as Age 3. J. Child. Psychol. Psychiatry 2009, 50, 1156–1166. [Google Scholar] [CrossRef] [Green Version]
- Wang, W.; Song, S.; Wang, J.; Liu, Q.; Huang, L.; Chen, X. Shame on You! When and Why Failure-Induced Shame Impedes Employees’ Learning From Failure in the Chinese Context. Front. Psychol. 2021, 12, 725277. [Google Scholar] [CrossRef]
- Goldsmith, H.H.; Buss, A.H.; Plomin, R.; Rothbart, M.K.; Thomas, A.; Chess, S.; Hinde, R.A.; McCall, R.B. Roundtable: What Is Temperament? Four Approaches. Child. Dev. 1987, 58, 505–529. [Google Scholar] [CrossRef]
- Felver, J.C.; Tipsord, J.M.; Morris, M.J.; Racer, K.H.; Dishion, T.J. The Effects of Mindfulness-Based Intervention on Children’s Attention Regulation. J. Atten. Disord. 2017, 21, 872–881. [Google Scholar] [CrossRef] [Green Version]
- Dignath, D.; Eder, A.B.; Steinhauser, M.; Kiesel, A. Conflict Monitoring and the Affective-Signaling Hypothesis—An Integrative Review. Psychon. Bull. Rev. 2020, 27, 193–216. [Google Scholar] [CrossRef]
- Wilson, B.J. The Role of Attentional Processes in Children’s Prosocial Behavior with Peers: Attention Shifting and Emotion. Dev. Psychopathol. 2003, 15, 313–329. [Google Scholar] [CrossRef]
- Mukherjee, S.; Srinivasan, N.; Kumar, N.; Manjaly, J.A. Perceptual Broadening Leads to More Prosociality. Front. Psychol. 2018, 9, 1821. [Google Scholar] [CrossRef]
- Olivo, D.; Di Ciano, A.; Mauro, J.; Giudetti, L.; Pampallona, A.; Kubera, K.M.; Hirjak, D.; Wolf, R.C.; Sambataro, F. Neural Responses of Benefiting From the Prosocial Exchange: The Effect of Helping Behavior. Front. Psychol. 2021, 12, 606858. [Google Scholar] [CrossRef] [PubMed]
- Yakobi, O.; Smilek, D.; Danckert, J. The Effects of Mindfulness Meditation on Attention, Executive Control and Working Memory in Healthy Adults: A Meta-Analysis of Randomized Controlled Trials. Cogn. Res. 2021, 45, 543–560. [Google Scholar] [CrossRef]
- Pérez-Edgar, K.; Bar-Haim, Y.; McDermott, J.M.; Chronis-Tuscano, A.; Pine, D.S.; Fox, N.A. Attention Biases to Threat and Behavioral Inhibition in Early Childhood Shape Adolescent Social Withdrawal. Emotion 2010, 10, 349–357. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pérez-Edgar, K.; Reeb-Sutherland, B.C.; McDermott, J.M.; White, L.K.; Henderson, H.A.; Degnan, K.A.; Hane, A.A.; Pine, D.S.; Fox, N.A. Attention Biases to Threat Link Behavioral Inhibition to Social Withdrawal over Time in Very Young Children. J. Abnorm. Child. Psychol. 2011, 39, 885–895. [Google Scholar] [CrossRef] [Green Version]
