
Physical Exercise Ameliorates Anxiety, Depression and Sleep Quality in College Students: Experimental Evidence from Exercise Intensity and Frequency


Abstract
:1. Introduction
2. Materials and Methods
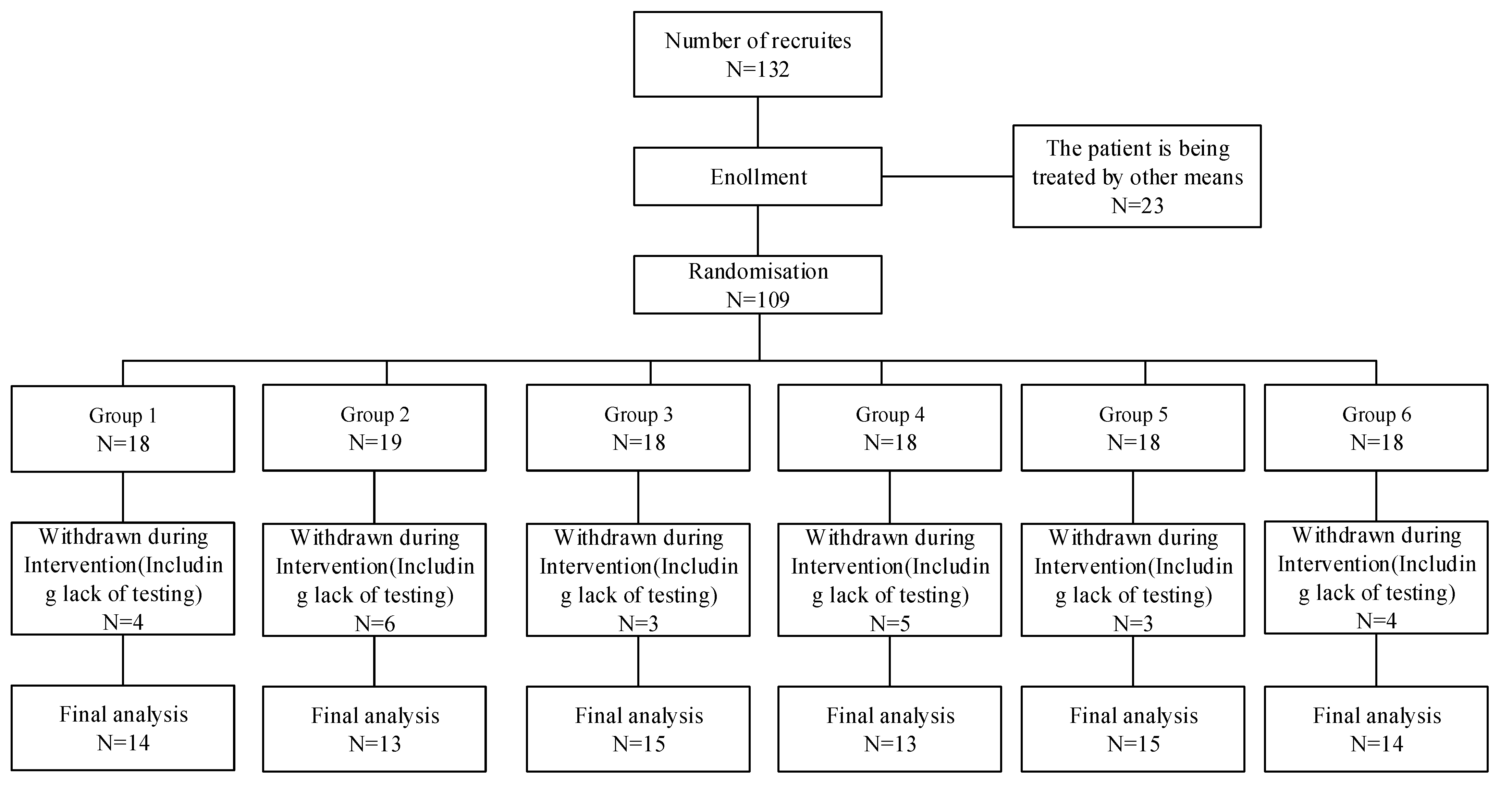
2.1. Participants
2.2. Study Methodology
2.3. Measuring Tools
2.4. Statistical Analysis
3. Results
3.1. Participant Characteristics
3.2. Baseline Analysis of Anxiety Symptoms, Depression Symptoms and Sleep Quality of College Students Pre-Test
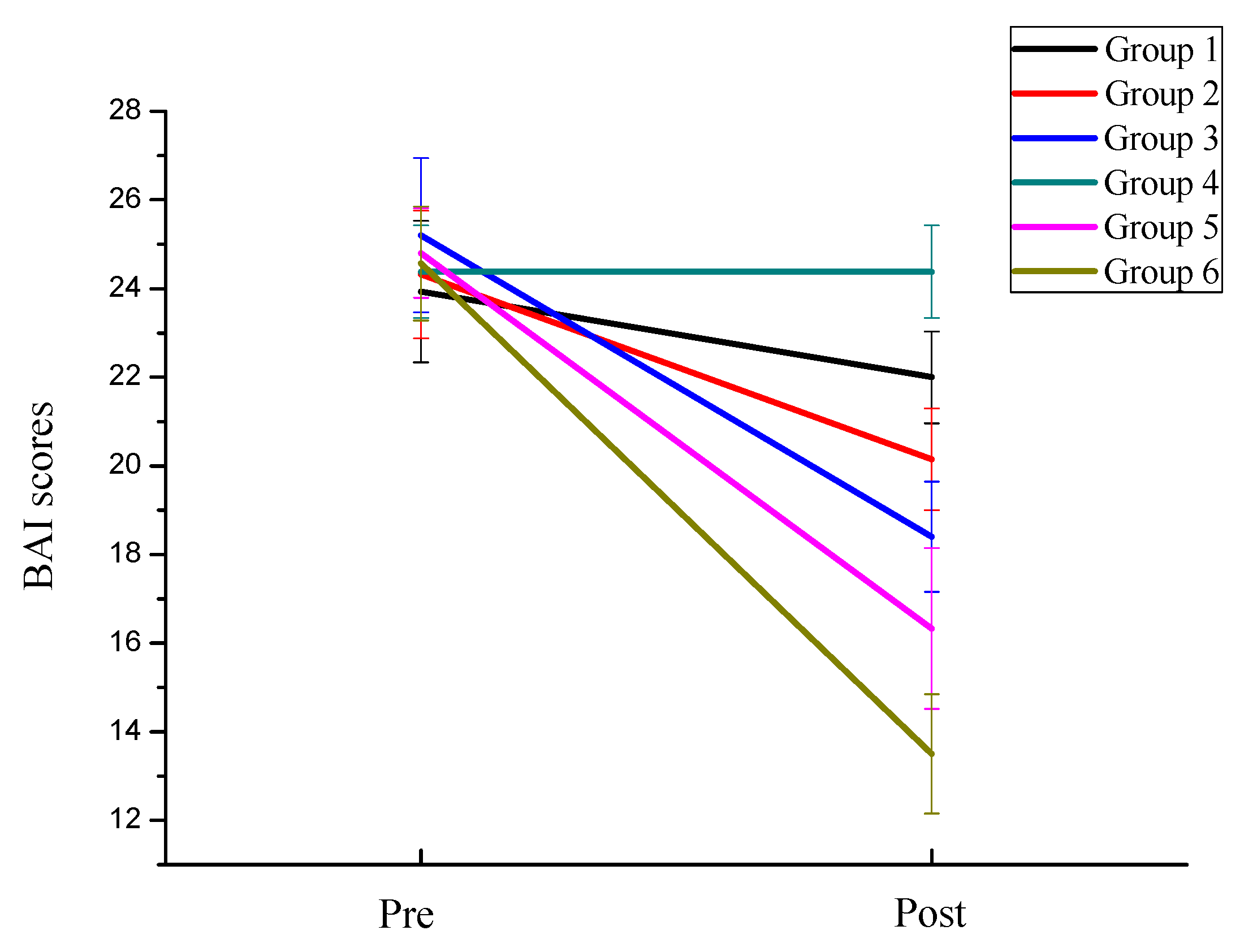
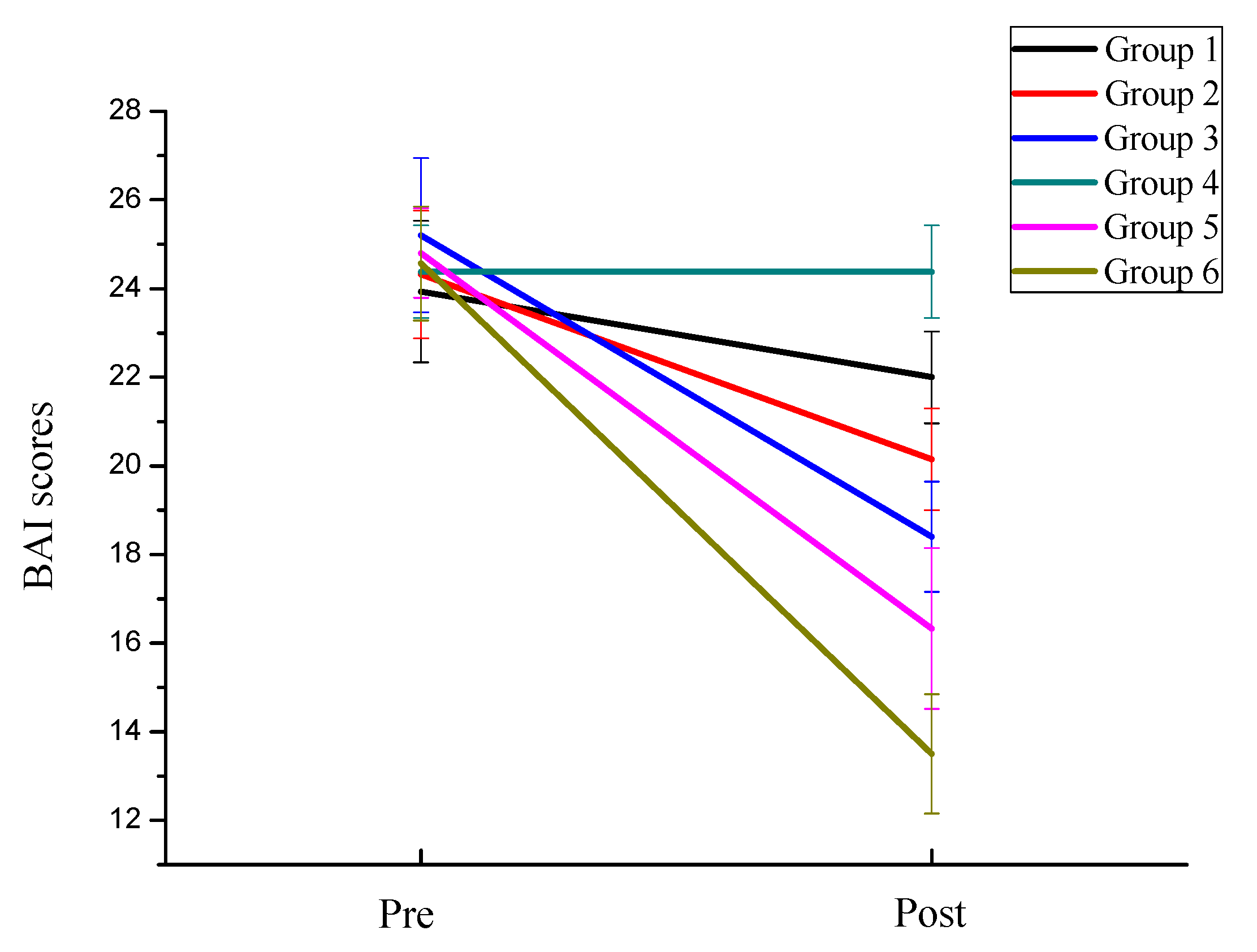
3.2.1. Effects of Exercise Intensity and Frequency on Anxiety Symptoms of College Students
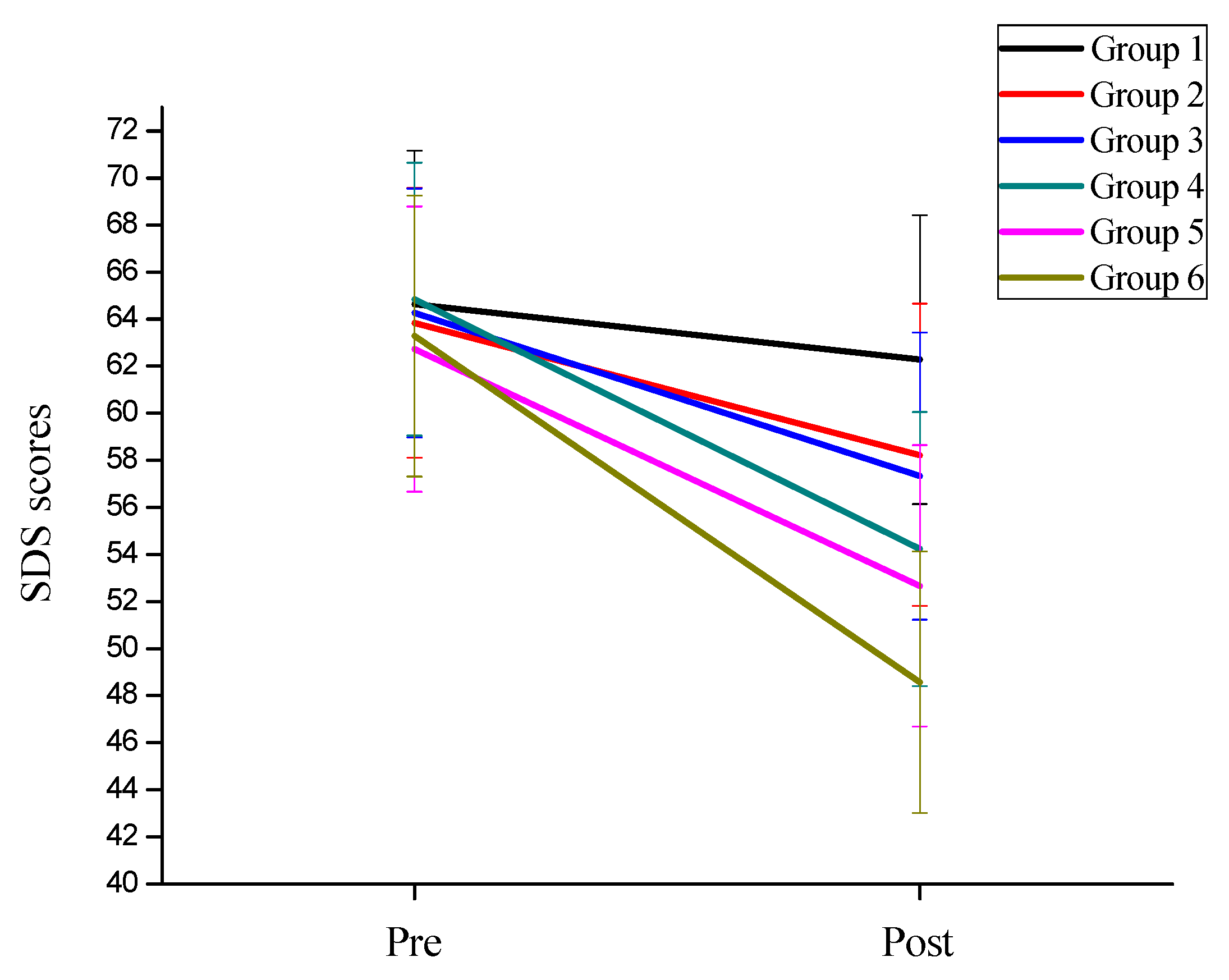
3.2.2. Effects of Exercise Intensity and Frequency on Depression Symptoms of College Students
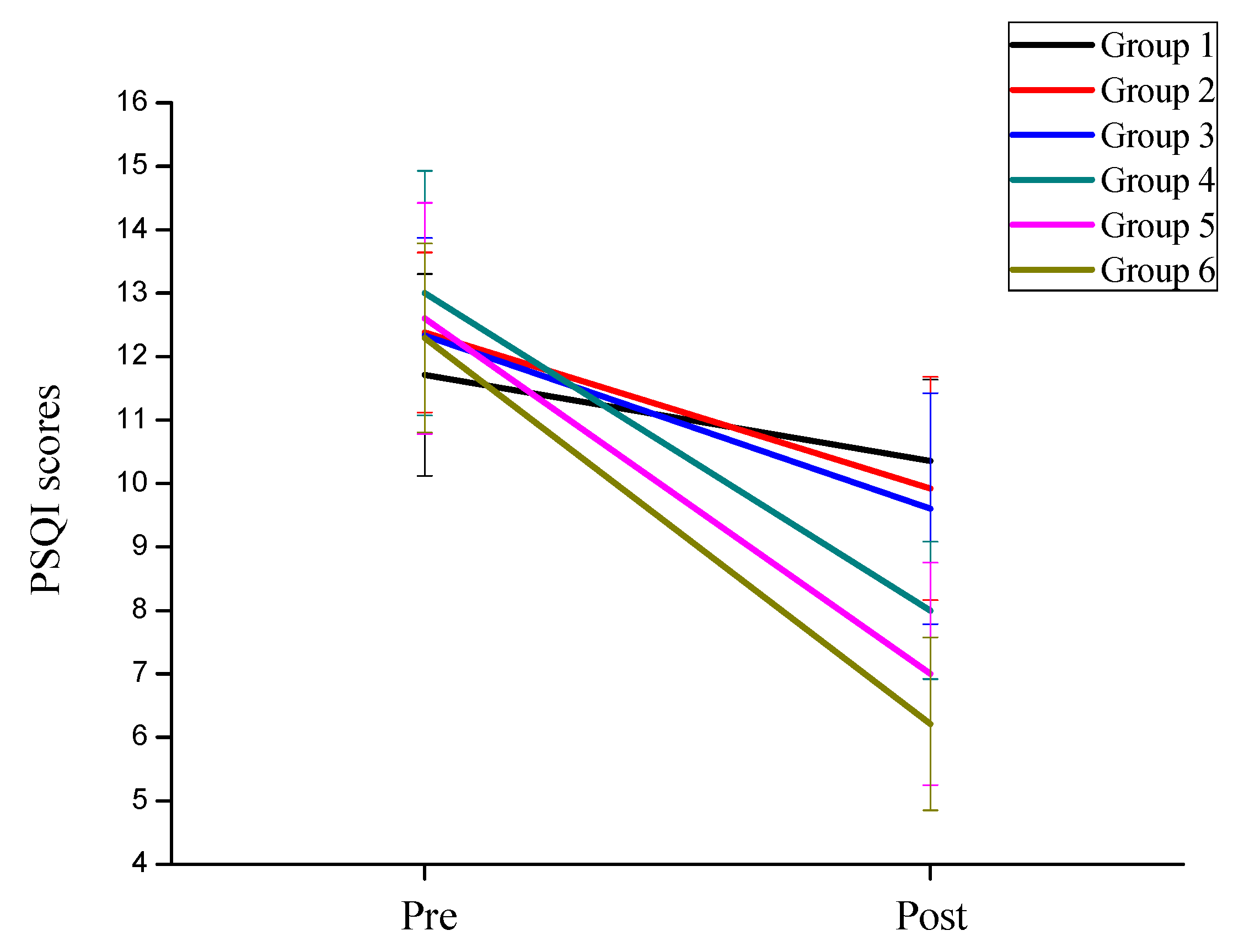
3.2.3. Effects of Exercise Intensity and Frequency on Sleep Quality Symptoms of College Students
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Zhan, H.; Zheng, C.; Zhang, X.; Yang, M.; Zhang, L.; Jia, X. Chinese college students’ stress and anxiety levels under COVID-19. Front. Psychiatry 2021, 12, 615390. [Google Scholar] [CrossRef] [PubMed]
- Han, W.; Xu, L.; Niu, A.; Jing, Y.; Qin, W.; Zhang, J.; Jing, X.; Wang, Y. Online-Based Survey on College Students’ Anxiety During COVID-19 Outbreak. Psychol. Res. Behav. Manag. 2021, 14, 385–392. [Google Scholar] [CrossRef] [PubMed]
- Patten, E.V.; Vaterlaus, J.M. Prevalence of depression, anxiety, and stress in undergraduate dietetics students. J. Nutr. Educ. Behav. 2021, 53, 67–74. [Google Scholar] [CrossRef] [PubMed]
- Anghel, E. Longitudinal invariance and information of the Depression, Anxiety, and Stress Scales. J. Clin. Psychol. 2020, 76, 1923–1937. [Google Scholar] [CrossRef] [PubMed]
- Ho, H.; Jose, I.; Cheesman, M.; Garrison, C.; Bishop, K.; Taber, S.; Witt, J.; Sin, M. Depression and anxiety management in parkinson disease. J. Neurosci. Nurs. 2021, 53, 170–176. [Google Scholar] [CrossRef]
- Kalin, N.H. Anxiety, depression, and suicide in youth. Am. J. Psychiat. 2021, 178, 275–279. [Google Scholar] [CrossRef]
- Kim, H.; Richardson, D.; Solberg, S.V. Understanding somatic symptoms associated with south korean adolescent suicidal ideation, depression, and social anxiety. Behav. Sci. 2021, 11, 151. [Google Scholar] [CrossRef]
- Malian, H.M.; Smith, P.J.; Hoffman, B.; Jiang, W.; Ammerman, K.; Kraus, W.E.; Hinderliter, A.; Sherwood, A.; Blumenthal, J.A. Effects of acute exercise on anxiety ratings in patients with coronary heart disease and elevated anxiety. J. Cardiopulm. Rehabil. 2021, 41, 277–281. [Google Scholar] [CrossRef]
- Ferreira, T.L.; Ribeiro, H.S.; Ribeiro, A.L.A.; Bonini-Rocha, A.C.; Lucena, J.M.S.; de Oliveira, P.A.; Amorim, F.R.S.; Ferreira, A.P.; Magno, L.A.V.; Martins, W.R. Exercise interventions improve depression and anxiety in chronic kidney disease patients: A systematic review and meta-analysis. Int. Urol. Nephrol. 2021, 53, 925–933. [Google Scholar] [CrossRef]
- Kandola, A.; Stubbs, B. Exercise and anxiety. Physical Exercise for Human Health. In Advances in Experimental Medicine and Biology; Xiao, J., Ed.; Springer: Singapore, 2020; Volume 1228, pp. 345–352. [Google Scholar]