- Poli, A.; Gemignani, A.; Conversano, C. The Psychological Impact of SARS-CoV-2 Quarantine: Observations through the Lens of the Polyvagal Theory. Clin. Neuropsychiatry 2020, 17, 112–114. [Google Scholar] [CrossRef]
- Brooks, S.K.; Webster, R.K.; Smith, L.E.; Woodland, L.; Wessely, S.; Greenberg, N.; Rubin, G.J. The Psychological Impact of Quarantine and How to Reduce It: Rapid Review of the Evidence. Lancet 2020, 395, 912–920. [Google Scholar] [CrossRef] [Green Version]
- Saurabh, K.; Ranjan, S. Compliance and Psychological Impact of Quarantine in Children and Adolescents Due to COVID-19 Pandemic. Indian J. Pediatr. 2020, 87, 532–536. [Google Scholar] [CrossRef]
- Tortella, G.R.; Seabra, A.B.; Padrão, J.; Díaz-San Juan, R. Mindfulness and Other Simple Neuroscience-Based Proposals to Promote the Learning Performance and Mental Health of Students during the COVID-19 Pandemic. Brain Sci. 2021, 11, 552. [Google Scholar] [CrossRef]
- Matiz, A.; Fabbro, F.; Paschetto, A.; Cantone, D.; Paolone, A.R.; Crescentini, C. Positive Impact of Mindfulness Meditation on Mental Health of Female Teachers during the COVID-19 Outbreak in Italy. Int. J. Environ. Res. Public Health 2020, 17, 6450. [Google Scholar] [CrossRef]
- Lindsay, E.K.; Young, S.; Brown, K.W.; Smyth, J.M.; Creswell, J.D. Mindfulness Training Reduces Loneliness and Increases Social Contact in a Randomized Controlled Trial. Proc. Natl. Acad. Sci. USA 2019, 116, 3488–3493. [Google Scholar] [CrossRef] [Green Version]
- Hashizume, S.; Nakano, M.; Kubota, K.; Sato, S.; Himuro, N.; Kobayashi, E.; Takaoka, A.; Fujimiya, M. Mindfulness Intervention Improves Cognitive Function in Older Adults by Enhancing the Level of MiRNA-29c in Neuron-Derived Extracellular Vesicles. Sci. Rep. 2021, 11, 21848. [Google Scholar] [CrossRef] [PubMed]
- Perona-Garcelán, S.; García-Montes, J.M.; Rodríguez-Testal, J.F.; López-Jiménez, A.M.; Ruiz-Veguilla, M.; Ductor-Recuerda, M.J.; Benítez-Hernández, M.d.M.; Arias-Velarde, M.Á.; Gómez-Gómez, M.T.; Pérez-Álvarez, M. Relationship Between Childhood Trauma, Mindfulness, and Dissociation in Subjects With and Without Hallucination Proneness. J. Trauma Dissociation 2014, 15, 35–51. [Google Scholar] [CrossRef] [PubMed]
- Poli, A.; Maremmani, A.G.I.; Conversano, C.; Muscas, G.; Gemignani, A.; Pozza, A.; Miccoli, M. Different Dissociation and Alexithymia Domains Specifically Relate to Patients with Psychogenic Non-Epileptic Seizures (PNES) and with PNES and Comorbid Epilepsy (PNES+EP). J. Affect. Disord. Rep. 2022, 7, 100296. [Google Scholar] [CrossRef]