- Bourbeau, K.; Moriarty, T.; Ayanniyi, A.; Zuhl, M. The combined effect of exercise and behavioral therapy for depression and anxiety: Systematic review and Meta-Analysis. Behav. Sci. 2020, 10, 116. [Google Scholar] [CrossRef]
- Gordon, B.R.; McDowell, C.P.; Lyons, M.; Herring, M.P. Resistance exercise training among young adults with analogue generalized anxiety disorder. J. Affect. Disord. 2021, 281, 153–159. [Google Scholar] [CrossRef] [PubMed]
- Axelsdottir, B.; Biedilae, S.; Sagatun, A.; Nordheim, L.V.; Larun, L. Review: Exercise for depression in children and adolescents—A systematic review and meta-analysis. Child. Adol. Ment. H-Uk. 2021, 26, 347–356. [Google Scholar] [CrossRef] [PubMed]
- Bellon, J.A.; Conejo-Ceron, S.; Sanchez-Calderon, A.; Rodriguez-Martin, B.; Bellon, D.; Rodriguez-Sanchez, E.; Mendive, J.M.; Ara, I.; Moreno-Peral, P. Effectiveness of exercise-based interventions in reducing depressive symptoms in people without clinical depression: Systematic review and meta-analysis of randomised controlled trials. Br. J. Psychiatry 2021, 219, 578–587. [Google Scholar] [CrossRef]
- Yin, J.; Tang, L.; Dishman, R.K. The effects of a single session of mindful exercise on anxiety: A systematic review and meta-analysis. Ment. Health Phys. Act. 2021, 21, 1–12. [Google Scholar] [CrossRef]
- Miyazaki, R.; Ayabe, M.; Kumahara, H.; Morimura, K.; Inukai, Y. Effects of light-to-moderate intensity aerobic exercise on objectively measured sleep parameters among community-dwelling older people. Arch. Gerontol. Geriat. 2021, 94, 104336. [Google Scholar] [CrossRef]
- Broman-Fulks, J.J.; Abraham, C.M.; Thomas, K.; Canu, W.H.; Nieman, D.C. Anxiety sensitivity mediates the relationship between exercise frequency and anxiety and depression symptomology. Stress Health 2018, 34, 500–508. [Google Scholar] [CrossRef]
- Hallgren, M.; Kandola, A.; Stubbs, B.; Thi-Thuy-Dung, N.; Wallin, P.; Andersson, G.; Ekblom-Bak, E. Associations of exercise frequency and cardiorespiratory fitness with symptoms of depression and anxiety—A cross-sectional study of 36,595 adults. Ment. Health Phys. Act. 2020, 19, 100351. [Google Scholar] [CrossRef]
- Oehlert, M.E.; Nelson, K.G.; King, N.; Reis, D.J.; Sumerall, S.; Neal, C.; Henry, P. Measurement-Based care: Use of the beck anxiety inventory (BAI) in a veteran population. Psychol. Serv. 2020, 17, 372–379. [Google Scholar] [CrossRef]
- Beck, A.T.; Brown, G.K.; Steer, R.A.; Kuyken, W.; Grisham, J. Psychometric properties of the Beck Self-Esteem Scales. Behav. Res. Ther. 2001, 39, 115–124. [Google Scholar] [CrossRef]
- Chen, X.; Hu, W.; Hu, Y.; Xia, X.; Li, X. Discrimination and structural validity evaluation of Zung self-rating depression scale for pregnant women in China. J. Psychosom. Obst. Gyn. 2020, 1–10. [Google Scholar] [CrossRef]
- Zhou, L.; Tian, Y.; Yu, J.; Chen, T.; An, F. Effect of at-home cognitive behavior therapy combined with nursing on revised piper fatigue scale, pittsburgh sleep quality index, self-rating anxiety scale and self-rating depression scale of ovarian cancer patients after chemotherapy. Int. J. Clin. Exp. Med. 2020, 13, 4227–4234. [Google Scholar]