- D’Antoni, F.; Feruglio, S.; Matiz, A.; Cantone, D.; Crescentini, C. Mindfulness Meditation Leads To Increased Dispositional Mindfulness And Interoceptive Awareness Linked To A Reduced Dissociative Tendency. J. Trauma Dissociation 2021, 23, 8–23. [Google Scholar] [CrossRef]

{kind=link}
{kind=link}
| Variable | Control—Pre | Mindfulness—Pre | p | Control—Post | Mindfulness—Post | p |
|---|---|---|---|---|---|---|
| 1. TAD-Anxiety | 105 (12.24) | 109.5 (13.07) | 0.378 | 99.70 (17.89) | 102.75 (13.42) | 0.269 |
| 102.5 [35] | 115 [40] | 90 [65] | 100 [45] | |||
| 2. TAD-Depression | 106.07 (17.34) | 105.75 (9.07) | 0.271 | 102.35 (14.15) | 103.5 (15.31) | 0.386 |
| 105 [65] | 102.5 [40] | 105 [60] | 105 [60] | |||
| 3. QUIT-SO | 4.37 (0.97) | 4.55 (0.84) | 0.738 | 4.35 (0.98) | 5.32 (0.61) | 0.002 |
| 4.19 [3.5] | 4.63 [2.87] | 4.15 [3.5] | 5.5 [1.87] | |||
| 4. QUIT-IN | 3.84 (1.27) | 3.08 (0.94) | 0.198 | 3.82 (1.25) | 2.06 (0.67) | <0.001 |
| 4.11 [4.44] | 3.11 [3.78] | 4 [4.44] | 1.89 [2.56] | |||
| 5. QUIT-MA | 3.05 (0.95) | 3.59 (1.18) | 0.207 | 3.03 (0.93) | 3.53 (0.44) | 0.004 |
| 2.8 [3.9] | 3.4 [3.7] | 2.8 [3.9] | 3.5 [1.9] | |||
| 6. QUIT-PE | 2.91 (1.34) | 3.61 (0.84) | 0.132 | 2.90 (1.34) | 4.86 (0.56) | <0.001 |
| 2.61 [4.34] | 3.67 [4] | 2.65 [4.4] | 5 [1.89] | |||
| 7. QUIT-NE | 3.61 (1.44) | 3.45 (0.94) | 0.792 | 3.59 (1.45) | 2.14 (0.68) | 0.004 |
| 3.61 [4.44] | 3.44 [3.22] | 3.6 [4.44] | 2.11 [2.44] | |||
| 8. QUIT-AT | 3.21 (1.11) | 3.88 (0.81) | 0.566 | 3.19 (1.13) | 4.93 (0.74) | <0.001 |
| 3.11 [3.66] | 3.89 [3.44] | 3.1 [3.66] | 5.11 [2.78] |
| Variable | Control—Pre | Control—Post | p | Mindfulness—Pre | Mindfulness—Post | p |
|---|---|---|---|---|---|---|
| 1. TAD-Anxiety | 105 (12.24) | 99.70 (17.89) | 0.602 | 109.5 (13.07) | 102.75 (13.42) | 0.006 |
| 102.5 [35] | 90 [65] | 115 [40] | 100 [45] | |||
| 2. TAD-Depression | 106.07 (17.34) | 102.35 (14.15) | 0.775 | 105.75 (9.07) | 103.5 (15.31) | 0.756 |
| 105 [65] | 105 [60] | 102.5 [40] | 105 [60] | |||
| 3. QUIT-SO | 4.37 (0.97) | 4.35 (0.98) | 0.908 | 4.55 (0.84) | 5.32 (0.61) | <0.001 |
| 4.19 [3.5] | 4.15 [3.5] | 4.63 [2.87] | 5.5 [1.87] | |||
| 4. QUIT-IN | 3.84 (1.27) | 3.82 (1.25) | 0.893 | 3.08 (0.94) | 2.06 (0.67) | <0.001 |
| 4.11 [4.44] | 4 [4.44] | 3.11 [3.78] | 1.89 [2.56] | |||
| 5. QUIT-MA | 3.05 (0.95) | 3.03 (0.93) | 0.991 | 3.59 (1.18) | 3.53 (0.44) | 0.715 |
| 2.8 [3.9] | 2.8 [3.9] | 3.4 [3.7] | 3.5 [1.9] | |||
| 6. QUIT-PE | 2.91 (1.34) | 2.90 (1.34) | 0.954 | 3.61 (0.84) | 4.86 (0.56) | <0.001 |
| 2.61 [4.34] | 2.65 [4.4] | 3.67 [4] | 5 [1.89] | |||
| 7. QUIT-NE | 3.61 (1.44) | 3.59 (1.45) | 0.881 | 3.45 (0.94) | 2.14 (0.68) | <0.001 |