- Jia, Y.; Chen, S.; Deutz, N.E.P.; Bukkapatnam, S.T.S.; Woltering, S. Examining the structure validity of the Pittsburgh Sleep Quality Index. Sleep Biol. Rhythms. 2019, 17, 209–221. [Google Scholar] [CrossRef]
- Ju, M.; Tao, Y.; Lu, Y.; Ding, L.; Weng, X.; Wang, S.; Fu, Q.; Li, X. Evaluation of sleep quality in adolescent patients with osteosarcoma using Pittsburgh Sleep Quality Index. Eur. J. Cancer Care 2019, 28, e13065. [Google Scholar] [CrossRef] [PubMed]
- Han, Q.; Liu, B.; Lin, S.; Li, J.; Liang, P.; Fu, S.; Zheng, G.; Yang, S.; Li, B.; Yang, Q. Pittsburgh Sleep Quality Index score predicts all-cause mortality in Chinese dialysis patients. Int. Urol. Nephrol. 2021, 53, 2369–2376. [Google Scholar] [CrossRef] [PubMed]
- Murphy, J.; Patte, K.A.; Sullivan, P.; Leatherdale, S.T. Exploring the association between sport participation and symptoms of anxiety and depression in a sample of canadian high school students. J. Clin. Sport Psychol. 2021, 15, 268–287. [Google Scholar] [CrossRef]
- Giles, A.; Nasstasia, Y.; Baker, A.; Kelly, B.; Ben, D.; Halpin, S.; Hides, L.; Callister, R. Exercise as treatment for youth with major depression: The healthy body healthy mind feasibility study. J. Psychiatr. Pract. 2020, 26, 444–460. [Google Scholar] [CrossRef]
- Jurado-Fasoli, L.; De-la-O, A.; Molina-Hidalgo, C.; Migueles, J.H.; Castillo, M.J.; Amaro-Gahete, F.J. Exercise training improves sleep quality: A randomized controlled trial. Eur. J. Clin. Investig. 2020, 50, e13202. [Google Scholar] [CrossRef]
- De Sousa, R.A.L.; Rocha-Dias, I.; de Oliveira, L.R.S.; Improta-Caria, A.C.; Monteiro-Junior, R.S.; Cassilhas, R.C. Molecular mechanisms of physical exercise on depression in the elderly: A systematic review. Mol. Biol. Rep. 2021, 48, 3853–3862. [Google Scholar] [CrossRef]
- Henriksson, M.; Wall, A.; Nyberg, J.; Adiels, M.; Lundin, K.; Bergh, Y.; Eggertsen, R.; Danielsson, L.; Kuhn, H.G.; Westerlund, M.; et al. Effects of exercise on symptoms of anxiety in primary care patients: A randomized controlled trial. J. Affect. Disord. 2022, 297, 26–34. [Google Scholar] [CrossRef]
- Anderson, C.L.; Feldman, D.B. Hope and physical exercise: The contributions of hope, Self-Efficacy, and optimism in accounting for variance in exercise frequency. Psychol. Rep. 2020, 123, 1145–1159. [Google Scholar] [CrossRef]
- Adams, T.G.; Forte, J.; Fogle, B.M.; Southwick, S.M.; Pietrzak, R.H. Self-reported exercise frequency and PTSD: Results from the National Health and Resilience in Veterans Study. Acta Psychiat. Scand. 2020, 142, 486–495. [Google Scholar] [CrossRef]
- Szuhany, K.L.; Otto, M.W. Assessing BDNF as a mediator of the effects of exercise on depression. J. Psychiatr. Res. 2020, 123, 114–118. [Google Scholar] [CrossRef] [PubMed]
- Johnston, S.A.; Roskowski, C.; He, Z.; Kong, L.; Chen, W. Effects of team sports on anxiety, depression, perceived stress, and sleep quality in college students. J. Am. Coll. Health 2021, 69, 791–797. [Google Scholar] [CrossRef] [PubMed]
- Lu, X.; Liu, L.; Yuan, R. Effect of the information support method combined with yoga exercise on the depression, anxiety, and sleep quality of menopausal women. Psychiat. Danub. 2020, 32, 380–388. [Google Scholar] [CrossRef] [PubMed]