| 3.61 [4.44] | 3.6 [4.44] | 3.44 [3.22] | 2.11 [2.44] | |||
| 8. QUIT-AT | 3.21 (1.11) | 3.19 (1.13) | 0.871 | 3.88 (0.81) | 4.93 (0.74) | <0.001 |
| 3.11 [3.66] | 3.1 [3.66] | 3.89 [3.44] | 5.11 [2.78] |
| Predictor | β | t | p |
|---|---|---|---|
| Criterion: QUIT-SO | |||
| Adjusted R2 = 0.447 | |||
| QUIT-IN | −0.038 (0.294) | −0.132 | 0.897 |
| QUIT-PE | 0.052 (0.309) | 0.169 | 0.868 |
| QUIT-NE | −0.244 (0.206) | 1.186 | 0.251 |
| QUIT-AT | 0.571 (0.211) | 2.705 | 0.015 |
| Criterion: QUIT-IN | |||
| Adjusted R2 = 0.705 | |||
| QUIT-SO | −0.025 (0.189) | −0.132 | 0.897 |
| QUIT-PE | −0.536 (0.214) | −2.503 | 0.022 |
| QUIT-NE | 0.071 (0.171) | 0.418 | 0.681 |
| QUIT-AT | 0.394 (0.178) | −2.213 | 0.040 |
| Criterion: QUIT-PE | |||
| Adjusted R2 = 0.624 | |||
| QUIT-SO | 0.03 (0.179) | 0.169 | 0.868 |
| QUIT-IN | −0.482 (0.193) | −2.503 | 0.022 |
| QUIT-NE | −0.273 (0.149) | −1.829 | 0.084 |
| QUIT-AT | −0.031 (0.190) | −0.166 | 0.87 |
| Criterion: QUIT-NE | |||
| Adjusted R2 = 0.465 | |||
| QUIT-SO | 0.297 (0.25) | 1.186 | 0.251 |
| QUIT-IN | 0.135 (0.322) | 0.418 | 0.681 |
| QUIT-PE | −0.574 (0.314) | −1.829 | 0.084 |
| QUIT-AT | −0.239 (0.27) | −0.883 | 0.389 |
| Criterion: QUIT-AT | |||
| Adjusted R2 = 0.67 | |||
| QUIT-SO | 0.506 (0.187) | 2.705 | 0.015 |
| QUIT-IN | −0.543 (0.245) | −2.213 | 0.04 |
| QUIT-PE | −0.048 (0.291) | −0.166 | 0.87 |
| QUIT-NE | −0.174 (0.197) | −0.883 | 0.389 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Poli, A.; Maremmani, A.G.I.; Gemignani, A.; Miccoli, M. Randomized Trial on the Effects of a Mindfulness Intervention on Temperament, Anxiety, and Depression: A Multi-Arm Psychometric Study. Behav. Sci. 2022, 12, 74. https://doi.org/10.3390/bs12030074
Poli A, Maremmani AGI, Gemignani A, Miccoli M. Randomized Trial on the Effects of a Mindfulness Intervention on Temperament, Anxiety, and Depression: A Multi-Arm Psychometric Study. Behavioral Sciences. 2022; 12(3):74. https://doi.org/10.3390/bs12030074
Chicago/Turabian StylePoli, Andrea, Angelo Giovanni Icro Maremmani, Angelo Gemignani, and Mario Miccoli. 2022. "Randomized Trial on the Effects of a Mindfulness Intervention on Temperament, Anxiety, and Depression: A Multi-Arm Psychometric Study" Behavioral Sciences 12, no. 3: 74. https://doi.org/10.3390/bs12030074
APA StylePoli, A., Maremmani, A. G. I., Gemignani, A., & Miccoli, M. (2022). Randomized Trial on the Effects of a Mindfulness Intervention on Temperament, Anxiety, and Depression: A Multi-Arm Psychometric Study. Behavioral Sciences, 12(3), 74. https://doi.org/10.3390/bs12030074