- Tseng, T.; Chen, H.; Wang, L.; Chien, M. Effects of exercise training on sleep quality and heart rate variability in middle-aged and older adults with poor sleep quality: A randomized controlled trial. J. Clin. Sleep Med. 2020, 16, 1483–1492. [Google Scholar] [CrossRef]
- Daniel Jimenez-Garcia, J.; Hita-Contrera, F.; Jesus De La Torre-Cruz, M.; Aibar-Almazan, A.; Achalandabaso-Ochoa, A.; Fabrega-Cuadros, R.; Martinez-Amat, A. Effects of HIIT and MIIT suspension training programs on sleep quality and fatigue in older adults: Randomized controlled clinical trial. Int. J. Environ. Res. Public Health 2021, 18, 1211. [Google Scholar] [CrossRef]
- Glavin, E.E.; Matthew, J.; Spaeth, A.M. Gender differences in the relationship between exercise, sleep, and mood in young adults. Health Educ. Behav. 2021, 2, 1–13. [Google Scholar] [CrossRef]
- Yuan, M.; Fu, H.; Liu, R.; Fang, Y. Effect of frequency of exercise on cognitive function in older adults: Serial mediation of depression and quality of sleep. Int. J. Environ. Res. Public Health 2020, 17, 709. [Google Scholar] [CrossRef] [Green Version]
- Bayan-Bravo, A.; Perez-Tasigchana, R.F.; Lopez-Garcia, E.; Martinez-Gomez, D.; Rodriguez-Artalejo, F.; Guallar-Castillon, P. The association of major patterns of physical activity, sedentary behavior and sleeping with mortality in older adults. J. Sport Sci. 2019, 37, 424–433. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Group 1 | Group 2 | Group 3 | Group 4 | Group 5 | Group 6 | p-Value | |
|---|---|---|---|---|---|---|---|
| Gender (male/female) | 9/5 | 7/6 | 8/7 | 7/6 | 6/9 | 8/6 | 0.872 |
| Age (year) | 23.59 ± 2.02 | 24.32 ± 1.98 | 24.11 ± 2.87 | 25.08 ± 2.99 | 23.97 ± 2.03 | 24.06 ± 3.05 | 0.314 |
| Body height (cm) | 172.13 ± 11.12 | 170.34 ± 10.97 | 171.33 ± 9.08 | 168.04 ± 10.95 | 168.32 ± 9.03 | 173.11 ± 11.49 | 0.103 |
| Body weight (kg) | 67.32 ± 8.12 | 69.46 ± 9.17 | 67.34 ± 8.97 | 68.21 ± 10.03 | 66.35 ± 9.90 | 70.23 ± 9.92 | 0.116 |
| BMI (kg/m2) | 22.69 ± 2.01 | 23.09 ± 2.96 | 22.95 ± 2.53 | 23.12 ± 2.08 | 23.54 ± 3.07 | 23.40 ± 2.60 | 0.317 |
| Resting heart rate (times/min) | 76.35 ± 10.22 | 75.54 ± 9.79 | 75.76 ± 11.78 | 78.13 ± 10.36 | 76.98 ± 11.45 | 75.90 ± 9.06 | 0.203 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ji, C.; Yang, J.; Lin, L.; Chen, S. Physical Exercise Ameliorates Anxiety, Depression and Sleep Quality in College Students: Experimental Evidence from Exercise Intensity and Frequency. Behav. Sci. 2022, 12, 61. https://doi.org/10.3390/bs12030061
Ji C, Yang J, Lin L, Chen S. Physical Exercise Ameliorates Anxiety, Depression and Sleep Quality in College Students: Experimental Evidence from Exercise Intensity and Frequency. Behavioral Sciences. 2022; 12(3):61. https://doi.org/10.3390/bs12030061
Chicago/Turabian StyleJi, Chaoxin, Jun Yang, Lin Lin, and Song Chen. 2022. "Physical Exercise Ameliorates Anxiety, Depression and Sleep Quality in College Students: Experimental Evidence from Exercise Intensity and Frequency" Behavioral Sciences 12, no. 3: 61. https://doi.org/10.3390/bs12030061
APA StyleJi, C., Yang, J., Lin, L., & Chen, S. (2022). Physical Exercise Ameliorates Anxiety, Depression and Sleep Quality in College Students: Experimental Evidence from Exercise Intensity and Frequency. Behavioral Sciences, 12(3), 61. https://doi.org/10.3390/bs12030061